
Flywheel Training in Older Adults—A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Identification
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Bias Risk Assessment
2.5. Data Extraction
3. Results
3.1. Study Quality
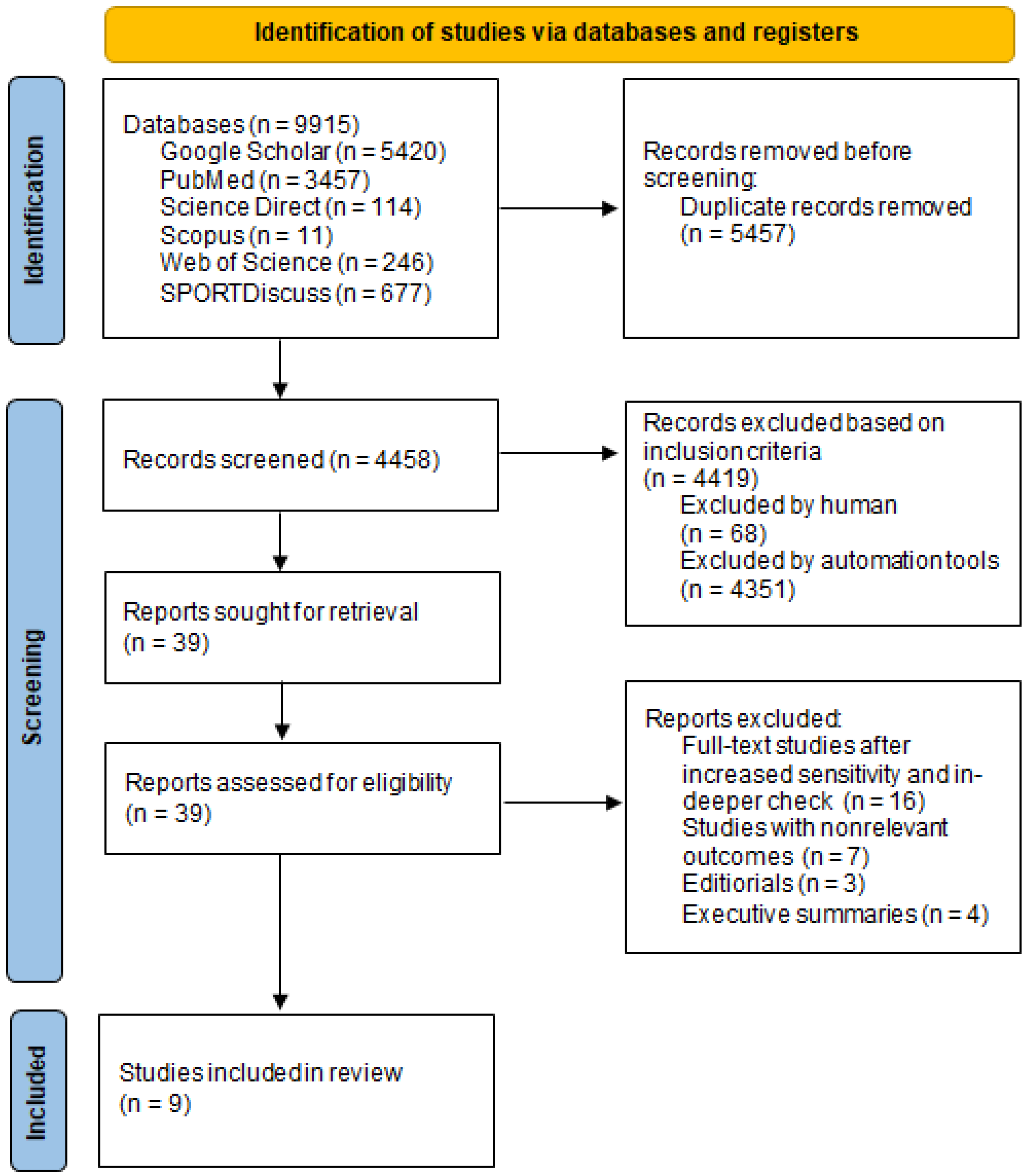
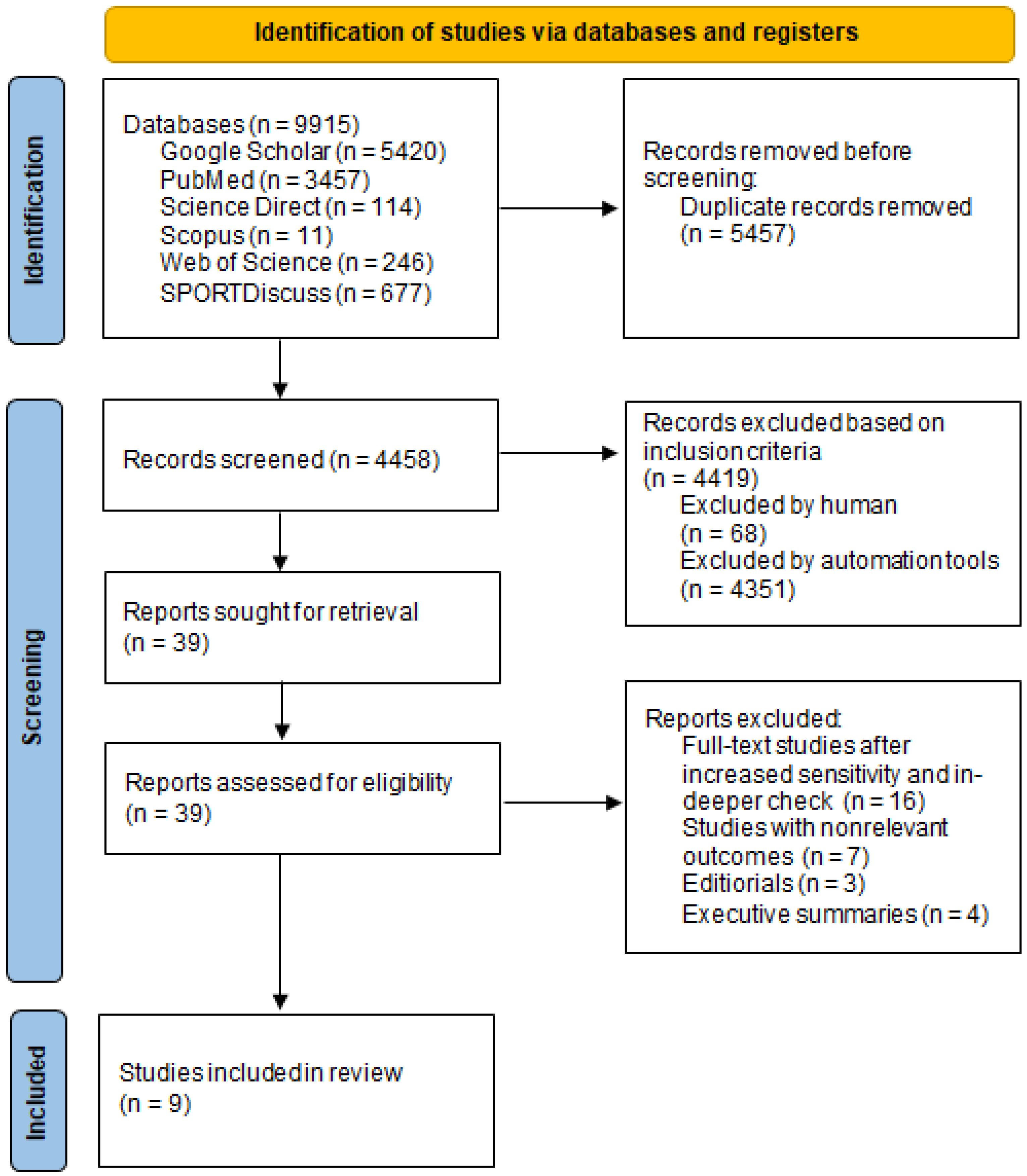
3.2. Selection and Characteristics of Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Desa, U. United nations department of economic and social affairs, population division. In World Population Prospects: The 2015 Revision, Key Findings and Advance Tables; Online Ed UN DESA: New York, NY, USA, 2015. [Google Scholar]
- Algilani, S.; Östlund-Lagerström, L.; Kihlgren, A.; Blomberg, K.; Brummer, R.J.; Schoultz, I. Exploring the concept of optimal functionality in old age. J. Multidiscip. Healthc. 2014, 7, 69. [Google Scholar] [PubMed] [Green Version]
- Kulkarni, D.; Gregory, S.; Evans, M. Effectiveness of eccentric-biased exercise interventions in reducing the incidence of falls and improving functional performance in older adults: A systematic review. Eur. Geriatr. Med. 2021, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Hairi, N.N.; Cumming, R.G.; Naganathan, V.; Handelsman, D.J.; Le Couteur, D.G.; Creasey, H.; Waite, L.M.; Seibel, M.J.; Sambrook, P.N. Loss of muscle strength, mass (sarcopenia), and quality (specific force) and its relationship with functional limitation and physical disability: The Concord Health and Ageing in Men Project. J. Am. Geriatr. Soc. 2010, 58, 2055–2062. [Google Scholar] [CrossRef] [PubMed]
- Vetrovsky, T.; Steffl, M.; Stastny, P.; Tufano, J.J. The efficacy and safety of lower-limb plyometric training in older adults: A systematic review. Sport Med. 2019, 49, 113–131. [Google Scholar] [CrossRef] [Green Version]
- Ward, R.E.; Leveille, S.G.; Beauchamp, M.K.; Travison, T.; Alexander, N.; Jette, A.M.; Bean, J.F. Functional performance as a predictor of injurious falls in older adults. J. Am. Geriatr. Soc. 2015, 63, 315–320. [Google Scholar] [CrossRef] [Green Version]
