
Designing IAQ-Resilient Post-Pandemic Buildings




Abstract
:1. Introduction
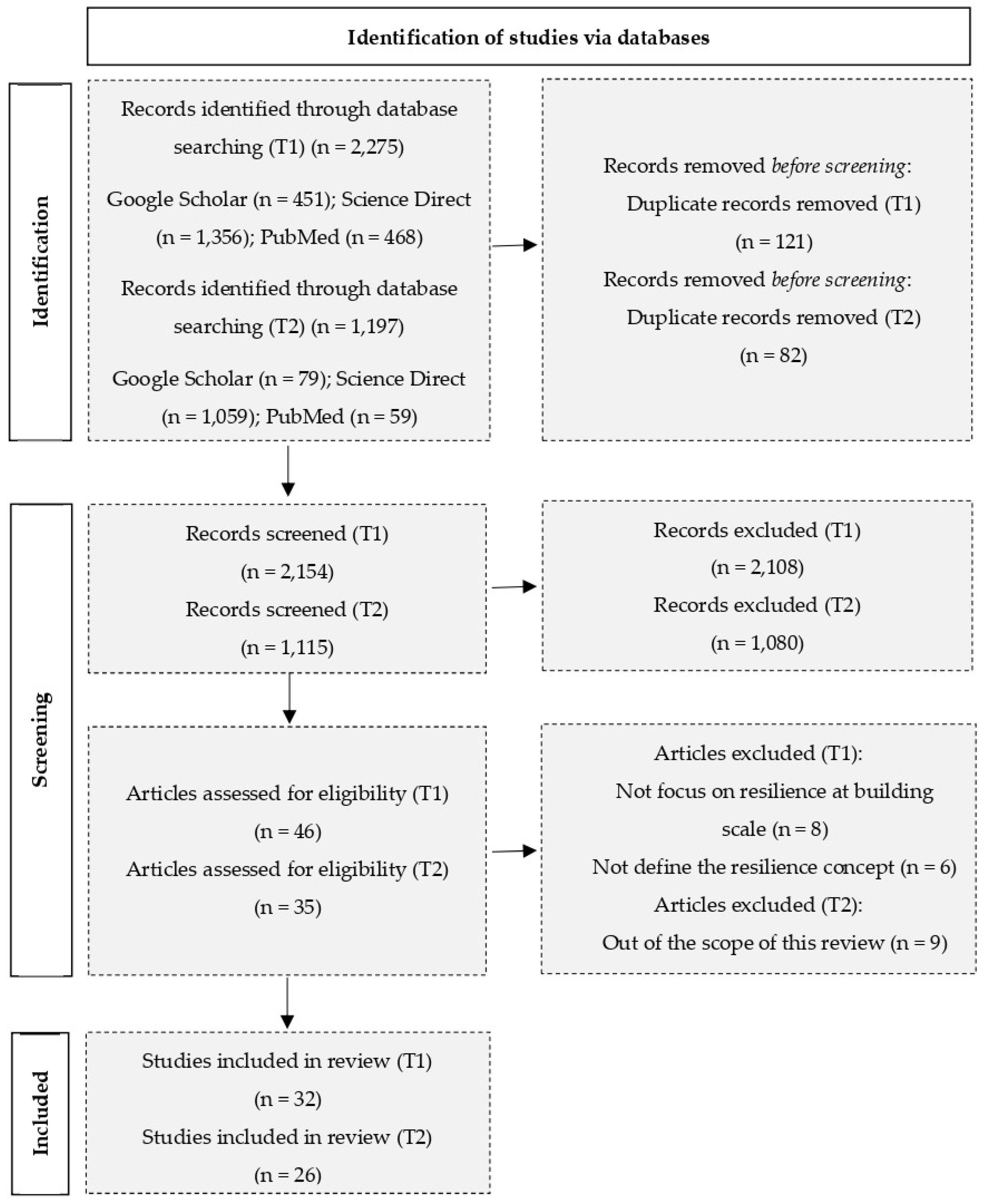
2. Methods
- The inclusion criteria were:
- (1)
- Published from 2020 and 2022 in accordance with the spread of the COVID-19 pandemic emergency;
- (2)
- Written in English;
- (3)
- Articles showing a definition of the concept of resilience in relation to the building energy sector;
- (4)
- Studies analyzing the relationship between the COVID-19 pandemic and the built environment.
- The exclusion criteria were:
- (1)
- Literature related to the concept of resilience without being linked to the built environment;
- (2)
- Study without any correlation between COVID-19 and the built environment;
- (3)
- The focus of the study was at the urban or city scale;
- (4)
- Not full-text content was available.
