1. Introduction
The COVID-19 pandemic is a public health crisis that has impacted the health of individuals around the globe. As of 17 March 2022, the World Health Organization reported 6,056,725 Coronavirus deaths globally, with the United States leading with a total of 960,194 deaths [
1]. Moreover, the CDC reports that 74.4% of COVID-19-related deaths in America were individuals 65 years old or older and that comorbid conditions (e.g., cancer, stroke) also increased the risk of serious illness or mortality [
2].
COVID-19 has threatened social sustainability in the United States and around the world. Eizenberg and Jabareen state that “social sustainability strives to confront risk while addressing social concerns” of equity, safety, eco-prosumption, and sustainable urban forms [
3]. Specifically, the COVID-19 pandemic has resulted in health disparities [
1,
4], threatened physical safety from serious illness and death, resulted in physical distancing and reduced ability to interact with others, and negatively impacted well-being ([
5]. To investigate the impact of COVID-19 on well-being and social inclusion (key concepts in social sustainability), this paper examined how increased COVID-19 risk, combined with concerns about the COVID-19 pandemic and lower feelings of control over one’s health and social life predicted engagement in protective health behaviors, and ultimately impacted feelings of depressive symptoms and loneliness in adults over the age of 50.
Physical distancing efforts in response to the COVID-19 pandemic have measurably influenced social relationships. Physical distancing refers to keeping a physical space of six feet or more between you and other individuals, while social distancing refers to the reduction of social interaction and communication between individuals [
6]. It is important to define some of the common vocabulary used in relation to the pandemic as many of these terms are used interchangeably, despite having different implications. Physical distancing regulations on access to community and assisted living facilities such as nursing homes, hospitals, and prisons—as well as travel restrictions—are associated with increased feelings of loneliness, and decreased feelings of friendship and connectedness [
7]. Many of these regulations began in the United States as early preventative responses to the spread of COVID-19, with the goal of protecting high-risk populations [
8]. Early media reports identified older adults as one of the most high-risk groups for negative consequences related to COVID-19, making this population a key target for preventative responses [
8]. However, these well-intentioned measures have influenced social distancing and feelings of isolation and depression in older adults. Many older adults who rely on social contact from community centers and places of worship are also experiencing significant disruptions in their social networks and relationships [
8].
In another study investigating disruptions in social networks and relationships, Ammar and colleagues examined the effects of home confinement in response to COVID-19 on social participation using survey respondents of adults ages 18 and over and found that social participation decreased by 42% among participants after home confinement as compared to before confinement [
9]. These findings suggest that confinement and quarantine efforts in response to COVID-19 have led to significant decreases in social participation and life satisfaction and demonstrate an increase in social exclusion [
9]. Other studies have reported negative effects of quarantine on adults of all ages, including confusion, anger, and post-traumatic stress symptoms [
10].
Along with the influence on social participation, these restrictive measures have also led to an increased reliance on the digitalization of life for both socialization as well as healthcare services. Yet, this technological push has digitally excluded individuals in vulnerable populations, and older adults are no exception to this [
11]. In fact, in a recent representative study, 7% of US adults over the age of 18 reported that they do not use the internet, with adults over the age of 65 being the largest group of digitally excluded individuals; 25% of older adults reported having never used the internet [
12]. Choi and colleagues demonstrated that although the use of telemedicine increased significantly during the pandemic compared to prior to the pandemic, adults aged 70 years and older were less likely to utilize telehealth than younger individuals [
13]. As a result of this digital exclusion and increased use of technology in healthcare, there were significantly fewer primary care physician visits in 2020 compared to previous years, which further increased the various social, mental and physical health effects of distancing efforts [
14].
1.1. Loneliness and Depression
Loneliness and depression are risk factors for mortality and other negative health outcomes. Loneliness refers to the perception of social isolation or the subjective feeling of being lonely that “occurs when there is a significant mismatch or discrepancy between a person’s actual social relations and his or her needed or desired social relations” [
15] (p. 571). When comparing the effects of loneliness and depression, Ng and colleagues found that loneliness is associated with a higher risk for mortality than depression among female older adults [
16]. Further, women in general are at higher risk for negative consequences of both loneliness and depression and report more worry, depression, and anxiety than males [
10,
15,
16].
