Abstract
Calcium deficiency during child growth leads to osteoporosis in later stages of life. Finger millet is one of the calcium dense foods, with three times the level of calcium than milk, and the only cereal that contains high calcium content which is consistent across different varieties (364 ± 58 mg/100 g). Thus, finger millet has potential for addressing calcium deficiency naturally. This study aimed to determine the retention and impact of finger millet calcium on bone turnover through a systematic review and meta-analysis. Three human studies were eligible for systematic review. Of these, only two were eligible for meta-analysis to assess the retention of calcium in children of 9 to 12 years. One study on bone turnover markers was not used in the meta-analysis as at least two studies are required to conduct meta-analysis. Due to the lack of complete data only four studies were eligible for meta-analysis to assess the in vitro bioavailability of calcium from unprocessed and a range of different types of processed finger millet. The result shows that there was significant retention (p < 0.05) of 23.4 ± 2.9% calcium from finger-millet-based diet which could help bone accretion during child growth if finger-millet-based diet is consumed. The bone turnover marker study shows that the resorption of calcium reduced by 28% and 47% among peri and post-menopausal women respectively after feeding the nutria mixed grain ball. However, there is no significant change in bone formation marker. Depending on the type of processing, calcium bioavailability either increased or decreased. One in vitro study showed that calcium bioavailability from finger millet was 28.6% when boiled, whereas three studies on processing show that certain processing can double the calcium bioavailability to 61.4%. Irrespective of the type of processing, finger millets contribute to high calcium retention and extremely high bioavailable calcium and could be useful for healthy growth and in dealing with complications related to calcium deficiency.
1. Introduction
Calcium is critical for the growth of babies through to adolescents. At an older age, osteoporosis is a serious public health issue and worldwide, its prevalence has increased substantially in recent times and is predicted to continue to rising in the future such that by 2040 subjects with a high fracture risk will be double that of 2010 [1]. Osteoporosis is mainly caused by a deficiency in dietary calcium as well as vitamin D which assists in the absorption of calcium. Several options have been applied to resolve these deficiencies including use of calcium and vitamin D supplements or fortification in food [2]. A safe and sustainable diet-based solution to combat calcium and vitamin D deficiency should start from early childhood, which can be achieved by consuming foods naturally rich in calcium while ensuring sufficient vitamin D status from the sunlight, food, and/or supplementation.
Plant-based calcium such as that found in traditional staple grains is important for diets in many countries. It is noteworthy that finger millet has been shown to be consistently high in calcium regardless of the variety (364 ± 58 mg/100 g) and is balanced with other minerals such as zinc and magnesium [3]. It is likely that this will be beneficial for strengthening bones during a child’s growth stage especially during adolescence, when most bone calcium accretion occurs and is crucial for the attainment of high peak bone mass which in turn is important for preventing osteoporosis and bone fractures in later life [4,5]. A common way to prevent or treat calcium deficiency is through supplemental calcium tablets or artificially fortified food. However, these tablets and fortification typically contain inorganic calcium compounds such as calcium carbonate, calcium citrate, and calcium phosphate, [6] which may be of modest bioavailability and can have undesirable effects such as kidney stone formation, constipation, bloating, and flatulence [7]. Calcium from most plant sources, on the other hand, is naturally balanced with other minerals and hence can be a safer option [7,8]. It is well recognized that calcium-fortified food and calcium supplements serve as a “supplement to” and not a “substitute for” natural dietary calcium [7].
While milk and milk products are popular dietary options in programs and campaigns to tackle calcium deficiency, finger millet also has great potential for such a role in terms of both calcium content and affordability in the countries where it is grown. Millets are recognized as smart food [9] for being “good for you” (healthy and nutritious), “good for the planet” (e.g., survives with less water and lower carbon footprint), and “good for the farmer” (e.g., climate resilient). Millets contain calcium, iron, zinc, selenium, magnesium, fiber, protein, and other nutrients which are several times higher than milled rice and refined wheat [3]. Previous systematic review and meta-analyses conducted on millets, showed millet-based diets (including finger millet) help manage blood glucose concentration and reduce the risk of developing type 2 diabetes [10], help manage blood lipid profile, obesity, hypertension thereby reducing the risk of developing cardiovascular diseases [11], and help improve hemoglobin level thereby reducing the risk of iron deficiency anemia [12]. In particular, finger millet was reported to contain 364 mg calcium/100 g according to studies conducted in India [3], which is exceptionally high. Even when varieties from various countries are considered, the calcium content is reportedly higher (364 ± 58 mg/100 g) than other commonly known high-calcium food like milk which has one-third the level of calcium as finger millet. Although milk-based products such as paneer (476 ± 35.7 mg/100 g), an Indian cottage cheese or cheddar cheese (740 mg/100 g) are rich in calcium, their consumption preferences depend on income elasticity and almost nil is consumed by those of low income group [13]. Moreover, in countries where finger millet is a traditional food or regularly produced, like India and East and Southern Africa, finger millet is more affordable than dairy products. High cost is again one of the reasons why milk intake is low among young children and pregnant women from underprivileged socioeconomic segments in India [14] compared to the rich social segments, despite the country being among the largest producers of milk globally. Other calcium-rich sources such as sesame seed and almond are more expensive than finger millet, in India in particular. Needless to say, almond and sesame seed cannot be eaten in a quantity large enough to provide the equivalent amount of calcium. On the other hand, finger millet, being a traditional staple food, can occupy a major portion of the diet, thereby contributing substantially to nutrient intake. Additionally, if finger millet is incorporated as a staple, this could lead to market and economic growth along with improved nutrition security. With such a high calcium content finger millet has the potential to reduce the calcium-related health issues such as osteoporosis if consumed adequately and regularly and an excellent sustainable dietary option for developing countries which is not yet fully explored. Despite millets having high nutrient content and proven health benefits, it has been known for quite some time that millets contain phytates, phenols, and tannins which can substantially reduce nutrient bioavailability [15]. Therefore, it is important to have science-backed information on the impact of consuming finger millets on calcium levels.
This systematic review and meta-analysis was conducted with the aim to collate the available evidence on calcium retention or accretion upon consuming finger-millet-based diet and/or its bioavailability from finger millet together with the effects of various processing methods on the calcium bioavailability.
Research Questions
Does consumption of finger-millet-based meals contribute to better calcium retention, calcium resorption, and/or bioavailability compared to other non-millet-based regular diets? Do different forms of cooking and processing of finger millet affect calcium bioavailability?
2. Materials and Methods
2.1. Study Period
A systematic review and meta-analysis was conducted from October 2017 to February 2021 and was registered in the online platform called “research registry” with the unique registration number of reviewregistry 1136. A 27-item PRISMA checklist was used for conducting the systematic review and meta-analysis [16].
