
Implementation of Sustainable Development Goal 3: Good Health and Well-Being in European Union Countries in the Context of the COVID-19 Pandemic


Abstract
:1. Introduction
- To what extent has the level of implementation of SDG 3 changed in individual EU-26 member states during the study period?
- During the analyzed period, has there been a reduction or deepening of disparities in the implementation of SDG 3 between the EU-26 countries?
2. Materials and Methods
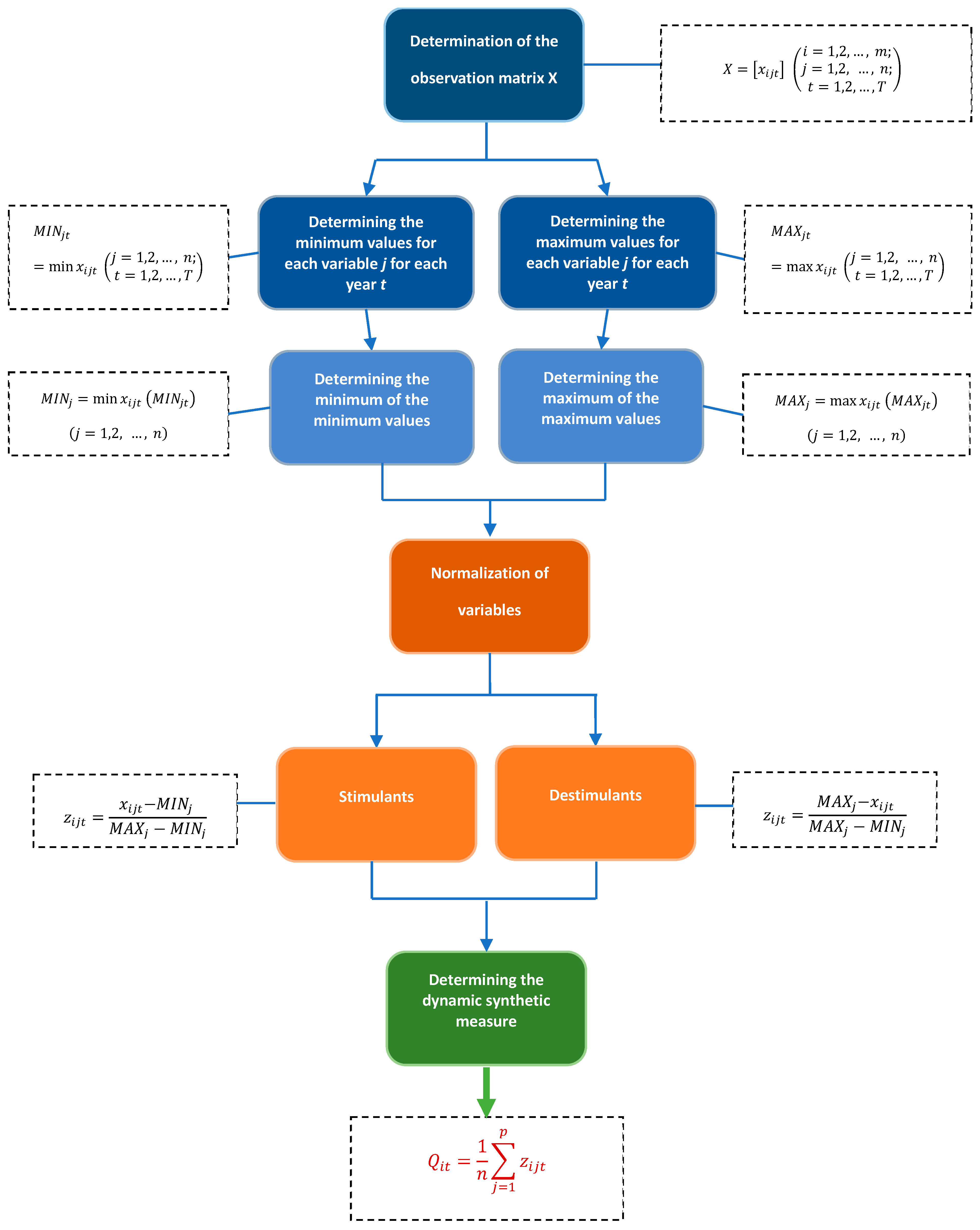
- Elimination of units of measurement for the diagnostic features;
- Reduction of the magnitude order of diagnostic variables to a comparable state, meaning equalizing the ranges of the variability of features and, consequently, enabling their aggregation;
- Equality in the range of variability of all standardized features (constant range) and uniformity in the lower and upper limits of their variability range, specifically within the interval [0, 1];
- Capability to normalize diagnostic features with positive, negative, or exclusively negative values;
- Capability to normalize features that assume a value of zero;
- Non-negative values for standardized features;
- Existence of straightforward formulas within the normalization procedure that standardize the characteristics of the variables.
- for stimulating factors:
- for destimulant factors:where zijt is the normalized value of xijt, xijt denotes the value of the j-th feature for the i-th object in year t, MINj is the minimum value that the j-th variable attains in the studied years, and MAXj is the maximum value that the j-th variable attains in the studied years.
3. Results
- Share of people with good or very good perceived health (x1);
- Self-reported unmet needs for medical care (x2);
- Standardized death rate due to tuberculosis, HIV, and hepatitis (x3);
- Preventable and treatable mortality rate (x4);
- Fatal accidents at work per 100,000 workers (x5);
- Premature deaths due to exposure to fine particulate matter PM2.5 (x6).
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Keeble, B.R. The Brundtland Report: ‘Our Common Future’. Med. War 1988, 4, 17–25. [Google Scholar] [CrossRef]
- Transforming Our World: The 2030 Agenda for Sustainable Development|Department of Economic and Social Affairs. Available online: https://sdgs.un.org/2030agenda (accessed on 30 June 2021).