- Goodpaster, B.H.; Park, S.W.; Harris, T.B.; Kritchevsky, S.B.; Nevitt, M.; Schwartz, A.V.; Simonsick, E.M.; Tylavsky, F.A.; Visser, M.; Newman, A.B. The loss of skeletal muscle strength, mass, and quality in older adults: The health, aging and body composition study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 1059–1064. [Google Scholar] [CrossRef]
- Zhang, L.; Ding, Z.; Qiu, L.; Li, A. Falls and risk factors of falls for urban and rural community-dwelling older adults in China. BMC Geriatr. 2019, 19, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Harridge, S.D.R.; Lazarus, N.R. Physical activity, aging, and physiological function. Physiology 2017, 32, 152–161. [Google Scholar] [CrossRef] [Green Version]
- Hill, M.W.; Roberts, M.; Price, M.J.; Kay, A.D. Effects of Flywheel Training With Eccentric Overload on Standing Balance, Mobility, Physical Function, Muscle Thickness, and Muscle Quality in Older Adults. J. Strength Cond. Res. 2021. [Google Scholar] [CrossRef]
- Norrbrand, L.; Pozzo, M.; Tesch, P.A. Flywheel resistance training calls for greater eccentric muscle activation than weight training. Eur. J. Appl. Physiol. 2010, 110, 997–1005. [Google Scholar] [CrossRef]
- Wonders, J. Flywheel training in musculoskeletal rehabilitation: A clinical commentary. Int. J. Sports Phys. Ther. 2019, 14, 994. [Google Scholar] [CrossRef] [PubMed]
- Berg, H.E.; Tesch, A. A gravity-independent ergometer to be used for resistance training in space. Aviat. Space Environ. Med. 1994, 65, 752–756. [Google Scholar] [PubMed]
- Maroto-Izquierdo, S.; García-López, D.; Fernandez-Gonzalo, R.; Moreira, O.C.; González-Gallego, J.; de Paz, J.A. Skeletal muscle functional and structural adaptations after eccentric overload flywheel resistance training: A systematic review and meta-analysis. J. Sci. Med. Sport 2017, 20, 943–951. [Google Scholar] [CrossRef] [PubMed]
- Romero-Rodriguez, D.; Gual, G.; Tesch, P.A. Efficacy of an inertial resistance training paradigm in the treatment of patellar tendinopathy in athletes: A case-series study. Phys. Ther. Sport 2011, 12, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Allen, W.J.C.; De Keijzer, K.L.; Raya-González, J.; Castillo, D.; Coratella, G.; Beato, M. Chronic effects of flywheel training on physical capacities in soccer players: A systematic review. Res. Sport Med. 2021, 1–21. [Google Scholar] [CrossRef] [PubMed]