- The inclusion criteria were:
- (1)
- Published from 2020 and 2022 in accordance with the spread of the COVID-19 pandemic emergency;
- (2)
- Written in English;
- (3)
- Articles describing the layers of the COVID-19 control hierarchy or the strategies of enhancing resilience in building designs;
- (4)
- Studies focusing on engineering controls in relation to IAQ and COVID-19.
- The exclusion criteria were:
- (1)
- Articles discussing building design strategies without any relation to the COVID-19 period;
- (2)
- Not full-text content was available.
3. Results and Discussion
3.1. Definitions of Resilience for the Built Environment
3.2. Hazard Control Measures of IAQ-Resilient Buildings
- Personal protective equipment (PPE). These measures are related to the personal protection of individuals, and include the use of masks in indoor spaces while also encouraging the adequate sanitization of the devices.
- Administrative controls. These include activities to educate people on how they should interact in enclosed environments to reduce opportunities for close contact with each other. Some of these control measures may include: (1) requiring people with COVID-19 symptoms to stay at home; (2) ensuring cleaning and disinfection actions; and (3) staggering entry and exit times from workplaces.
- Engineering controls. These refer to strategies aiming to redesign or modify the building’s systems to mitigate the risk of infection. Among these actions, preventive measures including the ventilation of the building have proven to be the most effective in reducing the risk of the SARS-CoV-2 virus spreading.
- Elimination and substitution. In the context of COVID-19 pandemic, these control measures included all the actions that eliminated the potential for SARS-CoV-2 exposure, such as: (1) isolating infected persons from others,(2) eliminating or reducing person-to-person interactions, (3) reducing the occupancy in indoor environments, and (4) moving activities to outdoor spaces.
- Maintaining a high ventilation rate despite variations in occupancy. As [66] showed, it was recommended to extend the operation times of mechanical ventilation systems by keeping the ventilation on 24/7.
- Opening windows was a key recommendation to rapidly increase the IAQ during the COVID-19 pandemic period [69].
- Introducing CO2 monitoring to assess the adequacy of ventilation in the indoor environment. This type of measure allows the occupants to act when the CO2 level exceeds a certain threshold by opening a window or reducing the occupancy [70].
4. A CBA Decision-Making Tool to Boost IAQ-Resilient Buildings
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Organization for Economic Co-Operation and Development (OECD). Environmental Health and Strengthening Resilience to Pandemics. Available online: https://read.oecd-ilibrary.org/view/?ref=129_129937-jm4ul2jun9&title=Environmental-health-and-strengthening-resilience-to-pandemics (accessed on 15 June 2022).
- American Society of Heating, Refrigerating and Air Conditioning Engineers (ASHRAE). In Handbook of Fundamentals, 1st ed.; American Society of Heating, Refrigerating and Air Conditioning Engineers: Atlanta, GA, USA, 2005.
- Heidari, L.; Younger, M.; Chandler, G.; Gooch, J.; Schramm, P. Integrating Health into Buildings of the Future. J. Sol. Energy Eng. 2016, 139, 010802. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Directive (EU) 2018/844 of the European Parliament and of the Council of 30 May 2018 amending Directive 2010/31/EU on the Energy Performance of Buildings and Directive 2012/27/EU on Energy Efficiency; European Commission: Geneva, Switzerland, 2018. [Google Scholar]
- ABM Industries Inc. Indoor Air Quality and Facility Resilience. Creating Safer, Healthier Indoor Spaces. Available online: https://www.abm.com/wp-content/uploads/2021/02/ABM_EnhancedFacility_IndoorAirQualityandFacilityResilience_eBook_1.20.pdf (accessed on 15 June 2022).
- Marcu, F.; Hodor, N.; Indrie, L.; Dejeu, P.; Ilieș, M.; Albu, A.; Sandor, M.; Sicora, C.; Costea, M.; Ilieș, D.C.; et al. Microbiological, Health and Comfort Aspects of Indoor Air Quality in a Romanian Historical Wooden Church. Int. J. Environ. Res. Public Health 2021, 18, 9908. [Google Scholar] [CrossRef] [PubMed]
- Awada, M.; Becerik-Gerber, B.; Hoque, S.; O’Neill, Z.; Pedrielli, G.; Wen, J.; Wu, T. Ten questions concerning occupant health in buildings during normal operations and extreme events including the COVID-19 pandemic. Build. Environ. 2020, 188, 107480. [Google Scholar] [CrossRef] [PubMed]
- Harvard T.H. Chan School of Public Health. Healthy Buildings. Available online: https://www.hsph.harvard.edu/healthybuildings/ (accessed on 15 June 2022).