- United Nations Millennium Declaration. Available online: https://www.ohchr.org/en/instruments-mechanisms/instruments/united-nations-millennium-declaration (accessed on 15 July 2024).
- Brzyska, J.; Szamrej-Baran, I. The COVID-19 Pandemic and the Implementation of Sustainable Development Goals: The EU Perspective. Sustainability 2023, 15, 13503. [Google Scholar] [CrossRef]
- European Union. Sustainable Development in the European Union—Monitoring Report on Progress towards the SDGs in an EU Context, 2023rd ed.; European Union: Brussels, Belgium, 2023; ISBN 978-92-68-00374-9. [Google Scholar]
- Acharya, S.; Lin, V.; Dhingra, N. The Role of Health in Achieving the Sustainable Development Goals. Bull. World Health Organ. 2018, 96, 591. [Google Scholar] [CrossRef] [PubMed]
- Egbende, L.; Helldén, D.; Mbunga, B.; Schedwin, M.; Kazenza, B.; Viberg, N.; Wanyenze, R.; Ali, M.M.; Alfvén, T. Interactions between Health and the Sustainable Development Goals: The Case of the Democratic Republic of Congo. Sustainability 2023, 15, 1259. [Google Scholar] [CrossRef]
- Venkatesh, G. A Brief Analysis of SDG 3—Good Health and Well-Being—And Its Synergies and Trade-Offs with the Other Sustainable Development Goals. Probl. Ekorozwoju 2022, 17, 140–147. [Google Scholar] [CrossRef]
- Howden-Chapman, P.; Siri, J.; Chisholm, E.; Chapman, R.; Doll, C.N.; Capon, A. SDG 3: Ensure Healthy Lives and Promote Wellbeing for All at All Ages. In A Guide to SDG Interactions: From Science to Implementation; International Council for Science: Paris, France, 2017; pp. 81–126. [Google Scholar]
- De Neve, J.-E.; Sachs, J.D. Sustainable Development and Human Well-Being. In World Happiness Report; Sustainable Development Solutions Network: New York, NY, USA, 2020; pp. 112–127. [Google Scholar]
- Pakkan, S.; Sudhakar, C.; Tripathi, S.; Rao, M. A Correlation Study of Sustainable Development Goal (SDG) Interactions. Qual. Quant. 2023, 57, 1937–1956. [Google Scholar] [CrossRef]
- Nunes, A.R.; Lee, K.; O’Riordan, T. The Importance of an Integrating Framework for Achieving the Sustainable Development Goals: The Example of Health and Well-Being. BMJ Glob. Health 2016, 1, e000068. [Google Scholar] [CrossRef]
- Meurs, M.; Seidelmann, L.; Koutsoumpa, M. How Healthy Is a ‘Healthy Economy’? Incompatibility between Current Pathways towards SDG3 and SDG8. Glob. Health 2019, 15, 83. [Google Scholar] [CrossRef]
- Głąbicka, K. Ochrona Zdrowia w Unii Europejskiej. Stud. Med. 2012, 26, 93–106. [Google Scholar]
- World Health Organization Constitution of the World Health Organization. Available online: https://apps.who.int/gb/bd/PDF/bd47/EN/constitution-en.pdf?ua=1 (accessed on 3 July 2024).
- World Health Organization. Good Health Adds Life to Years: Global Brief for World Health Day 2012; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Blas, E.; Kurup, A.S. Equity, Social Determinants and Public Health Programmes; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Strange, T.; Bayley, A. OECD Insights Sustainable Development Linking Economy, Society, Environment: Linking Economy, Society, Environment; OECD Publishing: Paris, France, 2008; ISBN 978-92-64-05574-2. [Google Scholar]
- Tsoukalis, L. What Kind of Europe? Oxford University Press: Oxford, NY, USA, 2003; ISBN 978-0-19-926666-1. [Google Scholar]
- Oppenheim, B.; Gallivan, M.; Madhav, N.K.; Brown, N.; Serhiyenko, V.; Wolfe, N.D.; Ayscue, P. Assessing Global Preparedness for the next Pandemic: Development and Application of an Epidemic Preparedness Index. BMJ Glob. Health 2019, 4, e001157. [Google Scholar] [CrossRef]
- GHS Index 2019. Available online: https://ghsindex.org/archive/ (accessed on 15 July 2024).