- De Keijzer, K.; McErlain-Naylor, S.A.; Brownlee, T.E.; Raya-González, J.; Beato, M. Perception and application of flywheel training by professional soccer practitioners. Biol. Sport 2021, 39, 809–817. [Google Scholar] [CrossRef]
- Maroto-Izquierdo, S.; McBride, J.M.; Gonzalez-Diez, N.; García-López, D.; González-Gallego, J.; de Paz, J.A. Comparison of Flywheel and Pneumatic Training on Hypertrophy, Strength, and Power in Professional Handball Players. Res. Q. Exerc. Sport 2020, 93, 1–15. [Google Scholar] [CrossRef]
- Arede, J.; Gonzalo-Skok, O.; Bishop, C.; Schollhorn, W.; Leite, N. Rotational flywheel training in youth female team sport athletes: Could inter-repetition movement variability be beneficial? J. Sports Med. Phys. Fit. 2020, 60, 1444–1452. [Google Scholar] [CrossRef]
- Trajković, N.; Đorđević, D.; Stanković, M.; Petrušič, T.; Bogataj, Š.; Peršič, V. Exercise-Based Interventions in Middle-Aged and Older Adults after Myocardial Infarction: A Systematic Review. Life 2021, 11, 928. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B. PRISMA-S: An extension to the PRISMA statement for reporting literature searches in systematic reviews. Syst. Rev. 2021, 10, 1–19. [Google Scholar] [CrossRef] [PubMed]
- de Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Onambélé, G.L.; Maganaris, C.N.; Mian, O.S.; Tam, E.; Rejc, E.; McEwan, I.M.; Narici, M.V. Neuromuscular and balance responses to flywheel inertial versus weight training in older persons. J. Biomech. 2008, 41, 3133–3138. [Google Scholar] [CrossRef] [PubMed]
