
Adaptation and Validation of the Nursing Attitude Questionnaire in a Spanish Population


 , , and
, , and
Abstract
:1. Introduction
1.1. Social Image of Nursing: Definition and Importance
1.2. Measures of the Social Image of Nursing
- -
- The Belgian Professional Self-Image Instrument for Nursing Students [34]: Designed to determine the issues affecting the recruitment and retention of nurses in Belgian hospitals.
- -
- The Porter Nursing Scale [35]: Analyzes perception differences in nursing among nurses based on variables such as years of experience, type of shift, or training.
- -
- The Professional Self-Concept of Nursing Instrument [36]: Evaluates constructs such as flexibility/creativity, knowledge, skill/competence, care, communication, leadership, and satisfaction.
- -
- The Nurses Self-Concept Instrument [37]: Analyzes the self-concept of nurses both locally and internationally.
- -
- The Nurses Self-Concept Questionnaire [38]: Designed to measure the self-concept of a group of nurses and to evaluate aspects related to nursing itself.
- -
- The Nurse Self-Description Form [39]: Measures variables such as empathy, professionalism, and ethics in nursing work.
- -
- The Nursing Brand Image Scale, Nursing Current Brand Position, and Nursing Desired Brand Position [40]: These three scales were designed to measure the corporate image of nursing.
- -
- The Nursing Image Scale: Initially developed by Özsoy [41], the original version consisted of 35 items organized into five factors: general appearance, communication, working, education level, and profession-related suggestions.
1.3. Nursing Attitude Questionnaire (NAQ)
- -
- Analyze the internal structure of the NAQ: Determine the number of dimensions that comprise it and assess whether these dimensions are hierarchically grouped under a general factor and associated specific factors, or if they are organized into correlated first-order factors.
- -
- Calculate the internal consistency of each identified factor.
- -
- Obtain evidence of convergent and discriminant validity by correlating the NAQ to other measures including nursing image, medical empathy, professional values, and communication skills.
- -
- Investigate evidence of differential validity of the NAQ based on gender.
- -
- Establish the norms for the evaluated sample.
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Instruments
2.4. Procedure
2.5. Ethical Considerations
2.6. Data Analysis
3. Results
3.1. Descriptive Analysis
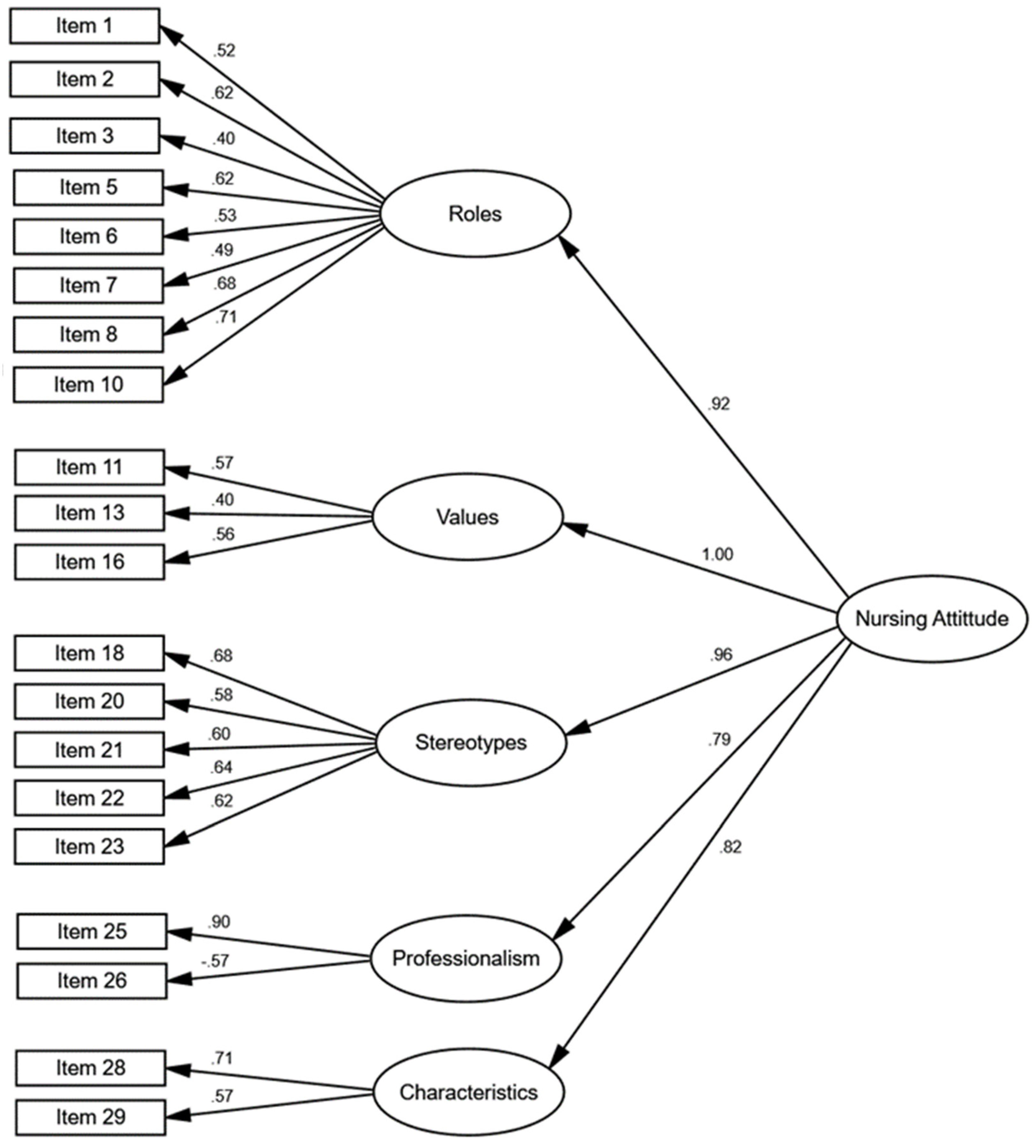
3.2. Internal Validity Evidence
3.3. Reliability Evidence of the 21-Item Test
3.4. Convergent and Discriminant Validity Evidence
3.5. Differential Validity Evidence
3.6. Norms/Scales
4. Discussion
4.1. Implications of the Present Study
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Acknowledgments
Conflicts of Interest
Appendix A. Nursing Attitude Questionnaire (Original Version)
- Nurses are patient advocates.