2.2. Information Sources
Studies that were published in the English language were considered. The study included the articles from the period of 1950 to the first quarter of 2021. The search engines Google Scholar, Scopus, Web of Science, PubMed, and CAB Abstract were used for finding the studies that were relevant to the research questions as per the search strategy and keywords given in Table 1. The search was conducted using the search strategy and key words and articles found were further screened for their relevance, completeness in information, and quality of the research based on the inclusion and exclusion criteria. If the abstract was suitable, then efforts were made to download open access articles or collect full papers from the library. All the relevant papers downloaded were further checked for relevance and papers were only used if they addressed the research questions. After obtaining the full papers, if any further detail was required, the authors were contacted and additional information was obtained for use in the meta-analysis. Furthermore, a manual search was undertaken with articles in the reference lists of downloaded articles to find additional research articles.

Table 1.
Search criteria and keywords.
2.3. Inclusion Criteria
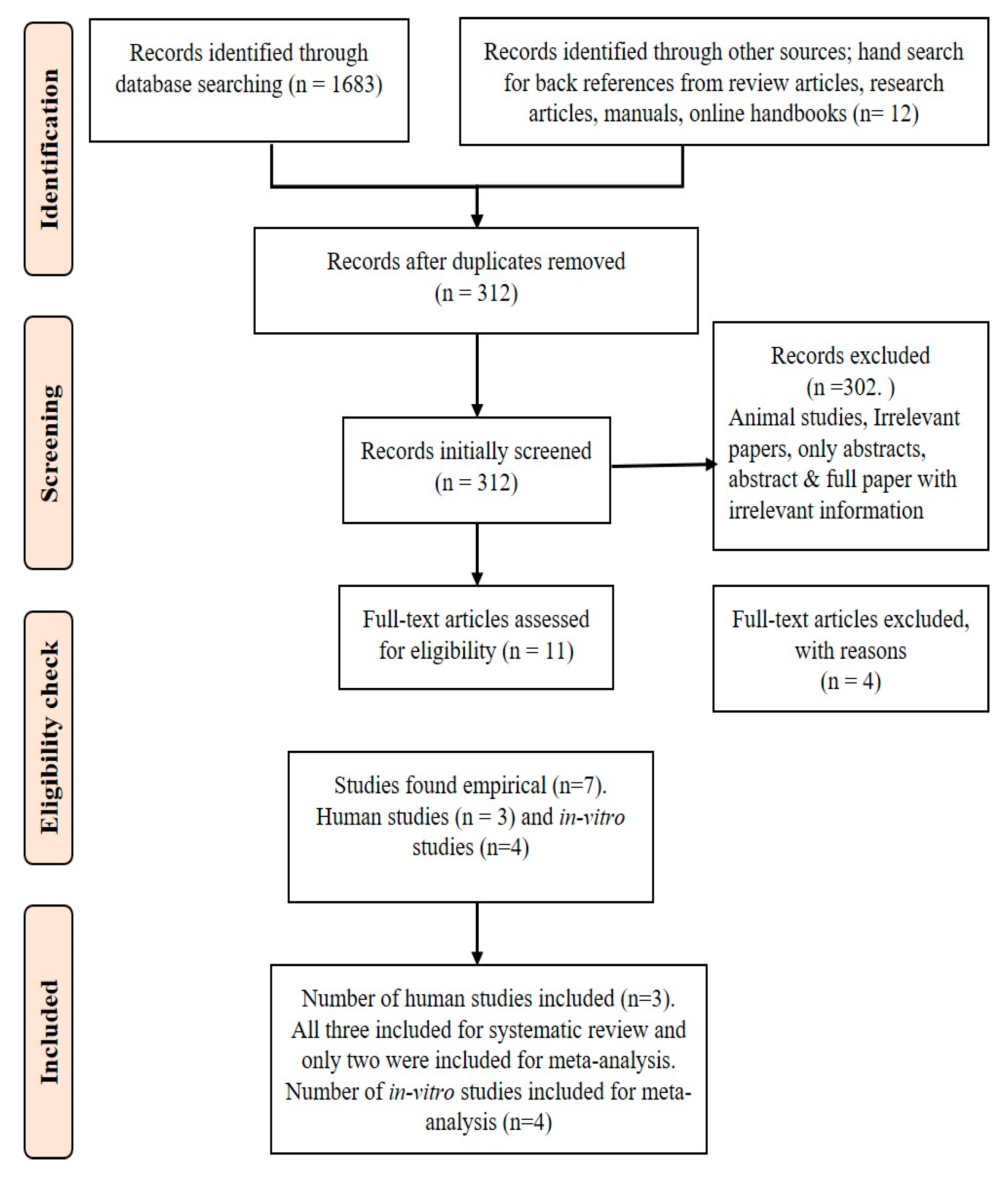
The PRISMA flow diagram (Figure 1) shows the steps involved in the inclusion of the studies: 1. Randomized controlled trials, non-randomized observational or cohort studies to measure the calcium bioavailability, retention, and/or bone resorption markers by feeding finger millet were included. 2. In vitro laboratory studies on calcium bioavailability were included; but, treated independently. 3. Studies to assess the effect of any type of cooking or processing of finger millet such as fermentation, germination, and/or malting on calcium bioavailability were included. 4. Only peer reviewed journal articles were included. 5. Regardless of the time period all the articles published in this area were included. 6. Articles that had complete data required for meta-analysis were included for meta-analysis. 7. Metabolic studies to determine calcium retention by feeding finger-millet-based diet were included.
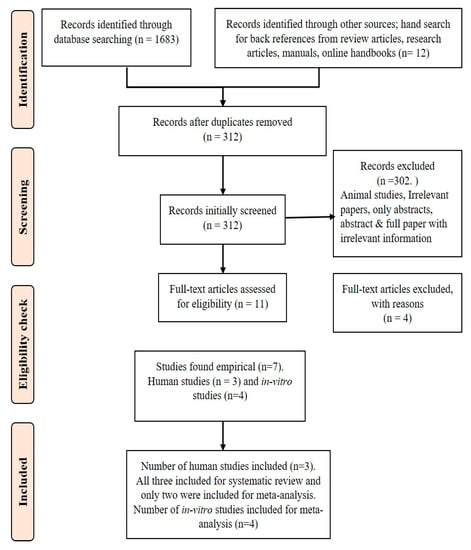
Figure 1.
PRISMA flow diagram of systematic review.
2.4. Exclusion Criteria
1. Review articles were excluded. 2. Animal studies were excluded. 3. If the data were found incomplete, the authors were contacted. If complete data were still not accessible, then the articles were excluded. 4. Although several articles (312) were obtained during the first screening, only 7 qualified articles were included, other articles which looked related but had information only on nutrient composition of finger millet were rejected.
2.5. Data Extraction
Each study was labelled with author details and year. The data were then entered by two investigators into an Excel spreadsheet as per the guidelines provided in Harrer et al. (2019) [17]. Mean and standard deviation (SD) for calcium retention in children was extracted in mg. If the standard error was recorded, it was converted to standard deviation (SD) to maintain the uniformity in unit. In addition, descriptive statistics were used to calculate the simple statistical differences within each outcome parameter.
