
Incentive Mechanism Design in Collaborative Management of Public Health Emergencies



Abstract
:1. Introduction
2. Literature Review
2.1. Emergency Management
2.2. Public Health Emergencies
2.2.1. Impact of Public Health Emergencies
2.2.2. Emergency Management of Public Health Emergencies
2.3. Collaborative Management
2.4. Summary
3. Model Formulation and Analysis
3.1. Decentralized Decision Model without GPI ()
3.2. Decentralized Decision Model with GPI ()
3.3. Collaborative Decision Model with GPI ()
3.3.1. Centralized Decision Model of PES
3.3.2. Decentralized Decision Model of PES
3.3.3. Collaborative Decision Model of PES
3.4. Discussions and Comparisons of Analytical Results
- (1)
- the equilibrium EMEs under the decentralized decision model with GPI are higher than those under the decentralized decision model without GPI, and the equilibrium EMEs under the collaborative decision model with GPI are higher than those under the decentralized decision model without GPI when condition 1 holds. Hereinto, condition 1 is the following inequality: .
- (2)
- the equilibrium comprehensive EME of the PES under the decentralized decision model with GPI are higher than those under the decentralized decision model without GPI, and the equilibrium comprehensive EME of the PES under the collaborative decision model with GPI are higher than those under the decentralized decision model without GPI when condition 1 holds.
- (3)
- the equilibrium effect of unit EME under the decentralized decision model with GPI are higher than those under the decentralized decision model without GPI, and the equilibrium effect of unit EME under the collaborative decision model with GPI are higher than those under the decentralized decision model without GPI when condition 1 holds.
4. Numerical and Sensitivity Analyses
4.1. Numerical Analysis
- (1)