- Renda, A.; Castro, R. Towards Stronger EU Governance of Health Threats after the COVID-19 Pandemic. Eur. J. Risk Regul. 2020, 11, 273–282. [Google Scholar] [CrossRef]
- Hörisch, J. The Relation of COVID-19 to the UN Sustainable Development Goals: Implications for Sustainability Accounting, Management and Policy Research. Sustain. Account. Manag. Policy J. 2021, 12, 877–888. [Google Scholar] [CrossRef]
- Amankwah-Amoah, J. Stepping up and Stepping out of COVID-19: New Challenges for Environmental Sustainability Policies in the Global Airline Industry. J. Clean. Prod. 2020, 271, 123000. [Google Scholar] [CrossRef] [PubMed]
- Galvani, A.; Lew, A.A.; Perez, M.S. COVID-19 Is Expanding Global Consciousness and the Sustainability of Travel and Tourism. In Global Tourism and COVID-19; Routledge: London, UK, 2021; pp. 567–576. ISBN 978-1-00-322325-2. [Google Scholar]
- Yeasmin, S.; Banik, R.; Hossain, S.; Hossain, M.N.; Mahumud, R.; Salma, N.; Hossain, M.M. Impact of COVID-19 Pandemic on the Mental Health of Children in Bangladesh: A Cross-Sectional Study. Child. Youth Serv. Rev. 2020, 117, 105277. [Google Scholar] [CrossRef] [PubMed]
- Ilyas, S.; Srivastava, R.R.; Kim, H. Disinfection Technology and Strategies for COVID-19 Hospital and Bio-Medical Waste Management. Sci. Total Environ. 2020, 749, 141652. [Google Scholar] [CrossRef]
- Gavurova, B.; Megyesiova, S. Sustainable Health and Wellbeing in the European Union. Front. Public Health 2022, 10, 851061. [Google Scholar] [CrossRef] [PubMed]
- Khetrapal, S.; Bhatia, R. Impact of COVID-19 Pandemic on Health System & Sustainable Development Goal 3. Indian J. Med. Res. 2020, 151, 395. [Google Scholar] [CrossRef]
- Zambrano-Monserrate, M.A.; Ruano, M.A.; Sanchez-Alcalde, L. Indirect Effects of COVID-19 on the Environment. Sci. Total Environ. 2020, 728, 138813. [Google Scholar] [CrossRef]
- Coccia, M. Factors Determining the Diffusion of COVID-19 and Suggested Strategy to Prevent Future Accelerated Viral Infectivity Similar to COVID. Sci. Total Environ. 2020, 729, 138474. [Google Scholar] [CrossRef]
- Mestdagh, B.; Sempiga, O.; Van Liedekerke, L. The Impact of External Shocks on the Sustainable Development Goals (SDGs): Linking the COVID-19 Pandemic to SDG Implementation at the Local Government Level. Sustainability 2023, 15, 6234. [Google Scholar] [CrossRef]
- Leal Filho, W.; Brandli, L.L.; Lange Salvia, A.; Rayman-Bacchus, L.; Platje, J. COVID-19 and the UN Sustainable Development Goals: Threat to Solidarity or an Opportunity? Sustainability 2020, 12, 5343. [Google Scholar] [CrossRef]
- The Sustainable Development Goals Report 2023: Special Edition|DESA Publications. Available online: https://desapublications.un.org/publications/sustainable-development-goals-report-2023-special-edition (accessed on 15 July 2024).
- Sachs, J.; Schmidt-Traub, G.; Kroll, C.; Lafortune, G.; Fuller, G.; Woelm, F. Sustainable Development Report 2020: The Sustainable Development Goals and COVID-19 Includes the SDG Index and Dashboards; Cambridge University Press: Cambridge, UK, 2021; ISBN 978-1-108-83420-9. [Google Scholar]
- van Kersen, W.; de Rooij, M.M.; Portengen, L.; Diez, N.S.; Pieterson, I.; Tewis, M.; Boer, J.M.; Koppelman, G.; Vonk, J.M.; Vermeulen, R. Impact of COVID-19 Containment Measures on Perceived Health and Health-Protective Behavior: A Longitudinal Study. Sci. Rep. 2024, 14, 419. [Google Scholar] [CrossRef]
- Santini, Z.I.; Koyanagi, A. Loneliness and Its Association with Depressed Mood, Anxiety Symptoms, and Sleep Problems in Europe during the COVID-19 Pandemic. Acta Neuropsychiatr. 2021, 33, 160–163. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M.; Badinlou, F.; Buhrman, M.; Brocki, K.C. Psychological Impact of COVID-19 in the Swedish Population: Depression, Anxiety, and Insomnia and Their Associations to Risk and Vulnerability Factors. Eur. Psychiatry 2020, 63, e81. [Google Scholar] [CrossRef] [PubMed]
- Armbruster, S.; Klotzbücher, V. Lost in Lockdown? COVID-19, Social Distancing, and Mental Health in Germany; Diskussionsbeiträge, 2020; Available online: https://www.econstor.eu/handle/10419/218885 (accessed on 16 July 2024).
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Di Marco, A.; Rossi, A.; Siracusano, A.; Di Lorenzo, G. COVID-19 Pandemic and Lockdown Measures Impact on Mental Health Among the General Population in Italy. Front. Psychiatry 2020, 11, 790. [Google Scholar] [CrossRef]
- Adams-Prassl, A.; Boneva, T.; Golin, M.; Rauh, C. The Impact of the Coronavirus Lockdown on Mental Health: Evidence from the United States. Econ. Policy 2022, 37, 139–155. [Google Scholar] [CrossRef]
- Fisher, C.B.; Tao, X.; Liu, T.; Giorgi, S.; Curtis, B. COVID-Related Victimization, Racial Bias and Employment and Housing Disruption Increase Mental Health Risk Among U.S. Asian, Black and Latinx Adults. Front. Public Health 2021, 9, 772236. [Google Scholar] [CrossRef]
- Gama, A.; Rocha, J.V.; Marques, M.J.; Azeredo-Lopes, S.; Pedro, A.R.; Dias, S. How Did the COVID-19 Pandemic Affect Migrant Populations in Lisbon, Portugal? A Study on Perceived Effects on Health and Economic Condition. Int. J. Environ. Res. Public Health 2022, 19, 1786. [Google Scholar] [CrossRef] [PubMed]