Depression is defined by the National Institute of Mental Health as a mood disorder that affects how you feel, think, and complete daily tasks [
17]. Probst and colleagues studied the effects of lockdown measures on feelings of depression in adults over the age of 35 and found that more individuals reported being depressed after lockdown measures compared to before lockdown measures. This analysis suggests that lockdown measures had lasting negative effects on depression and mental health as a result of stress, loneliness, and social isolation [
18] on adults in general.
A recent report by the National Academies of Science, Engineering, and Medicine (NASEM) took a deep look into the effects of social isolation and loneliness and reviewed over four decades of research that shows how lacking social connections are associated with significantly increased risk for premature mortality [
19]. Social isolation typically refers to the objective lack of (or limited) social contact with others, and it is marked by an individual having few social network ties, having infrequent social contact, or, potentially, living alone [
19]. Effects of social isolation, including loneliness and depression, have been exasperated by various COVID-19 protective behaviors, including physical distancing [
20].
1.2. COVID-19 Protective Behaviors
In addition to physical distancing and reducing the number of contacts with others, public health messages encouraged frequent hand washing, wearing masks in public areas, and getting vaccinated if/when possible. Adults over the age of 18 who were more concerned about getting and spreading COVID-19 were more likely to follow preventative guidelines and protective health behaviors, including physical distancing [
21,
22]. Likewise, women and those aged 65 and over were more likely to practice COVID-19 preventative measures than other groups of individuals [
21,
22].
1.3. COVID-19 Concerns
The COVID-19 pandemic has generated concerns about health as well as other dimensions of life. Common concerns about COVID-19 include potential risks and impacts, financial consequences, personal health and the health of loved ones, productivity, lack of access to reliable information, and prevalence of health misinformation on social media [
5,
21,
23,
24]. For example, in a sample of adults aged 60 and older, respondents reported anxiety about contracting or spreading the virus to others, and most decreased their social interactions with friends and relatives [
25]. Concern about the COVID-19 pandemic led to significant increases in disease avoidance and self-protection [
26,
27]. There is also a component of fear related to the COVID-19 pandemic as well. Adults of all ages have reported increased anxiety and fear of the unknown as it related to the pandemic, a fear of infection, and a fear of one’s own mortality [
28]. This increased fear among the general population can and has led to discrimination against people perceived to be “at fault” and deterioration of mental health [
28].
1.4. Theoretical Framework
Rogers originally proposed the Protection Motivation Theory (PMT) to describe factors that influence a person’s intentions to engage in protective behaviors: the degree of potential harmfulness, the likelihood of the event happening, and the efficacy of a protective response [
29]. Eberhardt and Ling built upon Rogers’s framework by revising the labeling of key concepts to threat appraisal and coping appraisal and adding the factor of knowledge/experience as a predictor of threat and coping appraisal [
30]. Together, these factors influence behavioral intention and, ultimately, behavior. Eberhardt and Ling applied this framework in their study to predict COVID-19 vaccination intention and vaccine behavior and found that individuals who had higher perceived severity and higher perceived susceptibility had higher intentions of receiving the vaccination when available to them [
30].
While existing literature highlights COVID-19 protective behaviors and concerns, there is little information regarding the direct relationship between these concerns about the pandemic and feelings of loneliness and depression. This research aims to bridge this gap in the literature by contributing to a more well-rounded understanding of the impacts the pandemic has on loneliness and depression. While PMT has health behaviors as the outcome, we extend this framework to predict depression and loneliness as outcomes (see
Figure 1). We also add to the Protection Motivation Theory Framework by explicitly including demographic factors. In our study we tested the following hypotheses:
Hypothesis 1. Being at high risk for COVID-19-related death or complications will be associated with higher threat appraisal.
Hypothesis 2. Being at high risk for COVID-19-related death or complications will be associated with a lower coping appraisal.
Hypothesis 3. Higher threat appraisal and higher coping appraisal will be associated with engaging in protective health behaviors.
Hypothesis 4. Protective health behaviors will mediate the relationships between threat appraisal and depressive symptoms and loneliness, and between coping appraisal and depressive symptoms and loneliness.