- Comparing the decentralized decision scenario without GPI and that with GPI, the equilibrium EMEs of all medical institutions under the decentralized decision scenario with GPI were higher than those without GPI; the equilibrium utilities of all medical institutions, government departments, and PES under the decentralized decision scenario with GPI, were higher than those without GPI.
- (2)
- Comparing the collaborative decision scenario with GPI and decentralized decision scenario with GPI, the equilibrium EMEs of all medical institutions under the collaborative decision scenario with GPI were higher than those under the decentralized decision scenario with GPI; the equilibrium utilities of all medical institutions, government departments, and PES under the collaborative decision scenario with GPI were higher than those under the decentralized decision scenario with GPI.
- (3)
- Comparing the collaborative decision scenario with GPI and decentralized decision scenario with GPI, the transfer payment coefficients of government department under the collaborative decision scenario with GPI were higher than those under the decentralized decision scenario with GPI.
4.2. Sensitivity Analysis
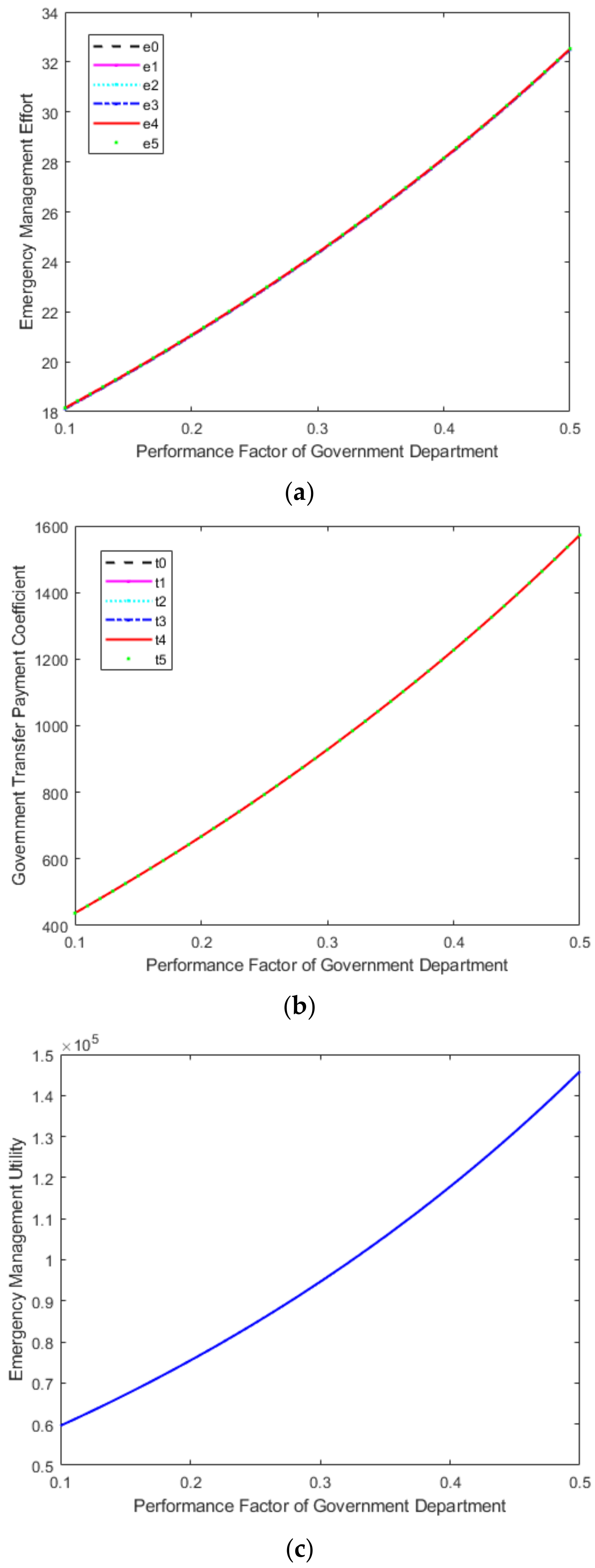
- (1)
- the sensitivity analysis results of performance factor of government department () are shown in Figure 1. As the performance factor of government department increased, the equilibrium EMEs of all medical institutions increased, the equilibrium transfer payment coefficients of the government department for medical institutions increased, and the equilibrium utility of PES increased.
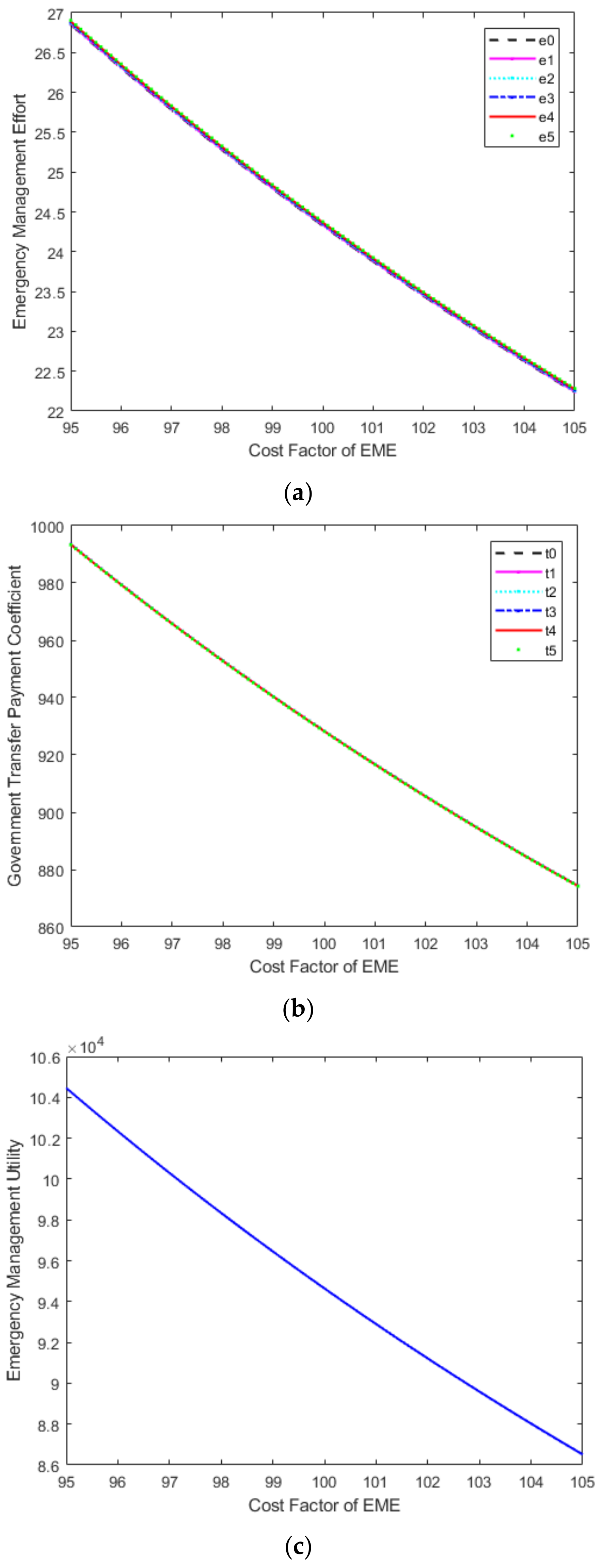
- (2)
- the sensitivity analysis results of the cost factor of the EME level () are shown in Figure 2. As the cost factor of the EME level increased, the equilibrium EMEs of all medical institutions decreased, the equilibrium transfer payment coefficients of the government department for medical institutions decreased, and the equilibrium utility of PES decreased.
