
The Role of Public Transport during the Second COVID-19 Wave in Italy

 ,
, 

Abstract
:1. Introduction
2. Study Area and Dataset
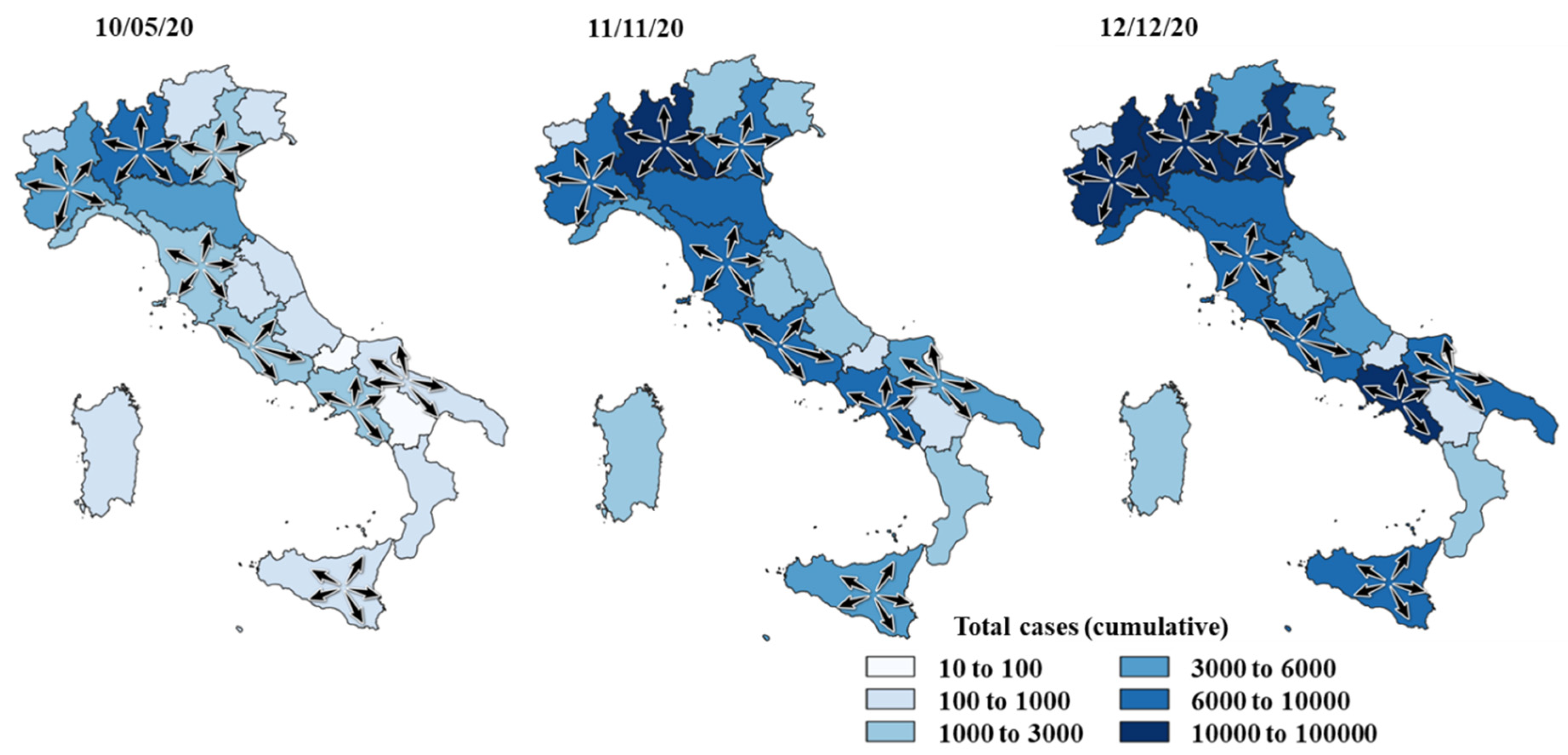
2.1. The Spread of COVID-19 in Italy
- -
- DPCM (the acronym used in Italy for the decrees issued by the president of the council of ministers) of 3 November 2020 (known as the DPCM of the “red zones”), which introduced the division of the territory into zones with different levels of severity and risk, limiting mobility trips between regions;
- -
- DPCM of 3 December 2020, which confirmed and temporally extended the diversification of the regulations adopted by the previous decree;
- -
- various Ordinances of the Ministry of Health which, in implementing the measures provided for in the DPCM of November and December, classified the regions into red, orange, and yellow zones on the basis of data processed by the National Control Center after consulting the Scientific Technical Committee on the monitored data;
- -
- legislative Decree of 18 December 2020 no. 172, known as the “Christmas Decree”, which provided a package of urgent measures for the Christmas holidays and the beginning of the New Year.
