
Effectiveness of a Sustainable Training Program Combining Supervised Outdoor Exercise with Telecoaching on Physical Performance in Elderly People

 ,
,  , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
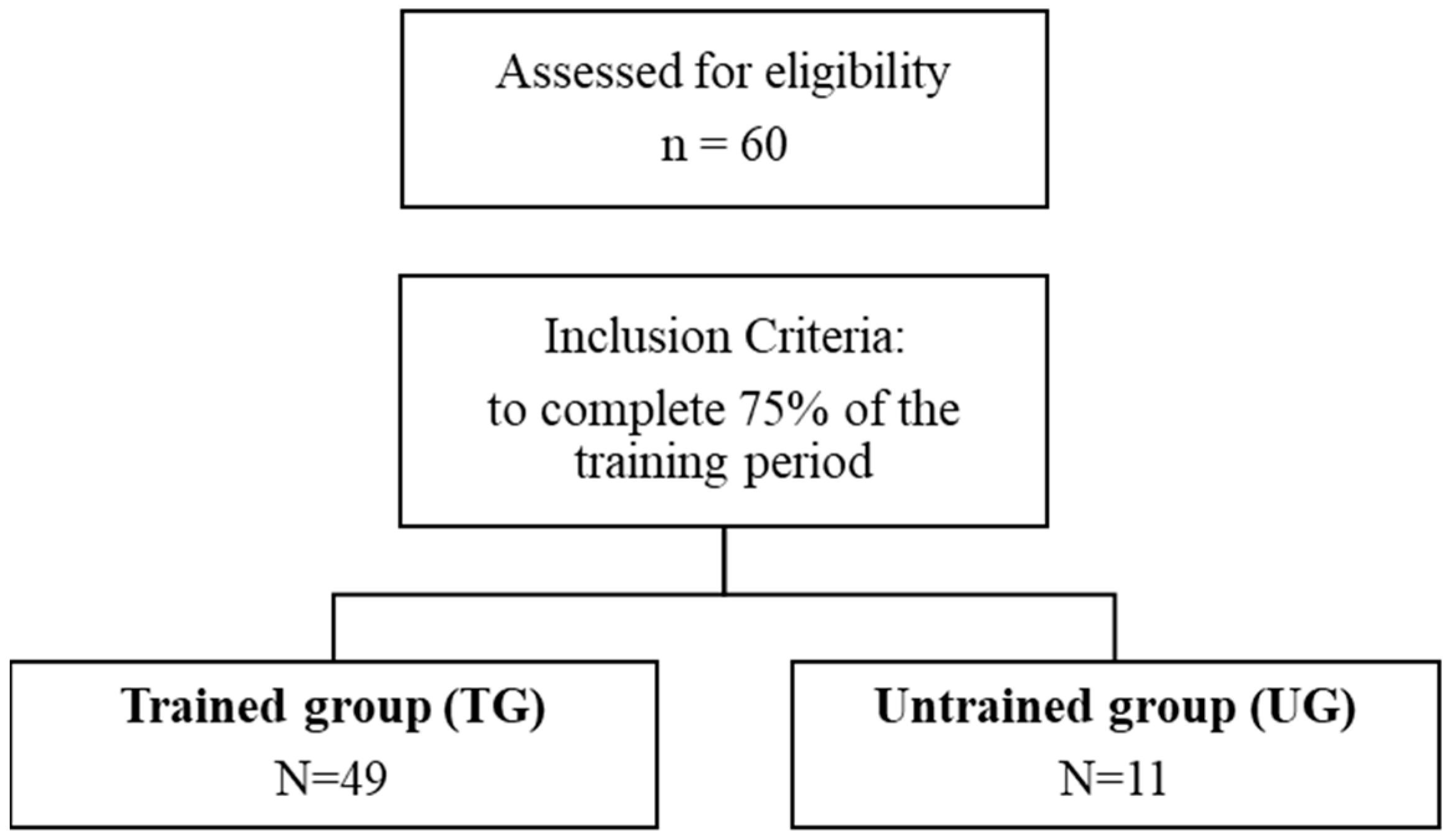
2.2. Participants
2.3. Measurements
- I.
