Improving Health Professionals’ Involvement Whilst Sustaining Work–Life Balance: Evidence from an Empirical Analysis


Abstract
:1. Introduction
- R.Q. 1: Does employees’ involvement affect the work–life balance of employees?
- R.Q. 2: Does a supportive organizational climate mediate the implications of employees’ involvement on individual work–life balance?
- R.Q. 3: Which kind of managerial interventions are needed for fostering the contribution of employees’ involvement on healthcare organizations’ sustainability?
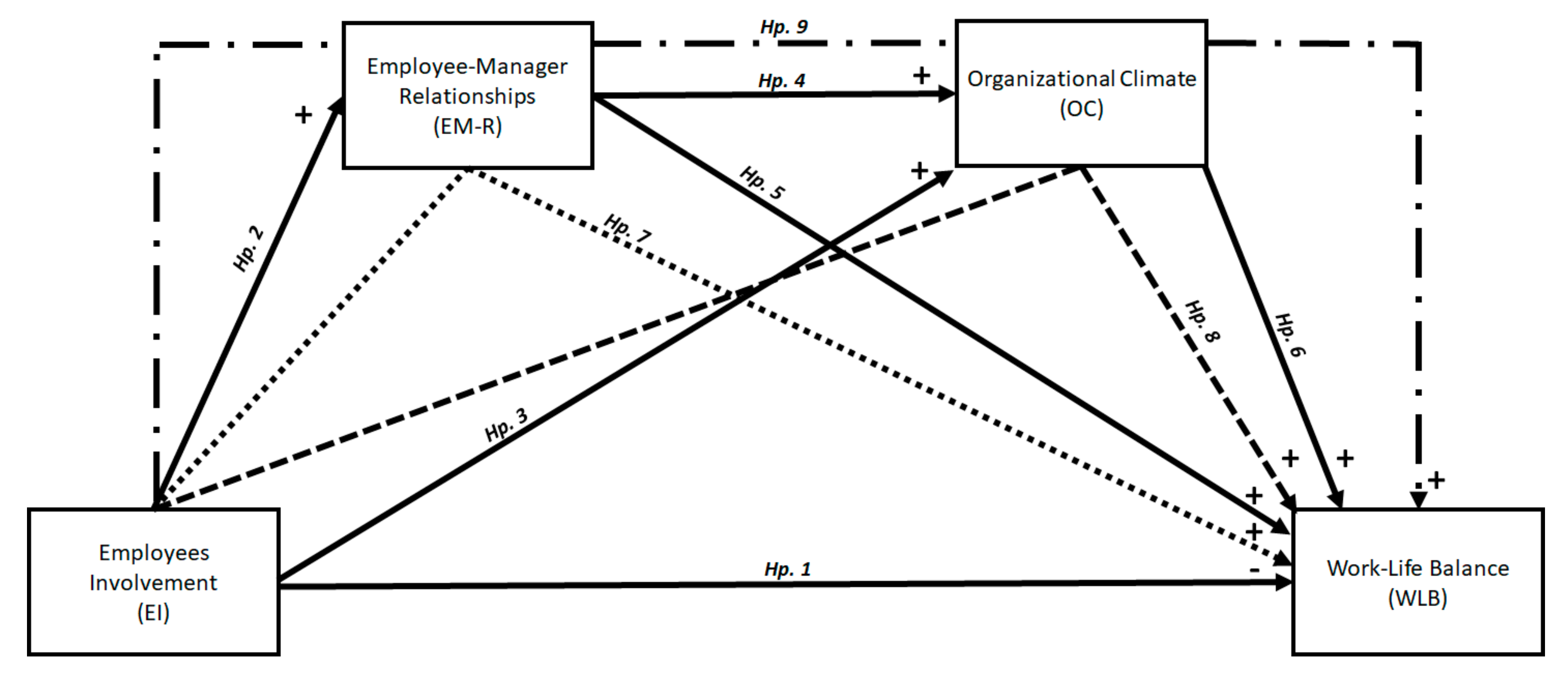
2. Theoretical Framework and Research Hypotheses
3. Methodology
3.1. Research Strategy
3.2. Data and Variables
3.3. Constructs’ Reliability and Consistency
3.4. Sample
4. Findings
5. Discussion
6. Conclusions
Funding
Conflicts of Interest
References
- Borgonovi, E.; Compagni, A. Sustaining Universal Health Coverage: The Interaction of Social, Political, and Economic Sustainability. Value Health 2013, 16, 34–38. [Google Scholar] [CrossRef] [Green Version]
- Podein, R.J.; Hernke, M.T. Integrating Sustainability and Health Care. Prim. Care 2010, 37, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Borgonovi, E.; Adinolfi, P.; Palumbo, R.; Piscopo, G. Framing the Shades of Sustainability in Health Care: Pitfalls and Perspectives from Western EU Countries. Sustainability 2018, 10, 4439. [Google Scholar] [CrossRef] [Green Version]
- Bhatia, V.; Orsini, M. Narrating Sustainability in Canadian Health Care Reform Discourse. Soc. Pol. Adm. 2016, 50, 297–315. [Google Scholar] [CrossRef]
- Harris, C.; Green, S.; Ramsey, W.; Allen, K.; King, R. Sustainability in Health care by allocating resources effectively (SHARE) 1: Introducing a series of papers reporting an investigation of disinvestment in a local healthcare setting. BMC Health Serv. Res. 2017, 17, 323. [Google Scholar] [CrossRef] [PubMed]
- Gruen, R.L.; Elliott, J.H.; Nolan, M.L.; Lawton, P.D.; Parkhill, A.; McLaren, C.J.; Lavis, J.N. Sustainability science: An integrated approach for health-programme planning. Lancet 2008, 372, 1579–1589. [Google Scholar] [CrossRef] [Green Version]
- Pammolli, F.; Riccaboni, M.; Magazzini, L. The sustainability of European health care systems: Beyond income and aging. Eur. J. Health Econ. 2012, 13, 623–634. [Google Scholar] [CrossRef]
- Kaplan, S.B.; Forst, L. Linking Environmental Sustainability, Health, and Safety Data in Health Care: A Research Roadmap. New Solut. 2017, 27, 189–209. [Google Scholar] [CrossRef] [PubMed]
- Garcés, J.; Ródenas, F.; Sanjosé, V. Towards a new welfare state: The social sustainability principle and health care strategies. Health Pol. 2003, 65, 201–215. [Google Scholar] [CrossRef]
- Bethencourt, C.; Galasso, V. Political complements in the welfare state: Health care and social security. J. Public Econ. 2008, 92, 609–632. [Google Scholar] [CrossRef]
- Lyons, G.J.; Duggan, J. System dynamics modelling to support policy analysis for sustainable health care. J. Simul. 2015, 9, 129–139. [Google Scholar] [CrossRef] [Green Version]
- Lega, F.; Prenestini, A.; Spurgeon, P. Is Management Essential to Improving the Performance and Sustainability of Health Care Systems and Organizations? A Systematic Review and a Roadmap for Future Studies. Value Health 2013, 16, 46–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olsen, I.T. Sustainability of Health Care: A Framework for Analysis. Health Policy Plan. 1998, 13, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.E.; Mascarenhas, A.; Bain, J.; Straus, S.E. Developing a comprehensive definition of sustainability. Implement. Sci. 2017, 12, 110. [Google Scholar] [CrossRef]
- Palumbo, R.; Annarumma, C.; Musella, M. Exploring the meaningfulness of healthcare organizations: A multiple case study. Int. J. Public Sect. Manag. 2017, 30, 503–518. [Google Scholar] [CrossRef]