- -
- yellow zones, in which the following measures were implemented: a strict travel ban from 10 p.m. to 5 a.m., with only working/necessity/safe activities allowed; closure of shopping malls on public holidays and the day preceding them, with only grocers, chemists, and stationers being permitted to open those days; restriction of bars and restaurants to opening only between 5 a.m. and 6 p.m., extended to 10 p.m. for takeaway services, with no limits for home deliveries; closure of museums, exhibitions, cinemas, games rooms, betting shops; the suspension of public and private competitions, except for those recruiting health system and civil protection teams; public transport vehicles allowed to run no more than half full, except for school buses; online lessons and lectures required for all schools and universities, starting from secondary level;
- -
- orange zones, with high risk and severity, in which the following additional measures were undertaken with respect to yellow zones: strict travel bans to regions or municipalities other than those of residence, except for those traveling for work, health, or safety reasons; restaurants and bars closed to the public except for takeaway services and home deliveries before 10 p.m.;
- -
- red zones, with the highest risk and severity, in which further additional measures were implemented: closure of all retail businesses except for grocers, chemists, and stationers; suspension of all group sport activities, with only individual sport activities being allowed in proximity to the home; online lessons and lectures required for all schools and universities, except for kindergartens, primary schools, and the first year of secondary schools; suspension of activities relating to personal care services, with the exception of laundries, dry cleaners, barbers, hairdressers, and funeral services; restricted access to public administration staff, and exclusively for necessary activities, promotion of the use of smart working for employees.
- -
- “red zones” at national scale on holidays and preceding days;
- -
- “orange zones” on weekdays;
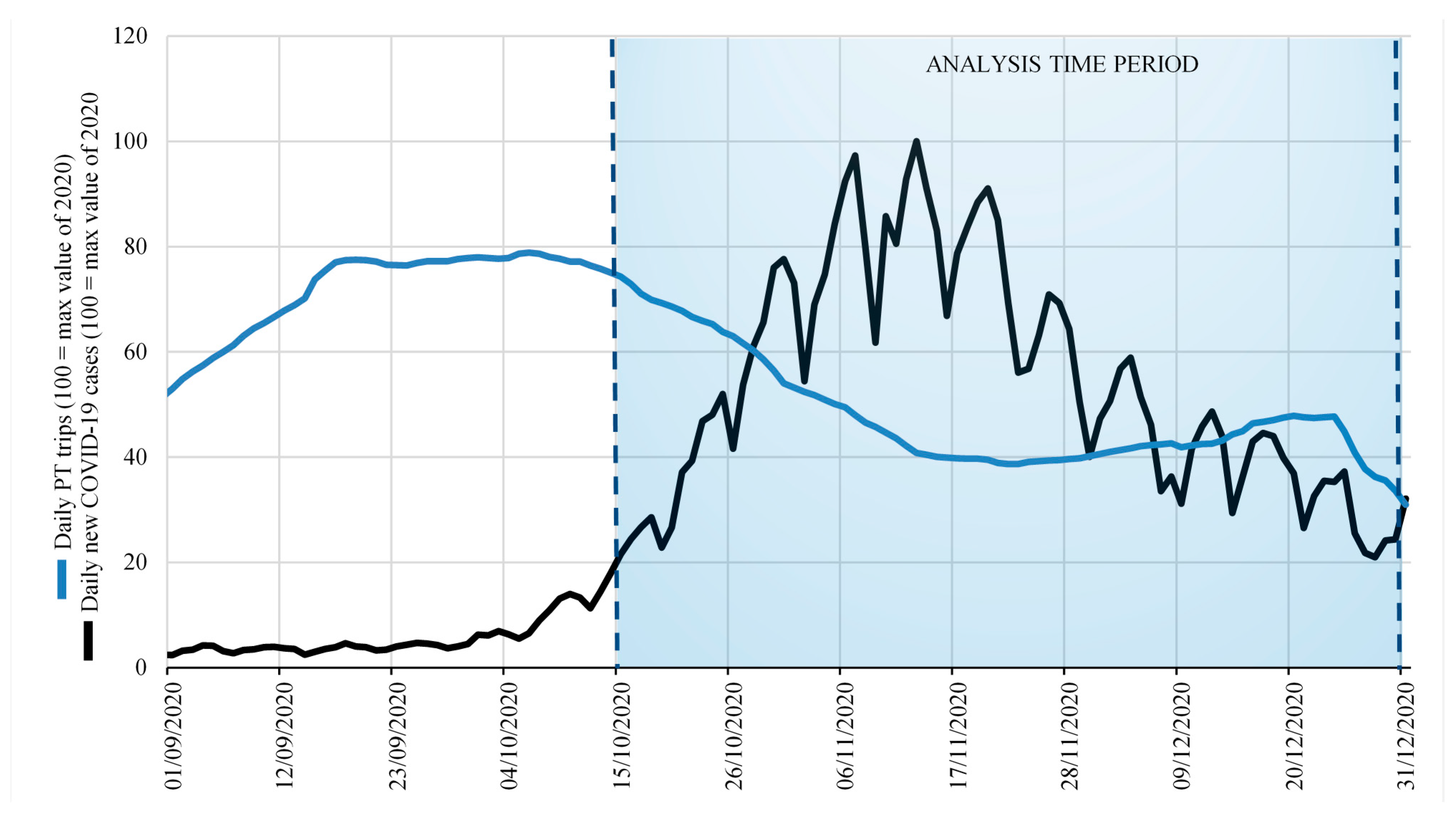
2.2. Data Collection
- ▪
- the Italian national census data relative to the year 2019 [41], useful for geographical representation and socio-economic quantitative representation (e.g., population; area in km2);
- ▪
- the daily new COVID-19 cases, sourced from the Italian Ministry of Health (2020);
- ▪
- the COVID-19 mobility observatory of the Italian Ministry of Sustainable Infrastructure and Mobility (2020), collecting the number of daily public transport trips.
