

Socio-Economic Vulnerability Assessment for Supporting a Sustainable Pandemic Management in Austria



Abstract
:1. Vulnerability and Sustainability in the Context of a Pandemic
2. Study Area
3. Method and Data
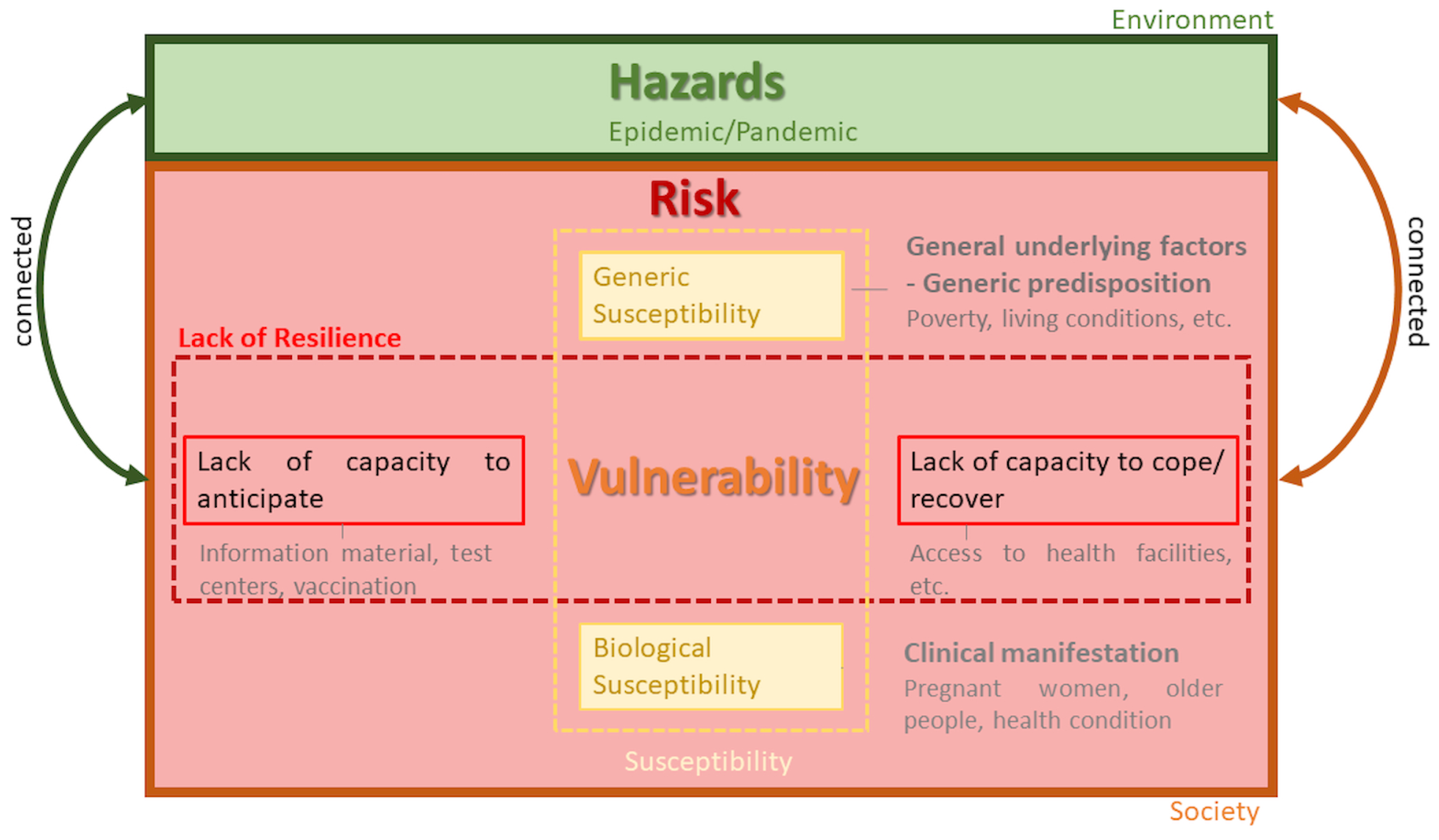
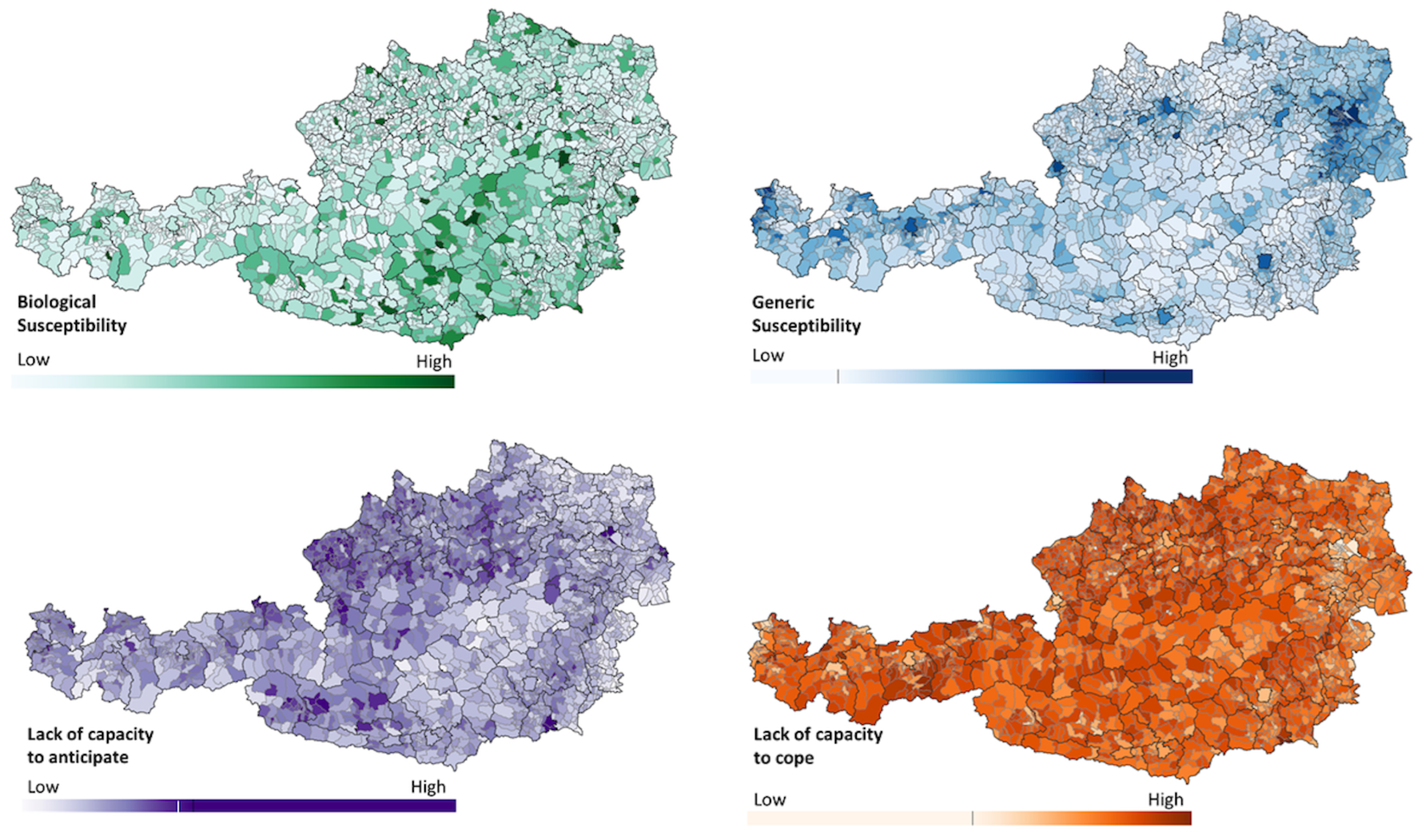
3.1. Vulnerability Assessment Framework
3.2. Indicators and Data Acquisition

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Domain | Category | Indicator (Level 1) | Indicator (Level 2) | Unit | Weights Influenza-Disease | Weights Vector-Disease | Data Source |
|---|---|---|---|---|---|---|---|
| Biological susceptibility (BS) | Health condition (BS_HC) | Care Level (BS_HC_CL) | Low care Level (1–3) [ambulant] | Percentage of people per municipality | 0.15 | 0.15 | Federal Ministry for Labor, Social Affairs, Health, and Consumer Protection (BMSGPK)/Association of Austrian Social Insurance Institutions (DVSV)—Care Allowance Statistics 2019; Gesundheit Österreich GmbH (GÖG)—G. Fülöp [41] |
| (BS_HC_CL_1) | |||||||
| High care Level (4–7) [ambulant] | 0.3 | 0.29 | |||||
| (BS_HC_CL_2) | |||||||
| Low care Level (1–3) [stationary] | 0.2 | 0.19 | |||||
| (BS_HC_CL_3) | |||||||
| High care Level (4–7) [stationary] | 0.36 | 0.37 | |||||
| (BS_HC_CL_4) | |||||||
| Generic susceptibility (GS) | Population Density (GS_PD) | Population Density (GS_P) | Number of inhabitants per km² | 0.07 | 0.06 | Statistic Austria (data as of 20 May 2019) [42]. | |