- Mosadeghrad, M.A. Obstacles to TQM success in health care systems. Int. J. Health Care Qual. Assur. 2013, 26, 147–173. [Google Scholar] [CrossRef] [PubMed]
- Mackie, K.S.; Holahan, C.K.; Gottlieb, N.H. Employee Involvement Management Practices, Work Stress, and Depression in Employees of a Human Services Residential Care Facility. Hum. Relat. 2001, 54, 1065–1092. [Google Scholar] [CrossRef]
- Welikala, D.; Sohal, A.S. Total Quality Management and employees’ involvement: A case study of an Australian organisation. Total Qual. Manag. 2008, 19, 627–642. [Google Scholar] [CrossRef]
- Zatzick, C.D.; Iverson, R.D. Putting employee involvement in context: A cross-level model examining job satisfaction and absenteeism in high-involvement work systems. Int. J. Hum. Resour. Manag. 2011, 22, 3462–3476. [Google Scholar] [CrossRef]
- Kossek, E.E.; Valcour, M.; Lirio, P. The sustainable workforce: Organizational strategies for promoting work-life balance and wellbeing. In Wellbeing: A Complete Reference Guide. Work and Wellbeing; Chen, P.Y., Cooper, C.L., Eds.; Wiley Blackwell: Hoboken, NJ, USA, 2014; pp. 295–318. [Google Scholar]
- Mushfiqur, R.; Mordi, C.; Oruh, E.S.; Nwagbara, U.; Mordi, T.; Turner, I.M. The impacts of work-life-balance (WLB) challenges on social sustainability: The experience of Nigerian female medical doctors. Empl. Relat. 2018, 40, 868–888. [Google Scholar] [CrossRef]
- Chu, K.W.K.; Cheung, L.L.W. Incorporating sustainability in small health-care facilities: An integrated model. Leasdersh Health Serv. 2018, 31, 441–451. [Google Scholar] [CrossRef]
- Kalliath, T.; Brough, P. Work–life balance: A review of the meaning of the balance construct. J. Manag. Organ. 2008, 14, 323–327. [Google Scholar] [CrossRef]
- Wood, S. HRM, organizational performance and employee involvement. In Comparative Employment Relations in the Global Economy; Frege, C., Kelly, J., Eds.; Taylor & Francis: London, UK, 2013; pp. 89–107. [Google Scholar]
- Tian, A.W.; Gamble, J. Challenged and satisfied: The role of organisational ownership and employee involvement. Int. J. Hum. Resour. Manag. 2018, 29, 2780–2803. [Google Scholar] [CrossRef] [Green Version]
- Engström, A.K.; Rosengren, K.; Hallberg, L.R.M. Balancing involvement: employees’ experiences of merging hospitals in Sweden. J. Adv. Nurs. 2002, 38, 11–18. [Google Scholar] [CrossRef]
- Lee, E.K.; Hong, W.; Avgar, A.C. Containing conflict: A relational approach to the study of high-involvement work practices in the health-care setting. Int. J. Hum. Resour. Manag. 2015, 26, 100–122. [Google Scholar] [CrossRef]
- Mosadegh, M.R.A.; Yarmohammadian, H.M. A study of relationship between managers’ leadership style and employees’ job satisfaction. Leadersh Health Serv. 2006, 19, 11–28. [Google Scholar]
- Wilkinson, A.; Marchington, M.; Goodman, J.; Ackers, P. Total Quality Management and Employee Involvement. Hum. Resour. Manag. J. 1992, 2, 1–20. [Google Scholar] [CrossRef]
- Riordan, C.M.; Vandenberg, R.J.; Richardson, H.A. Employee involvement climate and organizational effectiveness. Hum. Resour. Manag. 2005, 44, 471–488. [Google Scholar] [CrossRef]
- Wallace, J.C.; Butts, M.M.; Johnson, P.D.; Stevens, F.G.; Smith, M.B. A Multilevel Model of Employee Innovation. J. Manag. 2013, 42, 982–1004. [Google Scholar] [CrossRef] [Green Version]
- Brown, M.; Cregan, C. Organizational change cynicism: The role of employee involvement. Hum. Resour. Manag. 2008, 47, 667–686. [Google Scholar] [CrossRef]
- Cox, A.; Zagelmeyer, S.; Marchington, M. Embedding employee involvement and participation at work. Hum. Resour. Manag. J. 2006, 16, 250–267. [Google Scholar] [CrossRef]
- Wilkinson, A.; Godfrey, G.; Marchington, M. Bouquets, Brickbats and Blinkers: Total Quality Management and Employee Involvement in Practice. Organ. Stud. 1997, 18, 799–819. [Google Scholar] [CrossRef] [Green Version]