This study adds to the knowledge base about the impact of COVID-19 on social sustainability and does so through the lens of the Protection Motivation Theory. Furthermore, this application extends the Protection Motivation Theory by taking the behavioral outcomes (where PMT traditionally ends) and using those behaviors to predict the well-being outcomes of depression and loneliness (motivated, in part, by our focus on social sustainability). Using a national sample, this manuscript contributes to overall knowledge and understanding of the impact of the COVID-19 pandemic on middle-aged and older adults in the United States.
2. Materials and Methods
This study used data from the Health and Retirement Study, a longitudinal study of non-institutional adults over the age of 50 in the US (excluding Hawaii and Alaska); “The HRS (Health and Retirement Study) is sponsored by the National Institute on Aging (grant number NIA U01AG009740) and is conducted by the University of Michigan.” [
31]. Human subjects IRB approval was obtained by researchers at the University of Michigan, and IRB approval was also obtained for use of the publicly available data used in this study (Miami University, 01911e). When COVID-19 resulted in closures, mask mandates, and other protective measures, COVID-19 questions were added to the Psychosocial and Lifestyle Questionnaire. The 2020 COVID-19 project collected data from March 2020–May 2021 from approximately 25% of the HRS sample. In order to be included in this sample, respondents had to respond to the COVID-19 module questions (and not have a proxy respondent), be over the age of 50, and have complete data for the study variables—this resulted in a final sample size of 2145.
2.1. Measures
Depressive Symptoms (outcome) was measured using eight items (e.g., depressed, sad, could not get going) that HRS selected from the Centers for Epidemiologic Studies-Depression Scale [
32]. The CES-D has high internal item consistency (about 0.85), test-retest reliability, discriminant validity, and convergent validity [
32]. For HRS, items were asked as dichotomous questions (1 = yes, experienced “much of the time during the past week”; 0 = no); responses were summed to form a scale (higher = more symptoms; Cronbach’s alpha = 0.81). Loneliness (outcome) was assessed using the 11-item Loneliness index [
33]. These items (e.g., frequency of feeling isolated, alone, lacking companionship) were derived from the 20-item Revised UCLA Loneliness Scale, and asked respondents how much of the time they felt each feeling (1 = often, 2 = some of the time, 3 = hardly ever or never) [
34]. Psychometric evaluation indicates that the 20-item scale has high internal inconsistency (Cronbach’s alpha ranging 0.89 and 0.94) and strong validity, as measured by convergent, construct and confirmatory factor analysis approaches [
34]. The four positive-valence items were reverse coded so that higher scores were indicative of more frequent feelings of loneliness; responses were averaged across all 11 items; those missing more than five items were coded as missing [
33].
Protective Motivation Theory measures (key predictors). Knowledge/Experience was assessed by a high risk for COVID-19 complications and death (1 = have diabetes, cancer, lung disease, heart problem, or stroke [
4]. While the CDC includes other risk factors for complications (e.g., overweight and obesity, physical inactivity, mental health conditions, pregnancy, sickle cell disease, smoking, substance use disorders, tuberculosis) we chose to focus on the most prevalent chronic disease conditions. Select social determinants of COVID-19 complications (e.g., age, education, race, ethnicity) were included as control variables in the model.
Threat appraisal was assessed with two variables: level of concern about COVID-19 (1 = least concerned, to 10 = most concerned) and COVID-19 death (i.e., knowing someone who has died from COVID-19; 1 = yes, 0 = no). Two self-ratings of the amount of control these days over Health and Social Life (0 = no control at all, 10 = very much control) were used to assess coping appraisal. For preventative health behaviors, three measures of behaviors since COVID-19 began were used: mask-wearing when around other people outside their home, more frequent handwashing with soap, and physical distancing from others when leaving one’s home; all three of these measures were dichotomous (1 = always, 0 = sometimes, never, blank).