| Demography (GS_D) | Older people < 65 (GS_D_1) | Percentage of people per municipality | 0.39 | 0.39 | |||
| Children < 5 (GS_D_2) | 0.21 | 0.23 | |||||
| Teenagers 5–18 (GS_D_3) | 0.18 | 0.16 | |||||
| Women of childbearing age (16–49) (GS_D_3) | 0.22 | 0.22 | |||||
| National origin (GS_NO) | Austria (GS_NO_1) | 0.1 | 0.06 | Statistic Austria (data as of 31 October 2019 [43] | |||
| EU states (14) (GS_NO_2) | 0.05 | 0.03 | |||||
| EU states (10) (GS_NO_3) | 0.04 | 0.04 | |||||
| EU states (3) (GS_NO_4) | 0.05 | 0.05 | |||||
| Former Yugoslavia (without Slovenia, Croatia) (GS_NO_5) | 0.14 | 0.13 | |||||
| Turkey (GS_NO_6) | 0.13 | 0.15 | |||||
| EWR, Switzerland, associated small states (GS_NO_7) | 0.03 | 0.02 | |||||
| Other European states (GS_NO_8) | 0.05 | 0.04 | |||||
| Africa (GS_NO_9) | 0.12 | 0.15 | |||||
| North America (GS_NO_10) | 0.04 | 0.04 | |||||
| Latin American (GS_NO_11) | 0.08 | 0.11 | |||||
| Asia (excluding Turkey and Cyprus) (GS_NO_12) | 0.09 | 0.1 | |||||
| Oceania (GS_NO_13) | 0.08 | 0.1 | |||||
| Living situation (GS_LS) | Institutional households (nursing homes, prisons, monasteries, boarding schools, etc.) (GS_LS_1) | Number of institutions per municipality | 0.59 | 0.51 | Statistic Austria (data as of 31 October 2019) [44]. | ||
| Number of household members (GS_LS_2) | Average per municipality | 0.15 | 0.2 | ||||