2.6. Bias Assessment
A funnel plot was used to assess the publication bias and other biases such as selection bias, detection bias, attrition bias, and reporting bias using the guidelines provided in the Cochrane online handbook for systematic reviews of interventions [18,19,20].
2.7. Study Quality Assessment
Using the 8-item Newcastle-Ottawa Scale (NOS) which is generally applied to non-randomized trials, the quality [21,22] of each study was assessed by two investigators, and any disagreements were resolved by discussing it with a third reviewer. The researchers also applied the principle of Bell et al. (2019) [23] to further strengthen the quality assessment.
2.8. Summary Measures and Result Synthesis
The continuous data on calcium retention from finger-millet-based diets after the intervention were recorded against the control rice-based diet as mean calcium retention and subjected to meta-analysis to measure the standardized mean difference (SMD) and heterogeneity (I2). The overall effect of consuming finger-millet-based diets and significance of the outcomes such as calcium retention, in vitro bioavailability and effect of processing on in vitro bioavailability was determined using a fixed effect model or random effect model depending on the heterogeneity among study [24]. The results of the effect on in vitro bioavailability were interpreted using a random effect model [25]. Meta-analysis was conducted using the software R Studio version 4.0.4 (2021) to obtain forest plots along with heterogeneity (I2) and the overall test effect in both fixed and random effect models and funnel plots to assess the publication bias [17,26,27].
3. Results
Among the 1695 records identified through the database and other sources, only 312 were screened after removing duplicate articles. From these 312 articles, 302 irrelevant articles were removed including articles that had information on nutritional composition of millets but not bioavailable calcium or bioavailability percentage, studies conducted on animals and review articles. There were only three human studies available, two on calcium retention in children and the other on bone resorption markers in menopausal women. Table 2 contains details on study characteristics considered for systematic review and/or meta-analysis.
Table 2.
Study characteristics included for systematic review and meta-analysis.
3.1. Meta-Analysis on Calcium Retention in Children
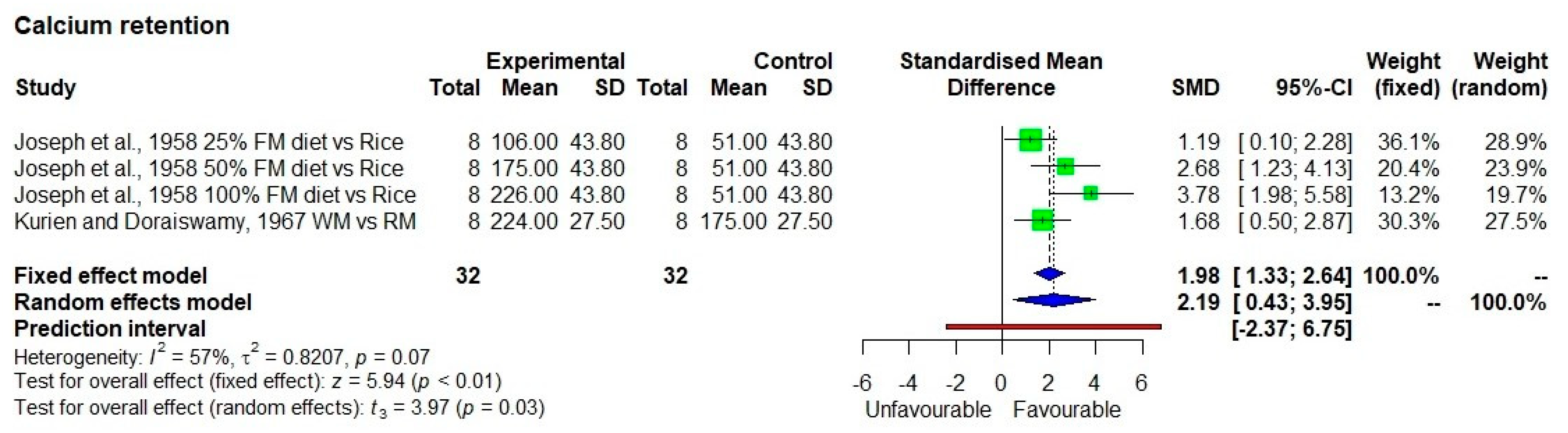
Calcium retention in children was significantly high from finger-millet-based diet (p < 0.05) compared to rice-based diet or refined finger-millet-based diet with moderate heterogeneity (I2 = 57%) among studies with standardized mean difference (SMD) of 2.19 and 95% confidence interval of 0.43; 3.95 (Figure 2). The sample size was 32 and average calcium retention was 23.4 ± 2.9% from finger-millet-based diet. The predication interval lies between −2.37 and 6.75 shows the slight possibility of non-significant results, indicating a need for more studies with high sample numbers.
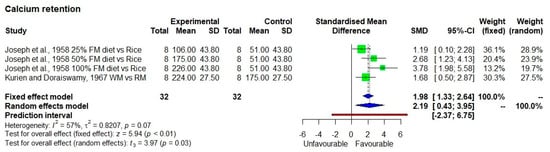
Figure 2.
Calcium retention from finger-millet-based diet. Abbreviations: FM, finger millet; WM, whole millet; RM, refined millet.
Among the two studies by Josheph et al. (1959) [28], four treatments were conducted by providing rice-based meals substituted with 25% (471 mg calcium/70 g finger millet), 50% (693 mg calcium/140 g finger millet), and 100% finger millet (1151 mg calcium/280 g finger millet) for 15 days, to 8 children of 9 to 10 years old. For the control group, 280 g of rice (258 mg calcium) was supplied for 15 days to 8 children of 9 to 10 years of age. The results show calcium retention of 19.7% (51 mg calcium) for the rice diet, 22% (106 mg calcium) for the 25% finger millet diet, 25% (175 mg calcium) for the 50% finger millet diet, and 19.6% (226 mg calcium) for the 100% finger millet diet. Although the percentage calcium retention was similar in all four treatments the calcium retention was 4.4 times higher from the 100% finger millet diet compared to 100% rice-based diet, because finger millet provided more dietary calcium.
Similarly, the study conducted by Kurien and Doraiswamy (1967) [29] fed 156 g of whole finger-millet-based diet with calcium content of 854 mg to the group of 8 children and 156 g of refined finger millet diet with calcium content of 692 mg to another group of 8 children to study the calcium retention shows that the calcium retention was 26% and 25% from whole and refined finger millet respectively. Simply because whole finger millet contains more calcium the retention was more (224 mg/854 mg calcium) compared to refined finger millet (175 mg/692 mg calcium).