- Brzenczek-Owczarzak, W.; Naczk, M.; Arlet, J.; Forjasz, J.; Jedrzejczak, T.; Adach, Z. Estimation of the efficacy of inertial training in older women. J. Aging Phys. Act. 2013, 21, 433–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez-Gonzalo, R.; Nissemark, C.; Åslund, B.; Tesch, P.A.; Sojka, P. Chronic stroke patients show early and robust improvements in muscle and functional performance in response to eccentric-overload flywheel resistance training: A pilot study. J. Neuroeng. Rehabil. 2014, 11, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Bruseghini, P.; Calabria, E.; Tam, E.; Milanese, C.; Oliboni, E.; Pezzato, A.; Pogliaghi, S.; Salvagno, G.L.; Schena, F.; Mucelli, R.P.; et al. Effects of eight weeks of aerobic interval training and of isoinertial resistance training on risk factors of cardiometabolic diseases and exercise capacity in healthy elderly subjects. Oncotarget 2015, 6, 16998. [Google Scholar] [CrossRef] [Green Version]
- Bruseghini, P.; Capelli, C.; Calabria, E.; Rossi, A.P.; Tam, E. Effects of High-Intensity Interval Training and Isoinertial Training on Leg Extensors Muscle Function, Structure, and Intermuscular Adipose Tissue in Older Adults. Front. Physiol. 2019, 10, 1260. [Google Scholar] [CrossRef]
- Roberts, M. Effect of Eccentric Flywheel Training on Musculoskeletal Characteristics and Physical Function in Older Adults. 2019. Available online: https://pure.coventry.ac.uk/ws/portalfiles/portal/31210514/Roberts_Pure.pdf (accessed on 11 December 2021).
- Sañudo, B.; González-Navarrete, Á.; Álvarez-Barbosa, F.; De Hoyo, M.; Del Pozo, J.; Rogers, M.E. Effect of flywheel resistance training on balance performance in older adults. A randomized controlled trial. J. Sports Sci. Med. 2019, 18, 344. [Google Scholar]
- Spudić, D.; Hadžić, V.; Vodičar, J.; Carruthers, J.; Pori, P. Influence of Inertial Resistance Squat Exercise Protocol Based on Novel Exercise Intensity Determination on Physical Fitness of Older Adult Women. Exerc. Qual. Life 2019, 11, 29–36. [Google Scholar] [CrossRef]
- Odeleye, O.O. A Comparative Study on the Effects of Eccentric Flywheel Overload and Traditional Resistance Training on the Physiological/Functional Performance in Healthy Older Adults. Univ. Sask. 2020. Available online: https://harvest.usask.ca/bitstream/handle/10388/12773/ODELEYE-THESIS-2020.pdf?sequence=1 (accessed on 17 December 2021).
