
Ecosystems Services and Green Infrastructure for Respiratory Health Protection: A Data Science Approach for Paraná, Brazil



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Research Methods
2.2.1. Data Acquisition and Preparation
2.2.2. Data Analysis
Basic Statistics and Multivariate Analysis
Associative Rules Mining
3. Results
3.1. Demography
3.2. Descriptive Statistics of Variables
3.2.1. Municipalities: Sizes of Population and Rural-Urban Typology
3.2.2. Basic Statistics of the Numerical Variables
3.3. Scatter Plots
3.4. Histograms
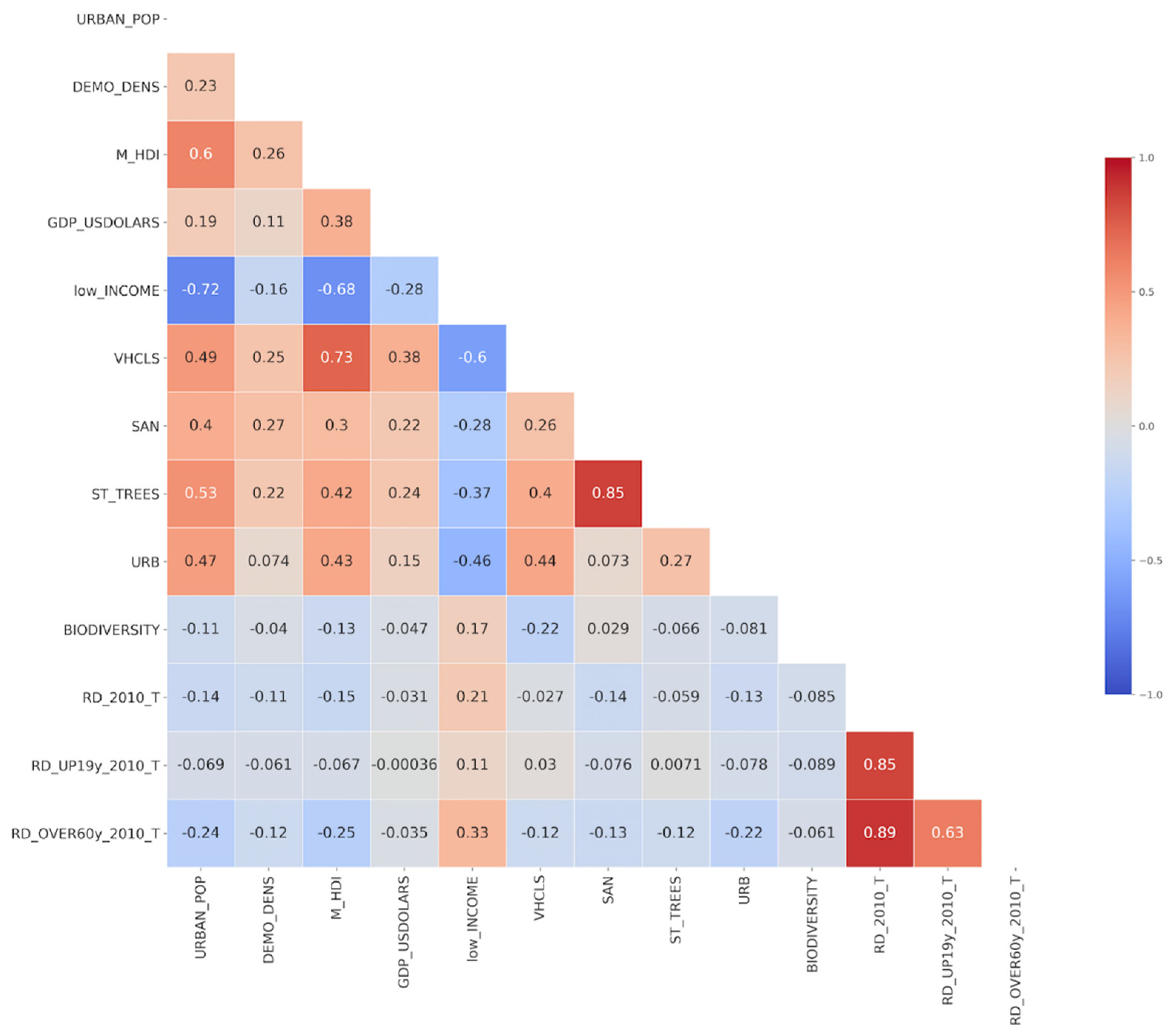
3.5. Autocorrelation Matrix
3.6. Cluster Analysis
3.7. Selection of Attributes (SelectKBest)
3.8. Associative Rules Mining
4. Discussion
4.1. UGI and RD
4.2. Socioeconomics, UGI and RD
4.3. Data Mining
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Scott, M.; Lennon, M.; Haase, D.; Kazmierczak, A.; Clabby, G.; Beatley, T. Nature-based solutions for the contemporary city/Re-naturing the city/Reflections on urban landscapes, ecosystems services and nature-based solutions in cities/Multifunctional green infrastructure and climate change adaptation: Brownfield greening as an adaptation strategy for vulnerable communities?/Delivering green infrastructure through planning: Insights from practice in Fingal, Ireland/Planning for biophilic cities: From theory to practice. Plan. Theory Pract. 2016, 17, 267–300. [Google Scholar] [CrossRef] [Green Version]
- Jaligot, R.; Chenal, J. Integration of ecosystem services in regional spatial plans in Western Switzerland. Sustainability 2019, 11, 313. [Google Scholar] [CrossRef] [Green Version]
- Parker, J.; de Baro, M.E.Z. Green infrastructure in the urban environment: A systematic quantitative review. Sustainability 2019, 11, 3182. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Housing, Communities and Local Government. National Planning Policy Framework (London, England). 2021; Volume 1, pp. 1–75. Available online: www.gov.uk/government/publications (accessed on 14 October 2021).
- Andersson-Sköld, Y.; Klingberg, J.; Gunnarsson, B.; Cullinane, K.; Gustafsson, I.; Hedblom, M.; Knez, I.; Lindberg, F.; Sang, Å.O.; Pleijel, H.; et al. A framework for assessing urban greenery’s effects and valuing its ecosystem services. J. Environ. Manag. 2018, 205, 274–285. [Google Scholar] [CrossRef]
- Barnes-Mauthe, M.; Oleson, K.L.L.; Brander, L.M.; Zafindrasilivonona, B.; Oliver, T.A.; van Beukering, P. Social capital as an ecosystem service: Evidence from a locally managed marine area. Ecosyst. Serv. 2015, 16, 283–293. [Google Scholar] [CrossRef] [Green Version]
- Garrigos-Simon, F.J.; Botella-Carrubi, M.D.; Gonzalez-Cruz, T.F. Social capital, human capital, and sustainability: A Bibliometric and visualization analysis. Sustainability 2018, 10, 4751. [Google Scholar] [CrossRef] [Green Version]