- Nurses protect patients in the healthcare system.
- Nursing professionals participate in the development of healthcare policy.
- Nursing professionals must wear white uniforms in order to be recognized.
- Nursing professionals are a resource for people with health problems.
- Nursing professionals are, in general, compassionate and kind people.
- It takes intelligence to be a nurse.
- The service provided by nurses is as important as the service provided by physicians.
- Everyone would benefit if nurses spent fewer hours in training and more time caring for patients.
- Nurses integrate theory and practice.
- Research is a vital part of the nursing profession.
- Nursing professionals are active in the political arena.
- Nursing professionals are able to work independently.
- Nurses speak out against undignified working conditions.
- The certainty that they are fasting people at work is sufficient compensation for nurses.
- Nurses should have the right to strike.
- Nursing professionals follow doctor’s orders without questioning them.
- Men make good nurses.
- Many of the nursing professionals would actually prefer to be physicians.
- Nursing is exciting.
- Nursing professionals include research findings in their clinical practice.
- The main objective of nursing research is to improve patient care.
- Nursing professionals value the time spent at the bedside caring for their patients.
- Nursing professionals should have a university degree for internships.
- Nurses make important contributions to patient care.
- One advantage of being a nurse is being able to marry a physician.
- Nursing is a respected profession.
- Nurses feel good about what they do.
- Nursing practice is continually being updated in relation to current health trends.
- Nurses are paid an adequate salary for the work they perform.
Appendix B. Nursing Attitude Questionnaire (Spanish Version)
- Los profesionales de enfermería son defensores de los pacientes.
- Los profesionales de enfermería protegen a los pacientes en el sistema de salud.
- Los profesionales de enfermería participan en el desarrollo de políticas de salud.
- Los profesionales de enfermería deben llevar uniforme blanco para poder ser reconocidos.
- Los profesionales de enfermería son un recurso para las personas con problemas de salud.
- Los profesionales de enfermería son, en general, personas compasivas y amables
- Se requiere inteligencia para ser enfermera.
- El servicio prestado por los profesionales de enfermería es tan importante como el que prestan los médicos.
- Todo el mundo se beneficiaría si los profesionales de enfermería pasaran menos horas formándose y más tiempo cuidando a pacientes.
- Los profesionales de enfermería integran teoría y práctica.
- La investigación es parte vital de la profesión enfermera.
- Los profesionales de enfermería son activos en el ámbito político.
- Los profesionales de enfermería son capaces de trabajar de forma independiente.
- Los profesionales de enfermería alzan la voz contra las condiciones laborales indignas.
- La certeza de que están ayunando a gente en su trabajo es compensación suficiente para los profesionales de enfermería.
- Los profesionales de enfermería deberían tener derecho a la huelga.
- Los profesionales de enfermería siguen las órdenes del médico sin cuestionarlas.
- Los hombres son buenos profesionales de enfermería.
- Muchos de los profesionales de enfermería en realidad preferirían ser médicos.
- La enfermería es emocionante.
- Los profesionales de enfermería incluyen en su práctica clínica resultados de investigación.
- El objetivo principal de la investigación en enfermería es mejorar la atención al paciente.
- Los profesionales de enfermería valoran el tiempo a pie de cama cuidando a sus pacientes.
- Los profesionales de enfermería deberían tener el título universitario para hacer prácticas.
- Los profesionales de enfermería hacen contribuciones importantes al cuidado de los pacientes.
- Una ventaja de ser enfermera es poder casarse con un médico.
- La enfermería es una profesión respetada.
- Las enfermeras se sienten bien con lo que hacen.
- La práctica enfermera está continuamente actualizándose en relación a las tendencias de salud actuales.
- Los profesionales de enfermería reciben un sueldo adecuado por el trabajo que realizan.