- Smith, V. Employee Involvement, Involved Employees: Participative Work Arrangements in a White-Collar Service Occupation. Soc. Probl. 1996, 43, 166–179. [Google Scholar] [CrossRef]
- Wilkinson, A.; Townsend, K.; Burgess, J. Reassessing employee involvement and participation: Atrophy, reinvigoration and patchwork in Australian workplaces. J. Ind. Relat. 2013, 55, 583–600. [Google Scholar] [CrossRef]
- Juravich, T.; Harris, H.; Brooks, A. Mutual gains? labor and management evaluate their employee involvement programs. J. Labor Res. 1993, 14, 165–185. [Google Scholar] [CrossRef]
- Lever-Tracy, C. Fordism Transformed? Employee Involvement and Workplace Industrial Relations at Ford. J. Ind. Relat. 1990, 32, 179–196. [Google Scholar] [CrossRef]
- Juravich, T. Empirical Research on Employee Involvement: A Critical Review for Labor. Lab. Stud. J. 1996, 21, 51–69. [Google Scholar]
- MacKy, K.; Boxall, P. High-involvement work processes, work intensification and employee well-being: A study of New Zealand worker experiences. Asia Pac. J. Hum. Resour. 2008, 46, 38–55. [Google Scholar] [CrossRef]
- Le Fevre, M.; Boxall, P.; Macky, K. Which workers are more vulnerable to work intensification? An analysis of two national surveys. Int. J. Manpow. 2015, 36, 966–983. [Google Scholar] [CrossRef]
- Schoneboom, A. It makes you make the time: ‘Obligatory’ leisure, work intensification and allotment gardening. Ethnography 2018, 19, 360–378. [Google Scholar] [CrossRef]
- Fenton-O’Creevy, M. Employee involvement and the middle manager: Evidence from a survey of organizations. J. Organ. Behav. 1998, 19, 67–84. [Google Scholar] [CrossRef]
- Kaufman, B.E. High-level employee involvement at Delta Air Lines. Hum. Resour. Manag. 2003, 42, 175–190. [Google Scholar] [CrossRef]
- Brad Shuck, M.; Rocco, T.S.; Albornoz, C.A. Exploring employee engagement from the employee perspective: Implications for HRD. J. Eur. Ind. Train. 2011, 35, 300–325. [Google Scholar] [CrossRef]
- Min, M.; Zhu, Y.; Bambacas, M. Implementing HPWS among the indigenous companies in China: Analysing from both managers’ and employees’ perspectives. J. Gen. Manag. 2018, 43, 175–187. [Google Scholar] [CrossRef]
- Sipa, M. The Factors Determining the Creativity of the Human Capital in the Conditions of Sustainable Development. Eur. J. Sustain. Develop. 2018, 7, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Ulhassan, W.M.; Von Thiele Schwarz, U.; Thor, J.; Westerlund, H. Interactions between lean management and the psychosocial work environment in a hospital setting—A multi-method study. BMC Health Serv. Res. 2014, 14, 480. [Google Scholar] [CrossRef] [Green Version]
- Lin, W.B. The exploration of employee involvement model. Expert Syst. Appl. 2006, 31, 69–82. [Google Scholar] [CrossRef]
- Schreurs, B.; Guenter, H.; Schumacher, D.; Van Emmerik, I.H.; Notelaers, G. Pay-Level satisfaction and employee outcomes: The Moderating effect of employee-involvement climate. Hum. Resour. Manag. 2013, 52, 399–421. [Google Scholar] [CrossRef]
- Koene, B.A.S.; Vogelaar, A.L.W.; Soeters, J.L. Leadership effects on organizational climate and financial performance: Local leadership effect in chain organizations. Leadersh Q. 2002, 13, 193–215. [Google Scholar] [CrossRef]
- Gould-Williams, J. HR practices, organizational climate and employee outcomes: Evaluating social exchange relationships in local government. Int. J. Hum. Resour. Manag. 2007, 18, 1627–1647. [Google Scholar] [CrossRef]
- Stavrou, E.; Ierodiakonou, C. Entitlement to Work-Life Balance Support: Employee/Manager Perceptual Discrepancies and Their Effect on Outcomes. Hum. Resour. Manag. 2016, 55, 845–869. [Google Scholar] [CrossRef]
- Gabler, C.B.; Hill, R.P. Abusive supervision, distributive justice, and work-life balance: Perspectives from salespeople and managers. J. Pers. Sell. Sale Manag. 2015, 35, 247–261. [Google Scholar] [CrossRef]