3.2. Markers of Bone Resorption in Menopausal Women
Gayathri and Hemamalini (2020) [30] studied two observations (finger millet vs. non-finger millet diet; pre- vs. post-treatment) on a marker of calcium resorption from bone (Beta Crosslaps (beta-CTX)). Beta-CTX is released into the bloodstream during bone resorption and serves as a marker for increased bone resorption. This is the only study conducted in this area and therefore not included in the meta-analysis. Fifteen post-menopausal and 15 peri-menopausal women were involved in the intervention, showed a significant (p < 0.05) reduction in beta-CTX after consuming 180 g and 120 g of nutria ball (made of finger millet, sesame, black gram and green leafy vegetable), respectively, as mid-morning and evening snacks for six months. Two control groups of 15 each did not consume any nutria balls. For the post-menopausal women, the beta-CTX reduced from 1.10 ± 0.29 to 0.53 ± 0.25 ng/mL, a 47% reduction, while for the peri-menopausal women, it reduced from 0.32 ± 0.13 to 0.25 ± 0.13 mg/mL, a 28% reduction. There was no change in the bone formation marker (P1NP) in either the treatment or control groups of post and peri-menopausal women.
3.3. Meta-Analysis of In Vitro Studies on the Effect of Cooking and Processing on Calcium Bioavailability
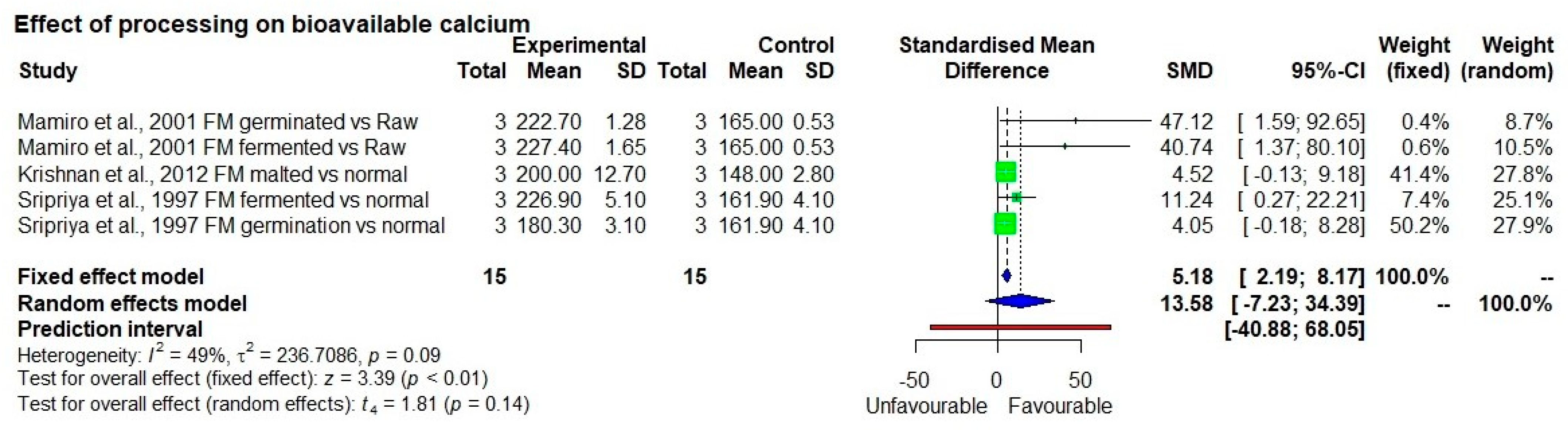
Among the eight studies identified, four studies were rejected as data were incomplete. Of the four eligible studies on calcium in vitro bioavailability, one study was on cooking [31], and three studies [32,33,34] were on other different processing methods such as germination, fermentation and soaking which were used for the meta-analysis. Albeit not shown in forest plot, nine observations from three studies on various methods of processing were included such as soaking, germination, fermentation, decortication, malting, expansion/extrusion/puffing (thermal process to increase size, shape, and volume), and popping. When all 9 observations were analyzed together, there was no significant change in calcium bioavailability as a result of processing (p = 0.15 and 0.38 in the fixed and random effect models, respectively). On the other hand, when the different types of processing methods were analyzed separately, decortication, popping, and extrusion processes led to a decrease in bioavailability of calcium. Five observations on germination, fermentation, and malting showed a significant increase (12.5 to 38.9%) in bioavailable calcium content (p < 0.01) (Figure 3) with low heterogeneity among studies (I2 = 49%) and SMD of 5.18 and 95% confidence interval of 2.19; 8.17 in fixed effect model. These forms of processing are commonly undertaken at the household level in rural Asia, Africa, and in some urban homes in these continents. It is noted that the bioavailable calcium content was high for finger millet compared to other staples (Figure 4).
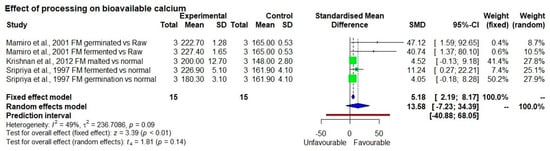
Figure 3.
Effect of traditional household processing on bioavailable calcium compared to raw grain.
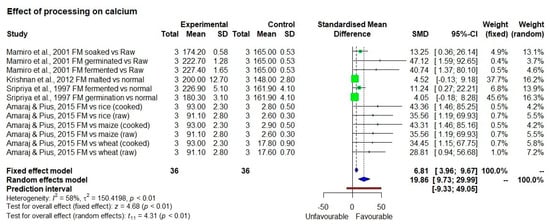
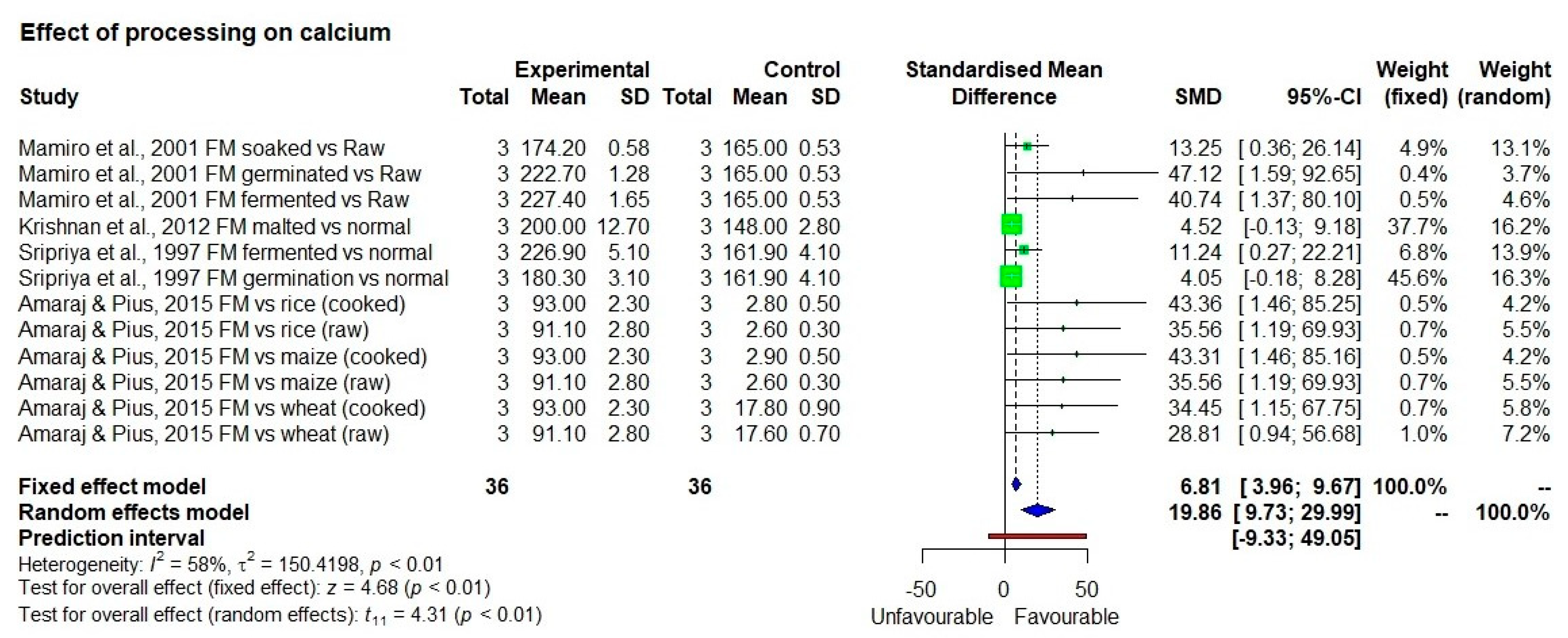
Figure 4.