| One-parent-family (only mother) (GS_LS_3) | Percentage per municipality | 0.16 | 0.13 | ||||
| One-parent-family (only father) (GS_LS_4) | 0.11 | 0.11 | |||||
| Economic situation (GS_ES) | Unemployment (GS_ES_U) | Percentage of people per municipality | 0.07 | 0.09 | Statistic Austria (data as of 30 Oktober 2021) [45]. | ||
| Lack of capacity to anticipate (LA) | Political situation (LA_PS) | Full immunization (COVID-19) | Percentage of people per municipality | 0.05 | 0.06 | Ministry of Health (2021). Basic immunized [46]. data as of 1 December 2021) | |
| Formal education (LA_FE) | Compulsory school (LA_FE_1) | 0.25 | 0.28 | Statistic Austria (data as of 31 October 2019) [43]. | |||
| Apprenticeship (LA_FE_2) | 0.12 | 0.13 | |||||
| Technical school (LA_FE_3) | 0.1 | 0.11 | |||||
| High school (LA_FE_4) | 0.09 | 0.1 | |||||
| Technical high school (LA_FE_5) | 0.09 | 0.1 | |||||
| College (LA_FE_6) | 0.07 | 0.07 | |||||
| Academy (LA_FE_7) | 0.07 | 0.07 | |||||
| University/ College (LA_FE_8) | 0.06 | 0.06 | |||||
| Not applicable (LA_FE_9) | 0.07 | 0.08 | |||||
| Lack of capacity to recover (LC) | Work (LC_W) | Primary economic sector [male] (LC_W_1) | Percentage of people per municipality | 0.1 | 0.1 | Statistic Austria (data as of 31 October 2019 [43]. | |
| Secondary economic sector [male] (LC_W_2) | 0.1 | 0.08 | |||||
| Tertiary economic sector [male] (LC_W_3) | 0.1 | 0.12 | |||||