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Hicks, G.E.; Shardell, M.; Alley, D.E.; Miller, R.R.; Bandinelli, S.; Guralnik, J.; Lauretani, F.; Simonsick, E.M.; Ferrucci, L. Absolute strength and loss of strength as predictors of mobility decline in older adults: The InCHIANTI study. J. Gerontol. Ser. A Biomed Sci. Med. Sci. 2012, 67, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Tanaka, K.; Yabushita, N.; Sakai, T.; Shigematsu, R. Effects of exercise frequency on functional fitness in older adult women. Arch. Gerontol. Geriatr. 2007, 44, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Vicens-Bordas, J.; Esteve, E.; Fort-Vanmeerhaeghe, A.; Bandholm, T.; Thorborg, K. Is inertial flywheel resistance training superior to gravity-dependent resistance training in improving muscle strength? A systematic review with meta-analyses. J. Sci. Med. Sport 2018, 21, 75–83. [Google Scholar] [CrossRef]
- Raya-González, J.; Castillo, D.; Beato, M. The flywheel paradigm in team sports: A soccer approach. Strength Cond. J. 2021, 43, 12–22. [Google Scholar] [CrossRef]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance training for older adults: Position statement from the national strength and conditioning association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.; Lamb, S.E. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2012, 9. [Google Scholar] [CrossRef]
- Howe, T.E.; Rochester, L.; Neil, F.; Skelton, D.A.; Ballinger, C. Exercise for improving balance in older people. Cochrane Database Syst. Rev. 2011, 11. [Google Scholar] [CrossRef]
- Beato, M.; Dello Iacono, A. Implementing flywheel (isoinertial) exercise in strength training: Current evidence, practical recommendations, and future directions. Front. Physiol. 2020, 11, 569. [Google Scholar] [CrossRef]
- González, J.R.; de Keijzer, K.; Beato, M. Effects of flywheel training on strength-related variables in female populations. A systematic review. Res. Sports Med. 2020, 1–18. [Google Scholar] [CrossRef]
- Hess, J.A.; Woollacott, M.; Shivitz, N. Ankle force and rate of force production increase following high intensity strength training in frail older adults. Aging Clin. Exp. Res. 2006, 18, 107–115. [Google Scholar] [CrossRef]
- Orr, R.; Raymond, J.; Singh, M.F. Efficacy of progressive resistance training on balance performance in older adults. Sports Med. 2008, 38, 317–343. [Google Scholar] [CrossRef] [PubMed]
- Pereira, A.; Izquierdo, M.; Silva, A.J.; Costa, A.M.; Bastos, E.; González-Badillo, J.; Marques, M.C. Effects of high-speed power training on functional capacity and muscle performance in older women. Exp. Gerontol. 2012, 47, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Sayers, S.P.; Gibson, K. High-speed power training in older adults: A shift of the external resistance at which peak power is produced. J. Strength Cond. Res. Strength Cond. Assoc. 2014, 28, 616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orr, R. Contribution of muscle weakness to postural instability in the elderly. Eur. J. Phys. Rehabil. Med. 2010, 46, 183–220. [Google Scholar] [PubMed]
- Van Roie, E.; Delecluse, C.; Coudyzer, W.; Boonen, S.; Bautmans, I. Strength training at high versus low external resistance in older adults: Effects on muscle volume, muscle strength, and force–velocity characteristics. Exp. Gerontol. 2013, 48, 1351–1361. [Google Scholar] [CrossRef]
- Schlicht, J.; Camaione, D.N.; Owen, S.V. Effect of intense strength training on standing balance, walking speed, and sit-to-stand performance in older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M281–M286. [Google Scholar] [CrossRef] [Green Version]