- Gama, A.; Alves, J.; Costa, D.; Laires, P.A.; Soares, P.; Pedro, A.R.; Moniz, M.; Solinho, L.; Nunes, C.; Dias, S. Double Jeopardy from the COVID-19 Pandemic: Risk of Exposure and Income Loss in Portugal. Int. J. Equity Health 2021, 20, 231. [Google Scholar] [CrossRef]
- Marmet, S.; Wicki, M.; Gmel, G.; Gachoud, C.; Daeppen, J.-B.; Bertholet, N.; Studer, J. The Psychological Impact of the COVID-19 Crisis Is Higher among Young Swiss Men with a Lower Socioeconomic Status: Evidence from a Cohort Study. PLoS ONE 2021, 16, e0255050. [Google Scholar] [CrossRef]
- Rathnayake, D.; Clarke, M.; Jayasinghe, V.I. Health System Performance and Health System Preparedness for the Post-Pandemic Impact of COVID-19: A Review. Int. J. Healthc. Manag. 2021, 14, 250–254. [Google Scholar] [CrossRef]
- Lin, Q.; Paykin, S.; Halpern, D.; Martinez-Cardoso, A.; Kolak, M. Assessment of Structural Barriers and Racial Group Disparities of COVID-19 Mortality with Spatial Analysis. JAMA Netw. Open 2022, 5, e220984. [Google Scholar] [CrossRef] [PubMed]
- Vandentorren, S.; Smaïli, S.; Chatignoux, E.; Maurel, M.; Alleaume, C.; Neufcourt, L.; Kelly-Irving, M.; Delpierre, C. The Effect of Social Deprivation on the Dynamic of SARS-CoV-2 Infection in France: A Population-Based Analysis. Lancet Public Health 2022, 7, e240–e249. [Google Scholar] [CrossRef]
- Pinto, A.d.S.; Rodrigues, C.A.; Nascimento, C.L.; Cruz, L.A.D.; Santos, E.G.D.; Nunes, P.C.; Costa, M.G.R.; Rocha, M.O.D.C. COVID-19 Epidemic Curve in Brazil: A Sum of Multiple Epidemics, Whose Inequality and Population Density in the States Are Correlated with Growth Rate and Daily Acceleration. An Ecological Study. Rev. Da Soc. Bras. De Med. Trop. 2022, 55, e0118. [Google Scholar] [CrossRef] [PubMed]
- Malmusi, D.; Pasarín, M.I.; Marí-Dell’Olmo, M.; Artazcoz, L.; Diez, E.; Tolosa, S.; Rodríguez-Sanz, M.; Pérez, G.; Peña-Gallardo, C.; Borrell, C. Multi-Level Policy Responses to Tackle Socioeconomic Inequalities in the Incidence of COVID-19 in a European Urban Area. Int. J. Equity Health 2022, 21, 28. [Google Scholar] [CrossRef] [PubMed]
- Grzebyk, M.; Stec, M.; Hejdukova, P. Implementation of Sustainable Development Goal 8 in European Union Countries–A Measurement Concept and a Multivariate Comparative Analysis. Sustain. Dev. 2023, 31, 2758–2769. [Google Scholar] [CrossRef]
- Kiselakova, D.; Stec, M.; Grzebyk, M.; Sofrankova, B. A Multidimensional Evaluation of the Sustainable Development of European Union Countries—An Empirical Study. J. Compet. 2020, 12, 56–73. [Google Scholar] [CrossRef]
- Fura, B.; Wang, Q. The Level of Socioeconomic Development of EU Countries and the State of ISO 14001 Certification. Qual. Quant. 2017, 51, 103–119. [Google Scholar] [CrossRef]
- Momete, D.C. Rational Development as a Sustainable Progress Welfare Vector: A Cross-Country Analysis. Sustain. Dev. 2017, 25, 189–199. [Google Scholar] [CrossRef]
- Information on Data—Eurostat. Available online: https://ec.europa.eu/eurostat/web/sdi/information-data (accessed on 27 August 2024).
- Eurostat Database. Selected Dataset. Sustainable Development Indicators. Available online: https://ec.europa.eu/eurostat/web/sdi/database (accessed on 10 June 2024).
- Bonner, W.I.A.; Weiler, R.; Orisatoki, R.; Lu, X.; Andkhoie, M.; Ramsay, D.; Yaghoubi, M.; Steeves, M.; Szafron, M.; Farag, M. Determinants of Self-Perceived Health for Canadians Aged 40 and Older and Policy Implications. Int. J. Equity Health 2017, 16, 94. [Google Scholar] [CrossRef] [PubMed]
- Glossary: Self-Perceived Health. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Glossary:Self-perceived_health (accessed on 27 August 2024).
- Grabiński, T. Wybrane problemy dynamicznej wielowymiarowej analizy porównawczej. Ruch Praw. Ekon. I Socjol. 1985, 47, 189–206. [Google Scholar]
- Bożek, J.; Szewczyk, J.; Badach, E.; Lisek, S. Ocena Poziomu Rozwoju Gospodarczego Województw z Zastosowaniem Metod Porządkowania Liniowego w Ujęciu Dynamicznym. Wiadomości Statystyczne. Pol. Stat. 2022, 67, 39–61. [Google Scholar]
- Sompolska-Rzechuła, A.; Kurdyś-Kujawska, A. Generation of Young Adults Living with Their Parents in European Union Countries. Sustainability 2022, 14, 4272. [Google Scholar] [CrossRef]
- Sompolska-Rzechuła, A. Selection of the Optimal Way of Linear Ordering of Objects: Case of Sustainable Development in EU Countries. Stat. Stat. Econ. J. 2021, 101, 24–36. [Google Scholar]
- Kukuła, K. Metoda Unitaryzacji Zerowanej Na Tle Wybranych Metod Normowania Cech Diagnostycznych (Zero Unitari-Sation Method against Selected Methods of Normalizing Diagnostic Features). Acta Sci. Acad. Ostroviensis 1999, 4, 5–31. [Google Scholar]
- Kukuła, K. Metoda Unitaryzacji Zerowanej; PWN: Warszawa, Poland, 2000; ISBN 83-01-13097-0. [Google Scholar]
- Kukuła, K. Analiza Własności Metody Unitaryzacji Zerowanej. Zesz. Nauk. SGGW-Ekon. I Organ. Gospod. Żywnościowej 2000, 42, 5–17. [Google Scholar] [CrossRef]
- Environmental Noise in Europe. 2020. Available online: https://www.eea.europa.eu/publications/environmental-noise-in-europe (accessed on 20 August 2024).