- Addae-Dapaah, K.; Wai, T.K.; Bin Dollah, M.J.; Foo, Y. Indoor Air Quality and Office Property Value. J. Sustain. Real Estate 2010, 2, 91–115. [Google Scholar] [CrossRef]
- Harvard T.H. Chan School of Public Health. The 9 Foundations of a Healthy Building. Available online: https://forhealth.org/9_Foundations_of_a_Healthy_Building.February_2017.pdf (accessed on 15 June 2022).
- Spengler, J.D.; Chen, Q.Y. Indoor air quality factors in designing a healthy building. Annu. Rev. Energy Environ. 2000, 25, 567–600. [Google Scholar] [CrossRef] [Green Version]
- U.S. Environmental Protection Agency (EPA). Report to Congress on Indoor Air Quality: Volume 2; U.S. Environmental Protection Agency: Washington, DC, USA, 1989.
- Settimo, G.; Avino, P. The Dichotomy between Indoor Air Quality and Energy Efficiency in Light of the Onset of the COVID-19 Pandemic. Atmosphere 2021, 12, 791. [Google Scholar] [CrossRef]
- Bahnfleth, W. IAQ Control for Healthy, Resilient, Low Energy Buildings. Available online: https://blog.belimo.com/blog/iaq-control-for-healthy-resilient-low-energy-buildings (accessed on 15 June 2022).
- Megahed, N.A.; Ghoneim, E.M. Indoor Air Quality: Rethinking rules of building design strategies in post-pandemic architecture. Environ. Res. 2021, 193, 110471. [Google Scholar] [CrossRef]
- Coleman, K.K.; Nguyen, T.T.; Yadana, S.; Hansen-Estruch, C.; Lindsley, W.G.; Gray, G.C. Bioaerosol Sampling for Respiratory Viruses in Singapore’s Mass Rapid Transit Network. Sci. Rep. 2018, 8, 17476. [Google Scholar] [CrossRef] [Green Version]
- Nishiura, H.; Oshitani, H.; Kobayashi, T.; Saito, T.; Sunagawa, T.; Matsui, T.; Wakita, T.; Suzuki., M. Closed environments Facilitate Secondary Transmission of Coronavirus Disease 2019 (COVID-19). medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- International WELL Building Institute. The WELL Building Standard Version 2 Pilot; International WELL Building Institute: New York, NY, USA, 2020. [Google Scholar]
- Xiang, X.; Ma, M.; Ma, X.; Chen, L.; Cai, W.; Feng, W.; Ma, Z. Historical decarbonization of global commercial building oper-ations in the 21st century. Appl. Energy 2022, 322, 119401. [Google Scholar] [CrossRef]
- Ma, M.; Feng, W.; Huo, J.; Xiang, X. Operational carbon transition in the megalopolises’ commercial buildings. Build. Environ. 2022, 226, 109705. [Google Scholar] [CrossRef]
- Royal Academy of Engineering; National Engineering Policy Centre; CIBSE. Infection Resilient Environments: Time for a Major Upgrade. Available online: https://www.raeng.org.uk/infection-resilient-environments-2 (accessed on 15 June 2022).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Jesse, B.-J.; Heinrichs, H.U.; Kuckshinrichs, W. Adapting the theory of resilience to energy systems: A review and outlook. Energy Sustain. Soc. 2019, 9, 27. [Google Scholar] [CrossRef] [Green Version]
- Folke, C. Resilience (Republished). Ecol. Soc. 2016, 21, 44. [Google Scholar] [CrossRef]
- Cerè, G.; Rexgui, Y.; Zhao, W. Critical review of existing built environment resilience frameworks: Directions for future research. Int. J. Disaster Risk Reduct. 2017, 25, 173–189. [Google Scholar] [CrossRef]
- Roege, P.E.; Collier, Z.A.; Mancillas, J.; McDonagh, J.A.; Linkov, I. Metrics for energy resilience. Energy Policy 2014, 72, 249–256. [Google Scholar] [CrossRef]
- International Energy Agency, OECD/IEA. Making the Energy Sector more Resilient to Climate Change. Available online: https://static1.squarespace.com/static/570b03987c65e49ce6174883/t/5be2e7cdc2241b9d4d539f18/1541597137574/COP21_Resilience_Brochure-Making+the+Energy+Sector+more+Resilient+to+Climate+Change.pdf (accessed on 15 June 2022).