- Okamoto, N.; Nakatani, T.; Okamoto, Y.; Iwamoto, J.; Saeki, K.; Kurumatani, N. Increasing the number of steps walked each day improves physical fitness in Japanese community-dwelling adults. Int. J. Sports Med. 2010, 31, 277–282. [Google Scholar] [CrossRef]
- Özkaya, G.Y.; Aydin, H.; Toraman, F.N.; Kizilay, F.; Özdemir, Ö.; Cetinkaya, V. Effect of strength and endurance training on cognition in older people. J. Sports Sci. Med. 2005, 4, 300. [Google Scholar]
- Nyland, J.; Frost, K.; Quesada, P.; Angeli, C.; Swank, A.; Topp, R.; Malkani, A.L. Self-reported chair-rise ability relates to stair-climbing readiness of total knee arthroplasty patients: A pilot study. J. Rehabil. Res. Dev. 2007, 44, 751–759. [Google Scholar] [CrossRef]
- Millor, N.; Lecumberri, P.; Gómez, M.; Martínez-Ramírez, A.; Izquierdo, M. An evaluation of the 30-s chair stand test in older adults: Frailty detection based on kinematic parameters from a single inertial unit. J. Neuroeng. Rehabil. 2013, 10, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Gonzalo, R.; Lundberg, T.R.; Alvarez-Alvarez, L.; de Paz, J.A. Muscle damage responses and adaptations to eccentric-overload resistance exercise in men and women. Eur. J. Appl. Physiol. 2014, 114, 1075–1084. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, S.; Salem, G.J.; Wang, M.-Y.; Sanker, S.E.; Greendale, G.A. Squatting exercises in older adults: Kinematic and kinetic comparisons. Med. Sci. Sports Exerc. 2003, 35, 635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raj, I.S.; Bird, S.; Westfold, B.; Shield, A. Effects of eccentrically biased versus conventional weight training in older adults. Med. Sci. Sports Exerc. 2012, 44, 1167–1176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dias, C.P.; Toscan, R.; de Camargo, M.; Pereira, E.P.; Griebler, N.; Baroni, B.M.; Tiggemann, C.L. Effects of eccentric-focused and conventional resistance training on strength and functional capacity of older adults. Age 2015, 37, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Mueller, M.; Breil, F.A.; Vogt, M.; Steiner, R.; Lippuner, K.; Popp, A.; Klossner, S.; Hoppeler, H.; Däpp, C. Different response to eccentric and concentric training in older men and women. Eur. J. Appl. Physiol. 2009, 107, 145–153. [Google Scholar] [CrossRef] [Green Version]
- Foldvari, M.; Clark, M.; Laviolette, L.C.; Bernstein, M.A.; Kaliton, D.; Castaneda, C.; Pu, C.T.; Hausdorff, J.M.; Fielding, R.A.; Singh, M.A.F. Association of muscle power with functional status in community-dwelling elderly women. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2000, 55, M192–M199. [Google Scholar] [CrossRef]
- Md, J.F.B.; Kiely, D.K.; Herman, S.; Leveille, S.G.; Mizer, K.; Frontera, W.R.; Fielding, R.A. The relationship between leg power and physical performance in mobility-limited older people. J. Am. Geriatr. Soc. 2002, 50, 461–467. [Google Scholar] [CrossRef]
- Tesch, P.A.; Fernandez-Gonzalo, R.; Lundberg, T.R. Clinical applications of iso-inertial, eccentric-overload (YoYoTM) resistance exercise. Front. Physiol. 2017, 8, 241. [Google Scholar] [CrossRef] [Green Version]
- Lorenz, D.; Morrison, S. Current concepts in periodization of strength and conditioning for the sports physical therapist. Int. J. Sports Phys. Ther. 2015, 10, 734. [Google Scholar]
- Folland, J.P.; Williams, A.G. Morphological and neurological contributions to increased strength. Sport Med. 2007, 37, 145–168. [Google Scholar] [CrossRef]