- Garmarudi, A.B.; Ghasemi, K.; Mozaffari, F.; Khorani, M.; Khanmohammadi, M. Most Common Techniques of Outlier Detection. Curr. Appl. Chemom. 2015, 12, 253–274. [Google Scholar]
- Cousineau, D.; Chartier, S. Outliers Detection and Treatment: A Review. Int. J. Psychol. Res. 2010, 3, 58–67. [Google Scholar] [CrossRef]
- Trzęsiok, M. Wybrane metody identyfikacji obserwacji oddalonych. Pr. Nauk. Uniw. Ekon. We Wrocławiu 2014, 327, 157–166. [Google Scholar]
- Sompolska-Rzechuła, A.; Kurdyś-Kujawska, A. Assessment of the Development of Poverty in EU Countries. Int. J. Environ. Res. Public Health 2022, 19, 3950. [Google Scholar] [CrossRef]
- Tukey, J.W. Exploratory Data Analysis; Reading, Mass.; Addison-Wesley Pub. Co.: Reading, MA, USA, 1977; ISBN 978-0-201-07616-5. [Google Scholar]
- Łuczak, A.; Kalinowski, S. Assessing the Level of the Material Deprivation of European Union Countries. PLoS ONE 2020, 15, e0238376. [Google Scholar] [CrossRef] [PubMed]
- Kendall, M.G. A New Measure of Rank Correlation. Biometrika 1938, 30, 81–93. [Google Scholar] [CrossRef]
- OECD. Netherlands: Country Health Profile 2023; Organisation for Economic Co-operation and Development: Paris, France, 2023. [Google Scholar] [CrossRef]
- OECD. Sweden: Country Health Profile 2023; Organisation for Economic Co-operation and Development: Paris, France, 2023. [Google Scholar] [CrossRef]
- Lupu, D.; Tiganasu, R. COVID-19 and the Efficiency of Health Systems in Europe. Health Econ. Rev. 2022, 12, 14. [Google Scholar] [CrossRef] [PubMed]
- OECD. Slovakia: Country Health Profile 2023; Organisation for Economic Co-operation and Development: Paris, France, 2023. [Google Scholar] [CrossRef]
- Willi, S.; Lüthold, R.; Hunt, A.; Hänggi, N.V.; Sejdiu, D.; Scaff, C.; Bender, N.; Staub, K.; Schlagenhauf, P. COVID-19 Sequelae in Adults Aged Less than 50 Years: A Systematic Review. Travel Med. Infect. Dis. 2021, 40, 101995. [Google Scholar] [CrossRef] [PubMed]
- Duncan, G.E.; Avery, A.R.; Seto, E.; Tsang, S. Perceived Change in Physical Activity Levels and Mental Health during COVID-19: Findings among Adult Twin Pairs. PLoS ONE 2020, 15, e0237695. [Google Scholar] [CrossRef]
- Findlay, L.C.; Arim, R.; Kohen, D. Understanding the Perceived Mental Health of Canadians during the COVTD-19 Pandemic. Health Rep. 2020, 31, 22–27. [Google Scholar] [PubMed]
- Ramage-Morin, P.L.; Polsky, J.Y. Health-Related Concerns and Precautions during the COVID-19 Pandemic: A Comparison of Canadians with and without Underlying Health Conditions. Health Rep. 2020, 31, 3–8. [Google Scholar] [PubMed]
- Yan, A.F.; Sun, X.; Zheng, J.; Mi, B.; Zuo, H.; Ruan, G.; Hussain, A.; Wang, Y.; Shi, Z. Perceived Risk, Behavior Changes and Health-Related Outcomes during COVID-19 Pandemic: Findings among Adults with and without Diabetes in China. Diabetes Res. Clin. Pract. 2020, 167, 108350. [Google Scholar] [CrossRef]
- Sarkar, D.; Jung, M.K.; Wang, H.J. Alcohol and the Immune System. Alcohol Res. Curr. Rev. 2015, 37, 153. [Google Scholar]
- De Bruin, W.B.; Bennett, D. Relationships between Initial COVID-19 Risk Perceptions and Protective Health Behaviors: A National Survey. Am. J. Prev. Med. 2020, 59, 157–167. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A. Impact of COVID-19 Pandemic on Mental Health in the General Population: A Systematic Review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Gao, J.; Zheng, P.; Jia, Y.; Chen, H.; Mao, Y.; Chen, S.; Wang, Y.; Fu, H.; Dai, J. Mental Health Problems and Social Media Exposure during COVID-19 Outbreak. PLoS ONE 2020, 15, e0231924. [Google Scholar]
- Moghanibashi-Mansourieh, A. Assessing the Anxiety Level of Iranian General Population during COVID-19 Outbreak. Asian J. Psychiatry 2020, 51, 102076. [Google Scholar] [CrossRef] [PubMed]
- Davillas, A.; Jones, A.M. Unmet Health Care Need and Income-Related Horizontal Equity in Use of Health Care during the COVID-19 Pandemic. Health Econ. 2021, 30, 1711–1716. [Google Scholar] [CrossRef] [PubMed]
- Janjani, H.; Aghaei, M.; Yunesian, M. Risk Factors Affecting the Mortality of COVID-19 Patients: Impacts of Modifiable Factors. Iran. J. Health Environ. 2021, 14, 363–378. [Google Scholar]
- Vera-Delgado, V.; García-Rosado, D.; Pérez-Hernández, O.; Martín-Ponce, E.; de La Paz-Estrello, A.M.; García-Marichal, C.; Pérez-Fernández, S.; Rodríguez-Morón, V.; Alemán-Valls, R.; González-Reimers, E. Mortality and COVID Infection: Predictors of Mortality 10 Months after Discharge. Diseases 2024, 12, 123. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Zhong, W.; Bian, Z.; Li, Z.; Zhang, K.; Liang, B.; Zhong, Y.; Hu, M.; Lin, L.; Liu, J. A Comparison of Mortality-Related Risk Factors of COVID-19, SARS, and MERS: A Systematic Review and Meta-Analysis. J. Infect. 2020, 81, e18–e25. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Fang, X.; Cai, Z.; Wu, X.; Gao, X.; Min, J.; Wang, F. Comorbid Chronic Diseases and Acute Organ Injuries Are Strongly Correlated with Disease Severity and Mortality among COVID-19 Patients: A Systemic Review and Meta-Analysis. Research 2020, 2020, 2402961. [Google Scholar] [CrossRef]