- Grant, C.A.; Wallace, L.M.; Spurgeon, P.C. An exploration of the psychological factors affecting remote e-worker’s job effectiveness, well-being and work-life balance. Empl. Relat. 2013, 35, 527–546. [Google Scholar] [CrossRef]
- Thiruvenkadam, T.; Jayasingh, S. Determinants of employee happiness in an information technology company in India. Int. J. Eng. Technol. 2018, 7, 173–178. [Google Scholar]
- Furnham, A. The People Business: Psychological Reflections on Management; Palgrave MacMillan: London, UK, 2005. [Google Scholar]
- Karatepe, O.M. The effects of work overload and work-family conflict on job embeddedness and job performance: The mediation of emotional exhaustion. Int. J. Contemp. Hosp. Manag. 2013, 25, 614–634. [Google Scholar] [CrossRef]
- Trauth, E.M.; Quesenberry, J.L.; Huang, H. Retaining women in the U.S. IT workforce: Theorizing the influence of organizational factors. Eur. J. Inf. Syst. 2009, 18, 476–497. [Google Scholar] [CrossRef]
- Forstadt, L.; Fortune, A. Personal sustainability: Listening to extension staff and observing organizational culture. J. Ext. 2016, 54, 2RB1. [Google Scholar]
- McCarthy, A.; Cleveland, J.N.; Hunter, S.; Darcy, C.; Grady, G. Employee work–life balance outcomes in Ireland: A multilevel investigation of supervisory support and perceived organizational support. Int. J. Hum. Resour. Manag. 2013, 24, 1257–1276. [Google Scholar] [CrossRef]
- Han, S.J.; McLean, G.N. Effects of family-supportive supervisor behaviors and organizational climate on employees. Eur. J. Train. Dev. 2020, 44, 659–674. [Google Scholar] [CrossRef]
- Yanadori, Y.; Van Jaarsveld, D.D. The Relationships of Informal High Performance Work Practices to Job Satisfaction and Workplace Profitability. Ind. Relat. 2014, 53, 501–534. [Google Scholar] [CrossRef]
- Aragón-Correa, J.A.; Martín-Tapia, I.; Hurtado-Torres, N.E. Proactive Environmental Strategies and Employee Inclusion: The Positive Effects of Information Sharing and Promoting Collaboration and the Influence of Uncertainty. Organ. Environ. 2013, 26, 139–161. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: London, UK, 2018. [Google Scholar]
- Netemeyer, R.G.; Bearden, W.O.; Sharma, S. Scaling Procedures: Issues and Applications; Sage Publications: London, UK, 2003. [Google Scholar]
- Hayton, J.C.; Allen, D.G.; Scarpello, V. Factor Retention Decisions in Exploratory Factor Analysis: A Tutorial on Parallel Analysis. Organ. Res. Methods 2004, 7, 191–205. [Google Scholar] [CrossRef]
- Kaiser, H.F. The application of electronic computers to factor analysis. Educ. Psychol. Meas. 1960, 20, 141–151. [Google Scholar] [CrossRef]
- Harrington, D. Confirmatory Factor Analysis; Oxford University Press: Oxford, UK, 2009. [Google Scholar]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]
- Kloutsiniotis, P.V.; Mihail, D.M. Is it worth it? Linking perceived high-performance work systems and emotional exhaustion: The mediating role of job demands and job resources. Eur. Manag. J. 2020, 38, 565–579. [Google Scholar] [CrossRef]
- Srivastava, A.K.; Chaturvedi, S. Negative Job Experiences and Employees Job Attitudes and Health in High-Performance Work Organizations. Metamorphosis 2014, 13, 22–28. [Google Scholar] [CrossRef]
- Dahl-Jørgensen, C.; Saksvik, P.Ø. The Impact of Two Organizational Interventions on the Health of Service Sector Workers. Int. J. Health Serv. 2005, 35, 529–549. [Google Scholar] [CrossRef]
- Liu, W. High-involvement human resource practices, employee learning and employability. Career Dev. Int. 2018, 23, 312–326. [Google Scholar] [CrossRef]
- Oluwatayo, A.A.; Adetoro, O. Influence of Employee Attributes, Work Context and Human Resource Management Practices on Employee Job Engagement. Glob. J. Flex. Syst. Manag. 2020. [Google Scholar] [CrossRef]