Bioavailable calcium from processed and cooked finger millet compared to raw and other staples.
The percentage bioavailability of calcium from finger millet, pearl millet, sorghum, maize, rice, and wheat which was cooked in microwave with water 28.6%, 30.3%, 26.5%, 27.4%, 26.5%, and 34.8% respectively with no significant differences between them. The mean in vitro bioavailable calcium content of finger millet was 93.0 ± 1.3 mg/100 g, while it was 13.0 ± 0.8, 7.1 ± 0.3, 17.8 ± 0.5, 2.9 ± 0.3, and 2.8 ± 0.3 mg/100 g for pearl millet, sorghum, wheat, maize, and rice respectively [27]. Nonetheless, bioavailable calcium content was 7.2, 13.0, 5.2, 32.0, and 33.0 times more in finger millet than in pearl millet, sorghum, wheat, maize, and rice respectively. The calcium content of the finger millet was 325.3 ± 2.6 mg/100 g, while it was 42.0 ± 1.7, 26.9 ± 1.5, 10.6 ± 0.4, 10.5 ± 0.2, and 51.3 ± 0.5 mg/100 g in pearl millet, sorghum, rice, wheat, and maize respectively, showing that finger millet naturally had 12.4 times higher calcium content than major cereals.
Descriptive statistics of four in vitro studies [32,33,34,35] were conducted on calcium bioavailability from various processing methods including soaking, germination, fermentation, malting, decortication, popping, and expansion. Among these, decortication, popping, and expansion showed a 24.5% decrease in bioavailable calcium from 148.0 ± 2.8 to 111.6 ± 15.4 mg/100 g, in finger millet compared to unprocessed finger millet (Table 2). In contrast, fermentation was superior to other processes. It increased the bioavailable calcium content by 38.9% and was followed by germination which increased the bioavailable calcium content in finger millet by 23.3%. Malting and soaking increased it by 12.5 and 5.5%, respectively (Table 3).
Table 3.
Effect of processing on bioavailable calcium from finger millet.
The average in vitro percentage bioavailability of calcium was 44.1 ± 14.5% in unprocessed raw grain and 61.4 ± 21.5% in processed finger millet (i.e., germination, fermentation, malting, decortication, expansion, and popping). Table 4 shows the estimated bioavailability of calcium in various food items including cooked finger millet [31]. The fractional absorption of bioavailable calcium was 28.6% for finger millet while it was 21.2% for almond.
Table 4.
Estimated calcium bioavailability of various foods.
The risk assessment on selection bias, detection bias, attrition bias, and reporting bias shows the major risk comes from the blinding of participants as the study used finger millet which is unique in color and texture therefore, blinding is not possible. Moreover, two studies although used random method the detailed methodology was not clearly explained. The publication bias was determined using trim and fit model in funnel plot to account for the small sample size in both the studies. Based on NOS the quality of the articles was moderately high.
4. Discussion
4.1. Human Studies
Assessment of bioavailability of calcium is not straightforward. Retention studies assess how much calcium is retained in the body after calcium excretion through urine and feces. Only two such studies were identified and compared regarding calcium retention in finger millet with that in rice or refined finger millet. Although conducted decades ago, that study provides the only evidence on calcium retention to date. The calcium retention was high in finger millet compared to non-finger millet diet which is not surprising as finger millet contains more calcium. However, the important point to notice is that despite finger millet having phytates, the calcium retention was high 23.4 ± 2.9%. The in vitro bioavailability of calcium was double in processed finger millet compared to unprocessed which suggests that there could be more calcium retention if finger millets are processed. Further investigation is needed to have a larger number of studies on calcium retention, bone turnover markers, impact of processed finger millet on bioavailability, and bone accretion. There was only one bone turnover maker assessment intervention recorded so far therefore, it was not used in the meta-analysis. Both calcium retention and bone turnover marker assessments are useful in determining the impact of finger millet consumption, however, more studies are required to confirm this, including various age groups to show how the high calcium level in finger millet can be a sustainable dietary approach for children’s growth and reduce the calcium-related health issues such as osteoporosis.
4.2. In Vitro Methods
All the existing calcium bioavailability studies on finger millet used in vitro methods. In humans, the intestinal calcium absorption is controlled by complex homeostatic mechanism and this internal regulation makes it difficult to rely solely on the in vitro measurement [38]. However, calcium has to be soluble in the gastrointestinal tract before it can be absorbed, thus, in vitro methods are useful to predict the calcium bioavailability from foods. In this paper, the four in vitro studies on calcium bioavailability from finger millet either used the iron solubility assay [32,34] or iron dialysability method [33,35]. Both methods are widely used to predict the bioavailability of minerals including calcium by simulating the gastric and small intestinal phase which involved the use of pepsin and pancreatin at pH 3 and 7 respectively followed by the measurement of the mineral in the soluble fraction after the small intestinal phase. Since most mineral absorption happens in the small intestine, including calcium, the end measurement would normally be after the intestinal phase. Sripriya et al. (1997) and Mamiro et al. (2001) adapted the iron solubility assay to predict the calcium bioavailability; however, the methods used for these two studies were different. Sripriya et al. (1997) used HCL-extractability method and did not involve the use of pepsin as it only mimics the gastric phase which may lead to under or overestimation. Mamiro et al. (2001) on the other hand used HCl-pepsin and pepsin-pancreatin mineral extractability, in which differences in the percentage of calcium bioavailability between these two methods were observed. This is due to different endpoint measurements where the latter measured the iron after the small intestinal stage and the other one after the gastric phase. Krishnan et al. (2012) and Platel et al. (2010) examined the calcium bioavailability using iron dialysability method whereby a dialysis bag was introduced in the intestinal phase and the calcium bioavailability was measured in the dialysate. According to Etcheverry et al. (2012), in vitro digestion coupled with human epithelial cell line called human colonic adenocarcinoma (Caco-2) is a recommended in vitro method for measuring the calcium bioavailability as the validity against human studies.