- Santurtún, A.; Shaman, J. Work Accidents, Climate Change and COVID-19. Sci. Total Environ. 2023, 871, 162129. [Google Scholar] [CrossRef]
- Huber, D.; Frank, R.; Crevenna, R. The Impact of Lockdowns during the COVID-19 Pandemic on Work-Related Accidents in Austria in 2020. Wien. Klin. Wochenschr. 2022, 134, 391–398. [Google Scholar] [CrossRef]
- Clay, K.; Lewis, J.; Severnini, E. Pollution, Infectious Disease, and Mortality: Evidence from the 1918 Spanish Influenza Pandemic. J. Econ. Hist. 2018, 78, 1179–1209. [Google Scholar] [CrossRef]
- Cui, Y.; Zhang, Z.-F.; Froines, J.; Zhao, J.; Wang, H.; Yu, S.-Z.; Detels, R. Air Pollution and Case Fatality of SARS in the People’s Republic of China: An Ecologic Study. Environ. Health 2003, 2, 15. [Google Scholar] [CrossRef]
- Bourdrel, T.; Annesi-Maesano, I.; Alahmad, B.; Maesano, C.N.; Bind, M.-A. The Impact of Outdoor Air Pollution on COVID-19: A Review of Evidence from in Vitro, Animal, and Human Studies. Eur. Respir. Rev. 2021, 30, 200242. [Google Scholar] [CrossRef] [PubMed]
- Mehmood, K.; Iqbal, M.; Abrar, M.M. Can Exposure to PM2. 5 Particles Increase the Incidence of Coronavirus Disease 2019 (COVID-19)? Sci. Total Environ. 2020, 741, 140441. [Google Scholar] [CrossRef]
- Zoran, M.A.; Savastru, R.S.; Savastru, D.M.; Tautan, M.N. Assessing the Relationship between Surface Levels of PM2. 5 and PM10 Particulate Matter Impact on COVID-19 in Milan, Italy. Sci. Total Environ. 2020, 738, 139825. [Google Scholar] [CrossRef]
- Renard, J.-B.; Surcin, J.; Annesi-Maesano, I.; Delaunay, G.; Poincelet, E.; Dixsaut, G. Relation between PM2. 5 Pollution and COVID-19 Mortality in Western Europe for the 2020–2022 Period. Sci. Total Environ. 2022, 848, 157579. [Google Scholar] [CrossRef] [PubMed]
- Commission Communication—Solidarity in Health: Reducing Health Inequalities in the EU—European Commission. Available online: https://health.ec.europa.eu/social-determinants/overview/commission-communication-solidarity-health-reducing-health-inequalities-eu_en (accessed on 27 August 2024).
- OECD. Health at a Glance 2021: OECD Indicators; Organisation for Economic Co-operation and Development: Paris, France, 2021. [Google Scholar]
- Drawing Light from the Pandemic: A New Strategy for Health and Sustainable Development—A Review of the Evidence. Available online: https://www.who.int/europe/publications/i/item/9789289051798 (accessed on 8 September 2024).
- A Global Deal for Our Pandemic Age. Available online: https://www.bruegel.org/external-publication/global-deal-our-pandemic-age (accessed on 7 September 2024).
- OECD. Access to COVID-19 Vaccines: Global Approaches in a Global Crisis; OECD: Paris, France, 2021. [Google Scholar]
- Mathieu, E.; Ritchie, H.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Hasell, J.; Macdonald, B.; Dattani, S.; Beltekian, D.; Ortiz-Ospina, E.; et al. Coronavirus Pandemic (COVID-19); Our World in Data: Oxford, UK, 2020. [Google Scholar]
- Beyond Containment: Health Systems Responses to COVID-19 in the OECD. Available online: https://www.oecd.org/en/publications/2020/04/beyond-containment-health-systems-responses-to-covid-19-in-the-oecd_ed89ef4f.html (accessed on 7 September 2024).
- OECD. Strengthening the Frontline: How Primary Health Care Helps Health Systems Adapt during the COVID 19 Pandemic; OECD: Paris, France, 2021. [Google Scholar]
- OECD. Health at a Glance: Europe 2020: State of Health in the EU Cycle; Organisation for Economic Co-operation and Development: Paris, France, 2020. [Google Scholar]
- OECD. Flattening the COVID-19 Peak: Containment and Mitigation Policies; OECD: Paris, France, 2020. [Google Scholar]
- Bourguignon, M.; Joan, D.; Doignon, Y.; Eggerickx, T.; Fontaine, S.; Lusyne, P.; Plavsic, A.; Sanderson, J.-P. Surmortalité Liée à La COVID-19 En Belgique: Variations Spatiales et Socio-Démographiques; HAL: Bangalore, India, 2020. [Google Scholar]
- Mateo-Urdiales, A.; Fabiani, M.; Rosano, A.; Vescio, M.F.; Del Manso, M.; Bella, A.; Riccardo, F.; Pezzotti, P.; Regidor, E.; Andrianou, X. Socioeconomic Patterns and COVID-19 Outcomes before, during and after the Lockdown in Italy (2020). Health Place 2021, 71, 102642. [Google Scholar] [CrossRef] [PubMed]
- Decoster, A.; Minten, T.; Spinnewijn, J. The Income Gradient in Mortality during the COVID-19 Crisis: Evidence from Belgium. J. Econ. Inequal. 2021, 19, 551–570. [Google Scholar] [CrossRef] [PubMed]
- Berchet, C.; Bijlholt, J.; Ando, M. Socio-Economic and Ethnic Health Inequalities in COVID-19 Outcomes across OECD Countries; OECD: Paris, France, 2023. [Google Scholar]
- Drefahl, S.; Wallace, M.; Mussino, E.; Aradhya, S.; Kolk, M.; Brandén, M.; Malmberg, B.; Andersson, G. A Population-Based Cohort Study of Socio-Demographic Risk Factors for COVID-19 Deaths in Sweden. Nat. Commun. 2020, 11, 5097. [Google Scholar] [CrossRef]
- Une Hausse Des Décès Deux Fois plus Forte Pour Les Personnes Nées à l’étranger Que Pour Celles Nées En France En Mars-Avril 2020—Insee Focus—198. Available online: https://www.insee.fr/fr/statistiques/4627049 (accessed on 7 September 2024).