Sociodemographics. Age was measured in years and was centered by subtracting 51 from all responses (minimum age for eligibility for this study). Sex was coded as 1 = female and 0 = male, and marital status was coded as 1 = married, 0 = all others (single, separated, divorced, widowed, and never married). Education (0–17+ years) was centered around the sample mean of 13.42 for the statistical analyses. For race/ethnicity, the HRS study asked separate questions for race (White, Black, Other race) and ethnicity (Hispanic/Latino or non-Hispanic/Latino). For this study, responses were combined to create the following groups: Black non-Hispanic, Other Race non-Hispanic, Hispanic, and White non-Hispanic (reference group).
2.2. Data Analysis
Descriptive statistics were run for all study variables as an initial step. Bivariate tests (chi-square tests and independent samples
t-tests) were also conducted to test for gender differences in responses to the study variables. To test the study’s hypotheses, data were analyzed using Structural Equation Modeling with SPSS AMOS 27 software (maximum likelihood estimation). Based on the examination of model indices, a decision was made to correlate the error terms for threat appraisal, coping appraisal, and two of the health behaviors. Due to large standardized residuals (i.e., greater than 2.0) with four other predictors, a variable was also removed from the model (1 = reduced contact with family/friends, 0 = no). The model was then re-run; model fit statistics improved, and the standardized residuals indicate that all remaining relationships were less than 2.0 (see
Table 1). The chi-square goodness of fit for the final model was not statistically significant, χ
2(31,
N = 2145) = 35.37,
p = 0.27 (relative χ2 = 1.14); which is indicative of acceptable model fit [
35]. Furthermore, four model fit indices supported the model: Steiger-Lind RMSEA = 0.008 [90% CI: 0.000, 0.019], Standardized RMR = 0.008, Bentler CFI = 0.999, and TLI = 0.996 [
36,
37].
3. Results
The majority of the sample were female, married, and White non-Hispanic. The average age was 69.06 (
SD = 9.92; range 51–99), and about half had at least one year of education post-high school (see
Table 2 and
Table 3). Over half of the sample had at least one comorbid health condition, and the mean level of concern about COVID-19 was 7.43 (
SD = 2.55). Similarly, the mean level of perceived control over one’s health was 7.40 (
SD = 2.22) and the mean level of perceived control over one’s social life was 7.52 (
SD = 2.51).