4.3. Effect of Processing on Bioavailable Calcium in In Vitro Method
Fermentation is a superior process in improving calcium bioavailability in finger millet. Fermentation is an age-old process followed by rural households in Asia and Africa. However, scientific evidence on the consumption of fermented products and its health benefits are scarce. In light of the health benefits of calcium and high calcium content in finger millet, it would be pertinent to conduct human studies on various forms of processed finger millets especially fermented food. Germination, fermentation, malting, and soaking increased the bioavailability of calcium while popping, decortication, and expansion decreased it. This could be due to the use of whole grain in germination and fermentation processes whereas the decortication and expansion processes involved loss of outer bran which contains calcium. Popping uses a whole grain but involves a high-temperature processing. The decrease in calcium bioavailability could be attributed to the high-temperature treatment applied during the expansion and popping [33].
4.4. Myths on Antinutrients
All plant-based foods contain antinutrients such as phytate and tannin. Finger millet contains these antinutrients at equal or less quantities than found in wheat, maize, and brown rice [3]. The effect of cooking reduced the level of phytates in finger millets only slightly (from 783.5 ± 2.5 to 781.6 ± 1.6 mg/100 g) and this reduction effect was similar across the cereals such as rice (289.9 ± 1.6 to 285.8 ± 1.1 mg/100 g), maize (851.5 ± 3.4 mg/100 g to 850.2 ± 2.8 mg/100 g), and wheat (792.1 ± 1.5 to 789.6 ± 1.5 mg/100 g). Similarly, the effect of cooking on reduction of tannin was very little in finger millet (264.1 ± 2.1 to 260.8 ± 2.8 mg/100 g) and other cereals such as rice (14.3 ± 1.3 to 14.9 ± 0.8 mg/100 g), wheat (287.3 ± 2.2 to 284.6 ± 1.5 mg/100 g), and maize (25.5 ± 1.1 to 24.5 ± 1.5 mg/100 g). Despite having phytates and tannin, the calcium bioavailability from finger millet was 28.6% upon cooking which is similar to milk (32.1%) [31]. This shows that finger millet can be a sustainable dietary option to tackle the calcium-related health issues. It was also evident that processing methods such as germination, fermentation, and malting reduce phytates by 60% [34] and increase the bioavailable calcium from finger millet by 61.4 ± 21.5%.
Finger millet was traditionally used as a baby porridge in some parts of India, possibly because of the high calcium content. Evaluations have not been undertaken on how to most effectively incorporate finger millet into diets, packaged foods, school meals, programs for overcoming malnutrition, baby food, and other specific uses where it has comparative advantages. Two studies were undertaken to assess the inclusion of finger millet in school-feeding programs in India and Tanzania respectively. The results show that the inclusion of finger millet increased the calcium content of mid-day meals compared to meals based on rice and maize [39,40].
Table 4 shows that 240 g of finger millet provides a large quantity, 250 mg, of absorbable calcium while 240 mL of cow milk provides 91 mg of absorbable calcium. Sesame with hull contains a high level of absorbable calcium, of 640 to 831 mg from 240 g which is more than the amount of bioavailable calcium that can be obtained from milk or finger millet. However, sesame is not eaten as a whole meal, in a quantity of 240 g, nor regular food in any part of the world.
Table 5 shows that just 100 g of finger millet can contribute 122% to the calcium RDA for infants, 73% of the RDA for growing children at 1–3 years, taking bioavailability into account. These are important growth stages where the calcium requirement needs to be met in order to avoid complications in later stages of life.
Table 5.
Percentage contribution of calcium from 100 g of finger millet to recommended dietary allowance (RDA).
Animal-sourced food is often not regularly consumed in rural areas where there is no livestock or is not affordable [42]. Moreover, there is a high prevalence of lactose intolerance globally. Lactose-intolerant individuals account for 75–90% of African-Americans, 100% of native Americans, 80–90% of Asian Americans, and 12% of Caucasians [43], suggesting the need for alternate calcium sources such as finger millet. Given all these facts, finger millet stands as an alternative staple food that could provide high content of calcium. However, in order to fully exploit high calcium millets, it will be important that diets also contain adequate amounts of other bonetrophic nutrients including phosphorus and magnesium and that the target population is of adequate vitamin D status.
4.5. Limitations
The major limitation was the small number of studies conducted to determine the effect of consuming finger millet. In this meta-analysis, only two calcium retention studies were conducted and these were undertaken between 1958 and 1957. Although there is no change in calcium content of finger millet and the methodology used was a standard practice, new studies should be undertaken. Apart from this, both studies had a sample size of only 8 individuals, and therefore of less power. However, they could not be eliminated as they were the only two studies available. These limitations suggest the requirement of more studies on this topic, especially considering the importance of finger millet as a sustainable dietary option [44]. It is also recommended that additional methodologies such as stable isotope methods, which are considered more accurate and reliable should also be used to study the bone calcium accretion.
4.6. Recommendation
1. There is thus far no bioavailability study conducted in humans on calcium from finger millet. Although in vitro studies prove the superiority of calcium content and bioavailable calcium from finger millet compared to other cereals, it is important to conduct human studies to further strengthen the evidence. In particular, a comparative study on bone calcium accretion and overall bone mineral mass would support the in vitro findings on finger millet as compared to other calcium-rich sources of food. 2. Some processing and cooking methods have been studied for their impact on the composition and bioavailability of calcium in finger millet. It is recommended that all major types of preparations, cooking, and processing should be studied systematically to gauge their impact on finger millet calcium levels and bioavailability. As the fermentation process is popular in rural areas of developing countries, it is important to conduct further studies to assess the efficacy of fermentation on calcium bioavailability in finger millet. 3. Interestingly, finger millet contains 41.60 µg/100 g of ergocalciferol (vitamin D2). Rice does not contain vitamin D2, while sorghum and wheat contain 3.96 µg/100 g and 6.73 µg/100 g of it, respectively [3]. Vitamin D2 is a plant and some fungi-based source of vitamin D, which provides the active form of vitamin D when consumed in higher dosage. The vitamin D2 co-present with calcium in finger millet should be studied for its role in impacting calcium absorption and bioavailability, and other health benefits. 4. The role of calcium in preventing stunting should be studied, including the benefits of calcium and protein from finger millet as a weaning food. 5. Further studies are encouraged on the design and impact of a finger-millet-based diet on bone health for babies, children, and especially during adolescence and on the prevention of osteoporosis at later age.