Appendix C. Norms for NAQ
| Percentile | Zn | T | Roles | ZRoles | Values | ZValues | Stereotypes | ZStereotypes | Professionalism | ZProfessionalism | Characteristics | ZCharacteristics | Total | ZTotal |
| 1 | −2.33 | 26.70 | 24.17 | −2.42 | 8.17 | −2.82 | 13.17 | −2.94 | 2.00 | −0.51 | 4.00 | −2.81 | 62.17 | −2.31 |
| 5 | −1.64 | 33.60 | 27.85 | −1.47 | 10.00 | −1.74 | 17.00 | −1.55 | 2.00 | −0.51 | 5.00 | −2.12 | 66.00 | −1.77 |
| 10 | −1.28 | 37.20 | 29.00 | −1.17 | 11.00 | −1.15 | 17.70 | −1.30 | 2.00 | −0.51 | 6.00 | −1.44 | 68.00 | −1.48 |
| 15 | −1.04 | 39.60 | 30.00 | −0.91 | 11.00 | −1.15 | 18.00 | −1.19 | 2.00 | −0.51 | 6.00 | −1.44 | 70.00 | −1.20 |
| 20 | −0.84 | 41.60 | 30.00 | −0.91 | 11.00 | −1.15 | 19.00 | −0.83 | 2.00 | −0.51 | 7.00 | −0.75 | 72.00 | −0.91 |
| 25 | −0.67 | 43.30 | 31.00 | −0.65 | 12.00 | −0.56 | 19.00 | −0.83 | 2.00 | −0.51 | 7.00 | −0.75 | 74.00 | −0.63 |
| 30 | −0.52 | 44.80 | 31.10 | −0.62 | 12.00 | −0.56 | 20.00 | −0.46 | 2.00 | −0.51 | 8.00 | −0.07 | 75.00 | −0.49 |
| 35 | −0.39 | 46.10 | 32.00 | −0.39 | 12.00 | −0.56 | 20.00 | −0.46 | 2.00 | −0.51 | 8.00 | −0.07 | 76.00 | −0.34 |
| 40 | −0.25 | 47.50 | 33.00 | −0.12 | 12.80 | −0.09 | 21.00 | −0.10 | 2.00 | −0.51 | 8.00 | −0.07 | 77.80 | −0.09 |
| 45 | −0.13 | 48.70 | 33.00 | −0.12 | 13.00 | 0.02 | 21.00 | −0.10 | 2.00 | −0.51 | 8.00 | −0.07 | 78.00 | −0.06 |
| 50 | 0.00 | 50.00 | 34.00 | 0.14 | 13.00 | 0.02 | 22.00 | 0.26 | 2.00 | −0.51 | 8.00 | −0.07 | 79.00 | 0.08 |
| 55 | 0.13 | 51.30 | 34.00 | 0.14 | 13.00 | 0.02 | 22.00 | 0.26 | 2.00 | −0.51 | 8.00 | −0.07 | 80.00 | 0.23 |
| 60 | 0.25 | 52.50 | 35.00 | 0.40 | 14.00 | 0.61 | 22.00 | 0.26 | 2.00 | −0.51 | 9.00 | 0.62 | 81.00 | 0.37 |
| 65 | 0.39 | 53.90 | 35.00 | 0.40 | 14.00 | 0.61 | 23.00 | 0.62 | 2.00 | −0.51 | 9.00 | 0.62 | 82.00 | 0.51 |
| 70 | 0.52 | 55.20 | 36.00 | 0.66 | 14.00 | 0.61 | 23.00 | 0.62 | 3.00 | 0.34 | 9.00 | 0.62 | 82.00 | 0.51 |
| 75 | 0.67 | 56.70 | 36.00 | 0.66 | 15.00 | 1.20 | 23.00 | 0.62 | 3.00 | 0.34 | 9.00 | 0.62 | 83.00 | 0.65 |
| 80 | 0.84 | 58.40 | 37.00 | 0.92 | 15.00 | 1.20 | 24.00 | 0.99 | 3.00 | 0.34 | 9.00 | 0.62 | 84.60 | 0.88 |
| 85 | 1.04 | 60.40 | 38.00 | 1.18 | 15.00 | 1.20 | 24.00 | 0.99 | 3.00 | 0.34 | 10.00 | 1.30 | 86.00 | 1.08 |
| 90 | 1.28 | 62.80 | 38.00 | 1.18 | 15.00 | 1.20 | 25.00 | 1.35 | 4.00 | 1.19 | 10.00 | 1.30 | 88.00 | 1.36 |
| 95 | 1.64 | 66.40 | 40.00 | 1.70 | 15.00 | 1.20 | 25.00 | 1.35 | 6.00 | 2.88 | 10.00 | 1.30 | 89.00 | 1.51 |
| 99 | 2.33 | 73.30 | 40.00 | 1.70 | 15.00 | 1.20 | 25.00 | 1.35 | 7.83 | 4.43 | 10.00 | 1.30 | 92.00 | 1.93 |
| n | 316 | 316 | 316 | 316 | 316 | 316 | 316 | 316 | 316 | 316 | 316 | 316 | 316 | 316 |
| Mean | 0.00 | 50.00 | 33.48 | 0.00 | 12.96 | 0.00 | 21.28 | 0.00 | 2.60 | 0.00 | 8.10 | 0.00 | 78.42 | 0.00 |
| SD | 1.00 | 10.00 | 3.84 | 1.00 | 1.70 | 1.00 | 2.76 | 1.00 | 1.18 | 1.00 | 1.46 | 1.00 | 7.02 | 1.00 |
| Note: n, sampling size; T, T-score; Z, standardized score; Zn, normalized standard score. | ||||||||||||||
References
- Braš, M.; Đordević, V.; Pjevač, N.; Kaštelan, S.; Klarica, M.; Orešković, S. How to teach person-centered medicine during the coronavirus disease 2019 pandemic? Croat Med. J. 2022, 63, 98–100. [Google Scholar] [CrossRef] [PubMed]
- Salihović, A.; Mahmutović, J.; Branković, S. Nursing students’ attitudes about their profession. J. Health Sci. 2024, 11, 168–171. [Google Scholar] [CrossRef]
- Wakefeld, M.; Williams, D.R.; Le Menestrel, S. The Future of Nursing 2020–2030: Charting a Path to Achieve Health Equity; National Academy of Sciences: Washington, DC, USA, 2021. [Google Scholar]
- Archibald, M.M.; Barnard, A. Futurism in nursing: Technology, robotics and the fundamentals of care. J. Clin. Nurs. 2018, 27, 2473–2480. [Google Scholar] [CrossRef]
- Grinberg, K.; Sela, Y. Perception of the image of the nursing profession and its relationship with quality of care. BMC Nurs. 2022, 21, 57. [Google Scholar] [CrossRef]
- Liu, N.Y.; Hsu, W.Y.; Hung, C.A.; Wu, P.L.; Pai, H.C. The effect of gender role orientation on student nurses’ caring behaviour and critical thinking. Int. J. Nurs. Stud. 2019, 1, 18–23. [Google Scholar] [CrossRef]