- Koc, C.B.; Osmond, P.; Peters, A. Towards a comprehensive green infrastructure typology: A systematic review of approaches, methods and typologies. Urban Ecosyst. 2017, 20, 15–35. [Google Scholar] [CrossRef]
- Fletcher, T.D.; Shuster, W.; Hunt, W.F.; Ashley, R.; Butler, D.; Arthur, S.; Trowsdale, S.; Barraud, S.; Semadeni-Davies, A.; Bertrand-Krajewski, J.-L.; et al. SUDS, LID, BMPs, WSUD and more—The evolution and application of terminology surrounding urban drainage. Urban Water J. 2015, 12, 525–542. [Google Scholar] [CrossRef]
- Sussams, L.W.; Sheate, W.R.; Eales, R.P. Green infrastructure as a climate change adaptation policy intervention: Muddying the waters or clearing a path to a more secure future? J. Environ. Manag. 2015, 147, 184–193. [Google Scholar] [CrossRef]
- Ferreira, J.C.; Monteiro, R.; Silva, V.R. Planning a green infrastructure network from theory to practice: The case study of Setúbal, Portugal. Sustainability 2021, 13, 8432. [Google Scholar] [CrossRef]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.; et al. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef] [PubMed]
- Suppakittpaisarn, P.; Jiang, X.; Sullivan, W.C. Green Infrastructure, Green Stormwater Infrastructure, and Human Health: A Review. Curr. Landsc. Ecol. Rep. 2017, 2, 96–110. [Google Scholar] [CrossRef] [Green Version]
- Amato-Lourenço, L.F.; Moreira, T.C.L.; de Arantes, B.L.; Filho, D.F.d.; Mauad, T. Metrópoles, cobertura vegetal, áreas verdes e saúde. Estud. Av. 2016, 30, 113–130. [Google Scholar] [CrossRef]
- Nowak, D.J.; Hirabayashi, S.; Doyle, M.; McGovern, M.; Pasher, J. Air pollution removal by urban forests in Canada and its effect on air quality and human health. Urban For. Urban Green. 2018, 29, 40–48. [Google Scholar] [CrossRef]
- Moktan, S.; Rai, P. Research Article Ethnobotanical Approach Against Respiratory Related Diseases and Disorders in Darjeeling Region of Eastern Himalaya. NeBIO 2019, 10, 99–105. [Google Scholar]
- Tai, A.; Tran, H.; Roberts, M.; Clarke, N.; Wilson, J.; Robertson, C.F. The association between childhood asthma and adult chronic obstructive pulmonary disease. Thorax 2014, 69, 805–810. [Google Scholar] [CrossRef] [Green Version]
- Annerstedt van den Bosch, M.; Mudu, P.; Uscila, V.; Barrdahl, M.; Kulinkina, A.; Staatsen, B.; Swart, W.; Kruize, H.; Zurlyte, I.; Egorov, A.I. Development of an urban green space indicator and the public health rationale. Scand. J. Public Health 2016, 44, 159–167. [Google Scholar] [CrossRef]
- van Dorn, A. Urban planning and respiratory health. Lancet Respir. Med. 2017, 5, 781–782. [Google Scholar] [CrossRef]
- WHO. Urban Green Space Interventions and Health: A Review of Impacts and Effectiveness; World Health Organization: Geneva, Switzerland, 2017.