3. Estimation Method
- ▪
- temporality, that is, the necessity that the cause precedes the effect over time (e.g., first breathing polluted and infected air, then remaining infected);
- ▪
- biological/physical plausibility, that is, the possibility that the cause produces the effect (e.g., PT trips could be a vehicle of virus contagion);
- ▪
- strength, that is, the estimated index value (e.g., with as high a value as possible);
- ▪
- consistency, with other scientific studies and/or research (e.g., similar results obtained in other case studies).
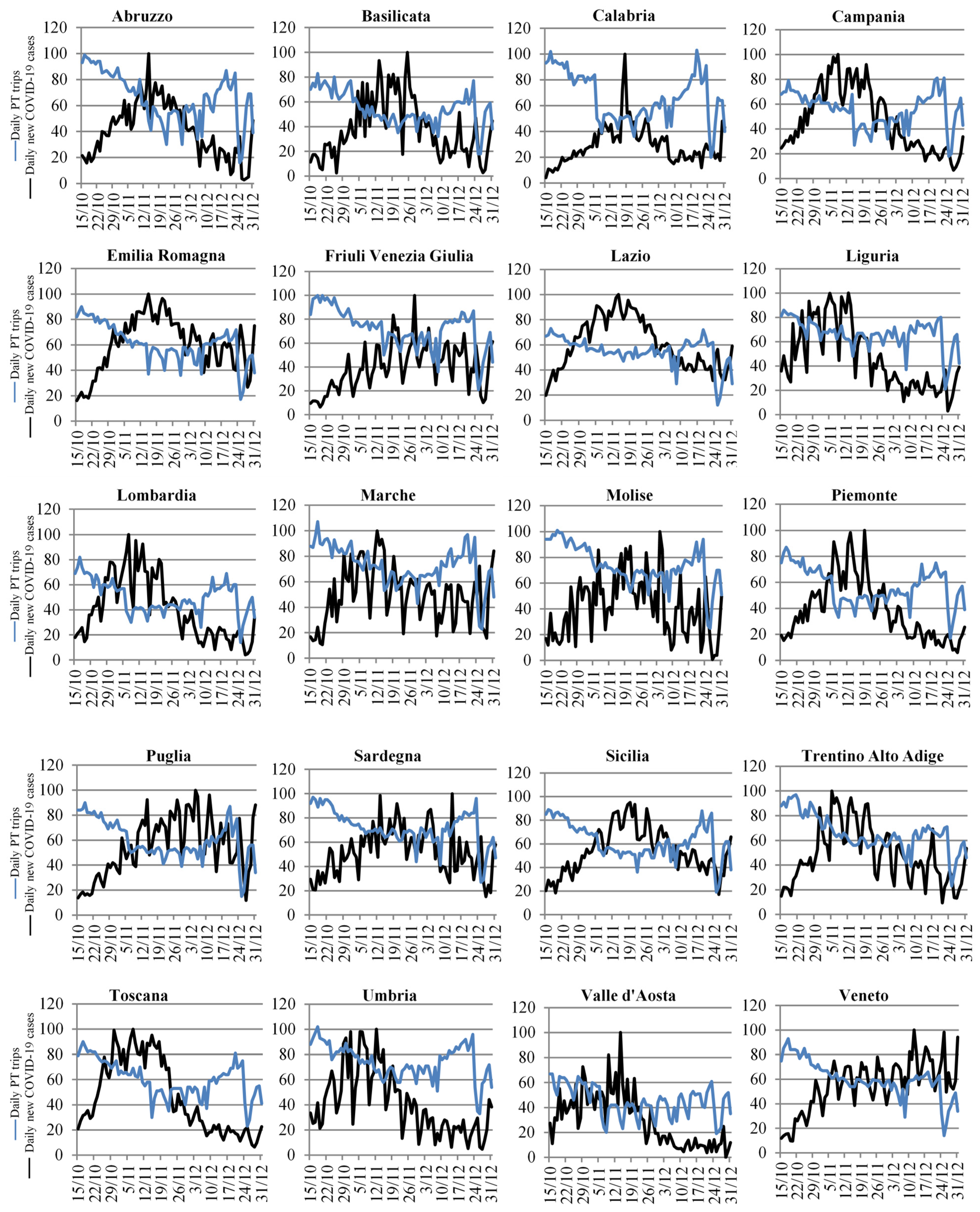
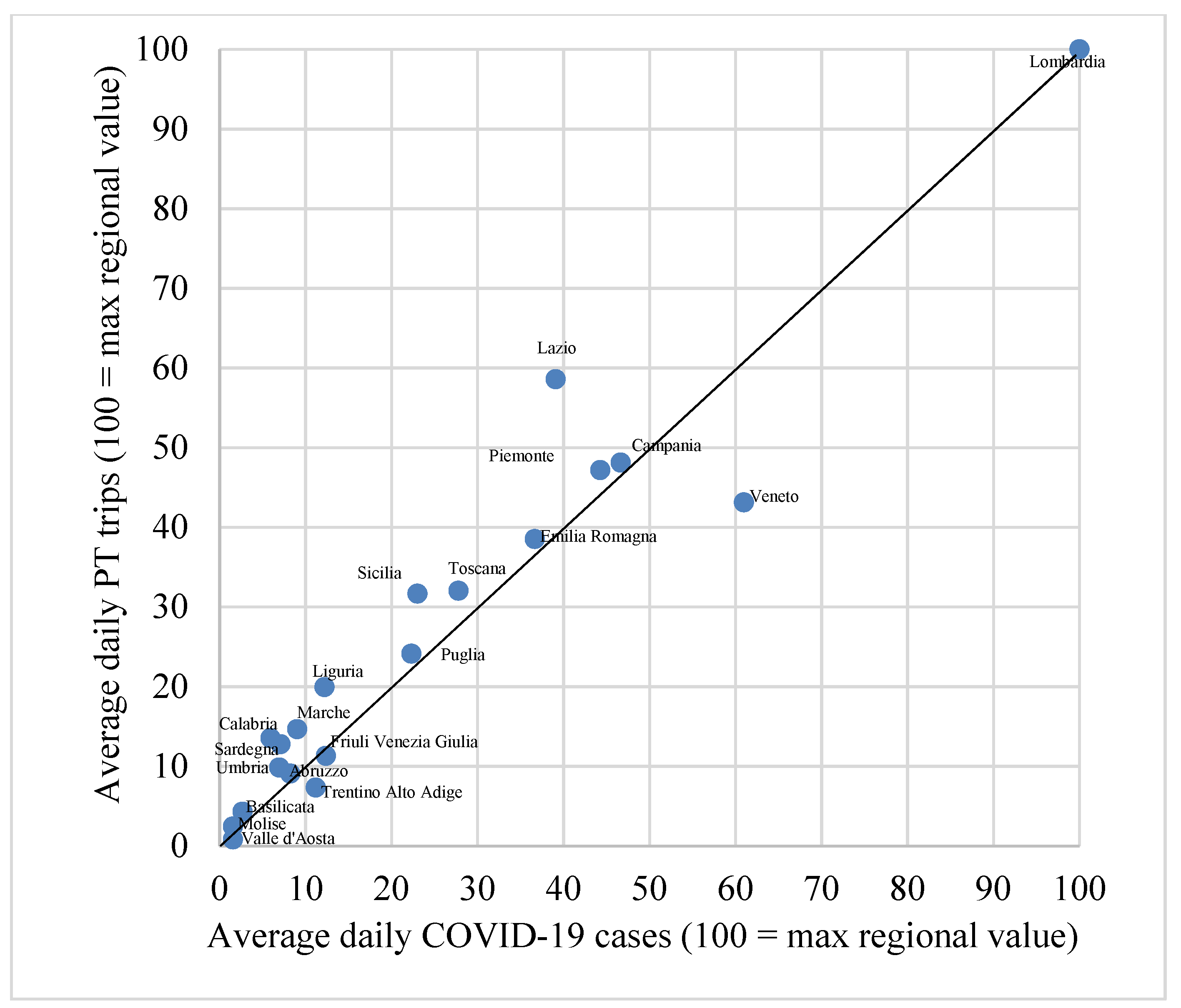
4. Results and Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bontempi, E. The Europe second wave of COVID-19 infection and the Italy “strange” situation. Environ. Res. 2021, 193, 110476. [Google Scholar] [CrossRef]
- Morawska, L.; Tang, J.W.; Bahnfleth, W.; Bluyssen, P.M.; Boerstra, A.; Buonanno, G.; Cao, J.; Dancer, S.; Floto, A.; Franchimon, F.; et al. How can airborne transmission of COVID-19 indoors be minimised? Environ. Int. 2020, 142, 105832. [Google Scholar] [CrossRef]
- Tirachini, A.; Cats, O. COVID-19 and public transportation: Current assessment, prospects, and research needs. J. Public Transp. 2020, 22, 1. [Google Scholar] [CrossRef]
- Bashir, M.F.; Ma, B.; Komal, B.; Bashir, M.A.; Tan, D.; Bashir, M. Correlation between climate indicators and COVID-19 pandemic in New York, USA. Sci. Total Environ. 2020, 728, 138835. [Google Scholar] [CrossRef]