5. Conclusions
The few available studies show that finger millet provides high calcium bioavailability, and contributes to higher calcium retention due to its calcium content compared to other staples and reduced bone resorption, hence can exert beneficial effects especially for children, the elderly, and women. Moreover, simple household level processing such as germination and fermentation further improves bioavailable calcium. The high levels of calcium in finger millet and the positive results in the existing studies hold a promise for health benefits associated with finger millet integration into more diets and programs. As this is a fairly new area of study with regard to finger millet with very old evidence, further studies should be prioritized to ensure that appropriate diet recommendations can be made. There is a need for generating science-based evidence on its potential for improving bone mineral mass and other functions in the body.
Author Contributions
Conceptualization, S.A. and J.K.-P.; methodology, S.A. and R.B.; software, R.B.; validation, S.A., R.B. and D.I.G.; formal analysis, R.B.; investigation, S.A.; resources, J.K.-P.; data curation, S.A. and K.S.; writing—original draft preparation, S.A., D.I.G., N.L.B.S. and T.W.T.; writing—review and editing, J.K.-P., D.I.G., S.A., T.W.T., A.R., D.J.P. and R.K.B.; funding acquisition, J.K.-P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Smart Food endowment fund, ICRISAT.
Institutional Review Board Statement
The study did not directly involved with any human samples therefore the ethical approval was not required for this study. However, the systematic review and meta-analysis protocol is registered in online platform “reviewregistry” with the unique identification number “reviewregistry1136”.
Acknowledgments
The authors acknowledge Joycelyn M. Boiteau, Division of Nutritional Sciences, Cornell University Tata-Cornell Institute for Agriculture and Nutrition, the United States of America for reviewing the case and her valuable inputs that contributed significantly to the quality of the study. The authors thank the support provided by Ramesh Kotnana for advice and assistance in sourcing scientific articles.
Conflicts of Interest
The authors declare no conflict of interest.
References
- IOF. Epidemiology of Osteoporosis and Fragility Fractures. 2021. Available online: www.osteoporosis.foundation/facts-statistics/epidemiology-of-osteoporosis-and-fragility-fractures (accessed on 28 May 2021).
- Puranik, S.; Kam, J.; Sahu, P.P.; Yadav, R.; Srivastava, R.K.; Ojulong, H.; Yadav, R. Harnessing finger millet to combat calcium deficiency in humans: Challenges and prospects. Front. Plant Sci. 2017, 8, 1311. [Google Scholar] [CrossRef] [Green Version]
- Longvah, T.; Ananthan, R.; Bhaskarachary, K.; Venkaiah, K. Indian Food Composition Table; National Institute of Nutrition: Hyderabad, India, 2017. [Google Scholar]
- Bailey, D.A.; Martin, A.D.; Mckay, H.A.; Whiting, S.; Mirwald, R. Calcium accretion in girls and boys during puberty: A longitudinal analysis. J. Bone Miner. Res. 2000, 15, 2245–2250. [Google Scholar] [CrossRef]
- Bhide, R.; Patil, S.; Shetty, S.; Narayanan, S. Comparative bioavailability studies of calcium from different sources. Asian J. Pharm. Clin. Res. 2013, 6, 147–148. [Google Scholar]
- Palacios, C.; Hofmeyr, G.J.; Cormick, G.; Garcia-Casal, M.N.; Pena-Rosas, J.P.; Betran, A.P. Current calcium fortification experiences: A review. Ann. N.Y. Acad. Sci. 2021, 1484, 55–73. [Google Scholar] [CrossRef]
- Miller, G.D.; Jarvis, J.K.; McBean, L.D. The importance of meeting calcium needs with foods. J. Am. Coll. Nutr. 2001, 20, 168S–185S. [Google Scholar] [CrossRef]
- Park, H.M.; Heo, J.; Park, Y. Calcium from plant sources is beneficial to lowering the risk of osteoporosis in postmenopausal Korean women. Nutr. Res. 2011, 31, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Poole, N.; Kane-Potaka, J. The smart food triple bottom line—Starting with diversifying staples—Including summary of latest smart food studies at ICRISAT. Agric. Dev. J. 2020, 41, 21–23. Available online: taa.org.uk/wp-content/uploads/2021/01/Ag4Dev41_Winter_2020_WEB.pdf (accessed on 3 March 2021).
- Anitha, S.; Kane-Potaka, J.; Tsusaka, T.W.; Botha, R.; Rajendran, A.; Givens, D.I.; Parasannanavar, D.J.; Subramaniam, K.; Kanaka, P.; Mani, V.; et al. A systematic review and meta-analysis of the potential of millets and sorghum for managing and preventing diabetes mellitus. Front. Nutr. 2021, 8, 386. [Google Scholar] [CrossRef]
- Anitha, S.; Botha, R.; Kane-Potaka, J.; Givens, D.I.; Rajendran, A.; Tsusaka, T.W.; Bhandari, R. Can millet consumption help to manage hyperlipidaemia and obesity—A systematic review and meta-analysis. Front. Nutr. 2021, 8, 478. [Google Scholar]
- Anitha, S.; Kane-Potaka, J.; Botha, R.; Givens, D.I.; Binti Sulaiman, N.L.; Upadhyay, S.; Longvah, T.; Rajendran, A.; Tsusaka, T.W.; Subramaniam, K.; et al. Millets can have a major impact on improving iron status, haemoglobin level and in reducing iron deficiency anaemia—A systematic review and meta-analysis. Front. Nutr. 2021, Submitted. [Google Scholar]
- Bhavya Bhanu, P.V.; Serma Saravana Pandian, A.; Vinothini, P.; Mathanghi, S.K. Analysing the consumer preference for dairy products in Trivandrum city, India. Int. J. Sci. Environ. 2017, 6, 650–654. [Google Scholar]
- Kumar, A.; Joshi, P.K.; Kumar, P.; Parappurathu, S. Trends in the consumption of milk and milk products in india: Implications for self-sufficiency in milk production. Food Sec. 2014, 6, 719–726. [Google Scholar] [CrossRef]
- Singh, P.; Raghuvanshi, R.S. Finger millet for food and nutritional security. Afr. J. Food Sci. 2011, 6, 77–84. [Google Scholar]
- Mohar, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analysis: The PRISMA statement. Open Med. 2009, 3, 123–130. [Google Scholar]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing Meta-Analysis in R: A Hands-On Guide; CRC Press: Raton, FL, USA, 2021; Available online: bookdown.org/MathiasHarrer/Doing_Meta_Analysis_in_R/ (accessed on 28 February 2021).