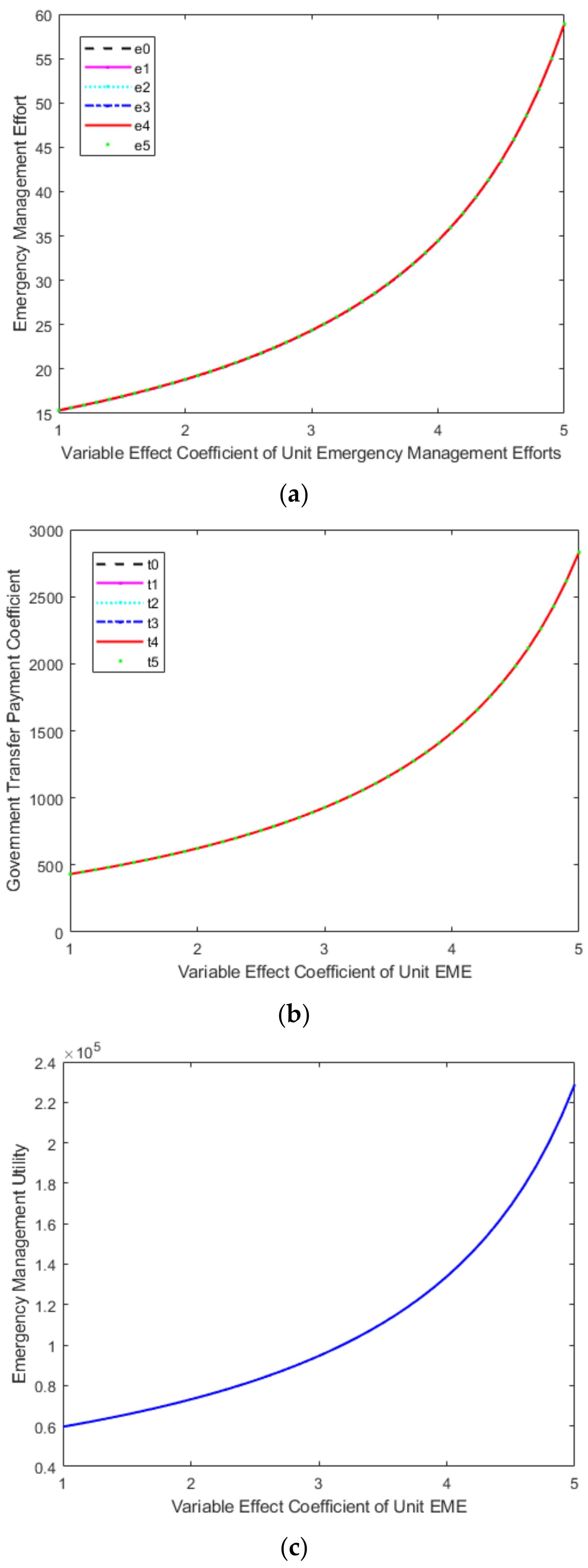
- (3)
- the sensitivity analysis results of variable effect coefficient of unit EME () are shown in Figure 3. As the variable effect coefficient of unit emergency management increased, the equilibrium EMEs of all medical institutions increased, the equilibrium transfer payment coefficients of the government department for medical institutions increased, and the equilibrium utility of PES increased.
5. Managerial Insights and Policy Implications
- (1)
- The government departments should use the “carrot + stick” type of public governance policy to incentivize medical institutions to strengthen their individual emergency management capabilities, thereby ultimately improving the overall emergency management effectiveness of the PES. For instance, the central government of China and the local government of Hunan province successively introduced a series of incentive policies and measures since February 2020, such as “Notice on several measures to improve the working conditions of frontline medical personnel and effectively care for the physical and mental health of medical personnel”; “Notice on several measures to further stimulate and care for the frontline staff of epidemic prevention and control”; and “Notice on the implementation of personnel and talent inclination policy measures for the frontline professionals and technicians of the prevention and control of the COVID-19 epidemic”, etc. These detailed incentive policies and measures include rapid promotion and advancement, rapid entry into the party for recognition and merit, rapid entry into the cadre (from contract workers to regular workers), and material incentives and subsidies among others. At the same time, incentive and accountability complement each other. Medical personnel who neglect their duties during the war against the epidemic should be strictly held accountable in accordance with relevant regulations, mainly including dismissal, warning, demerit, and other types of accountability measures.