- Guo, X.; Wang, J.; Hu, D.; Wu, L.; Gu, L.; Wang, Y.; Zhao, J.; Zeng, L.; Zhang, J.; Wu, Y. Survey of COVID-19 Disease Among Orthopaedic Surgeons in Wuhan, People’s Republic of China. J. Bone Jt. Surg. 2020, 102, 847–854. [Google Scholar] [CrossRef]
- Bosher, L. The need for built in resilience. In Hazards and the Built Environment-Attaining Built-In Resilience; Bosher, L., Ed.; Routledge: London, UK; New York, NY, USA, 2008; pp. 3–19. [Google Scholar]
- Faller, G. The resilience of timber buildings. In Research and Applications in Structural Engineering, Mechanics, and Computation, 1st ed.; Zingoni, A., Ed.; Balkema: Rotterdam, The Netherlands, 2013. [Google Scholar]
- Champagne, C.L.; Aktas, C. Assessing the Resilience of LEED Certified Green Buildings. Procedia Eng. 2016, 145, 380–387. [Google Scholar] [CrossRef] [Green Version]
- Pearson, L.J.; Flanery, T.H. Designing, planning, and managing resilient cities: A conceptual framework. Cities 2013, 35, 89–99. [Google Scholar] [CrossRef]
- Lupíšek, A.; Růžička, J.; Tywoniak, J.; Hájek, P.; Volf, M. Criteria for evaluation of resilience of residential buildings in central Europe. Int. Rev. Appl. Sci. Eng. 2018, 9, 89–93. [Google Scholar] [CrossRef]
- Homaei, S.; Hamdy, M. Thermal resilient buildings: How to be quantified? A novel benchmarking framework and labelling metric. Build. Environ. 2021, 201, 108022. [Google Scholar] [CrossRef]
- Moazami, A.; Carlucci, S.; Geving, S. Robust and resilient buildings: A framework for defining the protection against climate uncertainty. IOP Conf. Ser. Mater. Sci. Eng. 2019, 609, 072068. [Google Scholar] [CrossRef] [Green Version]
- Haigh, R.; Amaratunga, D. Introduction: Resilience in the built environment. In Post Disaster Reconstruction of the Built Environment: Rebuilding for Resilience; Amaratunga, D., Haigh, R., Eds.; Willey-Blackwell: Oxford, UK, 2011; pp. 1–11. [Google Scholar]
- Hewitt, E.; Oberg, A.; Coronado, C.; Andrews, C. Assessing “green” and “resilient” building features using a purposeful sys-tems approach. Sustain. Cities Soc. 2019, 48, 1–20. [Google Scholar] [CrossRef]
- Sun, K.; Specian, M.; Hong, T. Nexus of thermal resilience and energy efficiency in buildings: A case study of a nursing home. Build. Environ. 2020, 177, 106842. [Google Scholar] [CrossRef]
- UN-Habitat Annual Report 2021. Available online: https://unhabitat.org/annual-report-2021 (accessed on 10 January 2023).
- Folke, C.; Carpenter, S.; Elmqvist, T.; Gunderson, L.; Holling, C.S.; Walker, B. Resilience and sustainable development: Building adaptive capacity in a world of transformations. AMBIO J. Hum. Environ. 2002, 31, 437–440. [Google Scholar] [CrossRef]
- Liu, W.; Shan, M.; Zhang, S.; Zhao, X.; Zhai, Z. Resilience in infrastructure systems: A comprehensive review. Buildings 2022, 12, 759. [Google Scholar] [CrossRef]
- Bojović, M.; Rajković, I.; Perović, S.K. Towards Resilient Residential Buildings and Neighborhoods in Light of COVID-19 Pandemic—The scenario of Podgorica, Montenegro. Sustainability 2022, 14, 1302. [Google Scholar] [CrossRef]
- Pelling, M. The Vulnerability of Cities: Natural Disasters and Social Resilience; Earthscan Publications Ltd.: London, UK, 2003. [Google Scholar]
- Cutter, S.L.; Barnes, L.; Berry, M.; Burton, C.; Evans, E.; Tate, E.; Webb, J. A place-based model for understanding community resilience to natural disasters. Glob. Environ. Change 2008, 18, 598–606. [Google Scholar] [CrossRef]
- Lizarralde, G.; Chmutina, K.; Bosher, L.; Dainty, A. Sustainability and resilience in the built environment: The challenges of establishing a turquoise agenda in the UK. Sustain. Cities Soc. 2015, 15, 96–104. [Google Scholar] [CrossRef]