- Shweta, J.; Srirang, J. Determinants of Organizational Citizenship Behaviour: A Review of Literature. J. Manag. Public Pol. 2010, 1, 33–42. [Google Scholar]
- Van Vianen, A.E.M.; De Pater, I.E.; Bechtoldt, M.N.; Evers, A. The strength and quality of climate perceptions. J. Manag. Psychol. 2011, 26, 77–92. [Google Scholar] [CrossRef]
- Brandes, P.; Dharwadkar, R.; Wheatley, K. Social Exchanges Within Organizations and Work Outcomes: The Importance of Local and Global Relationships. Group Organ. Manag. 2004, 29, 276–301. [Google Scholar] [CrossRef]
- Ahmad, I.; Donia, M.B.L.; Khan, A.; Waris, M. Do as I say and do as I do? The mediating role of psychological contract fulfillment in the relationship between ethical leadership and employee extra-role performance. Pers. Rev. 2019, 48, 98–117. [Google Scholar] [CrossRef] [Green Version]
- Baral, R.; Bhargava, S. Work-family enrichment as a mediator between organizational interventions for work-life balance and job outcomes. J. Manag. Psychol. 2010, 25, 274–300. [Google Scholar] [CrossRef]
- Burke, R.J. Organizational culture: A key to the success of work-life integration. In Work-Life Balance: A Psychological Perspective; Jones, F., Burke, R.J., Westman, M., Eds.; Psychology Press: London, UK, 2006; pp. 235–260. [Google Scholar]
- Bertels, S.; Papania, L.; Papania, D. Embedding sustainability in organizational culture. In A Systematic Review of the Body of Knowledge; Ivey Business School, Network for Business Sustainability: London, UK, 2010. [Google Scholar]
- Florea, L.; Cheung, Y.H.; Herndon, N.C. For All Good Reasons: Role of Values in Organizational Sustainability. J. Bus. Ethics. 2013, 114, 393–408. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Variable (ID) | Definition | Illustrative Item | Type of Variable | No. of Items | Scale/Code | CR | α |
|---|---|---|---|---|---|---|---|
| Independent variable | |||||||
| Employees’ Involvement (EI) | Active participation of employees in organizational and managerial dynamics related to their work | You are involved in improving the work organization or work processes of your department or organization? | Continuous | 5 | 1 = lowest level of employees’ involvement 5 = highest level of employees’ involvement | 0.83 | 0.77 |
| Dependent variable | |||||||
| Work–Life Balance (WLB) | Employees’ self-rated ability to handle the work–life interface | How often have you kept worrying about work when you were not working? | Continuous | 5 | 1 = Lowest level of work–life balance 5 = Highest level of work–life balance | 0.82 | 0.75 |
| Mediating variables | |||||||
| Employee–Manager Relationships (EM-R) | Employees’ self-rated quality of relationship with their direct supervisor | Your immediate boss is helpful in getting the job done | Continuous | 6 | 1 = worst level of employee–manager relationships 5 = best level of employee–manager relationships | 0.89 | 0.90 |
| Organizational Climate (OC) | Quality of the social environment hosting the working activities of employees | The work is distributed fairly | Continuous | 6 | 1 = Poorest organizational climate 5 = Richest organizational climate | 0.83 | 0.85 |
| Total Variance Explained | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Components | Eigenvalues | Extraction Sums of Squared Loadings | Rotation Sums of Squared Loadings | ||||||
| Total | % of Variance | Cumulative % | Total | % of Variance | Cumulative % | Total | % of Variance | Cumulative % | |
| 1 | 7074 | 32,157 | 32,157 | 7074 | 32,157 | 32,157 | 4287 | 19,487 | 19,487 |
| 2 | 2494 | 11,336 | 43,493 | 2494 | 11,336 | 43,493 | 3218 | 14,626 | 34,113 |
| 3 | 1972 | 8963 | 52,455 | 1972 | 8963 | 52,455 | 2726 | 12,392 | 46,505 |
| 4 | 1263 | 5742 | 58,197 | 1263 | 5742 | 58,197 | 2572 | 11,692 | 58,197 |
| 5 | 0968 | 4399 | 62,596 | ||||||
| 6 | 0763 | 3469 | 66,064 | ||||||
| 7 | 0687 | 3122 | 69,187 | ||||||