- (2)
- Under the government’s public governance policy incentive, the collaborative decision mode should be adopted by the PES, which would help to improve the overall emergency management efficiency of the PES. In order to integrate the national epidemic and policy information resources, the national government should establish and improve the information sharing platform of the national public health system. This one-stop information service platform could maximize the linked emergency management capabilities of the government and medical institutions and promote the flattening of the organizational structure of the PES. After a public health emergency occurs, information can be directly transmitted and communicated within the PES based on this platform. This will enable medical institutions to provide timely and accurate information for research and judgment, rapidly transfer it to government departments, and quickly and efficiently formulate emergency policies based on the information.
- (3)
- In the PES, the superior government should enhance the performance assessment of emergency management for relevant government departments (i.e., improve the performance factor of government department), which would help to improve the transfer payment of the government department for medical institutions, enhance the emergency management efforts of medical institutions, and improve the overall emergency management efficiency of the PES. In order to improve the enthusiasm and initiative of relevant government departments in emergency management of public health emergencies, the assessment of public health, medical care, and other regular livelihood indicators could be added to the regular performance assessment mechanism of the relevant government. Furthermore, the emergency management of public health emergencies and other relevant indicators that show the responsibility and commitment of the government should be included in the “one vote veto” system, so as to curb the relevant government department’s various inaction behaviors in preventing and responding to public health emergencies and enhance their motivations to implement the policies from the higher government.
- (4)
- In the PES, medical institutions should reduce the costs of emergency management efforts (i.e., the cost factor of the emergency management effort level), which would help to improve the transfer payment of the government department for medical institutions, enhance the emergency management efforts of medical institutions, and improve the overall emergency management efficiency of the PES. In this COVID-19 pandemic, the medical institutions should flexibly adjust the medical materials procurement process in conjunction with the epidemic control situation, reasonably control procurement sources, dynamically manage procurement funds, strictly supervise procurement processes, reasonably use epidemic prevention and control resources, and effectively avoid the waste of medical resources. Furthermore, in large-scale, high-volume, population-based screening, the PES can use mixed-sample nucleic acid testing instead of single-sample nucleic acid testing according to the instructions of the epidemic prevention headquarters. This will improve the detection efficiency and achieve multi-screening, early detection, early isolation, early treatment and timely infection control, and thus effectively reducing emergency management costs.
- (5)
- In the PES, the government department and medical institutions should enhance the effectiveness of emergency management effort (i.e., the variable effect coefficient of unit emergency management effort), which would help to enhance the emergency management efforts of medical institutions and improve the overall emergency management efficiency of the PES. In the epidemiological investigation, the government department should make full use of technical means and big data information support to identify all close contacts, sub-close contacts, and general contacts of infected persons and other key populations quickly and accurately and catch the source of epidemic transmission precisely. Furthermore, based on the number of infected persons and trajectory investigation, medical institutions should propose the delineation of sealing control areas, control areas and prevention areas, report to the epidemic prevention and control command for approval and announcement, and propose dynamic adjustments according to the progress of epidemic prevention and control. Besides, the government department should delineate prevention and control areas scientifically, implement classification management measures more precisely, and curb the spread of the epidemic in the community effectively. These measures would effectively achieve the maximum prevention and control effect at the minimum cost and minimize the impact of the epidemic on economic and social development. Moreover, the government department should change the scope of nucleic acid testing from “full personnel” to “regional personnel” and scientifically define the size of the region according to the objective needs of epidemic prevention and control. Medical institutions could use nucleic acid testing in conjunction with antigen testing to enhance the quality control of nucleic acid testing, improve the effectiveness of accurate testing, and achieve the accurate prevention and control of epidemics.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 13 April 2022).