- Petré, H.; Wernstål, F.; Mattsson, C.M. Effects of flywheel training on strength-related variables: A meta-analysis. Sport Med. 2018, 4, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Papa, E.V.; Dong, X.; Hassan, M. Resistance training for activity limitations in older adults with skeletal muscle function deficits: A systematic review. Clin. Interv. Aging 2017, 12, 955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurley, B.F.; Roth, S.M. Strength training in the elderly: Effects on risk factors for age-related diseases. Sports Med. 2000, 30, 249–268. [Google Scholar] [CrossRef]
- Van Eijden, T.; Weijs, W.A.; Kouwenhoven, E.K.; Verburg, J. Forces acting on the patella during maximal voluntary contraction of the quadriceps femoris muscle at different knee flexion/extension angles. Cells Tissues Organs. 1987, 129, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Laursen, P.; Buchheit, M. Science and Application of High-Intensity Interval Training; Human Kinetics: Champagn, IL, USA, 2019. [Google Scholar]
- Beato, M.; Fleming, A.; Coates, A.; Dello Iacono, A. Validity and reliability of a flywheel squat test in sport. J. Sports Sci. 2021, 39, 482–488. [Google Scholar] [CrossRef]

{kind=link}
| Inclusion | Exclusion | |
|---|---|---|
| Population | Older adults (≥60 years) Males and females | Children, youth, adolescents, adults |
| Intervention | Flywheel training | Flexibility training, plyometric training, speed training |
| Control | - | - |
| Outcome | Post-flywheel intervention, strengh, balance, posture control, mobility, functional and cardiovascular performance, body composition | - |
| Study design | Randomized non-randomized studies, controlled studies, intervention studies | Case studies, systematic reviews, meta-analysis, case reports, Editorals, non-English studies |
| Criterion | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | ∑ |
| Onambele et al. (2008) [24] | Y | Y | Y | Y | N | Y | N | Y | Y | Y | Y | 8 |
| Brzenczek-Owczarzak et al. (2013) [25] | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7 |
| Fernandez-Gonzalo et al. (2014) [26] | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5 |
| Bruseghini et al. (2015) [27] | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5 |
| Bruseghini et al. (2019) [28] | Y | N | Y | Y | N | N | N | Y | Y | Y | Y | 6 |
| Roberts et al. (2019) [29] | Y | Y | Y | Y | N | Y | N | Y | Y | Y | Y | 8 |
| Sanudo et al. (2019) [30] | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7 |
| Spudić et al. (2019) [31] | Y | Y | Y | Y | N | Y | N | N | Y | Y | Y | 7 |
| Odeleye et al. (2020) [32] | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7 |
| First Author and Year of Publication | Aim | Sample of Participants | Exercise Program | Measurements | Results | ||
|---|---|---|---|---|---|---|---|
| Number and Groups | Age (Years) | ||||||
| Onambele et al. (2008) [24] | Effects of F inertial loading and comaparation with WT, on KE (indices of quadriceps strength) | N-24 M-12 F-12 E1-12 E2-12 | 69.9 ± 1.3 | 3x a week 12 weeks 1–4 sets 8–12 rep. ≈5 mrbs | PS tests, maximal peak isokinetic KE function, EMG recordings | ** E1 Maximal peak isokinetic KE (28%, p < 0.01) PS (45%, p < 0.01) | |
| Brzenczek-Owczarzak et al. (2013) [25] | To estimate the efficiency of short-term inertial training using ITMS | F-45 E1-17 E2-10 C-18 | E1-62.2 ± 5.4 E2-64.1 ± 5.4 C-63.4 ± 4 | 3x a week 4 weeks 45 min 3 sets 10 rep. ≈2 mrbs | Maximal torque, P | Maximal torque (Da) E1 ** (21.9%) E2 ** # (6.9%) C (2.2%) (NDa) E1 ** (10.7%) | PWR (Da) E1 ** (34.3%) E2 ** # (9.8%) C (−1.4%) (NDa) E1 ** (27.6%) E2 ** (18.2%) C (0.6%) |