| Private households [male] (LC_W_4) | 0.07 | 0.07 | |||||
| Exterritorial organizations [male]] (LC_W_5) | 0.05 | 0.05 | |||||
| Not applicable [male] (LC_W_6) | 0.03 | 0.04 | |||||
| Primary economic sector [female] (LC_W_7) | 0.1 | 0.1 | |||||
| Secondary economic sector [female] (LC_W_8) | 0.11 | 0.09 | |||||
| Tertiary economic sector [female] (LC_W_9) | 0.12 | 0.14 | |||||
| Private households [female] (LC_W_10) | 0.09 | 0.07 | |||||
| Exterritorial organizations [female]] (LC_W_11) | 0.05 | 0.05 | |||||
| Not applicable [female] (LC_W_12) | 0.03 | 0.04 | |||||
| Outbound commuters (LC_W_13) | 0.06 | 0.07 | |||||
| Access (LC_A) | Access to health facilities (traveling time) (LC_A_1) | Average from all raster cells for each municipality | 0.56 | 0.55 | Statistic Austria (2017). Grid-based indicators of accessibility of public utility infrastructure [47]. | ||
| Access to service centers (traveling time) (LC_A_2) | 0.44 | 0.45 | |||||
| Hospitals (LC_HF) | Systemic beds (LC_HF_1) | Number of beds per inhabitant | 0.43 | 0.43 | Gesundheit Österreich GmbH (2016). Austrian Health Information System—AHIS [48]. | ||
| Actual deployed beds (LC_HF_2) | 0.58 | 0.57 |
| Domain | Category | Indicator (Level 1) | Indicator (Level 2) | Resolution | Data Source |
|---|---|---|---|---|---|
| Biological susceptibility (BS) | Health condition (BS_HC) | Non-communicable diseases | Asthma | FS | Health survey—Statistic Austria |