- Schirmer, W.N.; Quadros, M.E. Compostos Orgânicos Voláteis Biogênicos Emitidos a Partir de Vegetação e Seu papel no ozônio troposférico urbano. Rev. Soc. Bras. Arborização Urbana 2010, 5, 25–42. [Google Scholar] [CrossRef]
- Eisenman, T.S.; Churkina, G.; Jariwala, S.P.; Kumar, P.; Lovasi, G.S.; Pataki, D.E.; Weinberger, K.R.; Whitlow, T.H. Urban trees, air quality, and asthma: An interdisciplinary review. Landsc. Urban Plan. 2019, 187, 47–59. [Google Scholar] [CrossRef]
- Russo, A.; Cirella, G.T. Modern compact cities: How much greenery do we need? Int. J. Environ. Res. Public Health 2018, 15, 2180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amano, T.; Butt, I.; Peh, K.S.H. The importance of green spaces to public health: A multi-continental analysis. Ecol. Appl. 2018, 28, 1473–1480. [Google Scholar] [CrossRef] [PubMed]
- Erdman, E.; Liss, A.; Gute, D.; Rioux, C.; Koch, M.; Naumova, E. Does the presence of vegetation affect asthma hospitalizations among the elderly? A comparison between rural, suburban, and urban areas. Int. J. Environ. Sustain. 2015, 4, 114. [Google Scholar] [CrossRef]
- Liddicoat, C.; Bi, P.; Waycott, M.; Glover, J.; Lowe, A.J.; Weinstein, P. Landscape biodiversity correlates with respiratory health in Australia. J. Environ. Manag. 2018, 206, 113–122. [Google Scholar] [CrossRef]
- Pimentel da Silva, L.; de Souza, F.T. Urban Management: Learning from Green Infrastructure, Socioeconomics and Health Indicators in the Municipalities of the State of Paraná, Brazil, Towards Sustainable Cities and Communities. In Universities and Sustainable Communities: Meeting the Goals of the Agenda 2030; World Sustainability Series; Leal Filho, W., Tortato, U., Frankenberger, F., Eds.; Springer: Cham, Switzerland, 2020. [Google Scholar] [CrossRef]
- Kowarik, I. Cities and Wilderness-A New Perspective. Int. J. Wilderness Int. J. Wilderness 2013, 19, 32–36. [Google Scholar]
- Alcock, I.; White, M.; Cherrie, M.; Wheeler, B.; Taylor, J.; McInnes, R.; Otte im Kampe, E. Land cover and air pollution are associated with asthma hospitalisations: A cross-sectional study. Environ. Int. 2017, 109, 29–41. [Google Scholar] [CrossRef]
- Hunter, R.F.; Cleland, C.; Cleary, A.; Droomers, M.; Wheeler, B.W.; Sinnett, D.; Nieuwenhuijsen, M.J.; Braubach, M. Environmental, health, wellbeing, social and equity effects of urban green space interventions: A meta-narrative evidence synthesis. Environ. Int. 2019, 130, 104923. [Google Scholar] [CrossRef]
- Aerts, R.; Honnay, O.; van Nieuwenhuyse, A. Biodiversity and human health: Mechanisms and evidence of the positive health effects of diversity in nature and green spaces. Br. Med. Bull. 2018, 127, 5–22. [Google Scholar] [CrossRef] [Green Version]
- Poverty, Health, & Environment. 2008. Available online: https://www.cbd.int/financial/doc/Pov-Health-Env-CRA.pdf (accessed on 20 January 2022).