Compared to males, females were less likely to be married, and less likely to be at high risk for COVID-19 complications. However, females were more likely to know someone who had died from COVID-19, to always wear a mask in public, to engage in more frequent handwashing, and to engage in physical distancing. Females also reported higher mean levels of COVID-19 concern and depression, compared to males.
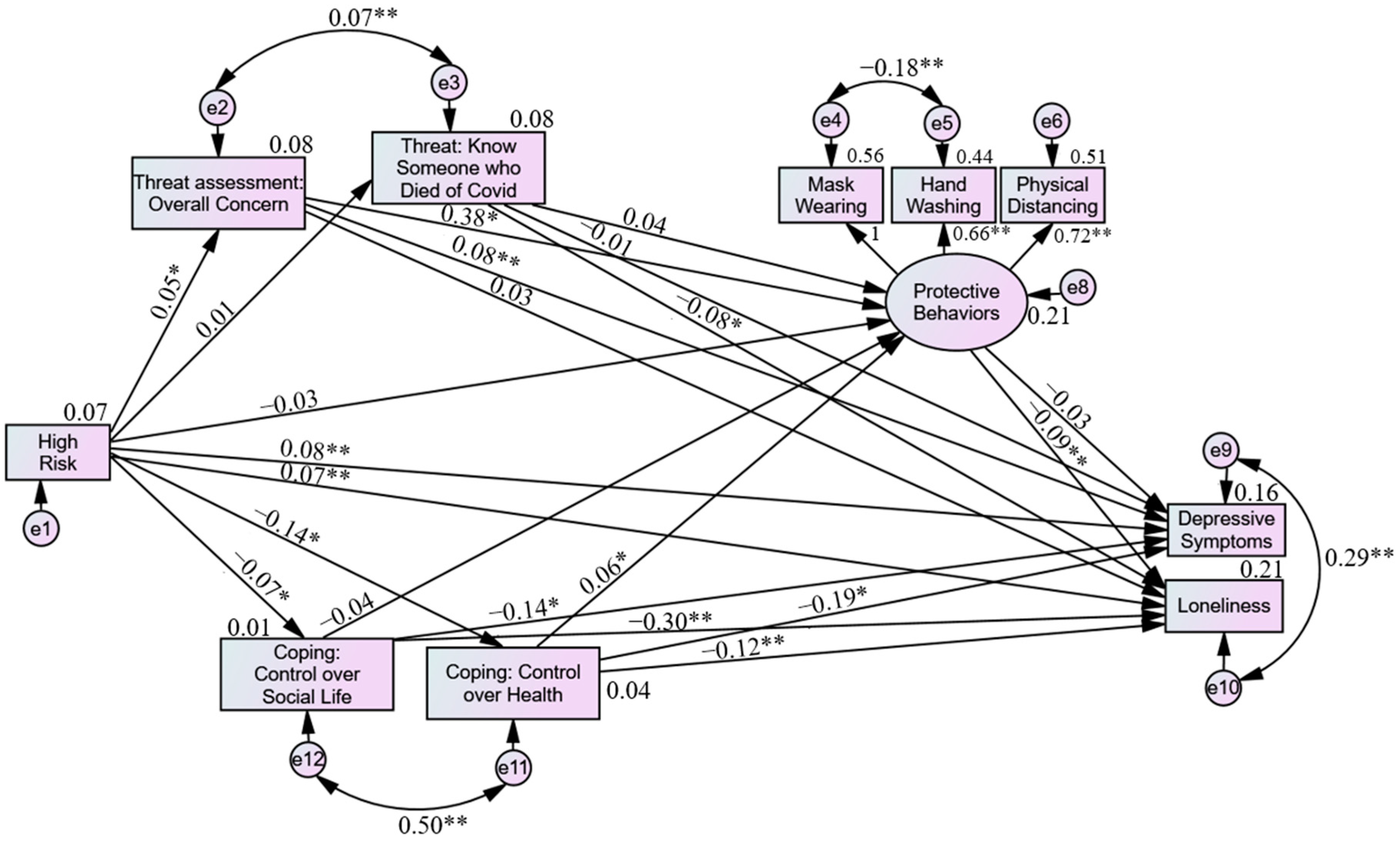
Figure 1.
Structural Equation Model Predicting Loneliness and Depressive Symptoms. Note. Model controls for age, education, race, ethnicity, and marital status (results not shown). * p < 0.05. ** p < 0.01.
Figure 1.
Structural Equation Model Predicting Loneliness and Depressive Symptoms. Note. Model controls for age, education, race, ethnicity, and marital status (results not shown). * p < 0.05. ** p < 0.01.
Results of the structural equation model (see
Figure 1) indicate that being at higher risk for COVID-19 complications or death and higher overall concern about COVID-19 were associated with more depressive symptoms, while higher coping health and social life appraisals were associated with fewer depressive symptoms. Protective health behaviors and knowing someone who died from COVID-19 did not have significant direct effects on depression. The following sociodemographic variables were significantly significant predictors of depressive symptoms: Hispanic ethnicity (β = 0.06), younger age (β = −0.06), lower education (β = −0.10), female sex (β = 0.10), and not being married (β = −0.15), all
p < 0.01. Examination of indirect effects and total effects suggest that protective health behaviors mediated the relationship between threat appraisals and coping appraisals and depressive symptoms, albeit in a very minor way.
For the outcome of loneliness, being at higher risk for COVID-19 complications and death, lower perceived control over one’s health and social life, fewer protective health behaviors, and not knowing anyone who had died from COVID-19 were statistically significant predictors (all p < 0.01). For sociodemographics, younger age (β = −0.14), lower education (β = −0.07), male sex (β = −0.06), and not being married (β = −0.17, p < 0.01) were associated with more loneliness (all p < 0.01). Level of COVID-19 concern, and race/ethnicity were not significant predictors of loneliness. The standardized indirect and total effects suggest that the relationships between threat and coping appraisals and loneliness were partially explained by protective health behaviors, but the effects were small.