| 8 | 0625 | 2842 | 72,029 | ||||||
| 9 | 0613 | 2787 | 74,816 | ||||||
| 10 | 0564 | 2561 | 77,377 | ||||||
| Rotated Component Matrix | |||||||||
| Components | |||||||||
| 1 | 2 | 3 | 4 | ||||||
| EI_1 | 0.105 | 0.037 | 0.707 | 0.036 | |||||
| EI_2 | 0.079 | 0.143 | 0.762 | 0.014 | |||||
| EI_3 | 0.190 | 0.150 | 0.697 | 0.050 | |||||
| EI_4 | 0.134 | 0.089 | 0.753 | 0.010 | |||||
| EI_5 | 0.089 | 0.062 | 0.591 | −0.074 | |||||
| EM-R_1 | 0.609 | 0.335 | 0.141 | 0.118 | |||||
| EM-R_2 | 0.790 | 0.167 | 0.206 | 0.074 | |||||
| EM-R_3 | 0.775 | 0.350 | 0.073 | 0.087 | |||||
| EM-R_4 | 0.753 | 0.194 | 0.097 | 0.055 | |||||
| EM-R_5 | 0.825 | 0.216 | 0.122 | 0.043 | |||||
| EM-R_6 | 0.823 | 0.202 | 0.195 | 0.044 | |||||
| OC_1 | 0.492 | 0.558 | 0.168 | 0.106 | |||||
| OC_2 | 0.202 | 0.721 | 0.089 | 0.084 | |||||
| OC_3 | 0.341 | 0.704 | 0.141 | 0.125 | |||||
| OC_4 | 0.238 | 0.722 | 0.082 | 0.147 | |||||
| OC_5 | 0.097 | 0.643 | 0.144 | 0.138 | |||||
| OC_6 | 0.397 | 0.680 | 0.050 | 0.083 | |||||
| WLB_1 | 0.196 | 0.099 | −0.143 | 0.604 | |||||
| WLB_2 | 0.096 | 0.092 | 0.079 | 0.670 | |||||
| WLB_3 | 0.103 | 0.126 | 0.030 | 0.749 | |||||
| WLB_4 | 0.005 | 0.114 | 0.033 | 0.744 | |||||
| WLB_5 | −0.072 | 0.057 | −0.002 | 0.720 | |||||
| Variable | Total | |
|---|---|---|
| No. | % | |
| Gender | ||
| Men | 363 | 18.8 |
| Women | 1564 | 81.1 |
| Do not know/Did not answer | 1 | 0.1 |
| Geographical area | ||
| Northern Europe | 433 | 22.5 |
| Western Europe | 547 | 28.4 |
| Southern Europe | 585 | 30.3 |
| Eastern Europe | 363 | 18.8 |
| Age group | ||
| 24 years and below | 76 | 3.9 |
| Between 25 and 34 years | 463 | 24 |
| Between 35 and 44 years | 490 | 25.4 |
| Between 35 and 54 years | 548 | 28.4 |
| Between 55 and 64 years | 325 | 16.9 |
| 65 years and above | 25 | 1.3 |
| Do not know/Did not answer | 1 | 0.1 |
| Country of birth | ||
| Some country of residence | 1673 | 86.8 |
| Foreign country | 247 | 12.8 |
| Do not know/Did not answer | 8 | 0.4 |
| Education (ISCED) | ||
| Lower secondary education | 56 | 2.9 |
| Upper secondary education | 508 | 26.3 |
| Post-secondary education | 187 | 9.7 |
| Short-cycle tertiary education | 379 | 19.7 |
| Bachelor or equivalent | 463 | 24 |
| Master or equivalent | 273 | 14.2 |
| Doctorate or equivalent | 62 | 3.2 |
| Sector | ||
| Public sector | 1281 | 66.4 |
| Private sector | 640 | 33.2 |
| Other | 7 | 0.4 |
| Type of contract | ||
| Unlimited duration contract | 1668 | 10.1 |
| Limited duration contract | 195 | 86.5 |
| Do not know/Did not answer | 65 | 3.4 |
| Part-time/Full-time | ||
| Full-time contract | 1466 | 76 |
| Part-time contract | 461 | 23.9 |
| Do not know/Did not answer | 1 | 0.1 |
| Organizational age | ||
| 1 year and below | 218 | 11.3 |
| Between 2 and 5 years | 442 | 23.9 |
| Between 6 and 10 years | 403 | 20.9 |
| Between 11 and 20 years | 466 | 24.2 |
| 21 years and above | 386 | 20 |
| Do not know/Did not answer | 13 | 0.7 |
| Organizational dimension (per employees’ number) | ||
| 9 employees or below | 288 | 14.9 |
| Between 10 and 249 employees | 671 | 34.8 |
| 250 employees and above | 922 | 47.8 |
| Do not know/Did not answer | 47 | 2.5 |
| Outcome Variable: EM-R | ||||||
|---|---|---|---|---|---|---|
| Model summary | ||||||
| R | R2 | MSE | F | df1 | df2 | p |
| 0.3537 | 0.1251 | 0.7297 | 230. | 1 | 1614 | 0.0000 |
| Model | ||||||
| Coeff. | SE | t | p | LLCI | ULCI | |
| Constant | 28,234 | 0.0762 | 37.0287 | 0.0000 | 2.6738 | 2.9730 |
| EI | 0.3587 *** | 0.0236 | 15.1915 | 0.0000 | 0.3124 | 0.4051 |
| Outcome variable: OC | ||||||
| Model summary | ||||||
| R | R2 | MSE | F | df1 | df2 | p |
| 0.6699 | 0.4487 | 0.3095 | 656.4999 | 2 | 1613 | 0.000 |
| Model | ||||||
| Coeff. | SE | t | p | LLCI | ULCI | |
| Constant | 1.6797 | 0.0675 | 24.8702 | 0.0000 | 1.5472 | 1.8122 |
| EI | 0.0916 *** | 0.0164 | 5.5689 | 0.0000 | 0.0593 | 0.1238 |