- Wei, X.; Li, L.; Zhang, F. The impact of the COVID-19 pandemic on socio-economic and sustainability. Environ. Sci. Pollut. Res. 2021, 28, 68251–68260. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Liu, G.; Mai, T.H.T.; Li, T.T. Research on the Allocation of 3D Printing Emergency Supplies in Public Health Emergencies. Front. Public Health 2021, 9, 657276. [Google Scholar] [CrossRef] [PubMed]
- Cao, D. Xi Urges Redoubling Contagion Fight. 2020. Available online: https://www.chinadaily.com.cn/a/202002/11/WS5e41adefa31012821727670d.html (accessed on 11 April 2020).
- Abubakar, I.; Dalglish, S.L.; Ihekweazu, A.C.; Bolu, O.; Aliyu, S.H. Lessons from co-production of evidence and policy in Nigeria’s COVID-19 response. BMJ Glob. Health 2021, 6, e004793. [Google Scholar] [CrossRef] [PubMed]
- Dalglish, S.L. COVID-19 gives the lie to global health expertise. Lancet 2020, 395, 1189. [Google Scholar] [CrossRef]
- Lal, A.; Erondu, N.A.; Heymann, D.L.; Gitahi, G.; Yates, R. Fragmented health systems in COVID-19: Rectifying the misalignment between global health security and universal health coverage. Lancet 2021, 397, 61–67. [Google Scholar] [CrossRef]
- Kang, L.; Li, Y.; Hu, S.; Chen, M.; Yang, C.; Yang, B.X.; Wang, Y.; Hu, J.; Lai, J.; Ma, X.; et al. The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. Lancet Psychiatry 2020, 7, e14. [Google Scholar] [CrossRef]
- Zhang, X.; Yang, S. “A community system”: A critical foundation for the epidemic prevention and control of SARS-CoV-2. Int. J. Health Plan. Manag. 2020, 35, 1246–1249. [Google Scholar] [CrossRef]
- Rangachari, P.; Woods, J.L. Preserving Organizational Resilience, Patient Safety, and Staff Retention during COVID-19 Requires a Holistic Consideration of the Psychological Safety of Healthcare Workers. Int. J. Environ. Res. Public Health 2020, 17, 4267. [Google Scholar] [CrossRef]
- Sheather, J.; Slattery, D. The great resignation—How do we support and retain staff already stretched to their limit? BMJ 2021, 375, n2533. [Google Scholar] [CrossRef]
- Shader, R.I.; Schwartz, A.J. Management of Reactions to Disaster. Soc. Work 1966, 11, 99–104. [Google Scholar] [CrossRef]
- Blanchard, B.W.; Canton, L.C.; Cwiak, C.L.; Goss, K.C.; McEntire, D.A.; Newsome, L.; Selves, M.D.; Sorchik, E.A.; Stenson, K.; Turner, J.E.; et al. Principles of Emergency Management Supplement; Federal Emergency Management Agency: Washington, DC, USA, 2007. [CrossRef]
- Huang, D.; Wang, S.; Liu, Z. A systematic review of prediction methods for emergency management. Int. J. Disaster Risk Reduct. 2021, 62, 102412. [Google Scholar] [CrossRef]
- Shareef, M.A.; Dwivedi, Y.K.; Mahmud, R.; Wright, A.; Rahman, M.M.; Kizgin, H.; Rana, N.P. Disaster management in Bangladesh: Developing an effective emergency supply chain network. Ann. Oper. Res. 2019, 283, 1463–1487. [Google Scholar] [CrossRef]
- Resodihardjo, S.L.; Van Genugten, M.; Ruiter, M.N. A theoretical exploration of resilience and effectiveness requirements’ compatibility in formal and permanent emergency networks. Saf. Sci. 2018, 101, 164–172. [Google Scholar] [CrossRef]
- Huang, H.-C.; Gao, H.-F. Game Analysis of Behavior Choice on Construction of the Social Emergency Rescue System Between Government and Enterprises. IEEE Access 2020, 8, 149595–149601. [Google Scholar] [CrossRef]
- Fan, B.; Liu, R.; Huang, K.; Zhu, Y. Embeddedness in cross-agency collaboration and emergency management capability: Evidence from Shanghai’s urban contingency plans. Gov. Inf. Q. 2019, 36, 101395. [Google Scholar] [CrossRef]
- Shen, Z.M.; Sun, Y. Strengthening supply chain resilience during COVID-19: A case study of JD.com. J. Oper. Manag. 2021, 1–25. [Google Scholar] [CrossRef]