Loneliness and depressive symptoms were positively correlated, as were the level of concerns about COVID-19 and knowing someone who had died of COVID-19 and perceived control over one’s health and social life. The protective health behavior of more frequent hand washing was negatively correlated with mask-wearing. The sociodemographic variables were also correlated with each other and the study outcomes (see
Table 4).
4. Discussion
This analysis presented several factors and interactions that influenced overall feelings of depression and loneliness during COVID-19 in middle-aged and older adults. Overall, the hypotheses presented for this analysis were supported by the results. Being at a higher risk for COVID-19 complications and death was associated with higher threat appraisal (higher concern about COVID-19; hypothesis 1). Additionally, being at higher risk was associated with lower coping appraisals (hypothesis 2). Higher threat appraisal (COVID-19 concern) and coping (health control) were associated with higher engagement in protective behaviors (hypothesis 3). Protective health behaviors reduced the strength of the relationships between threat and coping, and the outcomes of loneliness and depressive symptoms (hypothesis 4), but the effects were negligible. The study results provide partial support for the Protection Motivation Theory, as threat assessment (COVID-19 concern) and coping efficacy (perceived control over health) both were positively correlated with more protective behaviors, while high-risk status was not correlated with protective behaviors.
Higher concern about the pandemic was associated with more depressive symptoms, and those with higher levels of concern were more likely to engage in protective health behaviors (physical distancing, more frequent hand washing, mask-wearing) than those with lower levels of COVID-19 concern. This study found that more frequent hand washing was negatively correlated with always wearing a mask while out in public (e.g., in shops). It is likely that people who are more likely to engage in protective health behaviors (e.g., mask-wearing) are more likely to already be engaged in frequent hand washing with soap, so these individuals may not say that they have increased their handwashing due to the COVID-19 pandemic. There was no direct significant relationship between overall COVID-19 concern and feelings of loneliness among participants. While respondents were asked about their feelings of loneliness during the pandemic, the questions themselves were not COVID-19 specific. Nevertheless, it is likely that COVID-19 acted as both a cause and a barrier for the internal and external variables affecting feelings of loneliness in participants.
Other factors that increased feelings of depression and loneliness among respondents included lower age, not being married, and lower education status. Younger respondents were more likely to have high scores on the depression index and report feelings of loneliness, suggesting this age group may have had significant impacts on their social lives during the pandemic. It is possible that younger individuals had busier social schedules and more interactions with people, which resulted in a more noticeable day-to-day difference in their social lives compared to older adults. With isolation and loneliness being common issues among older adults before the pandemic, it may be difficult to gauge the specific impact that the pandemic has had on loneliness in older adults. The current analysis supports the need for further research specifically looking at the changes in loneliness in middle-aged and older adults during the COVID-19 pandemic.
Individuals who knew someone who died of COVID-19 reported lower feelings of loneliness compared to individuals who did not know someone who died. It is possible that people who knew someone who passed away from COVID-19 knew more people in general or had strong support systems in response to the death. More research is needed to understand how the experience of mass death, in the context of widespread events such as the COVID-19 pandemic, may contribute to a higher sense of community engagement and lower feelings of loneliness among people who are grieving. It is possible that the widespread experience related to death by COVID-19 decreased loneliness in this population due to shared experiences and support. Additionally, despite various regulations changing funeral practices in the United States, widespread adaptations of funeral practices have been adopted including more personalized and smaller in-person events, various cremation and ritual adaptations, live-streamed and virtual funeral services, and increased virtual social support such as social media interaction or virtual socialization to assist with the grieving process [
38,
39]. These adaptations may play a part in improving feelings of loneliness in middle-aged and older adults who knew people who died as a result of COVID-19.