| Chronic illness | |||||
| Autoimmune diseases | |||||
| Blood pressure | |||||
| Organically diseases | |||||
| Diabetic | |||||
| Communicable diseases | NA | ||||
| Vaccinations | Tetanus, Diphtheria, Measles, etc. | FS | Health survey—Statistic Austria | ||
| Mental Health | Drugs | ||||
| General well-being | |||||
| Psychological illnesses | |||||
| Physical disabilities | Seeing and hearing issues | ||||
| Mobility issues | |||||
| Generic susceptibility (GS) | Living situation (GS_LS) | Nursing staff | Mobile nursing staff | FS | |
| 24-h caretaking | |||||
| Economic situation (GS_LS) | Purchasing power | ||||
| Lack of capacity to anticipate (LA) | Trust in political institutions | NA | |||
| Criminality | |||||
| Dissemination | Media use | ||||
| Internet connection | |||||
| Formal education (LA_FE) | Illiterate | NA | |||
| Writing and Reading weakness | |||||
| Lack of capacity to recover (LC) | Health insurance | Number of insured people | NA | ||
| Language | Spoken language | ||||
| Hospitals (LC_HF) | Special medical equipment | D | |||
| Medical personal | |||||
| Intensive care unity |
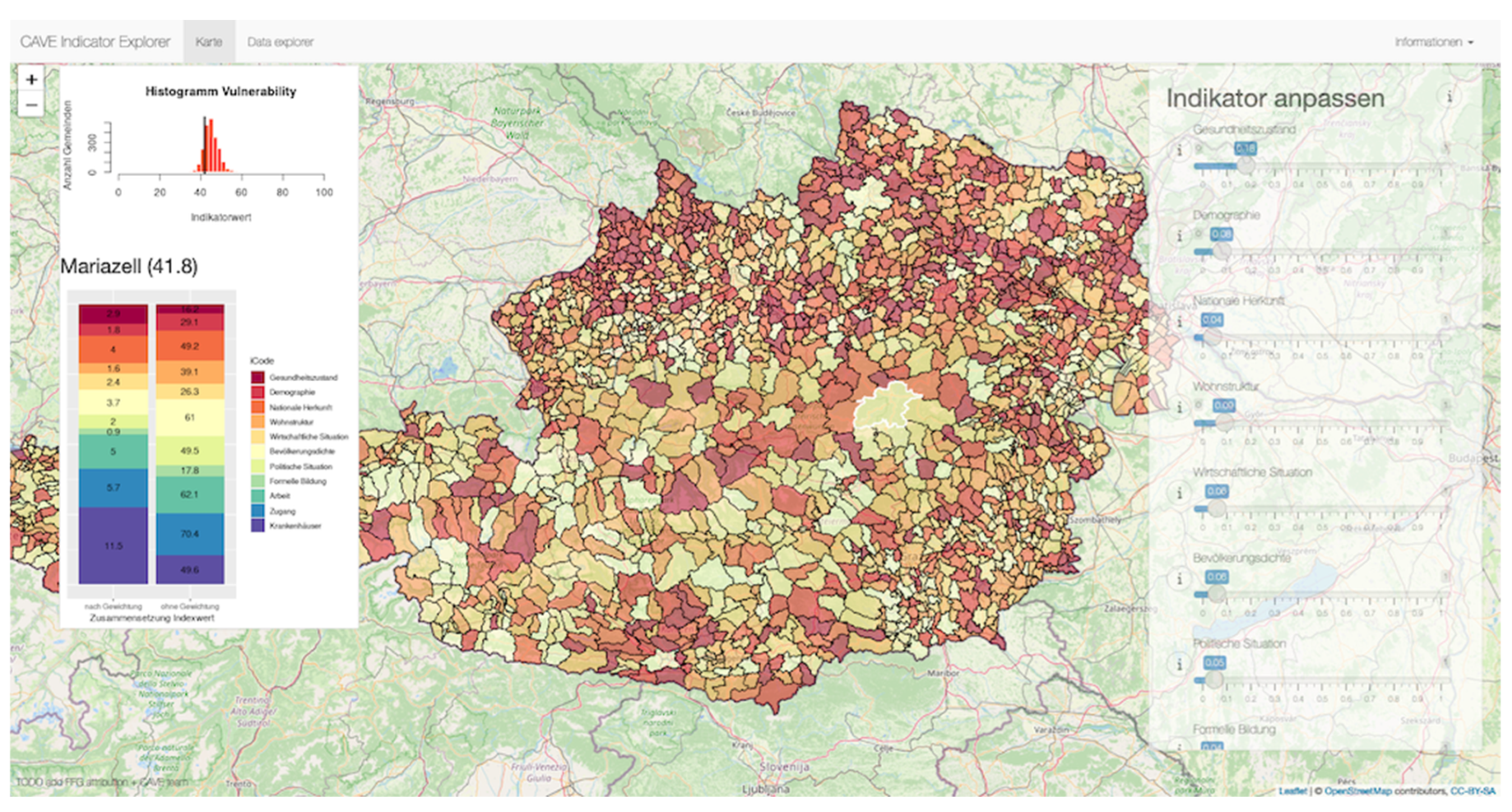
3.3. Tools
Interactive Web Map
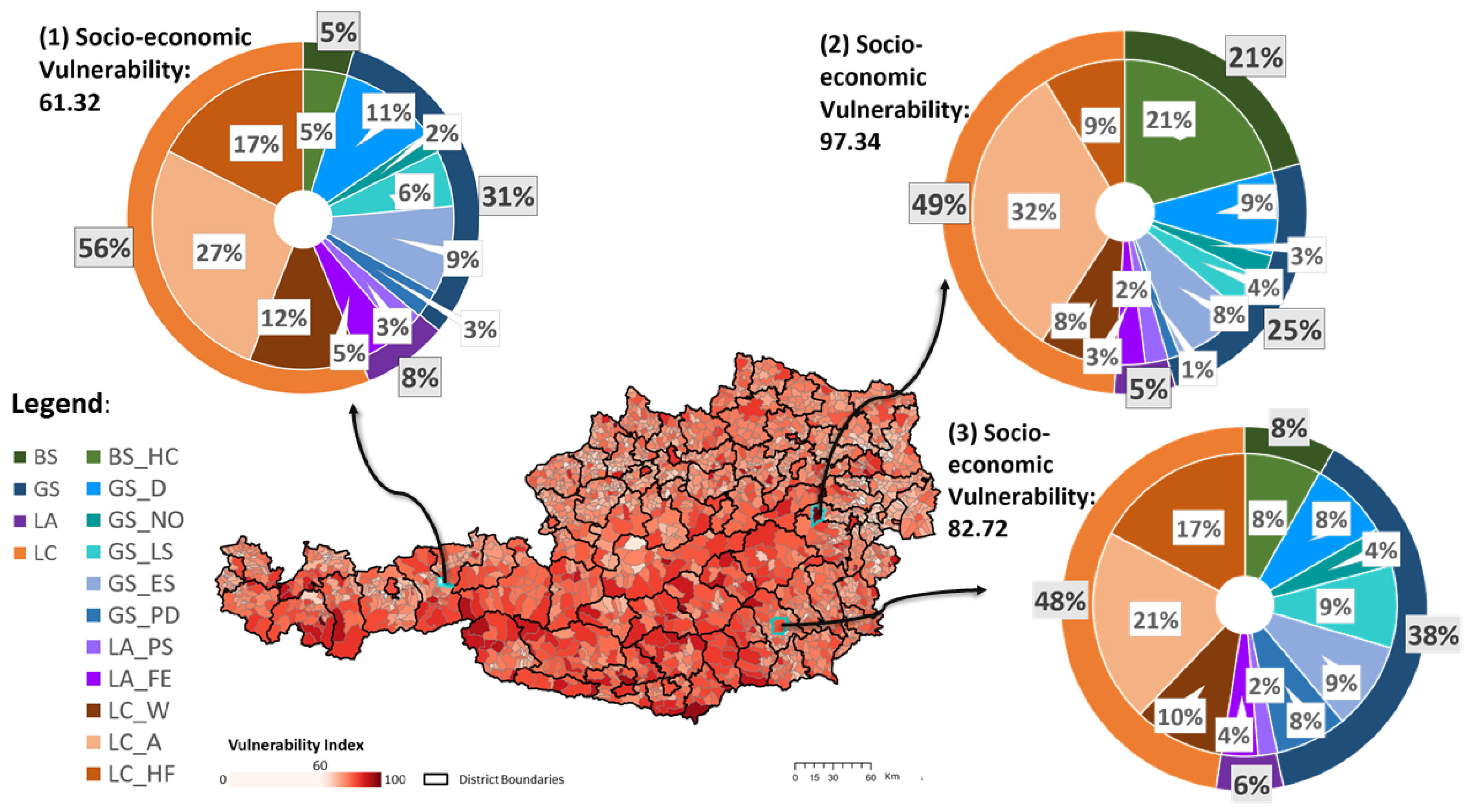
4. Results: Vulnerability Index
4.1. Socio-Economic Vulnerability to Influenza Diseases
4.2. Socio-Economic Vulnerability to Vector-Borne Diseases