- Braveman, P.; Gottlieb, L. The social determinants of health: It’s time to consider the causes of the causes. Public Health Rep. 2014, 129, 19–31. [Google Scholar] [CrossRef] [Green Version]
- IBGE, Brazilian Census. 2010. Available online: https://sidra.ibge.gov.br/acervo#/S/Q (accessed on 30 December 2021).
- Alvares, C.A.; Stape, J.L.; Sentelhas, P.C.; Gonçalves, J.L.d.; Sparovek, G. Köppen’s climate classification map for Brazil. Meteorol. Z. 2016, 22, 711–728. [Google Scholar] [CrossRef]
- IPARDES (Parana’s Institute of Economics and Social Development). Municipality, Statistics Notebook; Curitiba Municipality: Curitiba, Brazil, 2018; 44p. Available online: http://www.ipardes.gov.br/cadernos/MontaCadPdf1.php?Municipio=80000 (accessed on 30 December 2021)Curitiba, Brazil.
- SESA (PARANÁ). Relatório Anual de Gestão. Conselho Estadual de Saúde. Governo do Estado do Paraná. 2017; 178p. Available online: https://www.saude.pr.gov.br/Pagina/Relatorio-Anual-de-Gestao (accessed on 30 December 2021).
- O’Neill, M.S.; McMichael, A.J.; Schwartz, J.; Wartenberg, D. Poverty, environment, and health: The role of environmental epidemiology and environmental epidemiologists. Epidemiology 2007, 18, 664–668. [Google Scholar] [CrossRef] [PubMed]
- JHalonen, I.; Lanki, T.; Yli-Tuomi, T.; Kulmala, M.; Tiittanen, P.; Pekkanen, J. Urban air pollution, and asthma and COPD hospital emergency room visits. Thorax 2008, 63, 635–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, B.; Hsu, W.; Ma, Y. Integrating classification and association rule mining. In Knowledge Discovery and Data Mining; KDD’98; AAAI Press: New York, NY, USA., 1998; pp. 80–86. [Google Scholar]
- Souza, F.T.; Rabelo, W.S. A data mining approach to study the air pollution induced by urban phenomena and the association with respiratory diseases. In Proceedings of the 2015 11th International Conference on Natural Computation (ICNC), Zhangjiajie, China, 11 August 2015. [Google Scholar] [CrossRef]
- Cardoso, M.B.; de Souza, F.T. Prediction of hospitalizations caused by respiratory diseases by using data mining techniques: Some applications in Curitiba, Brazil and The Metropolitan Area. WIT Trans. Ecol. Environ. 2017, 211, 231–241. [Google Scholar]
- de Souza, F.T. Morbidity Forecast in Cities: A Study of Urban Air Pollution and Respiratory Diseases in the Metropolitan Region of Curitiba, Brazil. J. Urban Health 2019, 96, 591–604. [Google Scholar] [CrossRef] [PubMed]
- Belon, A.P.; Lima, M.G.; Barros, M.B.A. Gender differences in healthy life expectancy among Brazilian elderly. Health Qual. Life Outcomes 2014, 12, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IBGE. Classificação e Caracterização dos Espaços Rurais e Urbanos do Brasil: Uma Primeira Aproximação. Coordenação de Geografia—Rio de Janeiro. 2017; 84p. Available online: https://biblioteca.ibge.gov.br/visualizacao/livros/liv100643.pdf (accessed on 30 December 2021).