- American Nurses Association (ANA). Nursing Scope & Standards of Practice, 4th ed.; American Nurses Association: Silver Spring, MD, USA, 2021. [Google Scholar]
- Brandão, S.; Peres, M.; Aparibense, P.G.; Lopes, R.; Santos, J.; Brandão, M. Evidence of nursing patterns of knowing communicated by the brazilian press before Florence Nightingale’s model. Rev. Bras. Enferm. 2020, 73 (Suppl. S5), e20190790. [Google Scholar] [CrossRef]
- Hoseini, T.; Varasteh, S.; Esmaeili, M. Explain the professional identity of nursing during COVID-19 pandemic. Nurs. Open 2024, 11, e2253. [Google Scholar] [CrossRef]
- Smith, C.; Horne, C. Educational and professional experiences of men in nursing: An interpretive description study to guide change and foster inclusive environments for men in nursing. J. Prof. Nurs. 2024, 53, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.; Lane, S.; Brackney, D.; Horne, C.E. Role expectations and workplace relations experienced by men in nursing: A qualitative study through an interpretive description lens. J. Adv. Nurs. 2020, 76, 1211–1220. [Google Scholar] [CrossRef]
- Barros, A.; Menegaz, J.; Santos, J.; Polaro, S.; Trindade, L.; Meschial, W. Nursing care management concepts: Scoping review. Rev. Bras. Enferm. 2023, 76, e20220020. [Google Scholar] [CrossRef]
- Instituto Nacional de Estasítica. Available online: https://www.ine.es/jaxi/Datos.htm?tpx=49002 (accessed on 15 September 2024).
- Ahmadi, F.; Shaker, H.; Eterafi, M.; Kamran, A. Exploring nursing students’ perceptions from nursing role function (SP-NRF) during the COVID-19 pandemic in Ardabil Province: A cross-sectional study from Iran. BMC Nurs. 2023, 22, 219. [Google Scholar] [CrossRef] [PubMed]
- Dost, A.; Bahçecik, A.N. Determination of professional image perceptions of nursing students. J. Educ. Res. Nurs. 2022, 19, 350–355. [Google Scholar] [CrossRef]
- Sillero, A.; Gil, M.; Marques-Sulem, E.; Ayuso, R. Motivations and expectations of generation Z nursing students: A post-pandemic career choice qualitative analysis. J. Prof. Nurs. 2023, 49, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-González, R.; Martínez-Santos, A.; De La Fuente, N.; López-Pérez, M.; Fernandez-De-La-Iglesia, J. Identifying engagement and associated factors in nursing students: An exploratory study. J. Prof. Nurs. 2023, 48, 77–83. [Google Scholar] [CrossRef]
- Rubinstein, D. Professional identity and image as factors that affect the profession. In Contemporary Nursing Ethics; Rubinstein, D., Tabak, N., Eds.; Dyonon Publishing: Tel Aviv, Israel, 2013. (In Hebrew) [Google Scholar]
- Nursing and Midwifery Council. The Code. 2018. Available online: https://www.nmc.org.uk/standards/code/ (accessed on 10 July 2024).
- Abdelrahman, S. Relationship among public nursing image, self-image, and self-esteem of nurses. Nurs. Health Sci. 2018, 7, 10–16. [Google Scholar] [CrossRef]
- López-Verdugo, M.; Ponce-Blandón, J.A.; López-Narbona, F.J.; Romero-Castillo, R.; Guerra-Martín, M.D. Social image of nursing. An integrative review about a yet unknown profession. Nurs. Rep. 2021, 11, 460–474. [Google Scholar] [CrossRef]
- Maliheh, N.M.; Ashraf, A.; Hamid, H.; Taghi, S.M.; Fatemeh, H.N. The Public Nursing Image as Perceived by Nurses and Citizens: A Questionnaire Survey. Int. J. Caring Sci. 2021, 13, 1611–1617. [Google Scholar]
- Kristoffersen, M. Does professional identity play a critical role in the choice to remain in the nursing profession? Nurs. Open 2021, 8, 1928–1936. [Google Scholar] [CrossRef]
- Zhou, Y.; Weng, L.; Wang, M.; Huang, G. Male nursing students’ experiences of their clinical internships: A qualitative study. Heliyon 2024, 10, e31075. [Google Scholar] [CrossRef]
- Ulrich, B. What’s your professional identity as a nurse? Nephr. Nurs. J. 2023, 50, 377. [Google Scholar] [CrossRef]
- Cajachagua-Castro, M.; Roque-Guerra, E.; Conque-Machaca, N.; Mamani-Contreras, R.; Chavez-Sosa, J. Cuidado invisible e Imagen social de la enfermera comunitaria. ENE 2022, 16, 1297. Available online: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1988-348X2022000300009&lng=es&tlng=es (accessed on 2 August 2024).