- Roostaie, S.; Nawari, N.; Kibert, C. Sustainability and resilience: A review of definitions, relationships, and their integration into a combined building assessment framework. Build. Environ. 2019, 154, 132–144. [Google Scholar] [CrossRef]
- Tokazhanov, G.; Tleuken, A.; Guney, M.; Turkyilmaz, A.; Karaca, F. How is COVID-19 Experience Transforming Sustainability Requirements of Residential Buildings? A Review. Sustainability 2020, 12, 8732. [Google Scholar] [CrossRef]
- Tleuken, A.; Tokazhanov, G.; Guney, M.; Turkyilmaz, A.; Karaca, F. Readiness Assessment of Green Building Certification Systems for Residential Buildings during Pandemics. Sustainability 2021, 13, 460. [Google Scholar] [CrossRef]
- Tokazhanov, G.; Tleuken, A.; Durdyev, S.; Otesh, N.; Guney, M.; Turkyilmaz, A.; Karaca, F. Stakeholder based weights of new sustainability indicators providing pandemic resilience for residential buildings. Sustain. Cities Soc. 2021, 75, 103300. [Google Scholar] [CrossRef]
- Al-Humaiqani, M.M.; Al-Ghamdi, S.G. The built environment resilience qualities to climate change impact: Concepts, frameworks, and directions for future research. Sustain. Cities Soc. 2022, 80, 439–447. [Google Scholar] [CrossRef]
- Castaño-Rosa, R.; Pelsmakers, S.; Järventausta, H.; Poutanen, J.; Tähtinen, L.; Rashidfarokhi, A.; Toivonen, S. Resilience in the built environment: Key characteristics for solutions to multiple crises. Sustain. Cities Soc. 2022, 87, 104259. [Google Scholar] [CrossRef]
- Attia, S.; Levinson, R.; Ndongo, E.; Holzer, P.; Kazanci, O.B.; Homaei, S.; Zhang, C.; Olesen, B.W.; Qi, D.; Hamdy, M.; et al. Resilient cooling of buildings to protect against heat waves and power outages: Key concepts and definition. Energy Build. 2021, 239, 110869. [Google Scholar] [CrossRef]
- Megahed, N.A.; Ghoneim, E.M. Antivirus-built environment: Lessons learned from Covid-19 pandemic. Sustain. Cities Soc. 2020, 61, 102350. [Google Scholar] [CrossRef]
- Pinheiro, M.D.; Luís, N.C. COVID-19 Could Leverage a Sustainable Built Environment. Sustainability 2020, 12, 5863. [Google Scholar] [CrossRef]
- Cowman, K. Design Strategies for Resilient Buildings. Available online: https://www.bdcnetwork.com/blog/design-strategies-resilient-buildings (accessed on 15 June 2022).
- Leng, J.; Wang, Q.; Liu, K. Sustainable design of courtyard environment: From the perspectives of airborne diseases control and human health. Sustain. Cities Soc. 2020, 62, 102405. [Google Scholar] [CrossRef]
- Agarwal, N.; Meena, C.S.; Raj, B.P.; Saini, L.; Kumar, A.; Gopalakrishnan, N.; Kumar, A.; Balam, N.B.; Alam, T.; Kapoor, N.R.; et al. Indoor air quality improvement in COVID-19 pandemic: Review. Sustain. Cities Soc. 2021, 70, 102942. [Google Scholar] [CrossRef] [PubMed]
- Morawska, L.; Tang, J.; Bahnfleth, W.; Bluyssen, P.; Boerstra, A.; Buonanno, G. How can airborne transmission of COVID-19 indoors be minimized? Environ. Int. 2020, 142, 105832. [Google Scholar] [CrossRef] [PubMed]
- O’Keeffe, J.; Eykelbosh, A. COVID-19 and Indoor Air: Risk Mitigating Measures and Future-Proofing; National Collaborating Centre for Environmental Health: Vancouver, BC, Canada, 2021. Available online: http://www.bccdc.ca/resource-gallery/Documents/Guidelines%20and%20Forms/Guidelines%20and%20Manuals/Health-Environment/COVID-19_and_Indoor_%20Air_RiskMitigatingMeasuresAndFuture-proofing.pdf (accessed on 15 June 2022).
- Centers for Disease Control and Prevention (CDC). Hiearchy of Controls. Available online: https://www.cdc.gov/niosh/topics/hierarchy/default.html (accessed on 31 May 2022).