- Donovan, G.H.; Gatziolis, D.; Longley, I.; Douwes, J. Vegetation diversity protects against childhood asthma: Results from a large New Zealand birth cohort. Nat. Plants 2018, 4, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.W.; Lowe, A.J.; Lodge, C.J.; Heinrich, J.; Roponen, M.; Jalava, P.; Dong, G.H. Greenness surrounding schools is associated with lower risk of asthma in schoolchildren. Environ. Int. 2020, 143, 105967. [Google Scholar] [CrossRef]
- Shao, S.; Liu, L.; Tian, Z. Does the environmental inequality matter? A literature review. Environ. Geochem. Health 2021, 2, 124. [Google Scholar] [CrossRef]
- Kabisch, N.; van den Bosch, M.; Lafortezza, R. The health benefits of nature-based solutions to urbanization challenges for children and the elderly—A systematic review. Environ. Res. 2017, 159, 362–373. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Type | Description | Unit | Source |
|---|---|---|---|---|
| MUN | Categorical | Municipality Name | - | Cidades Platform (IBGE) |
| SIZE | Categorical | Municipality classification according to the population range | - | IBGE |
| TYPOLOGY | Categorical | Municipality typology rural-urban | - | IBGE |
| TOT_POP | Numerical | Number of people living in the municipality | number of persons | Cidades Platform (IBGE) |
| URBAN_POP | Numerical | Number of people living in areas designated as urban divided by the total population | ratio | SIDRA Platform (IBGE). Estimate from Table 207 of the 2010 Census. |
| DEMO_DENS | Numerical | TOT_POP divided by the area of the municipality | Number of persons per square kilometer | Cidades Platform (IBGE) |
| M_HDI | Numerical | Municipal Human Development Index | Ratio (0 to 1) | Cidades Platform (IBGE) |
| low_INCOME | Numerical | Number of households with a monthly income of up to half the Brazilian Minimum Salary in 2010, divided by the total households in the municipality | ratio | SIDRA Platform (IBGE). Table 3268 of the 2010 Census. |
| GDP_USDOLARS | Numerical | Gross Domestic Product per capita | USD | Cidades Platform (IBGE) |
| SAN | Numerical | Number of households with adequate sanitation divided by the total number of households | ratio | Cidades Platform (IBGE) |
| ST_TREES | Numerical | Number of people living in households located in urban areas with street trees divided by TOT_POP | ratio | SIDRA Platform (IBGE). Estimate from Table 3362 of the 2010 Census. |
| URB | Numerical | Number of households with adequate urban ordination (sidewalk, curb, paved streets) divided by the total number of households | ratio | Cidades Platform (IBGE) |
| BIODIVERSITY | Numerical | Hectares of biodiversity conservation unit divided by TOT_POP | ha/inhab | DIBAP/ICMS IAT-PR (http://www.iat.pr.gov.br/Pagina/ICMS-Ecologico-por-Biodiversidade (accessed on 14 October 2021); http://www.iat.pr.gov.br/sites/agua-terra/arquivos_restritos/files/documento/2020-03/repasse_icmse_2017_por_municipio.pdf. (accessed on 14 October 2021)) |
| VHCLS | Numerical | Total number of vehicles divided by TOT_POP | ratio | DENATRAN |
| RD | Numerical | Number of hospitalizations because of respiratory diseases divided by TOT_POP, times 100 | Hospitalizations per 100 inhab | MS/TabNet/DATASUS |
| Size | Number of Municipalities | Population Range |
|---|---|---|
| Small 1 (S_1) | 310 | Up to 20,000 |
| Small 2 (S_2) | 55 | Between 20,001 and 50,000 |
| Medium (M) | 14 | Between 50,001 and 100,000 |
| Large (L) | 17 | Between 100,001 and 900,000 |
| Metropolis (MEGA) | 1 | Over 900,000 |