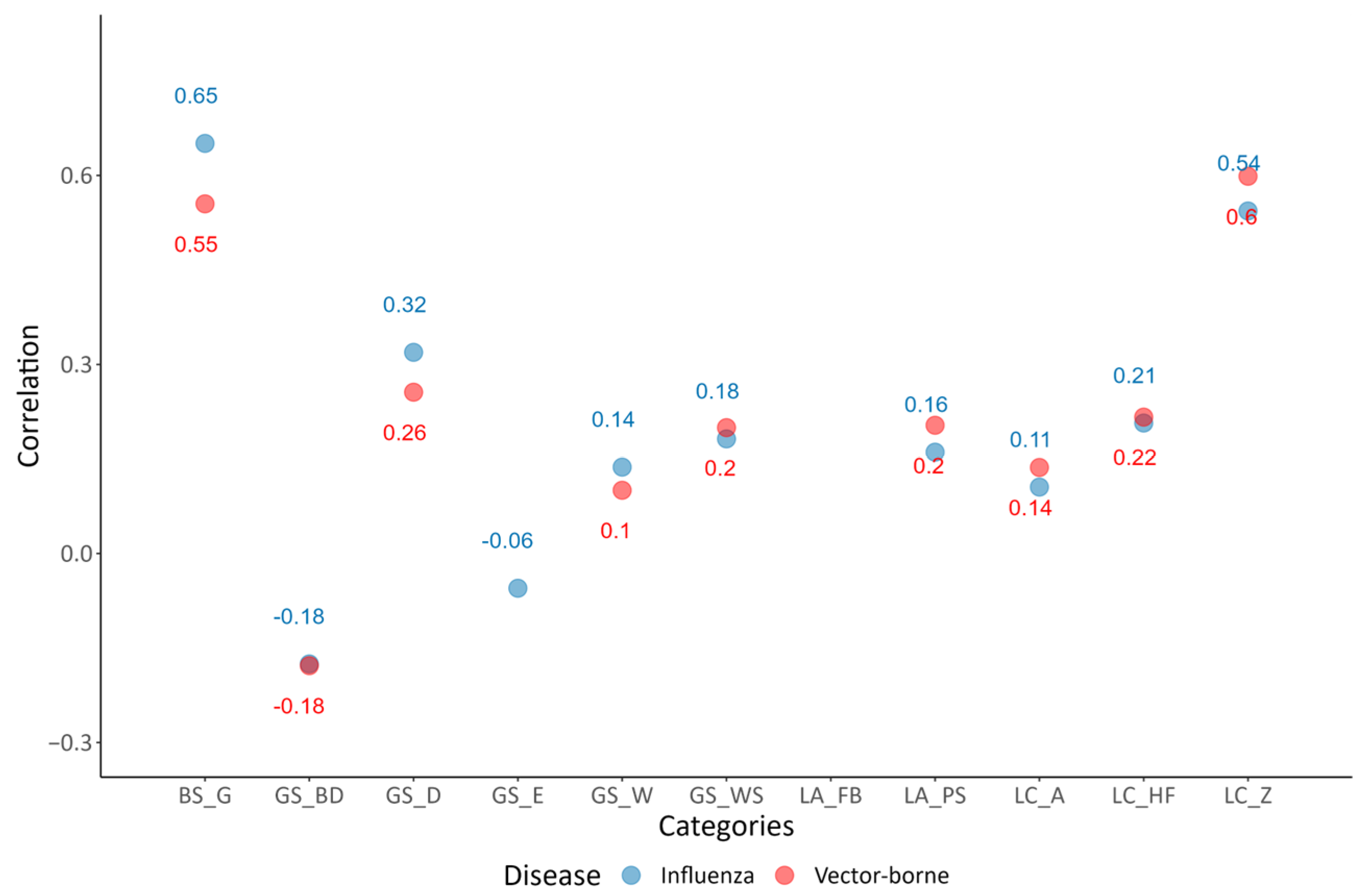
5. Validation
5.1. Comparing Influenza VI with COVID-19
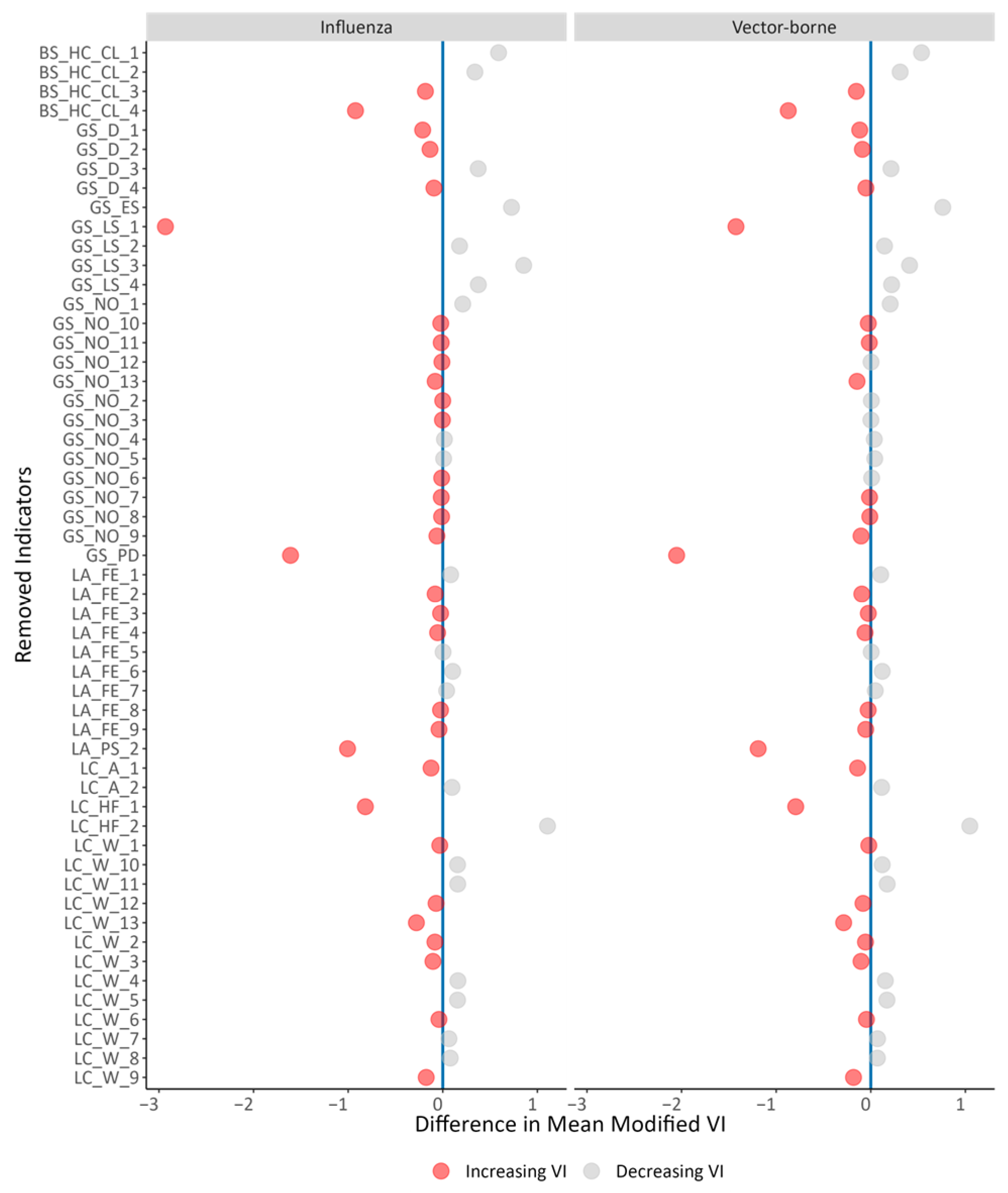
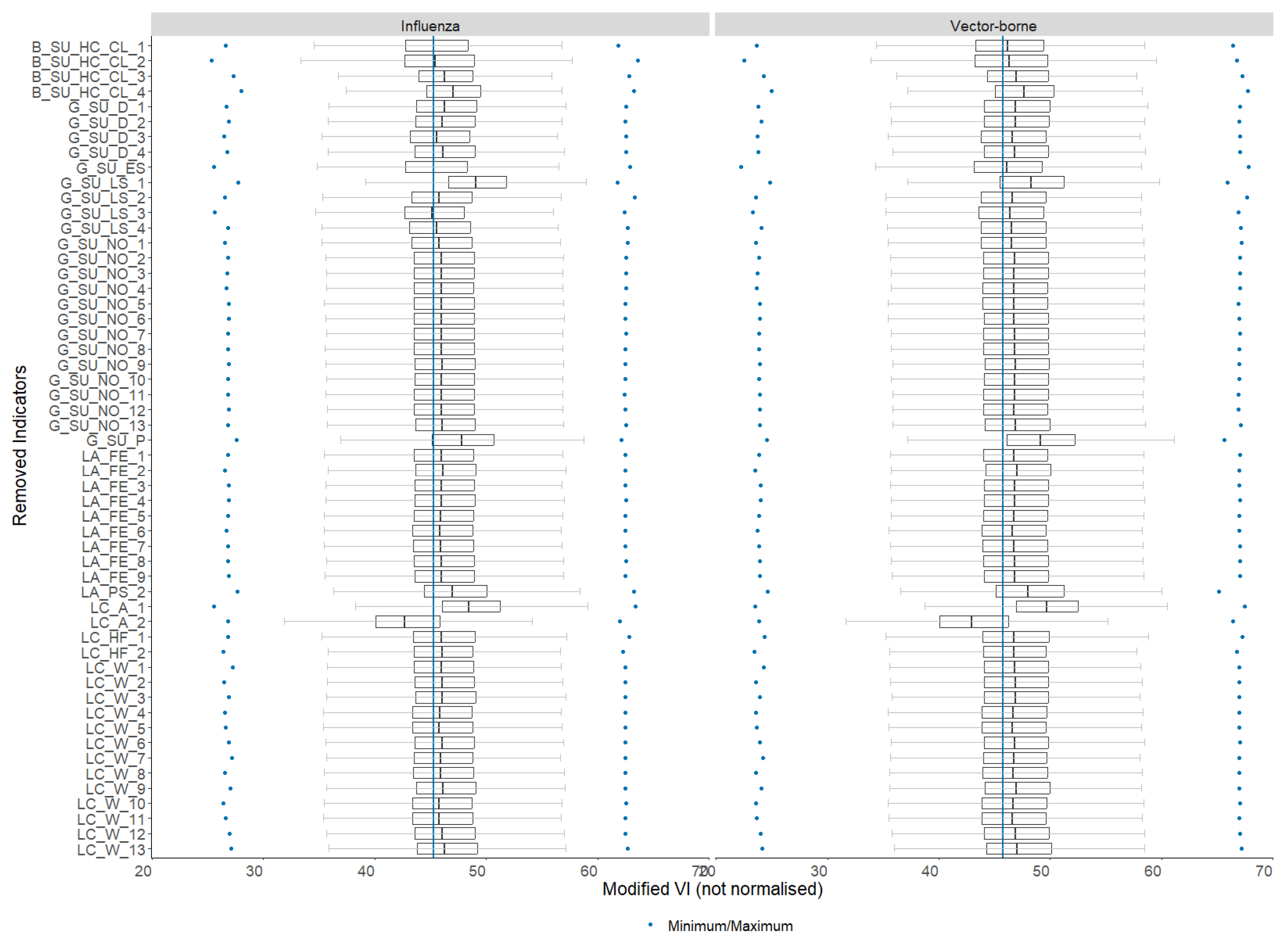
5.2. Sensitivity Analysis
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Das Deutsche Rote Kreuz. Epidemien und Pandemien: Hilfe bei Infektionsausbrüchen. Available online: https://www.drk.de/hilfe-weltweit/wann-wir-helfen/katastrophe/epidemien-pandemien/ (accessed on 12 July 2023).
- Prieto, J.; Malagón, R.; Gomez, J.; León, E. Urban Vulnerability Assessment for Pandemic Surveillance—The COVID-19 Case in Bogotá, Colombia. Sustainability 2021, 13, 3402. [Google Scholar] [CrossRef]
- Piret, J.; Boivin, G. Pandemics Throughout History. Front. Microbiol. 2021, 11. Available online: https://www.frontiersin.org/articles/10.3389/fmicb.2020.631736 (accessed on 10 August 2023).
- World Health Organization (WHO). Coronavirus Disease (COVID-19); World Health Organization: Geneva, Switzerland; Available online: https://www.who.int/health-topics/coronavirus#tab=tab_1 (accessed on 12 July 2023).
- Worldometer. Letalitätsrate Beim Coronavirus (COVID-19) in Den am Stärksten Betroffenen Ländern (Stand: 24. Juli 2023) [Graph]; Statista: New York, NY, USA, 2023; Available online: https://de.statista.com/statistik/daten/studie/1103785/umfrage/mortalitaetsrate-des-coronavirus-nach-laendern/ (accessed on 24 July 2023).