- Atashzadeh-Shoorideh, F.; Monjazabi, F.; Fathollahzadeh, E.; Parastoo, O. The obstacles to nurses being present with patients. Nurs. Open 2021, 8, 1115–1124. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Du, Y.; Shen, Z.; Qin, W.; Zhang, Y. How the public perceives the “good nurse” in China: A content analysis of national newspapers. J. Nurs. Scholarsh. 2024, 56, 164–173. [Google Scholar] [CrossRef]
- Wałowska, K.; Domaradzki, J. Superheroes or Super Spreaders? The Impact of the COVID-19 Pandemic on Social Attitudes towards Nurses: A Qualitative Study from Poland. Int. J. Environ. Res. Public Health 2023, 20, 2912. [Google Scholar] [CrossRef]
- Siebens, K.; De Casterlé, B.D.; Abraham, I.; Dierckx, K.; Braes, T.; Darras, E.; Dubois, Y.; Milisen, K.; BELIMAGE Group. The professional self-image of nurses in Belgian hospitals: A cross-sectional questionnaire survey. Int. J. Nurs. Stud. 2006, 43, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Porter, R.T.; Porter, M.J. Career development: Our professional responsibility. J. Prof. Nurs. 1991, 7, 208–212. [Google Scholar] [CrossRef]
- Arthur, D. Measurement of the professional self-concept of nurses: Developing a measurement instrument. Nurse Educ. Today 1995, 15, 328–335. [Google Scholar] [CrossRef]
- Angel, E.; Craven, R.; Denson, N. The nurses self-concept instrument (NSCI): Assessment of psychometric properties for Australian domestic and international student nurses. Int. J. Nurs. Stud. 2012, 49, 880–886. [Google Scholar] [CrossRef]
- Cowin, L. Measuring Nurses’ Self-Concept. West. J. Nurs. Res. 2001, 23, 313–325. [Google Scholar] [CrossRef]
- Dagenais, F.; Meleis, A.I. Professionalism, work ethic, and empathy in nursing: The nurse self-description form. West. J. Nurs. Res. 1982, 4, 407–422. [Google Scholar] [CrossRef]
- Godsey, J.; Hayes, T.; Schertzer, C.; Kallmeyer, R.; Mukherjee, A.; Weber, J. Development and testing of three unique scales measuring the brand image of nursing. Int. J. Pharm. Healthc. Mark. 2018, 12, 2–14. [Google Scholar] [CrossRef]
- Özsoy, S.A. Determination of nursing image in the community. J. Ege Univ. Fac. Nurs. 2000, 16, 1–19. [Google Scholar]
- Toth, J.C.; Dobratz, M.A.; Boni, M.S. Attitude toward nursing of students earning a second degree and traditional baccalaureate students: Are they different? Nurs. Outlook 1998, 46, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Hoskins, L.M. View of Nursing Questionnaire [Mimeograph]; The Catholic University of America: Washington, DC, USA, 1983. [Google Scholar]
- Cukljek, S.; Juresa, V.; Babic, J. The cross-cultural (transcultural) adaptation and validation of the nursing image questionnaire. Nurse Educ. Today 2017, 48, 67–71. [Google Scholar] [CrossRef]
- Hung, C.-A.; Wu, P.-L.; Liu, N.-Y.; Hsu, W.-Y.; Lee, B.-O.; Pai, H.-C. The effect of gender-friendliness barriers on perceived image in nursing and caring behaviour among male nursing students. J. Clin. Nurs. 2019, 28, 1465–1472. [Google Scholar] [CrossRef]
- Wang, Q.; Cao, X.; Du, T. First-year nursing students’ initial contact with the clinical learning environment: Impacts on their empathy levels and perceptions of professional identity. BMC Nurs. 2022, 21, 234. [Google Scholar] [CrossRef]
- Liebig, D.; Embree, J.L.; Lough, C. Values and Ethics Domain for Professional Identity in Nursing. J. Contin. Educ. Nurs. 2024, 55, 279–281. [Google Scholar] [CrossRef]
- Ding, X.; Wang, L.; Sun, J.; Li, D.; Zheng, B.; He, S.; Latour, J.M. Effectiveness of empathy clinical education for children’s nursing students: A quasi-experimental study. Nurse Educ. Today 2019, 85, 104260. [Google Scholar] [CrossRef]
- Çınar, Ş.; Demir, Y. Nursing Image in Society: A Scale Development Study. Anat. J. Nurs. Health Sci. 2010, 12, 24–33. [Google Scholar]
- Hojat, M.; Mangione, S.; Kane, G.; Gonnella, J.S. Relationships between scores of the Jefferson Scale of Physician Empathy (JSPE) and the Interpersonal Reactivity Index (IRI). Med. Teach. 2005, 27, 625–628. [Google Scholar] [CrossRef]