- Lin, C.; Lau, A.K.; Fung, J.C.; Guo, C.; Chan, J.W.; Yeung, D.W.; Zhang, Y.; Bo, Y.; Hossain, M.S.; Zeng, Y. A mechanism-based parameterisation scheme to investigate the association between transmission rate of COVID-19 and meteorological factors on plains in China. Sci. Total Environ. 2020, 737, 140348. [Google Scholar] [CrossRef] [PubMed]
- Prata, D.N.; Rodrigues, W.; Bermejo, P.H. Temperature significantly changes COVID-19 transmission in (sub) tropical cities of Brazil. Sci. Total Environ. 2020, 729, 138862. [Google Scholar] [CrossRef] [PubMed]
- Qi, H.; Xiao, S.; Shi, R.; Ward, M.P.; Chen, Y.; Tu, W.; Su, Q.; Wang, W.; Wang, X.; Zhang, Z. COVID-19 transmission in Mainland China is associated with temperature and humidity: A time-series analysis. Sci. Total Environ. 2020, 728, 138778. [Google Scholar] [CrossRef]
- Rashed, E.A.; Kodera, S.; Gomez-Tames, J.; Hirata, A. Influence of absolute humidity, temperature and population density on COVID-19 spread and decay durations: Multi-prefecture study in Japan. Int. J. Environ. Res. Public. Health 2020, 17, 5354. [Google Scholar] [CrossRef]
- Shi, P.; Dong, Y.; Yan, H.; Zhao, C.; Li, X.; Liu, W.; He, M.; Tang, S.; Xi, S. Impact of temperature on the dynamics of the COVID-19 outbreak in China. Sci. Total Environ. 2020, 728, 138890. [Google Scholar] [CrossRef]
- Tosepu, R.; Gunawan, J.; Effendy, D.S.; Lestari, H.; Bahar, H.; Asfian, P. Correlation between weather and COVID-19 pandemic in Jakarta, Indonesia. Sci. Total Environ. 2020, 725, 138436. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Jing, W.; Liu, J.; Ma, Q.; Yuan, J.; Wang, Y.; Du, M.; Liu, M. Effects of temperature and humidity on the daily new cases and new deaths of COVID-19 in 166 countries. Sci. Total Environ. 2020, 729, 139051. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Xie, J. Association between ambient temperature and COVID-19 infection in 122 cities from China. Sci. Total Environ. 2020, 724, 138201. [Google Scholar] [CrossRef] [PubMed]
- Carugno, M.; Dentali, F.; Mathieu, G.; Fontanella, A.; Mariani, J.; Bordini, L.; Milani, G.P.; Consonni, D.; Bonzini, M.; Bollati, V.; et al. PM10 exposure is associated with increased hospitalizations for respiratory syncytial virus bronchiolitis among infants in Lombardy, Italy. Environ. Res. 2018, 166, 452–457. [Google Scholar] [CrossRef]
- Setti, L.; Passarini, F.; De Gennaro, G.; Barbieri, P.; Perrone, M.G.; Borelli, M.; Palmisani, J.; Di Gilio, A.; Piscitelli, P.; Miani, A. Airborne transmission route of COVID-19: Why 2 meters/6 feet of inter-personal distance could not be enough. Multidisciplinary Digital Publishing Institute. Int. J. Environ. Res. Public Health 2020, 17, 2932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Setti, L.; Passarini, F.; De Gennaro, G.; Di Gilio, A.; Palmisani, J.; Buono, P.; Fornari, G.; Perrone, M.G.; Piazzalunga, A.; Barbieri, P. Evaluation of the Potential Relationship between Particulate Matter (PM) Pollution and COVID-19 Infection Spread in Italy. Soc. Italy di Med. Ambient. 2020. Available online: https://www.aircentre.org/wp-content/uploads/2020/04/Setti_et_al_2020.pdf (accessed on 1 September 2021).