Most notably, having lower perceived control over one’s health and social life was associated with higher ratings of depression and loneliness among participants. This demonstrates the influence that self-efficacy has on mental well-being and is consistent with literature suggesting that self-efficacy is the most influential factor in behavioral intention within the PMT [
39]. Williams and colleagues applied the PMT to predict social distancing behaviors in a simulated pandemic event and found that response efficacy and self-efficacy were the primary predictors of intention to engage in social distancing behaviors [
40]. Sholz and Freund also demonstrated that response-efficacy and self-efficacy were the most influential predictors for intention and engagement in protective behaviors in response to COVID-19 [
41]. Marceron and Roherbeck discussed the role that self-efficacy plays in emergency preparedness and suggested that self-efficacy and threat operate together to motivate individuals to take precautionary steps in preparing for natural and man-made disasters [
42]. In a study conducted by Zhou and colleagues, higher levels of self-efficacy were associated with higher engagement in active coping behaviors and fewer mental health problems during the COVID-19 pandemic [
43]. Unfortunately, self-efficacy was found to significantly drop during early COVID-19 lockdown measures compared to prior to the pandemic in adults between the ages of 19-80 [
44], suggesting that while self-efficacy is an important factor for mental well-being it was significantly impacted during the pandemic.
With the support for the importance that self-efficacy plays in ratings of depression and loneliness, future interventions for the impacts of the COVID-19 pandemic should consider influencing the self-efficacy of participants to improve mental health and behavior. Graf and colleagues presented several factors that can influence self-efficacy based on Bandura’s Social Cognitive Theory including social modeling, persuasive language, and psychological cues [
45,
46]. Additionally, emotional state can negatively impact feelings of self-efficacy in individuals who are depressed, stressed, or uncertain [
45]. Taylor and colleagues applied a mindfulness-based intervention to improve coping self-efficacy in individuals and found that this intervention, which included mindfulness meditations, reflective journaling, and group discussions, significantly improved ratings of stress, isolation, and coping self-efficacy [
47]. In the development of the Coping Self-Efficacy Scale, Chesney and colleagues suggest that measures of self-efficacy must be tailored to the specific activity or influential event [
48]. More research is necessary to understand the measures of self-efficacy as they relate to the COVID-19 pandemic. A variety of factors could have impacted individual self-efficacy during the COVID-19 pandemic, including ageism in protective measures and language, misinformation, and the technological shift to telehealth and virtual socialization. Future COVID-19 research and interventions should focus on factors that could improve coping self-efficacy, such as social modeling, the language used in behavioral promotion, and individual stress management. While feelings and messages of fear may influence engagement in protective measures, this analysis suggests that coping self-efficacy is an important factor that may be negatively impacted by fear and stress-inducing language. In future responses to pandemic-level events, behavioral interventions should focus on bolstering the self-efficacy of the individual rather than inducing fear-related protective behaviors.
Study Limitations and Strengths
This study has some limitations, including those related to sampling, measurement, and study design. While this study uses a national sample, the sample percentage of Hispanic respondents precluded any type of subgroup analyses for ethnicity, which ignores potentially important differences. In terms of measurement, COVID-19 protective behaviors (e.g., mask-wearing, frequency of handwashing, physical distancing) could be studied in a more nuanced way. For example, rather than simply comparing the frequency of mask-wearing in public (always, sometimes, never), additional information about the context (e.g., mandates vs. voluntary protective measures, mask characteristics, situational factors associated with wearing masks) would allow for a greater understanding of these health behaviors. This provides a promising direction for future qualitative research studies. It was also not possible to include some measures (e.g., vaccination status, COVID-19 diagnosis, severe complications from COVID-19) due to insufficient variability in responses during the 2020 wave of the HRS. Data are currently being collected as part of the 2021 HRS COVID-19 project, and this has the potential for researchers to examine how responses changed over time during the pandemic; however, the current study is cross-sectional, and therefore it is not possible to determine causality.
Other measures related to COVID-19 were excluded, as being beyond the scope of the study. These include the technological influence on social connectedness, telehealth, and health information seeking. Previous research has found that the technological push during the pandemic has led to an exclusion of older adults and both physical and mental health impacts [
11,
13,
14].
Despite its limitations, this study also has many strengths, including its theoretical grounding, multiple measures, statistical approach, and large sample size. The Protection Motivation Theory Framework provided structured and supported directions for analysis, and multiple measures were used to assess its key constructs of threat and coping appraisals, as opposed to single measure items. Outcome measures were assessed using a standardized scale and index for depression and loneliness, respectively. The structural equation modeling approach facilitated the examination of the relationships between PMT constructs. Finally, the sample for this analysis was a national sample with a large number of participants.




{kind=link}