- Navaratnam, S.; Nguyen, K.; Selvaranjan, K.; Zhang, G.; Mendis, P.; Aye, L. Designing Post COVID-19 Buildings: Approaches for Achieving Healthy Buildings. Buildings 2022, 12, 74. [Google Scholar] [CrossRef]
- ASHRAE Epidemic Task Force. Commercial C19 Guidance. Available online: https://www.ashrae.org/File%20Library/Technical%20Resources/COVID-19/ASHRAE-Commercial-C19-Guidance.pdf (accessed on 6 June 2022).
- World Health Organization (WHO). Roadmap to Improve and Ensure Good Indoor Ventilation in the Context of COVID-19. Available online: https://www.who.int/publications/i/item/9789240021280 (accessed on 6 June 2022).
- European Centre for Disease Prevention and Control (CDC). Heating, Ventilation and Air-Conditioning Systems in the Context of COVID-19. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Heating-ventilation-air-conditioning-systems-in-the-context-of-COVID-19-first-update.pdf (accessed on 4 June 2022).
- REHVA. How to operate and use building services in order to prevent the spread of the coronavirus disease (COVID-19) virus (SARS-CoV-2) in workplaces. In REHVA COVID-19 Guidance Version 4.0; REHVA: Brussels, Belgium, 2020. [Google Scholar]
- Bolashikov, Z.; Melikov, A.; Bolashikov, Z.; Melikov, A. Methods for air cleaning and protection of building occupants from airborne pathogens. Build. Environ. 2009, 44, 1378–1385. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Leung, G.M.; Tang, J.W.; Yang, X.; Chao, C.Y.H.; Lin, J.Z.; Lu, J.W.; Nielsen, P.V.; Niu, J.; Qian, H.; et al. Role of ventilation in airborne transmission of infectious agents in the built environment? a multidisciplinary systematic review. Indoor Air 2007, 17, 2–18. [Google Scholar] [CrossRef]
- Public Health Agency of Canada. COVID-19: Guidance on Indoor Ventilation during the Pandemic. Available online: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/guidance-documents/guide-indoor-ventilation-covid-19-pandemic.html (accessed on 31 May 2022).
- Centers for Disease Control and Prevention (CDC). Ventilation in Buildings. Available online: https://www.cdc.gov/coronavirus/2019-ncov/community/ventilation.html (accessed on 10 January 2023).
- Zheng, W.; Hu, J.; Wang, Z.; Li, J.; Fu, Z.; Li, H.; Jurasz, J.; Chou, S.; Yan, J. COVID-19 Impact on Operation and Energy Consumption of Heating, Ventilation and Air-Conditioning (HVAC) Systems. Adv. Appl. Energy 2021, 3, 100040. [Google Scholar] [CrossRef]
- Santos, H.R.R.; Leal, V.M.S. Energy vs. ventilation rate in buildings: A comprehensive scenario-based assessment in the Eu-ropean context. Energy Build. 2012, 54, 111–121. [Google Scholar] [CrossRef]
- United States Environmental Protection Agency. Energy Cost and IAQ Performance of Ventilation Systems and Controls. Available online: https://www.epa.gov/sites/default/files/2015-01/documents/energy_executive_summary.pdf (accessed on 15 June 2022).
- Gao, X.; Li, Y.; Leung, G. Ventilation control of indoor transmission of airborne diseases in an urban community. Indoor Built Environ. 2009, 18, 205–218. [Google Scholar]
- Goyal, S.M.; Anantharaman, S.; Ramakrishnan, M.; Sajja, S.; Kim, S.W.; Stanley, N.J.; Farnsworth, J.E.; Kuehn, T.H.; Raynor, P.C. Detection of viruses in used ventilation filters from two large public buildings. Am. J. Infect. Control. 2011, 39, e30–e38. [Google Scholar] [CrossRef]
- EN 1822-1; High Efficiency Air Filters (EPA, HEPA and ULPA)—Part 1: Classification, Performance Testing, Marking. European Committee for Standardization: Brussels, Belgium, 2019.