- Meng, Q. A Study on the Urban Emergency Management System Based on the Internet of Things. In Proceedings of the International Conference on Management Science and Engineering Management, Ontario, ON, Canada, 5–8 August 2019; Springer: Cham, Switzerland, 2019; pp. 645–655. [Google Scholar]
- Jia, D.; Wu, Z. Intelligent Evaluation System of Government Emergency Management Based on BP Neural Network. IEEE Access 2020, 8, 199646–199653. [Google Scholar] [CrossRef]
- Chen, Y.; Zhao, X.; Rich, E.; Luna-Reyes, L.F. Decision Models and Group Decision Support Systems for Emergency Management and City Resilience. In Research Anthology on Decision Support Systems and Decision Management in Healthcare, Business, and Engineering; IGI Global: Hershey, PA, USA, 2021; pp. 723–740. [Google Scholar]
- Ceschia, S.; Schaerf, A. Modeling and solving the dynamic patient admission scheduling problem under uncertainty. Artif. Intell. Med. 2012, 56, 199–205. [Google Scholar] [CrossRef]
- Guido, R.; Solina, V.; Mirabelli, G.; Conforti, D. Offline Patient Admission, Room and Surgery Scheduling Problems. In New Trends in Emerging Complex Real Life Problems; Daniele, P., Scrimali, L., Eds.; AIRO Springer Series; Springer: Cham, Switzerland, 2018; Volume 1, pp. 275–283. [Google Scholar] [CrossRef]
- Bastos, L.S.; Marchesi, J.F.; Hamacher, S.; Fleck, J.L. A mixed integer programming approach to the patient admission scheduling problem. Eur. J. Oper. Res. 2019, 273, 831–840. [Google Scholar] [CrossRef]
- Ye, J. The Role of Health Technology and Informatics in a Global Public Health Emergency: Practices and Implications From the COVID-19 Pandemic. JMIR Med. Inform. 2020, 8, e19866. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, X.; He, J. Challenges to the system of reserve medical supplies for public health emergencies: Reflections on the outbreak of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) epidemic in China. Biosci. Trends 2020, 14, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Kremer, M.; Levin, J.; Snyder, C.M. Designing Advance Market Commitments for New Vaccines. Manag. Sci. 2022, 1–29. [Google Scholar] [CrossRef]
- Breugem, T.; Van Wassenhove, L.N. The Price of Imposing Vertical Equity Through Asymmetric Outcome Constraints. Manag. Sci. 2022, 1–17. [Google Scholar] [CrossRef]
- Li, M.; Zhao, T.; Huang, E.; Li, J. How does a public health emergency motivate People’s impulsive consumption? An empirical study during the COVID-19 outbreak in China. Int. J. Environ. Res. Public Health 2020, 17, 5019. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Shen, Q.; Li, Z.; Chen, S. Stimulating Consumption at Low Budget: Evidence from a Large-Scale Policy Experiment Amid the COVID-19 Pandemic. Manag. Sci. 2021, 67, 7291–7307. [Google Scholar] [CrossRef]
- Ru, H.; Yang, E.; Zou, K. Combating the COVID-19 Pandemic: The Role of the SARS Imprint. Manag. Sci. 2021, 67, 5606–5615. [Google Scholar] [CrossRef]
- Chiossi, S.; Tsolova, S.; Ciotti, M. Assessing public health emergency preparedness: A scoping review on recent tools and methods. Int. J. Disaster Risk Reduct. 2021, 56, 102104. [Google Scholar] [CrossRef]
- Mao, Z.; Zou, Q.; Yao, H.; Wu, J. The application framework of big data technology in the COVID-19 epidemic emergency management in local government—A case study of Hainan Province, China. BMC Public Health 2021, 21, 147. [Google Scholar] [CrossRef]
- Wang, J.; Yuan, B.; Li, Z. Evaluation of Public Health Emergency Management in China: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 3478. [Google Scholar] [CrossRef]
- Troisi, R.; Alfano, G. Is regional emergency management key to containing COVID-19? A comparison between the regional Italian models of Emilia-Romagna and Veneto. Int. J. Public Sect. Manag. 2021, 35, 195–210. [Google Scholar] [CrossRef]