| EM-R | 0.5110 *** | 0.0162 | 31.5208 | 0.0000 | 0.4792 | 0.5428 |
| Outcome variable: WLB | ||||||
| Model summary | ||||||
| R | R2 | MSE | F | df1 | df2 | p |
| 0.3181 | 0.1012 | 0.4581 | 60.486 | 3 | 1612 | 0.000 |
| Model | ||||||
| Coeff. | SE | T | p | LLCI | ULCI | |
| Constant | 2.6576 | 0.0966 | 27.4983 | 0.0000 | 2.4680 | 2.8472 |
| EI | −0.0514 * | 0.0202 | −2.5462 | 0.0110 | −0.091 | −0.0118 |
| EM-R | 0.0152 | 0.0251 | 0.6054 | 0.5450 | −0.0340 | 0.0644 |
| OC | 0.3057 *** | 0.0303 | 10.0907 | 0.0000 | 0.2463 | 0.3651 |
| DIRECT AND INDIRECT EFFECTS OF WH ON WLB | ||||||
| Direct effect of EI on WLB | ||||||
| Effect | SE | t | p | LLCI | ULCI | |
| −0.0514 * | 0.0202 | −2.5462 | 0.0110 | −0.0910 | −0.0118 | |
| Indirect effect of EI on WLB | ||||||
| Effect | Boot SE | Boot LLCI | Boot ULCI | |||
| Total | 0.0895 * | 0.0103 | 0.0705 | 0.1102 | ||
| EI-->EM-R-->WLB | 0.0054 | 0.0099 | −0.0167 | 0.0248 | ||
| EI-->OC-->WLB | 0.0280 * | 0.0063 | 0.0167 | 0.0411 | ||
| EI-->EM-R-->OC-->WLB | 0.0560 * | 0.0074 | 0.0423 | 0.0717 | ||
| Outcome Variable: EM-R | ||||||
|---|---|---|---|---|---|---|
| Model summary | ||||||
| R | R2 | MSE | F | df1 | df2 | p |
| 0.3977 | 0.1582 | 0.7071 | 25.5383 | 11 | 1495 | 0.0000 |
| Model | ||||||
| Coeff. | SE | t | p | LLCI | ULCI | |
| Constant | 3.0852 | 0.1152 | 26.7883 | 0.0000 | 2.8593 | 3.3111 |
| EI | 0.3696 *** | 0.0246 | 15.0347 | 0.0000 | 0.3214 | 0.4179 |
| Gender (1 = Male) | −0.0881 | 0.0595 | −1.4798 | 0.1391 | −0.2048 | 0.0287 |
| Education | −0.0532 | 0.0490 | −1.0859 | 0.2777 | −0.1492 | 0.0429 |
| Sector Type (1 = Private) | 0.1024 * | 0.0503 | 2.0349 | 0.0420 | 0.0037 | 0.2011 |
| Type of contract (1 = Unlimited) | −0.1257 | 0.0753 | −1.6693 | 0.0953 | −0.2733 | 0.0220 |
| Part-time employment | −0.1292 * | 0.0527 | −2.4529 | 0.0143 | −0.2325 | −0.0259 |
| Organizational age | −0.0062 ** | 0.0022 | −2.7556 | 0.0059 | −0.0106 | −0.0018 |
| Working at night | 0.1171 | 0.0610 | 1.9188 | 0.0552 | −0.0026 | 0.2368 |
| Working on Sundays | −0.1644 * | 0.0743 | −2.2110 | 0.0272 | −0.3102 | −0.0185 |
| Working on Saturdays | 0.0786 | 0.0684 | 1.1480 | 0.2512 | −0.0577 | 0.2128 |
| Less than 11 h between 2 working days | −0.1881 *** | 0.0497 | −3.7879 | 0.0002 | −0.2856 | −0.0907 |
| Outcome variable: OC | ||||||
| Model summary | ||||||
| R | R2 | MSE | F | df1 | df2 | p |
| 0.6843 | 0.4682 | 0.3013 | 109.6099 | 12 | 1494 | 0.000 |
| Model | ||||||
| Coeff. | SE | t | p | LLCI | ULCI | |
| Constant | 1.8350 | 0.0915 | 20.0624 | 0.0000 | 1.6556 | 2.0144 |
| EI | 0.1008 *** | 0.0172 | 5.8529 | 0.0000 | 0.0670 | 0.1346 |
| EM-R | 0.4903 *** | 0.0169 | 29.0411 | 0.0000 | 0.4572 | 0.5234 |
| Gender (1 = Male) | −0.0041 | 0.0389 | −0.1062 | 0.9154 | −0.0804 | 0.0721 |
| Education | −0.1056 *** | 0.0320 | −3.3037 | 0.0010 | −0.1683 | −0.0429 |
| Sector Type (1 = Private) | 0.1349 *** | 0.0329 | 4.1023 | 0.0000 | 0.0704 | 0.1994 |
| Type of contract (1 = Unlimited) | −0.0049 | 0.0492 | −0.1002 | 0.9202 | −0.1014 | 0.0916 |
| Part-time employment | 0.0211 | 0.0344 | 0.6139 | 0.5394 | −0.0464 | 0.0887 |
| Organizational age | 0.0003 | 0.0015 | 0.2270 | 0.8205 | −0.20025 | 0.0032 |
| Working at night | −0.0070 | 0.0399 | −0.1754 | 0.8608 | −0.0852 | 0.0712 |
| Working on Sundays | −0.0697 | 0.0486 | −1.4336 | 0.1519 | −0.1650 | 0.0257 |
| Working on Saturdays | 0.0090 | 0.0447 | 0.2004 | 0.8412 | −0.0787 | 0.0966 |
| Less than 11 h between 2 working days | −0.1110 *** | 0.0326 | −3.4059 | 0.0007 | −0.1749 | −0.0471 |
| Outcome variable: WLB | ||||||
| Model summary | ||||||
| R | R2 | MSE | F | df1 | df2 | p |
| 0.3932 | 0.1546 | 0.4273 | 21.0047 | 13 | 1493 | 0.000 |
| Model | ||||||
| Coeff. | SE | T | p | LLCI | ULCI | |
| Constant | 2.7582 | 0.1227 | 22.4761 | 0.0000 | 2.5175 | 2.999 |
| EI | −0.0416 * | 0.0207 | −2.0039 | 0.0453 | −0.0822 | −0.0009 |