- Cartenì, A.; Di Francesco, L.; Martino, M. How mobility habits influenced the spread of the COVID-19 pandemic: Results from the Italian case study. Sci. Total Environ. 2020, 741, 140489. [Google Scholar] [CrossRef]
- Kraemer, M.U.; Yang, C.H.; Gutierrez, B.; Wu, C.H.; Klein, B.; Pigott, D.M.; Du Plessis, L.; Faria, N.R.; Li, R.; Hanage, W.P.; et al. The effect of human mobility and control measures on the COVID-19 epidemic in China. Science 2020, 368, 493–497. [Google Scholar] [CrossRef] [Green Version]
- Islam, N.; Sharp, S.J.; Chowell, G.; Shabnam, S.; Kawachi, I.; Lacey, B.; Massaro, J.M.; D’Agostino, R.B.; White, M. Physical distancing interventions and incidence of coronavirus disease 2019: Natural experiment in 149 countries. BMJ 2020, 370, m2743. [Google Scholar] [CrossRef]
- McGrail, D.J.; Dai, J.; McAndrews, K.M.; Kalluri, R. Enacting national social distancing policies corresponds with dramatic reduction in COVID19 infection rates. PLoS ONE 2020, 15, e0236619. [Google Scholar] [CrossRef]
- Auger, K.A.; Shah, S.S.; Richardson, T.; Hartley, D.; Hall, M.; Warniment, A.; Timmons, K.; Bosse, D.; Ferris, S.A.; Brady, P.W.; et al. Association Between Statewide School Closure and COVID-19 Incidence and Mortality in the US. JAMA 2020, 324, 859–870. [Google Scholar] [CrossRef]
- Im Kampe, E.O.; Lehfeld, A.S.; Buda, S.; Buchholz, U.; Haas, W. Surveillance of COVID-19 school outbreaks, Germany, March to August 2020. Eurosurveillance 2020, 25, 2001645. [Google Scholar] [CrossRef]
- Stein-Zamir, C.; Abramson, N.; Shoob, H.; Libal, E.; Bitan, M.; Cardash, T.; Cayam, R.; Miskin, I. A large COVID-19 outbreak in a high school 10 days after schools’ reopening, Israel, May 2020. Eurosurveillance 2020, 25, 2001352. [Google Scholar] [CrossRef]
- Jenelius, E.; Cebecauer, M. Impacts of COVID-19 on public transport ridership in Sweden: Analysis of ticket validations, sales and passenger counts. Transp. Res. Interdiscip. Perspect. 2020, 8, 100242. [Google Scholar] [PubMed]
- Vitrano, C. COVID-19 and Public Transport. A Review of the International Academic Literature; Media-Tryck: Lund, Sweden, 2021; Available online: https://www.k2centrum.se/sites/default/files/fields/field_uppladdad_rapport/covid-19_and_public_transport.pdf (accessed on 1 September 2021).
- Bucsky, P. Modal share changes due to COVID-19: The case of Budapest. Transp. Res. Interdiscip. Perspect. 2020, 8, 100141. [Google Scholar] [CrossRef]
- de Haas, M.; Faber, R.; Hamersma, M. How COVID-19 and the Dutch ‘intelligent lockdown’ change activities, work and travel behaviour: Evidence from longitudinal data in the Netherlands. Transp. Res. Interdiscip. Perspect. 2020, 6, 100150. [Google Scholar] [CrossRef]
- Aloi, A.; Alonso, B.; Benavente, J.; Cordera, R.; Echániz, E.; González, F.; Ladisa, C.; Lezama-Romanelli, R.; López-Parra, Á.; Mazzei, V.; et al. Effects of the COVID-19 lockdown on urban mobility: Empirical evidence from the city of Santander (Spain). Sustainability 2020, 12, 3870. [Google Scholar] [CrossRef]
- Hörcher, D.; Singh, R.; Graham, D.J. Social Distancing in Public Transport: Mobilising New Technologies for Demand Management under the COVID-19 Crisis. 2020. Available online: https://ssrn.com/abstract=3713518 (accessed on 1 September 2021). [CrossRef]
- de Lima, G.C.L.S.; de Carvalho, G.S.D.; Figueiredo, M.Z. Incomplete contracts for bus service during the COVID-19 pandemic. RAP Rev. Bras. Adm. Pública 2020, 54, 994–1009. [Google Scholar] [CrossRef]
- Budd, L.; Ison, S. Responsible Transport: A post-COVID agenda for transport policy and practice. Transp. Res. Interdiscip. Perspect. 2020, 6, 100151. [Google Scholar] [CrossRef]