- Guo, D.; Zhu, Y.; Yin, W. OSCAR: A framework to integrate spatial computing ability and data aggregation for emergency management of public health. GeoInformatica 2018, 22, 383–410. [Google Scholar] [CrossRef]
- Feng, Y.; Pan, Z. Optimization of Remote Public Medical Emergency Management System with Low Delay Based on Internet of Things. J. Health Eng. 2021, 2021, 5570500. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Gan, W.; Li, Z. Application of Medical Material Inventory Model Under Deep Learning in Supply Planning of Public Emergency. IEEE Access 2021, 9, 44128–44138. [Google Scholar] [CrossRef]
- Margherita, A.; Elia, G.; Klein, M. Managing the COVID-19 emergency: A coordination framework to enhance response practices and actions. Technol. Forecast. Soc. Chang. 2021, 166, 120656. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Jung, K. Dynamics of Interorganizational Public Health Emergency Management Networks: Following the 2015 MERS Response in South Korea. Asia Pac. J. Public Health 2018, 30, 207–216. [Google Scholar] [CrossRef]
- Huang, H.; Peng, Z.; Wu, H.; Xie, Q. A big data analysis on the five dimensions of emergency management information in the early stage of COVID-19 in China. J. Chin. Gov. 2020, 5, 213–233. [Google Scholar] [CrossRef]
- Wolf-Fordham, S. Integrating Government Silos: Local Emergency Management and Public Health Department Collaboration for Emergency Planning and Response. Am. Rev. Public Adm. 2020, 50, 560–567. [Google Scholar] [CrossRef]
- Khan, Y.; O’Sullivan, T.; Brown, A.; Tracey, S.; Gibson, J.; Généreux, M.; Schwartz, B. Public health emergency prepared-ness: A framework to promote resilience. BMC Public Health 2018, 18, 1344. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Huang, Y.; Zheng, Z.-J. Leveraging the Public Health Emergency Operation Center (PHEOC) for pandemic response: Opportunities and challenges. Glob. Health J. 2020, 4, 118–120. [Google Scholar] [CrossRef]
- Fan, R.; Wang, Y.; Lin, J. Study on Multi-Agent Evolutionary Game of Emergency Management of Public Health Emergencies Based on Dynamic Rewards and Punishments. Int. J. Environ. Res. Public Health 2021, 18, 8278. [Google Scholar] [CrossRef] [PubMed]
- Diehlmann, F.; Lüttenberg, M.; Verdonck, L.; Wiens, M.; Zienau, A.; Schultmann, F. Public-private collaborations in emergency logistics: A framework based on logistical and game-theoretical concepts. Saf. Sci. 2021, 141, 105301. [Google Scholar] [CrossRef]
- Bhaskaran, S.; Krishnan, V. Effort, Revenue, and Cost Sharing Mechanisms for Collaborative New Product Development. Manag. Sci. 2009, 55, 1152–1169. [Google Scholar] [CrossRef]
- Nip, K.; Wang, C.; Wang, Z. Competitive and Cooperative Assortment Games under Markov Chain Choice Model. Prod. Oper. Manag. 2021, 31, 1033–1051. [Google Scholar] [CrossRef]
- Chen, Y.; Özer, Ö. Supply Chain Contracts That Prevent Information Leakage. Manag. Sci. 2019, 65, 5449–5956. [Google Scholar] [CrossRef]
- Balcik, B.; Silvestri, S.; Rancourt, M.È.; Laporte, G. Collaborative prepositioning network design for regional disaster response. Prod. Oper. Manag. 2019, 28, 2431–2455. [Google Scholar] [CrossRef]
- Qiu, Y.; Shi, M.; Zhao, X.; Jing, Y. System dynamics mechanism of cross-regional collaborative dispatch of emergency supplies based on multi-agent game. Complex Intell. Syst. 2021, 1–12. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Literature | Emergency Management | Collaborative Management | Impact of Public Health Emergencies | Public Health Emergency Management Methods | Governance-Driven Operational Performance/Efficiency | Impact of Government’s Performance Factor | Incentive Mechanism |