- Hansson, E.; Albin, M.; Rasmussen, M.; Jakobsson, K. Large Differences in Excess Mortality in March-May 2020 by Country of Birth in Sweden. Lakartidningen 2020, 117, 20113. [Google Scholar]

{kind=link}
| Indicator Name | Definition |
|---|---|
| Share of people with good or very good perceived health (x1) | The indicator is a subjective measure of how people rate their overall health on a scale from “very good” to “very poor.” It is expressed as the percentage of the population aged 16 and over who consider their health to be “good” or “very good”. Unit of measurement: % of the population aged 16 and over. |
| Self-reported unmet needs for medical care (x2) | The indicator measures the proportion of the population aged 16 and over reporting unmet medical care needs for any of the following reasons: “financial reasons”, “waiting list”, and “too far to travel” (all three categories are combined). Unmet needs, as reported by the individual, refer to their assessment of whether they needed medical examinations or treatment (excluding dental care) but did not receive it or did not seek it. Unit of measurement: % of the population aged 16 and over. |
| Standardized death rate due to tuberculosis, HIV, and hepatitis (x3) | The indicator measures the standardized mortality rate due to tuberculosis, HIV, and hepatitis. The rate is calculated by dividing the number of individuals dying from the selected infectious diseases by the total population. The data are presented as standardized mortality rates, meaning they are adjusted to a standard age distribution to measure mortality rates independently of different age structures within populations. Unit of measurement: per 100,000 individuals. |
| Preventable and treatable mortality rate (x4) | This indicator includes both preventable and treatable causes of mortality. Preventable mortality refers to deaths that can be avoided mainly through effective public health interventions and primary prevention (i.e., before the onset of disease/injury to reduce incidence). Treatable mortality can be avoided mainly through timely and effective healthcare interventions, including secondary prevention and treatment (after the onset of disease to reduce mortality). The data are presented as standardized mortality rates, adjusted to a standard age distribution to measure mortality rates independently of different population age structures. Unit of measurement: number per 100,000 people under the age of 75. |
| Fatal accidents at work per 100,000 workers (x5) | The indicator measures the number of fatal occupational accidents that occur during work and result in the death of the victim within one year of the accident. Unit of measurement: number per 100,000 workers. |
| Premature deaths due to exposure to fine particulate matter PM2.5 (x6) | This indicator estimates the number of premature deaths attributable to long-term exposure to PM2.5 concentrations above 5 µg/m3 (the level recommended by the World Health Organization). PM2.5 refers to particulate matter with a diameter of fewer than 2.5 μm, which can penetrate deep into the lungs, causing inflammation and exacerbating conditions such as heart and lung diseases. Unit of measurement: number of deaths per 100,000 inhabitants. |
| Variable | Year | Mean | Median | Min | Max | Standard Deviation | Coefficient of Variation | Skewness |
|---|---|---|---|---|---|---|---|---|
| x1 | 2019 | 66.93 | 67.90 | 46.20 | 84.30 | 9.53 | 14.23 | −0.61 |
| 2020 | 67.96 | 69.20 | 44.30 | 84.50 | 9.41 | 13.84 | −0.77 | |
| 2021 | 67.73 | 68.50 | 47.90 | 81.70 | 8.50 | 12.55 | −0.89 | |
| x2 | 2019 | 2.04 | 1.40 | 0.00 | 5.86 | 1.78 | 87.11 | 0.93 |
| 2020 | 2.02 | 1.55 | 0.00 | 5.73 | 1.85 | 91.65 | 0.95 | |
| 2021 | 2.10 | 1.70 | 0.10 | 5.28 | 1.66 | 78.84 | 0.61 | |
| x3 | 2019 | 1.92 | 1.26 | 0.42 | 5.60 | 1.69 | 88.00 | 1.27 |
| 2020 | 1.85 | 1.20 | 0.43 | 5.27 | 1.53 | 82.90 | 1.41 | |
| 2021 | 1.71 | 1.08 | 0.38 | 5.22 | 1.60 | 93.72 | 1.48 | |
| x4 | 2019 | 284.46 | 228.13 | 170.21 | 504.81 | 111.91 | 39.34 | 0.81 |
| 2020 | 312.81 | 238.96 | 183.26 | 593.20 | 131.83 | 42.14 | 0.86 | |
| 2021 | 353.95 | 248.53 | 177.48 | 694.80 | 177.68 | 50.20 | 0.82 | |