- Pawar, D.S.; Yadav, A.K.; Akolekar, N.; Velaga, N.R. Impact of physical distancing due to novel coronavirus (SARS-CoV-2) on daily travel for work during transition to lockdown. Transp. Res. Interdiscip. Perspect. 2020, 7, 100203. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.A.; Judd, J. COVID-19: Vulnerability and the power of privilege in a pandemic. Health Promot. J. Aust. 2020, 31, 158. [Google Scholar] [CrossRef] [Green Version]
- Gutiérrez, A.; Miravet, D.; Domènech, A. COVID-19 and urban public transport services: Emerging challenges and research agenda. Cities Health 2020, 1–4. [Google Scholar] [CrossRef]
- Sutherland, M.; McKenney, M.; Elkbuli, A. Vehicle related injury patterns during the COVID-19 pandemic: What has changed? Am. J. Emerg. Med. 2020, 38, 1710–1714. [Google Scholar] [CrossRef]
- Aven, T.; Kristensen, V. Perspectives on risk: Review and discussion of the basis for establishing a unified and holistic approach. Reliab. Eng. Syst. Saf. 2005, 90, 1–14. [Google Scholar] [CrossRef]
- Aven, T. Risk assessment and risk management: Review of recent advances on their foundation. Eur. J. Oper. Res. 2016, 253, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Junior, J.A.G.; Busso, C.M.; Gobbo, S.C.O.; Carreão, H. Making the links among environmental protection, process safety, and industry 4.0. Process. Saf. Environ. Prot. 2018, 117, 372–382. [Google Scholar]
- Khan, F.; Rathnayaka, S.; Ahmed, S. Methods and models in process safety and risk management: Past, present and future. Process. Saf. Environ. Prot. 2015, 98, 116–147. [Google Scholar] [CrossRef]
- Pepe, E.; Bajardi, P.; Gauvin, L.; Privitera, F.; Lake, B.; Cattuto, C.; Tizzoni, M. COVID-19 outbreak response: A first assessment of mobility changes in Italy following national lockdown. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Cartenì, A.; Di Francesco, L.; Martino, M. The role of transport accessibility within the spread of the Coronavirus pandemic in Italy. Saf. Sci. 2021, 133, 104999. [Google Scholar] [CrossRef] [PubMed]
- [Dataset] ISTAT. 2020. Available online: https://www.istat.it/it/archivio/222527 (accessed on 6 May 2020).
- [Dataset] Italian Ministry of Sustainable Infrastructure and Mobility. Strategic and Infrastructures Development Office: COVID-19 Mobility Observatory. 2020. Available online: http://www.mit.gov.it/ (accessed on 15 January 2021).
- [Dataset] Italian Ministry of Health. Daily Reports on COVID-19 Positive Cases. 2020. Available online: http://www.salute.gov.it/portale/home.html (accessed on 15 January 2021).
- Bookbinder, M.; Panosian, K.J. Using the coefficient of correlation in method-comparison studies. Clin. Chem. 1987, 33, 1170–1176. [Google Scholar] [CrossRef]
- Masyn, K.; Nathan, P.; Little, T. The Oxford Handbook of Quantitative Methods; Little, T.D., Ed.; Oxford University Press: Oxford, UK, 2013; Volume 2, pp. 551–611. [Google Scholar]
- Asuero, A.G.; Sayago, A.; Gonzalez, A.G. The Correlation Coefficient: An Overview. Crit. Rev. Anal. Chem. 2006, 36, 41–59. [Google Scholar] [CrossRef]
- Beck, M.J.; Hensher, D.A.; Nelson, J.D. Public transport trends in Australia during the COVID-19 pandemic: An investigation of the influence of bio-security concerns on trip behaviour. J. Transp. Geogr. 2021, 96, 103167. [Google Scholar] [CrossRef]
- Carteni’, A. A cost-benefit analysis based on the carbon footprint derived from plug-in hybrid electric buses for urban public transport services. WSEAS Trans. Environ. Dev. 2018, 14, 125–135, ISSN/E-ISSN 1790-5079/2224-3496. [Google Scholar]
- Carteni’, A.; Henke, I.; Molitierno, C. A cost-benefit analysis of the metro line 1 in Naples, Italy. WSEAS Trans. Bus. Econ. 2018, 15, 529–538, ISSN 1109-9526. [Google Scholar]