|---|---|---|---|---|---|---|---|
| [12] | √ | × | × | × | × | × | × |
| [13] | √ | × | × | × | × | × | × |
| [14] | √ | × | × | T | × | × | × |
| [15] | √ | √ | × | × | × | × | × |
| [16] | √ | √ | × | × | × | × | × |
| [17] | √ | √ | × | × | √ | √ | √ |
| [18] | √ | √ | × | × | × | × | × |
| [19] | √ | √ | × | × | √ | × | × |
| [20] | √ | √ | × | T | × | × | × |
| [21] | √ | √ | × | T | × | × | × |
| [22] | √ | √ | × | T | × | × | × |
| [23] | √ | × | × | M | × | × | × |
| [24] | √ | × | × | M | × | × | × |
| [25] | √ | × | × | M | × | × | × |
| [26] | × | × | √ | × | × | × | × |
| [27] | √ | √ | √ | M | × | × | × |
| [28] | √ | × | √ | × | × | × | × |
| [29] | √ | × | √ | × | × | × | × |
| [30] | × | × | √ | × | × | × | × |
| [31] | × | × | √ | × | × | × | × |
| [32] | × | × | √ | × | × | × | × |
| [33] | √ | √ | √ | M | × | × | × |
| [34] | √ | √ | × | T | × | × | × |
| [35] | √ | √ | × | M | × | × | × |
| [36] | √ | √ | × | M | √ | × | × |
| [37] | √ | √ | √ | T | × | × | × |
| [38] | √ | √ | √ | T | × | × | × |
| [39] | √ | √ | √ | T | × | × | × |
| [40] | √ | √ | √ | M | × | × | × |
| [41] | √ | √ | √ | M | × | × | × |
| [42] | √ | √ | √ | M | × | × | × |
| [43] | √ | √ | √ | M | × | × | × |
| [44] | √ | √ | √ | M | × | × | × |
| [45] | √ | √ | √ | M | × | × | × |
| [46] | √ | √ | √ | M | × | √ | √ |
| [47] | √ | √ | √ | M | × | √ | √ |
| [48] | × | √ | × | × | × | × | √ |
| [49] | × | √ | × | × | × | × | √ |
| [50] | × | √ | × | × | × | × | √ |
| [51] | √ | √ | × | × | × | × | √ |
| [52] | √ | √ | × | × | √ | √ | √ |
| This paper | √ | √ | √ | M | √ | √ | √ |
| Strategy | ||||
|---|---|---|---|---|
| Outcomes | ||||
| NA | ||||
| note | , | |||
| 0 | 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|---|
| 7.0 | 6.0 | 5.0 | 4.0 | 3.0 | 2.0 | |
| 20.0 | 21.0 | 22.0 | 23.0 | 24.0 | 25.0 | |
| 21.5 | 22.5 | 23.0 | 24.0 | 25.0 | 26.0 |
| Decision Variables/Outcomes | |||
|---|---|---|---|
| - | 533.73 | 928.34 | |
| - | 581.73 | 928.31 | |
| - | 629.73 | 928.28 | |
| - | 677.73 | 928.25 | |
| - | 725.73 | 928.22 | |
| - | 773.73 | 928.19 | |
| 12.58 | 19.61 | 24.33 | |
| 12.59 | 20.12 | 24.34 | |
| 12.60 | 20.62 | 24.35 | |
| 12.61 | 21.13 | 24.36 | |
| 12.62 | 21.63 | 24.37 | |
| 12.63 | 22.14 | 24.38 | |
| 7432.72 | 7405.70 | 7854.21 | |
| 7444.91 | 6807.30 | 6949.41 | |
| 7457.11 | 6136.89 | 6508.83 | |
| 7469.33 | 5394.46 | 5604.15 | |
| 7481.55 | 4580.02 | 4699.55 | |
| 7493.78 | 3693.56 | 3795.02 | |
| 27,827.14 | 58,482.32 | 59,231.03 | |
| 120,584.26 | 92,500.25 | 94,642.21 |
| Parameter | Original Value | ±Increment | Range | |
|---|---|---|---|---|
| performance factor of government department | 0.30 | 0.01 | [0.10, 0.50] | |
| cost factor of EME | 100 | 0.1 | [95, 105] | |
| variable effect coefficient of unit EME | 3.0 | 0.1 | [1.0, 5.0] | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.; Lou, X.; Wang, C.; Chen, Z. Incentive Mechanism Design in Collaborative Management of Public Health Emergencies. Sustainability 2022, 14, 7155. https://doi.org/10.3390/su14127155
Huang Y, Lou X, Wang C, Chen Z. Incentive Mechanism Design in Collaborative Management of Public Health Emergencies. Sustainability. 2022; 14(12):7155. https://doi.org/10.3390/su14127155
Chicago/Turabian StyleHuang, Yaxin, Xinyu Lou, Changqing Wang, and Zhisong Chen. 2022. "Incentive Mechanism Design in Collaborative Management of Public Health Emergencies" Sustainability 14, no. 12: 7155. https://doi.org/10.3390/su14127155
APA StyleHuang, Y., Lou, X., Wang, C., & Chen, Z. (2022). Incentive Mechanism Design in Collaborative Management of Public Health Emergencies. Sustainability, 14(12), 7155. https://doi.org/10.3390/su14127155