- Prussin, A.J.; Marr, L.C. Sources of airborne microorganisms in the built environment. Microbiome 2015, 3, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Batterman, S.A.; Burge, H. HVAC Systems as Emission Sources Affecting Indoor Air Quality: A Critical Review. HVAC&R Res. 1995, 1, 61–78. [Google Scholar] [CrossRef]
- Pejtersen, J.; Bluyssen, P.; Kondo, H.; Clausen, G.; Fanger, P.O. Air pollution sources in ventilation systems. In Proceedings of the Clima 2000 World Congress on Heating, Ventilating, Refrigerating and Air Conditioning, Sarajevo, Yugoslavia, 27 August–1 September 1989. [Google Scholar]
- Ghezzi, S.; Pagani, I.; Poli, G.; Perboni, S.; Vicenzi, E. Rapid inactivation of severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2) by Tungsten Trioxide-based (WO3) Photocatalysis. bioRxiv 2020. [Google Scholar] [CrossRef]
- Bono, N.; Ponti, F.; Punta, C.; Candiani, G. Effect of UV Irradiation and TiO2-Photocatalysis on Airborne Bacteria and Viruses: An Overview. Materials 2021, 14, 1075. [Google Scholar] [CrossRef]
- Biloria, N.; Thakkar, Y. Integrating algae building technology in the built environment: A cost and benefit perspective. Front. Arch. Res. 2020, 9, 370–384. [Google Scholar] [CrossRef]
- Sublett, J.L. Effectiveness of Air Filters and Air Cleaners in Allergic Respiratory Diseases: A Review of the Recent Literature. Curr. Allergy Asthma Rep. 2011, 11, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Regency Lighting. Using UV LIght to Kill Viruses like COVID-19. Available online: https://insights.regencylighting.com/can-uv-light-kill-viruses-like-covid-19 (accessed on 7 June 2022).
- Biasin, M.; Bianco, A.; Pareschi, G.; Cavalleri, A.; Cavatorta, C.; Fenizia, C.; Galli, P.; Lessio, L.; Lualdi, M.; Tombetti, E.; et al. UV-C irradiation is highly effective in inactivating SARS-CoV-2 replication. Sci. Rep. 2021, 11, 6260. [Google Scholar] [CrossRef]
- Vranay, F.; Pirsel, L.; Kacik, R.; Vranayova, Z. Adaptation of HVAC Systems to Reduce the Spread of COVID-19 in Buildings. Sustainability 2020, 12, 9992. [Google Scholar] [CrossRef]
- Zeng, Y.; Manwatkar, P.; Laguerre, A.; Beke, M.; Kang, I.; Ali, A.S.; Farmer, D.K.; Gall, E.T.; Heidarinejad, M.; Stephens, B. Evaluating a commercially available in-duct bipolar ionization device for pollutant removal and potential byproduct formation. Build. Environ. 2021, 195, 107750. [Google Scholar] [CrossRef]
- European Parliament. Directive 2010/31/EU of the European Parliament and of the Council of 19 May 2010 on the Energy Performance of Buildings (Recast); European Commission: Brussels, Belgium, 2010. [Google Scholar]
- European Commission. Guide to Cost-Benefit Analysis of Investment Projects: Structural Funds, Cohesion Fund and Instrument for Pre-Accession, Directorate-General for Regional Policy; European Commission: Brussels, Belgium, 2014. [Google Scholar]
- Becchio, C.; D’Agostino, D.; Zangheri, P. Evaluation tools: Cost-optimal and cost-benefit analysis. Rehva J. 2022, 2, 5–9. [Google Scholar]
- Mitchell, R.C.; Carson, R.T. Using Surveys to Value Public Goods: The Contingent Valuation Method, 1st ed.; Resources for the Future: New York, NY, USA; Washington, DC, USA, 1989; pp. 1–484. [Google Scholar] [CrossRef]
- Haaijer, M.E. Modeling Conjoint Choice Experiments with the Probit Model; Labyrint Publications: Amsterdam, The Netherlands, 1999; pp. 1–177. [Google Scholar]
- Louviere, J. Conjoint analysis modelling of stated preferences: A review of theory, methods, recent developments and external validity. J. Transp. Econ. Policy 1988, 22, 93–119. [Google Scholar]
- Rosen, S. Hedonic Prices and Implicit Markets: Product Differentiation in Pure Competition. J. Political Econ. 1974, 82, 34–55. [Google Scholar] [CrossRef]
- Jefferson, T.; Mugford, M.; Demicheli, V. Elementary Economic Evaluation in Health Care, 2nd ed.; BMJ Book: London, UK, 2000; pp. 1–148. [Google Scholar]
- Becchio, C.; Bottero, M.C.; Corgnati, S.P.; Dell’Anna, F.; Fabi, V.; Lingua, C.; Prendin, L.; Ranieri, M. Effects on energy savings and occupant health of an antibacterial filter. In Proceedings of the E3S Web of Conference, Bucharest, Romania, 26–29 May 2019. [Google Scholar]
- Jo, C. Cost-of-illness studies: Concepts, scopes, and methods. Clin. Mol. Hepatol. 2014, 20, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Broome, J. The economic value of life. In Economica; New Series: Bristol, UK, 1985; Volume 52, pp. 281–294. [Google Scholar]