| EM-R | 0.0308 | 0.0251 | 1.2255 | 0.2206 | −0.0185 | 0.0801 |
| OC | 0.2680 *** | 0.0308 | 8.6988 | 0.0000 | 0.2076 | 0.3284 |
| Gender (1 = Male) | 0.2142 *** | 0.0463 | 4.6254 | 0.0000 | 0.1233 | 0.3050 |
| Education | 0.0986 *** | 0.0382 | −2.5814 | 0.0099 | −0.1736 | −0.0237 |
| Sector Type (1 = Private) | −0.0452 | 0.0394 | −1.1477 | 0.2513 | −0.1736 | −0.0237 |
| Type of contract (1 = Unlimited) | 0.1090 | 0.0586 | 1.8599 | 0.0631 | −0.0060 | 0.2239 |
| Part-time employment | 0.0940 * | 0.0410 | 2.2909 | 0.0221 | 0.0135 | 0.1745 |
| Organizational age | 0.0030 | 0.0017 | 1.7320 | 0.0835 | −0.0004 | 0.0065 |
| Working at night | −0.0166 | 0.0475 | −0.3505 | 0.7260 | −0.1098 | 0.0765 |
| Working on Sundays | −0.0494 | 0.0579 | −0.8524 | 0.3941 | −0.1630 | 0.0643 |
| Working on Saturdays | −0.0791 | 0.0532 | −1.4852 | 0.1377 | −0.1835 | 0.0254 |
| Less than 11 h between 2 working days | −0.1714 *** | 0.0389 | −4.4018 | 0.0000 | −0.2478 | −0.0950 |
| Direct and Indirect Effects of WH on WLB | ||||||
| Direct effect of EI on WLB | ||||||
| Effect | SE | t | p | LLCI | ULCI | |
| −0.0416 * | 0.0207 | −2.0039 | 0.0453 | −0.0822 | −0.0009 | |
| Indirect effect of EI on WLB | ||||||
| Effect | Boot SE | Boot LLCI | Boot ULCI | |||
| Total | 0.0870 * | 0.0103 | 0.0675 | 0.1076 | ||
| EI-->EM-R-->WLB | 0.0144 | 0.0100 | −0.0085 | 0.0303 | ||
| EI-->OC-->WLB | 0.0270 * | 0.0059 | 0.0164 | 0.0392 | ||
| EI-->EM-R-->OC-->WLB | 0.0486 * | 0.0073 | 0.0353 | 0.0636 | ||
| # Hypothesis | Contents | Result |
|---|---|---|
| H1 | Employees’ involvement may have some negative effects on the workforce’s ability to handle the work–life interface, due to increased occurrence of work intensification | Supported |
| H2 | Employees’ involvement enhances the employee–manager relationships, boosting the establishment of positive exchanges | Supported |
| H3 | Employees’ involvement contributes to the amelioration of the organizational climate, sustaining a sense of fairness, trust, and collaboration in the workplace | Supported |
| H4 | Better employee–manager relationships foster an improvement of the organizational climate, paving the way for an aggregating working environment | Supported |
| H5 | Better employee–manager relationships contributes to the improvement of the employees’ perception about their ability to manage the work–life interplay | Not supported |
| H6 | Positive organizational climate sustains the employees’ perception of work–life balance | Supported |
| H7 | Employee–manager relationships mediate the implications of employees’ involvement on work–life balance, so that the employees’ perceptions of managing the work–life interplay are better | Not supported |
| H8 | A positive organizational climate mediates the implications of employees’ involvement on work–life balance, so that the employees’ perceptions of managing the work–life interplay are better | Supported |
| H9 | Employee–manager relationships and organizational climate serially mediate the implications of employees’ involvement on work–life balance, so that the employees’ perceptions of managing the work–life interplay are better | Supported |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palumbo, R. Improving Health Professionals’ Involvement Whilst Sustaining Work–Life Balance: Evidence from an Empirical Analysis. Sustainability 2020, 12, 9291. https://doi.org/10.3390/su12219291
Palumbo R. Improving Health Professionals’ Involvement Whilst Sustaining Work–Life Balance: Evidence from an Empirical Analysis. Sustainability. 2020; 12(21):9291. https://doi.org/10.3390/su12219291
Chicago/Turabian StylePalumbo, Rocco. 2020. "Improving Health Professionals’ Involvement Whilst Sustaining Work–Life Balance: Evidence from an Empirical Analysis" Sustainability 12, no. 21: 9291. https://doi.org/10.3390/su12219291