- Henke, I.; Carteni, A.; Molitierno, C.; Errico, A. Decision-Making in the transport sector: A sustainable evaluation method for road infrastructure. Sustainability 2020, 12, 764. [Google Scholar] [CrossRef] [Green Version]
- Cascetta, E.; Cartenì, A. A quality-based approach to public transportation planning: Theory and a case study. Int. J. Sustain. Transp. 2014, 8, 84–106. [Google Scholar] [CrossRef] [Green Version]
- Cascetta, E.; Cartenì, A.; Henke, I. Stations quality, aesthetics and attractiveness of rail transport: Empirical evidence and mathematical models (Qualità delle stazioni, estetica e attrattività del trasporto ferroviario: Evidenze empiriche e modelli matematici). Ing. Ferrov. 2014, 69, 307–324, ISSN 0020-0956. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indicator | First Wave Period (22 February–31 August) | Second Wave Period (1 September–31 December) |
|---|---|---|
| Number of days | 191 | 121 |
| Number of total infected cases | 269,214 | 1,837,952 |
| Number of total deaths | 35,483 | 38,676 |
| Number of total tests performed | 8,644,859 | 17,953,748 |
| Region | The Italian DPCM “RED ZONE” Decree | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| DPCM 3 Nov. 2020 | DPCM 3 Dec. 2020 | DL no. 172 18 Dec. 2020 | |||||||||
| 6 Nov.–10 Nov. | 11 Nov.–14 Nov. | 15 Nov.–21 Nov. | 22 Nov.–28 Nov. | 29 Nov.–05 Dec. | 6 Dec.–12 Dec. | 13 Dec.–19 Dec. | 20 Dec.–23 Dec. | 24 Dec.–27 Dec. | 28 Dec.–30 Dec. | 31 Dec.–3 Jan. | |
| Liguria | |||||||||||
| Lombardia | |||||||||||
| Piemonte | |||||||||||
| Valle d’Aosta | |||||||||||
| Emilia-Romagna | |||||||||||
| Friuli Venezia Giulia | |||||||||||
| Trentino Alto Adige | |||||||||||
| Veneto | |||||||||||
| Lazio | |||||||||||
| Marche | |||||||||||
| Toscana | |||||||||||
| Umbria | |||||||||||
| Abruzzo | |||||||||||
| Basilicata | |||||||||||
| Calabria | |||||||||||
| Campania | |||||||||||
| Molise | |||||||||||
| Puglia | |||||||||||
| Sardegna | |||||||||||
| Sicilia | |||||||||||
| Region | Pearson | Spearman | Somers |
|---|---|---|---|
| Abruzzo | 0.678 | 0.705 | 0.507 |
| Basilicata | 0.561 | 0.602 | 0.444 |
| Calabria | 0.410 | 0.467 | 0.325 |
| Campania | 0.863 | 0.809 | 0.644 |
| Emilia romagna | 0.720 | 0.749 | 0.565 |
| Friuli venzia giulia | 0.583 | 0.322 | 0.193 |
| Lazio | 0.811 | 0.747 | 0.601 |
| Liguria | 0.807 | 0.621 | 0.468 |
| Lombardia | 0.935 | 0.733 | 0.541 |
| Marche | 0.328 | 0.377 | 0.278 |
| Molise | 0.318 | 0.394 | 0.266 |
| Piemonte | 0.862 | 0.629 | 0.455 |
| Puglia | 0.343 | 0.410 | 0.236 |
| Sardegna | 0.363 | 0.419 | 0.295 |
| Sicilia | 0.380 | 0.498 | 0.358 |
| Toscana | 0.937 | 0.759 | 0.603 |
| Trentino alto adige | 0.526 | 0.504 | 0.362 |
| Umbria | 0.493 | 0.504 | 0.373 |
| Valle d’aosta | 0.524 | 0.451 | 0.303 |
| Veneto | 0.703 | 0.705 | 0.253 |
| Italy | 0.866 | 0.735 | 0.552 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cartenì, A.; Di Francesco, L.; Henke, I.; Marino, T.V.; Falanga, A. The Role of Public Transport during the Second COVID-19 Wave in Italy. Sustainability 2021, 13, 11905. https://doi.org/10.3390/su132111905
Cartenì A, Di Francesco L, Henke I, Marino TV, Falanga A. The Role of Public Transport during the Second COVID-19 Wave in Italy. Sustainability. 2021; 13(21):11905. https://doi.org/10.3390/su132111905
Chicago/Turabian StyleCartenì, Armando, Luigi Di Francesco, Ilaria Henke, Teresa Valentina Marino, and Antonella Falanga. 2021. "The Role of Public Transport during the Second COVID-19 Wave in Italy" Sustainability 13, no. 21: 11905. https://doi.org/10.3390/su132111905
APA StyleCartenì, A., Di Francesco, L., Henke, I., Marino, T. V., & Falanga, A. (2021). The Role of Public Transport during the Second COVID-19 Wave in Italy. Sustainability, 13(21), 11905. https://doi.org/10.3390/su132111905