- Koopmanschap, M.A.; Rutten, F.F.; van Ineveld, B.M.; van Roijen, L. The friction cost method for measuring indirect costs of disease. J. Health Econ. 1995, 14, 171–189. [Google Scholar] [CrossRef] [PubMed]
- Richardson, L.; Loomis, J.; Kroeger, T.; Casey, F. The role of benefit transfer in ecosystem service valuation. Ecol. Econ. 2015, 115, 51–58. [Google Scholar] [CrossRef]
- Sassi, F. Calculating QALYs, comparing QALY and DALY calculations. Health Policy Plan. 2006, 21, 402–408. [Google Scholar] [CrossRef] [Green Version]
- Drummond, M.F.; Sculpher, M.J.; Claxton, K.; Stoddart, G.L.; Torrance, G.W. Methods for the Economic Evaluation of Health Care Programmes, 4th ed.; Oxford University Press: Oxford, UK, 2015; pp. 1–445. [Google Scholar]
- Anand, S.; Hanson, K. Disability-adjusted life years: A critical review. J. Health Econ. 1997, 16, 685–702. [Google Scholar] [CrossRef]
- Torrance, G.W.; Feeny, D. Utilities and Quality-Adjusted Life Years. Int. J. Technol. Assess. Health Care 1989, 5, 559–575. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Reference | Definition |
|---|---|
| [30] | “A resilient built environment as one designed, located, built, operated, and maintained in a way that maximizes the ability of built assets, associated support systems (physical and institutional) and the people that reside or work within the built assets, to withstand, recover from, and mitigate the impacts of threats” |
| [31] | “Buildings resilience could be seen as an ability to withstand the effects of earthquakes, extreme winds, flooding and fire, and their ability to be quickly returned after such event” |
| [32] | “A building’s ability to withstand severe weather and natural disasters along with its ability to recover in a timely and efficient manner if it does incur damages” |
| [33] | “The capacity of the city (built infrastructure, material flows, etc.) to undergo change while still maintaining the same structure, functions and feedbacks, and therefore identity” |
| [34] | “A single building is resilient if it has the ability to quickly adapt to changes in conditions and continue to function smoothly” |
| [35] | “The building is defined to be resilient if it is able to prepare for, absorb, adapt to and recover from the disruptive event” |
| [36] | “A resilient building is a building that not only is robust but also can fulfill its functional requirements during a major disruption. Its performance might even be disrupted but has to recover to an acceptable level in a timely manner in order to avoid disaster impacts” |
| [37] | “A resilient built environment will ensue when we design, develop and manage context sensitive buildings, spaces and places that have the capacity to resist or change in order to reduce hazard vulnerability, and enable society to continue functioning, economically, socially, when subjected to a hazard event” |
| [38] | “Resilience in buildings […] is framed as the ability of the building to serve the occupants’ needs in times of crisis or shocks. […] The capacity of a building to sustain atypical operating conditions in disaster situations, rather than succumbing to building failure, is the critical measure of its resilience” |
| [39] | “The ability of a building to prepare for, withstand, recover rapidly from, and adapt to major disruptions due to extreme weather conditions” |
| [40] | The concept of resilience in the built environment is understood as “the ability of any urban system, with its inhabitants, to maintain continuity through all shocks and stresses, while positively adapting and transforming toward sustainability” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lingua, C.; Crespi, G.; Becchio, C.; Corgnati, S.P. Designing IAQ-Resilient Post-Pandemic Buildings. Sustainability 2023, 15, 2187. https://doi.org/10.3390/su15032187
Lingua C, Crespi G, Becchio C, Corgnati SP. Designing IAQ-Resilient Post-Pandemic Buildings. Sustainability. 2023; 15(3):2187. https://doi.org/10.3390/su15032187
Chicago/Turabian StyleLingua, Carola, Giulia Crespi, Cristina Becchio, and Stefano Paolo Corgnati. 2023. "Designing IAQ-Resilient Post-Pandemic Buildings" Sustainability 15, no. 3: 2187. https://doi.org/10.3390/su15032187
APA StyleLingua, C., Crespi, G., Becchio, C., & Corgnati, S. P. (2023). Designing IAQ-Resilient Post-Pandemic Buildings. Sustainability, 15(3), 2187. https://doi.org/10.3390/su15032187