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Version 6.2 (updated February 2021); Cochrane: London, UK, 2021; Available online: www.training.cochrane.org/handbook (accessed on 13 April 2021).
- Ahn, E.; Kang, H. Introduction to systematic review and meta-analysis. Korean J. Anaesthesiol. 2019, 71, 103–112. [Google Scholar] [CrossRef] [Green Version]
- Andrade, C. Understanding the basics of meta-analysis and how to read a forest plot: As simple as it gets. J. Clin. Psychiatry 2020, 81, e1–e5. [Google Scholar] [CrossRef]
- Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-Randomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011. [Google Scholar]
- Luchini, C.; Stubbs, B.; Solmi, M.; Veronese, N. Assessing the quality of studies in meta-analyses: Advantages and limitations of the Newcastle Ottawa Scale. World J. Meta-Anal. 2017, 5, 80–84. [Google Scholar] [CrossRef]
- Bell, A.; Fairbrother, M.; Jones, K. Fixed and random effects models: Making an informed choice. Qual. Quant. 2019, 53, 1051–1074. [Google Scholar] [CrossRef] [Green Version]
- Hak, T.; Van Rhee, H.J.; Suurmond, R. How to Interpret Results of Meta-Analysis; Version 1.3.; Erasmus Rotterdam institute of management: Rotterdam, The Netherlands, 2018; Available online: www.erim.eur.nl/research-support/meta-essentials/downloads (accessed on 26 April 2021).
- Isreal, H.; Richter, R.P. A guide to understanding meta-analysis. J. Orthop. Sports Phys. Ther. 2011, 41, 496–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial? Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Zlowodzki, M.; Poolman, R.W.; Kerkhoffs, G.M.; Tornetta, P.; Bhandari, M. How to interpret a meta-analysis and judge its value as a guide for clinical practice? Acta Orthop. 2007, 78, 598–609. [Google Scholar] [CrossRef] [PubMed]
- Joseph, K.; Kurien, P.P.; Swaminathan, M.; Subramaniyan, V. The effect of partial or complete replacement of rice in poor vegetarian diets by ragi (Eleusine coracana) on the metabolism of nitrogen, calcium and phosphorus. Brit. J. Nutr. 1958, 12, 213–218. [Google Scholar]
- Kurien, P.P.; Doraiswamy, T.R. Effect of replacing cereal in a poor diet with whole or refined ragi four on the nutritional status and metabolism of nitrogen, calcium and phosphorus in children (boys). J. Nutr. Dietet. 1967, 4, 102–109. [Google Scholar]
- Gayathri, G.; Hemamalini, A.J. Plant based Indigenous dietary Calcium supplementation on bone turnover markers among Peri and postmenopausal women: A randomised controlled trial. Indian J. Comm. Health 2020, 32, 705–712. [Google Scholar] [CrossRef]
- Amalraj, A.; Pius, A. Influence of Oxalate, Phytate, Tannin, dietary fiber and cooking on Calcium bioavailability of commonly consumed cereals and millets in India. Cereal Chem. 2015, 92, 389–394. [Google Scholar] [CrossRef]
- Mamiro, P.R.S.; Van Camp, J.; Mwikya, S.M.; Huyghebaert, A. In vitro extractability of calcium, iron, and zinc in finger millet and kidney beans during processing. Food Chem. Toxicol. 2001, 66, 1271–1275. [Google Scholar] [CrossRef]
- Krishnan, R.; Dharmaraj, U.; Malleshi, N.G. Influence of decortication, popping and malting on bioaccessibility of calcium, iron, and zinc in finger millet. Food Sci. Technol. 2012, 48, 169–174. [Google Scholar] [CrossRef]
- Sripriya, G.; Antony, U.; Chandra, T.S. Changes in carbohydrate, free amino acids, organic acids, phytate and HCl extractability of minerals during germination and fermentation of finger millet (Eleusine coracana). Food Chem. 1997, 58, 345–350. [Google Scholar] [CrossRef]
- Platel, K.; Epieson, S.W.; Srinivasan, K. Bioaccessible mineral content of malted finger millet (Eleusine coracana), wheat (Triticum aestivum), and Barley (Hordeum Vulgare). J. Agric. Food Chem. 2010, 58, 8100–8103. [Google Scholar] [CrossRef]
- Weaver, C.M.; Plawecki, K.L. Dietary calcium: Adequacy of a vegetarian diet. Am. J. Clin. Nutr. 1994, 59, 1238S–1241S. [Google Scholar] [CrossRef]
- Weaver, C.M.; Proulx, W.R.; Heaney, R. Choices for achieving adequate dietary calcium with a vegetarian diet. Am. J. Clin. Nutr. 1999, 70, 543s–548s. [Google Scholar] [CrossRef] [PubMed]
- Etcheverry, P.; Grusak, M.A.; Fleige, L.E. Application of in vitro bioaccessibility and bioavailability methods for calcium, carotenoids, folate, iron, magnesium, polyphenols, zinc, and vitamins B6, B12, D, and E. Front. Physiol. 2012, 3, 317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anitha, S.; Kane-Potaka, J.; Tsusaka, T.W.; Tripathi, D.; Upadhyay, S.; Kavishwar, A.; Jalagam, A.; Sharma, N.; Nedumaran, S. Acceptance and impact of millet-based mid-day meal on the nutritional status of adolescent school going children in a peri urban region of Karnataka state in India. Nutrients 2019, 11, 2077. [Google Scholar] [CrossRef] [Green Version]
- Wangari, C.; Mwema, C.; Siambi, M.; Silim, S.; Ubwe, R.; Malesi, K.; Anitha, S.; Kane-Potaka, J. Changing perception through a participatory approach by involving adolescent school children in evaluating smart food dishes in school feeding programs—Real time experience from central and northern Tanzania. Ecol. Food Nutr. 2020, 59, 472–485. [Google Scholar] [CrossRef] [Green Version]
- ICMR. Recommended Dietary Allowances and Estimated Average Requirements; National Institute of Nutrition: Hyderabad, India, 2020; pp. 1–319. [Google Scholar]
- Bai, Y.; Alemu, R.; Bloack, S.A.; Headey, D.; Masters, W.A. Cost and affordability of nutritious diet at retail prices: Evidence from 177 countries. Food Policy 2021, 99, 101983. [Google Scholar] [CrossRef]
- Hodges, J.K.; Cao, S.; Cladis, D.P.; Weaver, C.M. Lactose intolerance and bone health: The challenge of ensuring adequate calcium intake. Nutrients 2019, 11, 718. [Google Scholar] [CrossRef] [Green Version]
- Turner, R.M.; Bird, S.M.; Higgins, J.P.T. The impact of study size on meta-analyses: Examination of underpowered studies in Cochrane Reviews. PLoS ONE 2013, 8, e59202. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).