- Weis, D.; Schank, M.J. Development and psychometric evaluation of the Nurses Professional Values Scale Revised. J. Nurs. Meas. 2009, 17, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Leal-Costa, C.; Tirado, S.; Ramos-Morcillo, A.J.; Ruzafa-Martínez, M.; Díaz, J.L.; Van-der Hofstadt, C.J. Communication Skills and Professional Practice: Does It Increase Self-Efficacy in Nurses? Front. Psychol. 2020, 12, 1169. [Google Scholar] [CrossRef] [PubMed]
- Sousa, V.D.; Rojjanasrirat, W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: A clear and user-friendly guideline. J. Eval. Clin. Pract. 2011, 17, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Kirchherr, J.; Charles, K. Enhancing the sample diversity of snowball samples: Recommendations from a research project on anti-dam movements in Southeast Asia. PLoS ONE 2018, 13, e0201710. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar]
- Bentler, P.M.; Bonett, D.G. Significance tests and goodness of fit in the analysis of covariance structures. Acad. Psychol. Bull. 1980, 88, 588–606. [Google Scholar] [CrossRef]
- Jöreskog, K.G.; Sörbom, D. LISREL 8: User’s Guide; Scientific Software International: Chicago, IL, USA, 1993. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fi t indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Hair, J.F.; Anderson, R.E.; Tatham, R.L.; Black, W.C. Análisis Multivariante; Prentice Hall: Englewood Cliffs, NJ, USA, 1999. [Google Scholar]
- James, L.R.; Mulaik, S.A.; Brett, J.M. Causal Analysis: Models, Assumptions and Data; Sage: Thousand Oaks, CA, USA, 1982. [Google Scholar]
- Byrne, B.M. Structural Equation Modeling with AMOS Basic Concepts, Applications, and Programming; Lawrence Erlbaum: Mahwah, NJ, USA, 2001. [Google Scholar]
- Arbuckle, J.L. Amos 7.0 User’s Guide; SPSS: Chicago, IL, USA, 2006. [Google Scholar]
- West, S.G.; Finch, J.F.; Curran, P.J. Structural equation models with non-normal variables. In Structural Equation Modeling: Concepts, Issues and Applications; Hoyle, R.H., Ed.; Sage: Thousand Oaks, CA, USA, 1995; pp. 56–75. [Google Scholar]
- Bollen, K.A.; Stine, R.A. Bootstrapping goodness-of-fit measures in structural equation models. In Testing Structural Equation Models; Bollen, K.A., Long, J.S., Eds.; Sage: Thousand Oaks, CA, USA, 1993; pp. 111–135. [Google Scholar]
- Cohen, J. A Power Primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Zhou, L.; Sukpasjaroen, K.; Cai, E.; Moonsri, K.; Imsiri, P.; Chankoson, T. The psychometric properties of nursing image measurement instruments: A systematic review. Nurs. Open 2023, 10, 5056–5078. [Google Scholar] [CrossRef]
- Solera-Gómez, S.; Sancho-Cantus, D.; Privado, J.; Cunha-Pérez, C.; Benedito-Monleón, A.; Llinares-Insa, L.-I. (In review) Adaptation and validation of the Nursing Image Scale in a Spanish population. Int. Nurs. Rev.
- Fernández-Feito, A.; Palmeiro-Longo, M.; Hoyuelos, S.; García-Díaz, V. How work setting and job experience affect professional nurses’ values. Nurs. Ethics 2019, 26, 134–147. [Google Scholar] [CrossRef]
- Blanco, J.M.; Blanco, A.; Caballero, F.; Hawkins, M.; Fernández, T.; Lledó, L.; López, A.; Piñas, A.; Vara, E.; Monge, D. Medical empathy in medical students in Madrid: A proposal for empathy level cut-off points for Spain. PLoS ONE 2022, 17, e0267172. [Google Scholar] [CrossRef] [PubMed]
- Montilva, M.; Garcia, M.; Torres, A.; Puertas, M.; Zapata, E. Empatía según la escala de Jefferson en estudiantes de Medicina y Enfermería en Venezuela. Investig. Educ. Méd. 2015, 4, 223–228. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Instrument | Author/s | Sample | Factorial Structure | Reliability | Validity |
|---|---|---|---|---|---|
| Porter Nursing Scale | Porter and Porter (1991) | 303 nurses (90% women) | 3: interpersonal power, interpersonal skills, interpersonal relationships | α = 0.85 | |
| The Nursing Attitudes/Image Questionnaire (NAQ/NIQ) | Toth et al. (1998) | 338 people. Six of the traditional students were enrolled in a Bachelor of Science in nursing degree/Master of Science in nursing degree program, 31 were RNs, 22 held associate’s degrees, and 9 were diploma graduates. | 5 dimensions, 30 items: 1. Roles 2. Values 3. Stereotypes 4. Professionalism 5. Nursing characteristics | α = 0.75–0.80 | Content Validity: Determined by a panel of undergraduate nursing students. Construct Validity: Measured by comparing 45 registered nurses with 45 non-registered nurses. |