| x5 | 2019 | 1.97 | 1.90 | 0.48 | 3.53 | 0.88 | 44.51 | 0.12 |
| 2020 | 2.02 | 1.82 | 0.30 | 4.45 | 1.00 | 49.59 | 0.41 | |
| 2021 | 1.94 | 1.79 | 0.33 | 4.29 | 1.01 | 52.02 | 0.59 | |
| x6 | 2019 | 48.45 | 41.00 | 3.00 | 94.30 | 29.35 | 60.58 | 0.17 |
| 2020 | 47.62 | 36.00 | 1.00 | 105.00 | 33.21 | 69.75 | 0.45 | |
| 2021 | 54.18 | 41.50 | 3.00 | 112.40 | 36.74 | 67.80 | 0.23 |
| EU Country | The Value of the Synthetic Variable | Ranking Position | The Value of the Synthetic Variable | Ranking Position | The Value of the Synthetic Variable | Ranking Position |
|---|---|---|---|---|---|---|
| 2019 | 2020 | 2021 | ||||
| The Netherlands | 0.888 | 2 | 0.913 | 1 | 0.888 | 1 |
| Sweden | 0.894 | 1 | 0.903 | 2 | 0.879 | 2 |
| Luxembourg | 0.803 | 5 | 0.837 | 4 | 0.852 | 3 |
| Ireland | 0.851 | 3 | 0.845 | 3 | 0.849 | 4 |
| Cyprus | 0.754 | 10 | 0.673 | 13 | 0.805 | 5 |
| Belgium | 0.774 | 8 | 0.788 | 8 | 0.793 | 6 |
| Denmark | 0.772 | 9 | 0.809 | 5 | 0.791 | 7 |
| Germany | 0.786 | 7 | 0.796 | 7 | 0.779 | 8 |
| Finland | 0.742 | 11 | 0.737 | 10 | 0.774 | 9 |
| Malta | 0.844 | 4 | 0.798 | 6 | 0.757 | 10 |
| Spain | 0.794 | 6 | 0.755 | 9 | 0.753 | 11 |
| Austria | 0.702 | 12 | 0.736 | 11 | 0.723 | 12 |
| France | 0.685 | 13 | 0.696 | 12 | 0.652 | 13 |
| Czechia | 0.682 | 14 | 0.666 | 14 | 0.649 | 14 |
| Slovenia | 0.675 | 15 | 0.648 | 15 | 0.622 | 15 |
| Greece | 0.609 | 17 | 0.619 | 16 | 0.613 | 16 |
| Portugal | 0.553 | 18 | 0.536 | 19 | 0.576 | 17 |
| Croatia | 0.513 | 19 | 0.507 | 21 | 0.527 | 18 |
| Slovakia | 0.626 | 16 | 0.584 | 17 | 0.505 | 19 |
| Poland | 0.502 | 21 | 0.541 | 18 | 0.478 | 20 |
| Hungary | 0.509 | 20 | 0.533 | 20 | 0.467 | 21 |
| Bulgaria | 0.494 | 22 | 0.435 | 23 | 0.424 | 22 |
| Estonia | 0.431 | 23 | 0.499 | 22 | 0.417 | 23 |
| Lithuania | 0.341 | 24 | 0.321 | 24 | 0.249 | 24 |
| Romania | 0.285 | 25 | 0.251 | 26 | 0.240 | 25 |
| Latvia | 0.280 | 26 | 0.292 | 25 | 0.166 | 26 |
| Max | 0.894 | 0.913 | 0.888 | |||
| Min | 0.280 | 0.251 | 0.166 | |||
| Range | 0.614 | 0.661 | 0.722 | |||
| Average | 0.646 | 0.643 | 0.624 | |||
| Coefficient of variation | 27.53947 | 28.12259 | 32.5184 | |||
| EU Country | |||
|---|---|---|---|
| The Netherlands | 0.025 | −0.024 | 0.001 |
| Sweden | 0.009 | −0.023 | −0.015 |
| Luxembourg | 0.034 | 0.014 | 0.048 |
| Ireland | −0.006 | 0.004 | −0.002 |
| Cyprus | −0.081 | 0.133 | 0.052 |
| Belgium | 0.014 | 0.005 | 0.019 |
| Denmark | 0.036 | −0.018 | 0.018 |
| Germany | 0.010 | −0.016 | −0.007 |
| Finland | −0.005 | 0.037 | 0.032 |
| Malta | −0.046 | −0.041 | −0.087 |
| Spain | −0.039 | −0.002 | −0.041 |
| Austria | 0.033 | −0.012 | 0.021 |
| France | 0.011 | −0.044 | −0.033 |
| Czechia | −0.016 | −0.017 | −0.033 |
| Slovenia | −0.027 | −0.026 | −0.053 |
| Greece | 0.010 | −0.006 | 0.004 |
| Portugal | −0.016 | 0.040 | 0.024 |
| Croatia | −0.006 | 0.020 | 0.014 |
| Slovakia | −0.042 | −0.079 | −0.122 |
| Poland | 0.039 | −0.063 | −0.025 |
| Hungary | 0.024 | −0.066 | −0.042 |
| Bulgaria | −0.059 | −0.011 | −0.069 |
| Estonia | 0.068 | −0.082 | −0.013 |
| Lithuania | −0.020 | −0.072 | −0.092 |
| Romania | −0.033 | −0.012 | −0.045 |
| Latvia | 0.012 | −0.125 | −0.114 |
| Year | 2019 | 2020 | 2021 |
|---|---|---|---|
| 2019 | 1.00 | 0.89 | 0.86 |
| 2020 | 0.89 | 1.00 | 0.86 |
| 2021 | 0.86 | 0.86 | 1.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mikuła, A.; Raczkowska, M.; Utzig, M. Implementation of Sustainable Development Goal 3: Good Health and Well-Being in European Union Countries in the Context of the COVID-19 Pandemic. Sustainability 2024, 16, 7921. https://doi.org/10.3390/su16187921
Mikuła A, Raczkowska M, Utzig M. Implementation of Sustainable Development Goal 3: Good Health and Well-Being in European Union Countries in the Context of the COVID-19 Pandemic. Sustainability. 2024; 16(18):7921. https://doi.org/10.3390/su16187921
Chicago/Turabian StyleMikuła, Aneta, Małgorzata Raczkowska, and Monika Utzig. 2024. "Implementation of Sustainable Development Goal 3: Good Health and Well-Being in European Union Countries in the Context of the COVID-19 Pandemic" Sustainability 16, no. 18: 7921. https://doi.org/10.3390/su16187921