- Al-Salem, W.; Moraga, P.; Ghazi, H.; Madad, S.; Hotez, P.J. The Emergence and Transmission of COVID-19 in European Countries, 2019–2020: A Comprehensive Review of Timelines, Cases and Containment. Int. Health 2021, 13, 383–398. [Google Scholar] [CrossRef]
- Sarkodie, S.A.; Owusu, P.A. Global Assessment of Environment, Health and Economic Impact of the Novel Coronavirus (COVID-19). Environ. Dev. Sustain. 2021, 23, 5005–5015. [Google Scholar] [CrossRef] [PubMed]
- Macassa, G.; Tomaselli, G. Rethinking Developed Nations’ Health Systems through A Social Sustainability Perspective in the Light of the COVID-19 Pandemic. A Viewpoint. J. Public Health Res. 2020, 9, jphr.2020.1834. [Google Scholar] [CrossRef] [PubMed]
- Sajjad, A. The COVID-19 Pandemic, Social Sustainability and Global Supply Chain Resilience: A Review. Corp. Gov. Int. J. Bus. Soc. 2021, 21, 1142–1154. [Google Scholar] [CrossRef]
- Imran, N.; Zeshan, M.; Pervaiz, Z. Mental Health Considerations for Children & Adolescents in COVID-19 Pandemic. Pak. J. Med. Sci. 2020, 36, S67–S72. [Google Scholar] [CrossRef]
- Blanco, E.; Baier, A.; Holzmeister, F.; Jaber-Lopez, T.; Struwe, N. Substitution of Social Sustainability Concerns under the Covid-19 Pandemic. Ecol. Econ. 2022, 192, 107259. [Google Scholar] [CrossRef]
- Donkor, F.K.; Mitoulis, S.-A.; Argyroudis, S.; Aboelkhair, H.; Canovas, J.A.B.; Bashir, A.; Cuaton, G.P.; Diatta, S.; Habibi, M.; Hölbling, D.; et al. SDG Final Decade of Action: Resilient Pathways to Build Back Better from High-Impact Low-Probability (HILP) Events. Sustainability 2022, 14, 15401. [Google Scholar] [CrossRef]
- Bian, W.; Hou, H.; Chen, J.; Zhou, B.; Xia, J.; Xie, S.; Liu, T. Evaluating the Spatial Risk of Bacterial Foodborne Diseases Using Vulnerability Assessment and Geographically Weighted Logistic Regression. Remote Sens. 2022, 14, 3613. [Google Scholar] [CrossRef]
- Kienberger, S.; Hagenlocher, M. Spatial-Explicit Modeling of Social Vulnerability to Malaria in East Africa. Int. J. Health Geogr. 2014, 13, 29. [Google Scholar] [CrossRef] [PubMed]
- Macharia, P.M.; Joseph, N.K.; Okiro, E.A. A Vulnerability Index for COVID-19: Spatial Analysis at the Subnational Level in Kenya. BMJ Glob. Heal. 2020, 5, e003014. [Google Scholar] [CrossRef] [PubMed]
- Hagenlocher, M.; Hölbling, D.; Kienberger, S.; Vanhuysse, S.; Zeil, P. Spatial Assessment of Social Vulnerability in the Context of Landmines and Explosive Remnants of War in Battambang Province, Cambodia. Int. J. Disaster Risk Reduct. 2016, 15, 148–161. [Google Scholar] [CrossRef]
- Diaz-Sarachaga, J.M.; Jato-Espino, D. Analysis of Vulnerability Assessment Frameworks and Methodologies in Urban Areas. Nat. Hazards 2020, 100, 437–457. [Google Scholar] [CrossRef]
- Bizimana, J.-P.; Twarabamenye, E.; Kienberger, S. Assessing the Social Vulnerability to Malaria in Rwanda. Malar. J. 2015, 14, 2. [Google Scholar] [CrossRef] [PubMed]
- Streifeneder, V.; Kienberger, S.; Hölbling, D. Vulnerabilitätsanalyse Für Zukünftige Epidemien in Österreich. In Proceedings of the Disaster Research Days 2022, Innsbruck, Austria, 13–14 October 2022; pp. 125–127. [Google Scholar]
- Bachtrögler, J.; Firgo, M.; Fritz, O.; Klien, M.; Mayerhofer, P.; Piribauer, P.; Streicher, G. Regionale Unterschiede Der Ökonomischen Betroffenheit von Der Aktuellen COVID-19-Krise in Österreich. Ein Strukturansatz Auf Ebene Der Bundesländer [Regional Differences in the Economic Vulnerability to the Current COVID-19 Crisis in Austria]. WIFO Work. Pap. 2020, 597, 1–44. [Google Scholar]
- Simon, J.; Helter, T.M.; White, R.G.; van der Boor, C.; Łaszewska, A. Impacts of the COVID-19 Lockdown and Relevant Vulnerabilities on Capability Well-Being, Mental Health and Social Support: An Austrian Survey Study. BMC Public Health 2021, 21, 314. [Google Scholar] [CrossRef]
- WHO COVID-19 Dashboard; World Health Organization: Geneva, Switzerland, 2019; Available online: https://covid19.who.int/ (accessed on 12 July 2023).
- Birkmann, J.; Cardona, O.D.; Carreño, M.L.; Barbat, A.H.; Pelling, M.; Schneiderbauer, S.; Kienberger, S.; Keiler, M.; Alexander, D.; Zeil, P.; et al. Framing Vulnerability, Risk and Societal Responses: The MOVE Framework. Nat. Hazards 2013, 67, 193–211. [Google Scholar] [CrossRef]
- Hagenlocher, M.; Delmelle, E.; Casas, I.; Kienberger, S. Assessing Socioeconomic Vulnerability to Dengue Fever in Cali, Colombia: Statistical vs Expert-Based Modeling. Int. J. Health Geogr. 2013, 12, 36. [Google Scholar] [CrossRef]
- Rovan, J. Composite Indicators. In International Encyclopedia of Statistical Science; Lovric, M., Ed.; Springer: Berlin/Heidelberg, Germany, 2011; pp. 275–276. [Google Scholar] [CrossRef]
- Toubasi, A.A.; AbuAnzeh, R.B.; Tawileh, H.B.A.; Aldebei, R.H.; Alryalat, S.A.S. A Meta-Analysis: The Mortality and Severity of COVID-19 among Patients with Mental Disorders. Psychiatry Res. 2021, 299, 113856. [Google Scholar] [CrossRef]
- Treskova-Schwarzbach, M.; Haas, L.; Reda, S.; Pilic, A.; Borodova, A.; Karimi, K.; Koch, J.; Nygren, T.; Scholz, S.; Schönfeld, V.; et al. Pre-Existing Health Conditions and Severe COVID-19 Outcomes: An Umbrella Review Approach and Meta-Analysis of Global Evidence. BMC Med. 2021, 19, 212. [Google Scholar] [CrossRef] [PubMed]
- Wojczewski, S.; Grohma, P.; Kutalek, R. Communication Is Key: Die Rolle von Community Engagement in Der Bewältigung von COVID-19 in Österreich. In Proceedings of the Disaster Research Days 2022, Innsbruck, Austria, 13–14 October 2022; pp. 27–29. [Google Scholar]
- O’Sullivan, T.; Bourgoin, M. Vulnerability in an Influenza Pandemic: Looking Beyond Medical Risk. 2010. Available online: https://ighhub.org/sites/default/files/Lit%20Review%20-%20Vulnerability%20in%20Pandemic_FINAL.pdf (accessed on 28 August 2023).