| Belgian professional self-image instrument for nursing students, | Siebens et al. (2006) | 9638 nurses from 22 hospitals in Belgium | 3 dimensions, 52 items: 1. Competence 2. Nursing care 3. Team | ||
| The Professional Self-concept of Nurses Instrument | Arthur (1995) | 170 third-year nursing students | 3 dimensions, 5 subdimensions, 27 items: 1. Professional practice 2. Satisfaction 3. Communication | α = 0.89 | EFA: 40%–57.30% of the variance was explained (n = 170) |
| The Nurses Self-Concept Instrument | Angel et al. (2012) | 253 university nursing students from Sydney | 4 dimensions, 14 items: 1. Care 2. Knowledge 3. Relationship with the staff 4. Leadership | α = 0.94 | CFA showed good fit of the original factor structure, RMSEA = 0.066 (95% CI: 0.051–0.080), NNFI = 0.98, CFI = 0.99, x2 = 148.89, df = 71, p-value for test of close fit = 0.025 |
| The Nurses Self-Concept Questionnaire, NSCQ | Cowin (2001) | 506 undergraduate nursing students and 508 practicing nurses | 6 dimensions, 36 items: 1. General nursing 2. Care 3. Relationship with the staff 4. Communication 5. Knowledge 6. Leadership | α = 0.90 | CFA: 72.9% of the variance was explained. CFA showed good fit, TLI = 0.911, RNI = 0.887, GFI = 0.906, x2 = 787.05, df = 120 |
| The Nurse Self-Description Form, NSDF | Dagenais and Meleis (1982) | 186 graduate nurses | 3 dimensions, 19 items: 1. Professionalism 2. Empathy 3. Ethical work | α = 0.90 | EFA: 62.5 of the variance was explained |
| The Nursing Brand Image Scale, NBIS | Godsey et al. (2018) | 286 participants, 152 nurses | 7 dimensions, 42 sentences: 1. Leaders’ influence 2. Qualification for advanced nursing practice 3.Qualified caregivers 4. Strong interpersonal skills 5. Lack of authority 6. Expert healthcare providers 7. Appreciation by society | α = 0.92 | EFA: 61.6% of the variance was explained |
| Nursing’s Current Brand Position Scale, NCPBS | Godsey et al. (2018) | 286 participants, 152 nurses | 3 dimensions, 10 items: 1. Influence of leaders 2. Patient-centered care 3. Patient advocates | α = 0.92 | CFA: 68.4% of the variance was explained |
| Nursing’s Desired Brand Position Scale, NDBPS | Godsey et al., 2018 | 286 participants, 152 nurses | 2 dimensions, 10 items: 1. Influence of leaders 2. Patient-centered care | α = 0.90 | CFA: 68.3% of the variance was explained |
| Nurse Image questionnaire | Özsoy, 2000 | 5 factors: General Impression, Communication, Working Conditions, Level of Education, and Suggestions Related to the Profession | The internal consistency coefficient is α = 0.709 | The scale was validated on a sample of 500 individuals in Turkey, with a gender distribution of 50.0% women. Of the total sample, 44.4% had completed secondary education |
| Measures | M | SD | Skewness | Kurtosis | α | Item-Total Corrected Correlation |
|---|---|---|---|---|---|---|
| Roles (NAQ) | 33.48 | 3.84 | −0.57 | 1.30 | 0.652 | 0.19 to 0.57 |
| Values (NAQ) | 12.96 | 1.70 | −0.42 | −0.58 | 0.125 | 0.05 to 0.09 |
| Stereotypes (NAQ) | 21.28 | 2.76 | −0.53 | −0.34 | 0.614 | 0.26 to 0.45 |
| Professionalism (NAQ) | 2.60 | 1.18 | 2.73 | 8.87 | 0.493 | 0.33 |
| Characteristics (NAQ) | 8.10 | 1.46 | −0.63 | −0.04 | 0.491 | 0.33 |
| Nursing attitude (NAQ) | 78.42 | 7.02 | −0.25 | −0.55 | 0.789 | 0.18 to 0.53 |
| Working Conditions (NIS) | 4.17 | 1.15 | 0.71 | −0.36 | 0.394 | |
| Education (NIS) | 6.91 | 1.46 | 2.00 | 4.26 | 0.626 | |
| Occupation (NIS) | 11.50 | 2.14 | 0.88 | 0.70 | 0.579 | |
| General View (NIS) | 5.75 | 1.49 | 0.59 | −0.67 | 0.664 | |
| Empathy (NIS) | 8.62 | 2.33 | 0.69 | −0.51 | 0.765 | |
| Nursing Image (NIS) | 36.95 | 5.98 | 0.93 | 1.18 | 0.826 | |
| Perspective-Taking (JSE-HP) | 62.65 | 6.93 | −1.17 | 1.07 | 0.820 | |
| Compassionate Care (JSE-HP) | 41.52 | 7.21 | −1.13 | 1.09 | 0.713 | |
| Empathy (JSE-HP) | 14.22 | 3.13 | −0.37 | 0.23 | 0.343 | |