| Typology (Rural-Urban) | Number of Municipalities |
|---|---|
| Adjacent-rural | 230 |
| Urban | 102 |
| Adjacent-intermediary | 65 |
| Variables | Mean | Minimum | Maximum | STD | Median |
|---|---|---|---|---|---|
| URBAN_POP | 0.678 | 0.090 | 1.000 | 0.203 | 0.710 |
| DEMO_DENS | 62.269 | 3.310 | 4027.040 | 240.760 | 25.040 |
| M_HDI | 0.702 | 0.546 | 0.823 | 0.039 | 0.706 |
| GDP_USD | 8665.71 | 3288.76 | 37,905.70 | 4088.78 | 7682.85 |
| low_INCOME | 0.028 | 0.002 | 0.133 | 0.024 | 0.020 |
| VHCLS | 0.372 | 0.047 | 0.682 | 0.087 | 0.369 |
| SAN | 0.326 | 0.006 | 0.972 | 0.272 | 0.265 |
| ST_STREET | 0.216 | 0.000 | 0.910 | 0.221 | 0.144 |
| URB | 0.337 | 0.000 | 0.919 | 0.217 | 0.300 |
| BIODIVERSITY | 0.353 | 0.000 | 27.095 | 1.739 | 0.000 |
| RD_2010_T | 1.851 | 0.182 | 7.328 | 1.191 | 1.569 |
| RD_2010_F | 1.842 | 0.162 | 7.767 | 1.259 | 1.568 |
| RD_2010_M | 1.853 | 0.178 | 7.592 | 1.141 | 1.639 |
| RD_UP19y_2010_T | 2.402 | 0.080 | 9.235 | 1.547 | 2.020 |
| RD_UP19y_2010_F | 2.202 | 0.000 | 7.731 | 1.464 | 1.835 |
| RD_UP19y_2010_M | 2.597 | 0.000 | 10.697 | 1.734 | 2.160 |
| RD_OVER60y_2010_T | 5.242 | 0.167 | 23.681 | 3.471 | 4.613 |
| RD_OVER60y_2010_F | 5.171 | 0.000 | 28.150 | 3.874 | 4.444 |
| RD_OVER60y_2010_M | 5.346 | 0.000 | 22.133 | 3.518 | 4.774 |
| Population Groups | TOT_POP | DEMO_ DENS | M_HDI | GDP_ USD | Low_ INCOME | VHCLS | SAN | ST_TREES | URB | BIODIVERSITY |
|---|---|---|---|---|---|---|---|---|---|---|
| All | 6 | 4 | 5 | 10 | 1 | 9 | 3 | 8 | 2 | 7 |
| Women | 3 | 6 | 4 | 10 | 1 | 9 | 5 | 8 | 2 | 7 |
| Men | 6 | 5 | 4 | 10 | 1 | 9 | 2 | 7 | 3 | 8 |
| All up to 19 years old | 9 | 3 | 6 | 8 | 5 | 1 | 4 | 10 | 7 | 2 |
| Women up to 19 years old | 3 | 7 | 1 | 9 | 4 | 2 | 6 | 10 | 8 | 5 |
| Men up to 19 years old | 8 | 6 | 2 | 9 | 1 | 7 | 3 | 10 | 4 | 5 |
| All over 60 years old | 4 | 7 | 3 | 9 | 1 | 8 | 6 | 5 | 2 | 10 |
| Women over 60 years old | 3 | 8 | 2 | 9 | 1 | 5 | 6 | 7 | 4 | 10 |
| Men over de 60 years old | 4 | 5 | 3 | 9 | 1 | 8 | 6 | 7 | 2 | 10 |
| Rule | Logic Sentence | Support | Confidence | |
|---|---|---|---|---|
| IF | THEN | |||
| 1 | URB (high) | ST_TREES (high) | 12.06 | 97.92 |
| SAN (high) | ||||
| 2 | M_DHI (high) | ST_TREES (high) | 17.839 | 97.18 |
| SAN (high) | ||||
| 3 | SAN (low) | ST_TREES (low) | 10.05 | 87.5 |
| RD_2010_T (high) | ||||
| 4 | ST_TREES (low) | SAN (low) | 9.548 | 92.11 |
| RD_2010_T (high) | ||||
| 5 | ST_TREES (high) | SAN (high) | 9.296 | 86.49 |
| RD_2010_T (medium) | ||||
| 6 | RD_2010_T (low) | URBAN_POP (high) | 4.774 | 100 |
| VHCLS (high) | ||||
| low_INCOME (low) | ||||
| BIODIVERSITY (medium) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pimentel da Silva, L.; da Fonseca, M.N.; de Moura, E.N.; de Souza, F.T. Ecosystems Services and Green Infrastructure for Respiratory Health Protection: A Data Science Approach for Paraná, Brazil. Sustainability 2022, 14, 1835. https://doi.org/10.3390/su14031835
Pimentel da Silva L, da Fonseca MN, de Moura EN, de Souza FT. Ecosystems Services and Green Infrastructure for Respiratory Health Protection: A Data Science Approach for Paraná, Brazil. Sustainability. 2022; 14(3):1835. https://doi.org/10.3390/su14031835
Chicago/Turabian StylePimentel da Silva, Luciene, Murilo Noli da Fonseca, Edilberto Nunes de Moura, and Fábio Teodoro de Souza. 2022. "Ecosystems Services and Green Infrastructure for Respiratory Health Protection: A Data Science Approach for Paraná, Brazil" Sustainability 14, no. 3: 1835. https://doi.org/10.3390/su14031835