- Venkatapuram, S. Human Capabilities and Pandemics. J. Hum. Dev. Capab. 2020, 21, 280–286. [Google Scholar] [CrossRef]
- Burton-Jeangros, C.; Duvoisin, A.; Lachat, S.; Consoli, L.; Fakhoury, J.; Jackson, Y. The Impact of the COVID-19 Pandemic and the Lockdown on the Health and Living Conditions of Undocumented Migrants and Migrants Undergoing Legal Status Regularization. Front. Public Health 2020, 8, 596887. [Google Scholar] [CrossRef] [PubMed]
- Molarius, A.; Persson, C. Living Conditions, Lifestyle Habits and Health among Adults before and after the COVID-19 Pandemic Outbreak in Sweden—Results from a Cross-Sectional Population-Based Study. BMC Public Health 2022, 22, 171. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, F.; Acharya, D.; Kumar, K.; Paudyal, V. Impact of COVID-19 Pandemic on Ethnic Minority Communities: A Qualitative Study on the Perspectives of Ethnic Minority Community Leaders. BMJ Open 2021, 11, e050584. [Google Scholar] [CrossRef] [PubMed]
- Peacock, I.; Ryo, E. A Study of Pandemic and Stigma Effects in Removal Proceedings. J. Empir. Leg. Stud. 2022, 19, 560–593. [Google Scholar] [CrossRef]
- Partida, Y. Language Barriers and the Patient Encounter. AMA J. Ethics 2007, 9, 566–571. [Google Scholar] [CrossRef]
- Libório, M.P.; Martinuci, O.S.; Bernardes, P.; Krohling, N.C.A.C.C.; Castro, G.; Guerra, H.L.; Ribeiro, E.A.; Fonzar, U.J.V.; Francisco, Í.C. Social Vulnerability and COVID-19 in Maringá, Brazil. Spat. Inf. Res. 2023, 31, 51–59. [Google Scholar] [CrossRef]
- Storopoli, J.; Braga da Silva Neto, W.L.; Mesch, G.S. Confidence in Social Institutions, Perceived Vulnerability and the Adoption of Recommended Protective Behaviors in Brazil during the COVID-19 Pandemic. Soc. Sci. Med. 2020, 265, 113477. [Google Scholar] [CrossRef]
- Kashem, S.B.; Baker, D.M.; González, S.R.; Lee, C.A. Exploring the Nexus between Social Vulnerability, Built Environment, and the Prevalence of COVID-19: A Case Study of Chicago. Sustain. Cities Soc. 2021, 75, 103261. [Google Scholar] [CrossRef]
- De Coninck, D.; D’Haenens, L.; Matthijs, K. Perceived Vulnerability to Disease and Attitudes towards Public Health Measures: COVID-19 in Flanders, Belgium. Pers. Individ. Dif. 2020, 166, 110220. [Google Scholar] [CrossRef] [PubMed]
- Sannigrahi, S.; Pilla, F.; Basu, B.; Basu, A.S.; Molter, A. Examining the Association between Socio-Demographic Composition and COVID-19 Fatalities in the European Region Using Spatial Regression Approach. Sustain. Cities Soc. 2020, 62, 102418. [Google Scholar] [CrossRef] [PubMed]
- Fülöp, G (Austrian Public Health Institute (GÖG), Vienna, Austria). Pflegegeldstatistik 2019. Bundesministerium für Arbeit, Soziales, Gesundh. und Konsum./Dachverband der österreichischen Sozialversicherungen—Pflegegeldstatistik 2019. 2019; (Personal Communication, Unpublished Work). [Google Scholar]
- Statistik Austria. Population at the Beginning of the Year 2019 (Regional Status of 2022). Available online: https://www.data.gv.at/katalog/de/dataset/stat_bevolkerungsstand-2019dbafe (accessed on 30 April 2022).
- Statistik Austria. Paket Demographie, Erwerbsstatus und Bildung—Gemeinde. Regionalstatistische Raster. Available online: https://www.statistik.at/atlas/reg-datenkatalog/ (accessed on 30 May 2022).
- Statistik Austria. Paket Haushalte—Gemeinde. Regionalstatistische Raster. Available online: https://www.statistik.at/atlas/reg-datenkatalog/ (accessed on 30 May 2022).
- Statistik Austria. Gemeindeergebnisse der Abgestimmten Erwerbsstatistik und Arbeitsstättenzählung ab 2011. Available online: http://data.statistik.gv.at (accessed on 1 July 2022).
- Dachverband der Sozialversicherungsträger, COVID-19: Impfungen auf Gemeindeebene 2020. Available online: https://www.data.gv.at/katalog/de/dataset/covid-19-impfdaten-auf-gemeindeebene-2022-11-22 (accessed on 1 June 2022).
- Saul, S. Grid-Based Indicators of Accessibility of Public Utility Infrastructure: Project Report Eurostat Grant “Merging Statistics and Geospatial Information in Member States”; (Agreement No. Agreement Number 08143.2015.001-2015.712); Statistik Austria: Vienna, Austria, 2017. [Google Scholar]
- Fülöp, G. Austrian Health Information System (AHIS); Gesundheit Österreich GmbH: Vienna, Austria, 2016. [Google Scholar]
- Greco, S.; Ishizaka, A.; Tasiou, M.; Torrisi, G. On the Methodological Framework of Composite Indices: A Review of the Issues of Weighting, Aggregation, and Robustness. Soc. Indic. Res. 2019, 141, 61–94. [Google Scholar] [CrossRef]
- Chang, W.; Cheng, J.; Allaire, J.; Sievert, C.; Schloerke, B.; Xie, Y.; Allen, J.; McPherson, J.; Dipert, A.; Borges, B. Shiny: Web Application Framework for R. 2023. Available online: https://github.com/rstudio/shiny (accessed on 15 June 2023).
- Becker, W.; Saisana, M.; Paruolo, P.; Vandecasteele, I. Weights and Importance in Composite Indicators: Closing the Gap. Ecol. Indic. 2017, 80, 12–22. [Google Scholar] [CrossRef]
- Libório, M.P.; Ekel, P.Y.; de Abreu, J.F.; Laudares, S. Factors That Most Expose Countries to COVID-19: A Composite Indicators-Based Approach. GeoJournal 2022, 87, 5435–5449. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Streifeneder, V.; Kienberger, S.; Reichel, S.; Hölbling, D. Socio-Economic Vulnerability Assessment for Supporting a Sustainable Pandemic Management in Austria. Sustainability 2024, 16, 78. https://doi.org/10.3390/su16010078
Streifeneder V, Kienberger S, Reichel S, Hölbling D. Socio-Economic Vulnerability Assessment for Supporting a Sustainable Pandemic Management in Austria. Sustainability. 2024; 16(1):78. https://doi.org/10.3390/su16010078
Chicago/Turabian StyleStreifeneder, Vanessa, Stefan Kienberger, Steffen Reichel, and Daniel Hölbling. 2024. "Socio-Economic Vulnerability Assessment for Supporting a Sustainable Pandemic Management in Austria" Sustainability 16, no. 1: 78. https://doi.org/10.3390/su16010078
APA StyleStreifeneder, V., Kienberger, S., Reichel, S., & Hölbling, D. (2024). Socio-Economic Vulnerability Assessment for Supporting a Sustainable Pandemic Management in Austria. Sustainability, 16(1), 78. https://doi.org/10.3390/su16010078