| Medical Empathy (JSE-HP) | 118.39 | 13.86 | −0.89 | 0.48 | 0.832 | |
| Ethics (NPVS) | 42.44 | 3.80 | −2.12 | 4.93 | 0.845 | |
| Commitment (NPVS) | 36.90 | 3.76 | −1.48 | 1.81 | 0.863 | |
| Mastery (NPVS) | 41.62 | 4.10 | −1.65 | 2.66 | 0.840 | |
| Professional Values (NPVS) | 120.95 | 10.92 | −1.91 | 3.91 | 0.941 | |
| Empathy (HP-CSS) | 26.82 | 3.65 | −1.74 | 3.97 | 0.893 | |
| Informative Communication (HP-CSS) | 31.29 | 4.01 | −1.24 | 2.36 | 0.801 | |
| Respect (HP-CSS) | 16.36 | 2.05 | −1.69 | 3.99 | 0.832 | |
| Social Skills (HP-CSS) | 17.90 | 3.24 | −0.06 | -0.33 | 0.561 | |
| Total Communication Skills (HP-CSS) | 97.68 | 11.37 | −1.27 | 2.75 | 0.913 |
| Model | χ2/df | GFI | NFI | PGFI | PNFI | SRMR |
|---|---|---|---|---|---|---|
| Five correlated factors with 30 items | 3.55 | 0.907 | 0.836 | 0.770 | 0.750 | 0.078 |
| Five correlated factors with 21 items | 1.62 | 0.972 | 0.956 | 0.740 | 0.805 | 0.063 |
| Hierarchical model with 30 items | 3.52 | 0.906 | 0.825 | 0.782 | 0.761 | 0.078 |
| Hierarchical model with 21 items | 1.65 | 0.970 | 0.954 | 0.767 | 0.833 | 0.065 |
| Convergent Validity | 143.15 | 0.995 | 0.990 | 0.758 | 0.834 | 0.055 |
| Roles (NAQ) | Values (NAQ) | Stereotypes (NAQ) | Professionalism (NAQ) | Characteristics (NAQ) | Nursing Attitude (NAQ) | |
|---|---|---|---|---|---|---|
| Working Conditions (NIS) | −0.16 | −0.21 | −0.15 | 0.21 | −0.09 | −0.17 |
| Education (NIS) | −0.31 | −0.35 | −0.32 | 0.34 | −0.17 | −0.33 |
| Occupation (NIS) | −0.34 | −0.43 | −0.41 | 0.31 | −0.26 | −0.42 |
| General View (NIS) | −0.26 | −0.20 | −0.17 | 0.16 | −0.21 | −0.25 |
| Empathy (NIS) | −0.41 | −0.26 | −0.29 | 0.18 | −0.29 | −0.40 |
| Nursing Image (NIS) | 0.45 | 0.42 | 0.40 | 0.34 | 0.31 | 0.48 |
| Perspective-Taking (JSE-HP) | 0.42 | 0.34 | 0.42 | 0.49 | 0.32 | 0.43 |
| Compassionate Care (JSE-HP) | 0.31 | 0.27 | 0.27 | 0.45 | 0.20 | 0.28 |
| Empathy (JSE-HP) | 0.11 | 0.12 | 0.13 | 0.19 | 0.07 | 0.11 |
| Medical Empathy (JSE-HP) | 0.42 | 0.37 | 0.41 | 0.53 | 0.31 | 0.42 |
| Ethics (NPVS) | 0.30 | 0.27 | 0.35 | 0.31 | 0.21 | 0.33 |
| Commitment (NPVS) | 0.29 | 0.31 | 0.34 | 0.30 | 0.19 | 0.33 |
| Mastery (NPVS) | 0.30 | 0.30 | 0.32 | 0.36 | 0.19 | 0.32 |
| Professional Values (NPVS) | 0.31 | 0.31 | 0.35 | 0.34 | 0.21 | 0.35 |
| Empathy (HP-CSS) | 0.39 | 0.29 | 0.42 | 0.28 | 0.32 | 0.43 |
| Informative Communication (HP-CSS) | 0.36 | 0.30 | 0.39 | 0.31 | 0.33 | 0.40 |
| Respect (HP-CSS) | 0.40 | 0.31 | 0.45 | 0.32 | 0.35 | 0.45 |
| Social Skills (HP-CSS) | 0.21 | 0.16 | 0.24 | 0.15 | 0.15 | 0.24 |
| Total Communication Skills (HP-CSS) | 0.40 | 0.31 | 0.44 | 0.31 | 0.34 | 0.45 |
| Measures | Male M (SD) | Female M (SD) | t-Test | Cohen’s d |
|---|---|---|---|---|
| Roles | 33.91 (4.68) | 33.38 (3.61) | t314 = 0.98, p = 0.326 | 0.14 |
| Values | 12.81 (1.79) | 13.00 (1.68) | t314 = −0.79, p = 0.431 | 0.11 |
| Stereotypes | 21.17 (2.81) | 21.31 (2.75) | t314 = −0.36, p = 0.722 | 0.05 |
| Professionalism | 2.94 (1.57) | 2.51 (1.05) | t78 = 2.59, p = 0.044 | 0.36 |
| Characteristics | 7.92 (1.57) | 8.14 (1.43) | t314 = -1.08, p = 0.280 | 0.15 |
| Nursing Attitude | 78.75 (7.48) | 78.34 (6.91) | t314 = 0.42, p = 0.678 | 0.06 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solera-Gómez, S.; Sancho-Cantus, D.; Privado, J.; Cunha-Pérez, C.; Benedito-Monleón, A.; Llinares-Insa, L.I. Adaptation and Validation of the Nursing Attitude Questionnaire in a Spanish Population. Nurs. Rep. 2024, 14, 2758-2776. https://doi.org/10.3390/nursrep14040204
Solera-Gómez S, Sancho-Cantus D, Privado J, Cunha-Pérez C, Benedito-Monleón A, Llinares-Insa LI. Adaptation and Validation of the Nursing Attitude Questionnaire in a Spanish Population. Nursing Reports. 2024; 14(4):2758-2776. https://doi.org/10.3390/nursrep14040204
Chicago/Turabian StyleSolera-Gómez, Silvia, David Sancho-Cantus, Jesús Privado, Cristina Cunha-Pérez, Amparo Benedito-Monleón, and Lucía Inmaculada Llinares-Insa. 2024. "Adaptation and Validation of the Nursing Attitude Questionnaire in a Spanish Population" Nursing Reports 14, no. 4: 2758-2776. https://doi.org/10.3390/nursrep14040204