| Fernandez-Gonzalo et al. (2014) [26] | To estimate the efficacy of ECC-overload F RE training to improve force, P, B, and FP in physically active chronic stroke patients | N-12 M-9 F-3 | 63.3 ± 8.1 | 2x a week 8 weeks 4 sets 7 max. rep. ≈3 mrbs | B, FP, spasticity and RPE, isometric and isokinetic KE torque, peak P isometric leg press force | Peak PWR ** ECC (34%, p = 0.009) CON (44%, p = 0.003) Isokinetic torque ECC ** (p = 0.0005) CON (p = 0.002) Isometric leg press 10–20% (p < 0.05) | |
| Bruseghini et al. (2015) [27] | Effect of 8 weeks of HIT and IRT on CVF, MS mass, and risk factors of metabolic syndrome | M-12 | 68 ± 4 | 3x a week 8 weeks 3–4 sets 7 max. rep. ≈3 mrbs | BC, muscle structure, MS, maximal test, exercise efficiency | MS ** (HIT, IRT #) CON 60° (p = 0.0004) 120° (0.0049) ECC 60° (p = 0.0102) 120° (0.0010) | |
| Bruseghini et al. (2019) [28] | Comparation of effects of HIIT and IRT on strength, mass, architecture, IMAT quality, and Na | M-12 | 69.3 ± 4.2 | 3x a week 8 weeks 3 sets 7 rep. ≈3 mrbs | VO2max, muscle volume, IMAT, Na MS, muscle architecture | IRT muscle volume (p = 0.003), HIIT muscle volume (p = 0.001) IRT IMAT (p = 0.001) HIIT IMAT (p = 0.003) | |
| Roberts (2019) [29] | To determine the effectiveness of a short period of F eccentric RE and to compare changes in MS and mass, physical function, and fall risk | N-21 M-10 F-11 E-13 C-8 | 62.52 ± 6.72 | 2x a week 6 weeks 4 sets 8–12 rep. | 30 sec Sts, TUAG, 5x Sts, isometric strength | 30 sec Sts (p = 0.248) TUAG (p = 0.157) 5x Sts (p = 0.389) | |
| Sanudo et al. (2019) [30] | To assess the effects of F RE training on PS and M | N-34 E-17 C-17 | 65 ± 4 E-64.4 ± 3.61 C-66.38 ± 4.85 | 2–3x a week 6 weeks 4 sets 9 rep. ≈3 mrbs | PS, P | E ** # TUAG (p < 0.01) PWR (p < 0.05) | |
| Spudić et al. (2019) [31] | To examine the effects of inertial device exercies protocol compared to the traditional weight-based, on KE MS, agility, B, CVE, and RPE | F-37 E1-14 E2-12 C-11 | E1-71.6 ± 6.4 E2-68.8 ± 6.4 C-67.3 ± 4.5 | 8 weeks 2–4 sets 10–22 rep. ≈1.5 mrbs | 6MWT, Sts, TUAG, FR, RPE | E2 # Sts (p = 0.018) RPE # (E1,E2,C, p > 0.05)TUAG (ES% = −0.44) 6MWT (ES% = 0.47) | |
| Odeleye (2020) [32] | To compare the effects of eccentric Fly overload training and traditional RE on MS, muscle thickness, BC, and FP | N-19 M-6 F-13 E-11 C-8 | E1-63.2 ± 7.8 C-63.8 ± 5.2 | 3x a week 13 weeks 3 + 3 + 3 + 3 max. reps ≈1 mrbs | MS of quadriceps (KE), FP (shuttle walk test, FR, 30 sec Sts, up and down stair climb P test) | (E1, E2) ** (p < 0.001) (PWR, Sts, up and down stair climb) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Čokorilo, N.; Horvatin, M.; Đorđević, D.; Stanković, M.; Pekas, D. Flywheel Training in Older Adults—A Systematic Review. Sustainability 2022, 14, 4137. https://doi.org/10.3390/su14074137
Čokorilo N, Horvatin M, Đorđević D, Stanković M, Pekas D. Flywheel Training in Older Adults—A Systematic Review. Sustainability. 2022; 14(7):4137. https://doi.org/10.3390/su14074137
Chicago/Turabian StyleČokorilo, Nebojša, Maja Horvatin, Dušan Đorđević, Mima Stanković, and Damir Pekas. 2022. "Flywheel Training in Older Adults—A Systematic Review" Sustainability 14, no. 7: 4137. https://doi.org/10.3390/su14074137
APA StyleČokorilo, N., Horvatin, M., Đorđević, D., Stanković, M., & Pekas, D. (2022). Flywheel Training in Older Adults—A Systematic Review. Sustainability, 14(7), 4137. https://doi.org/10.3390/su14074137