- Anthropometric measurements
- II.
- Handgrip test
- III.
- Timed Up and Go (TUG) test
- IV.
- Short physical performance battery (SPPB)
- V.
- Tinetti Scale
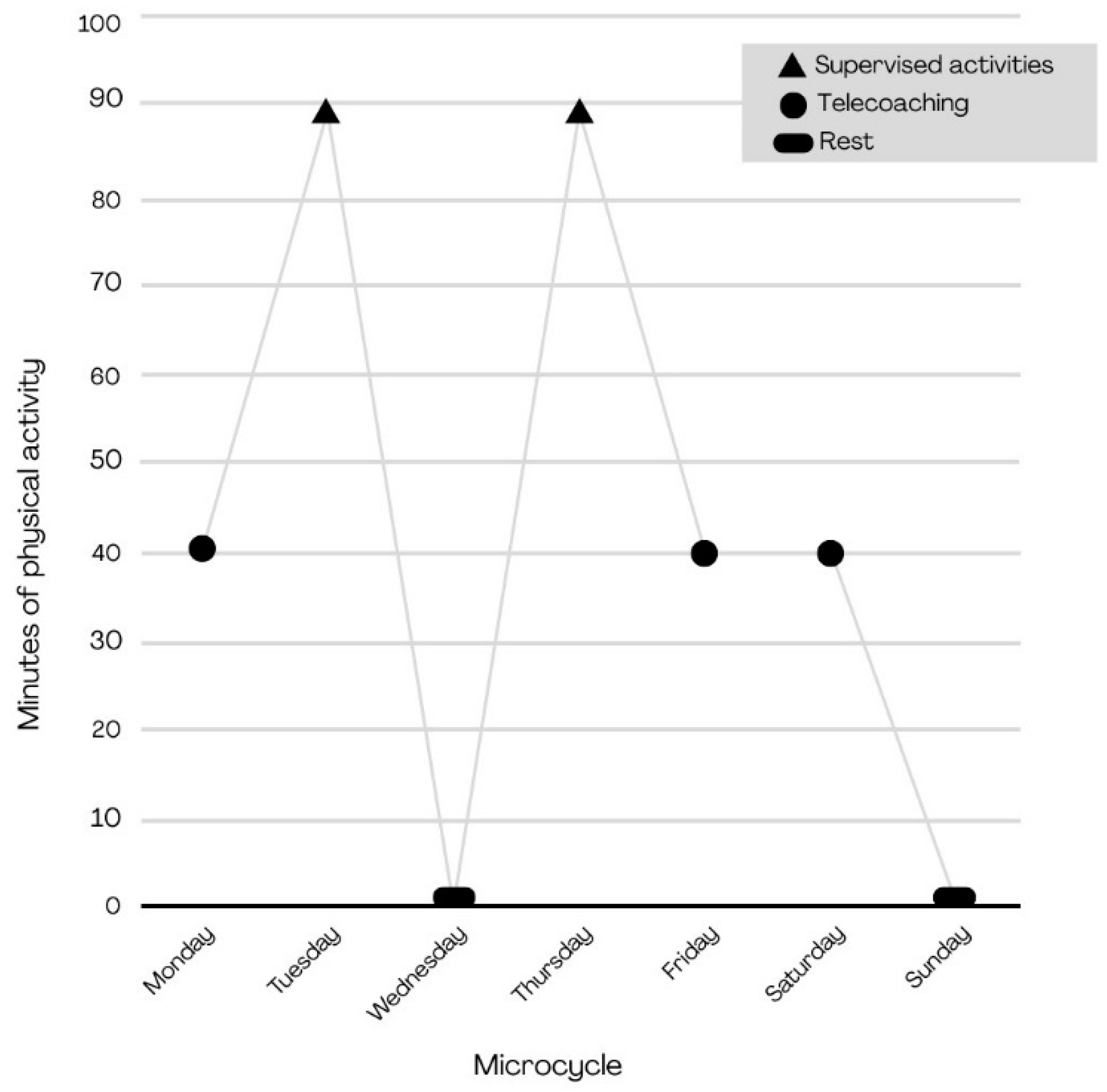
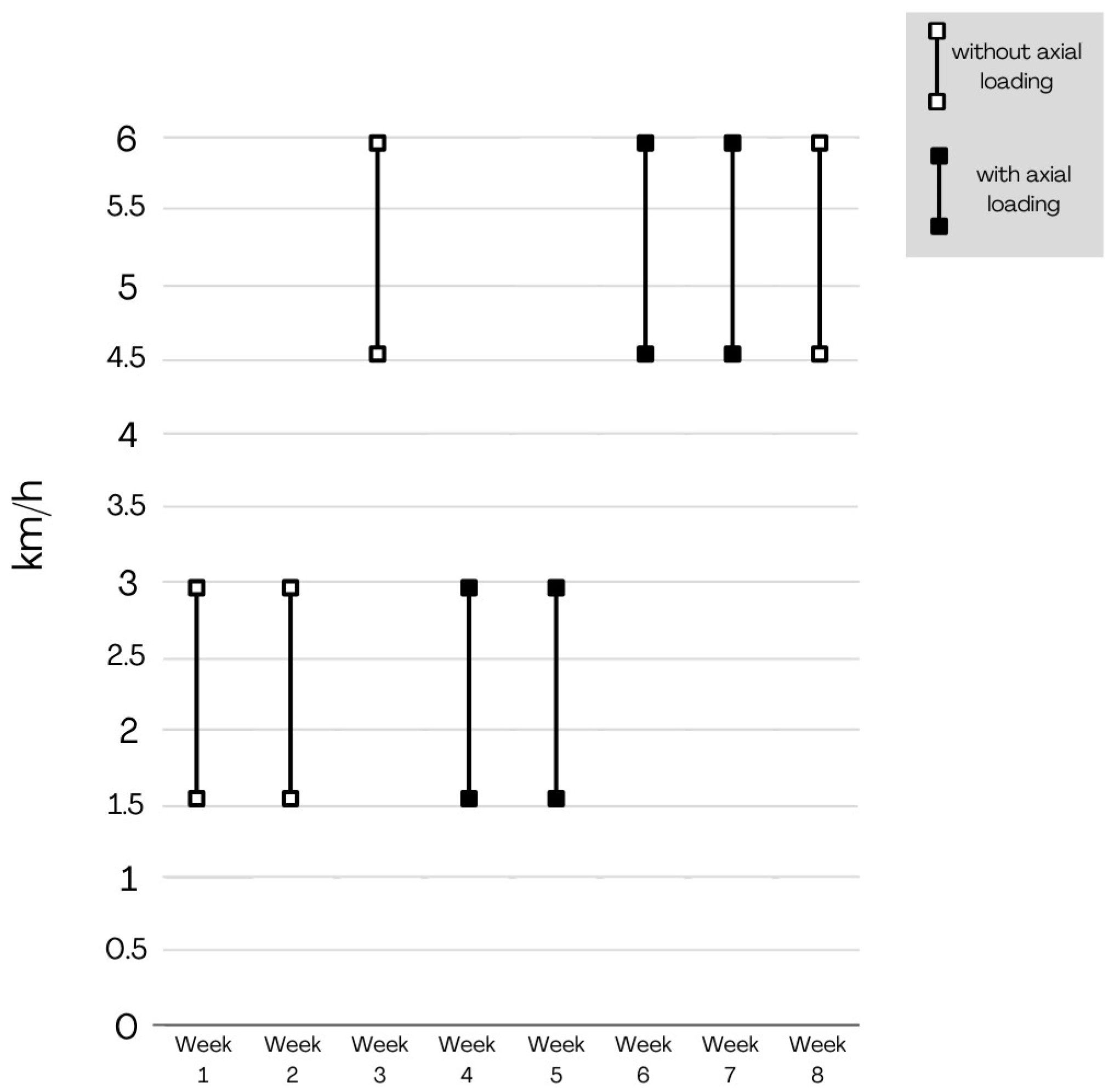
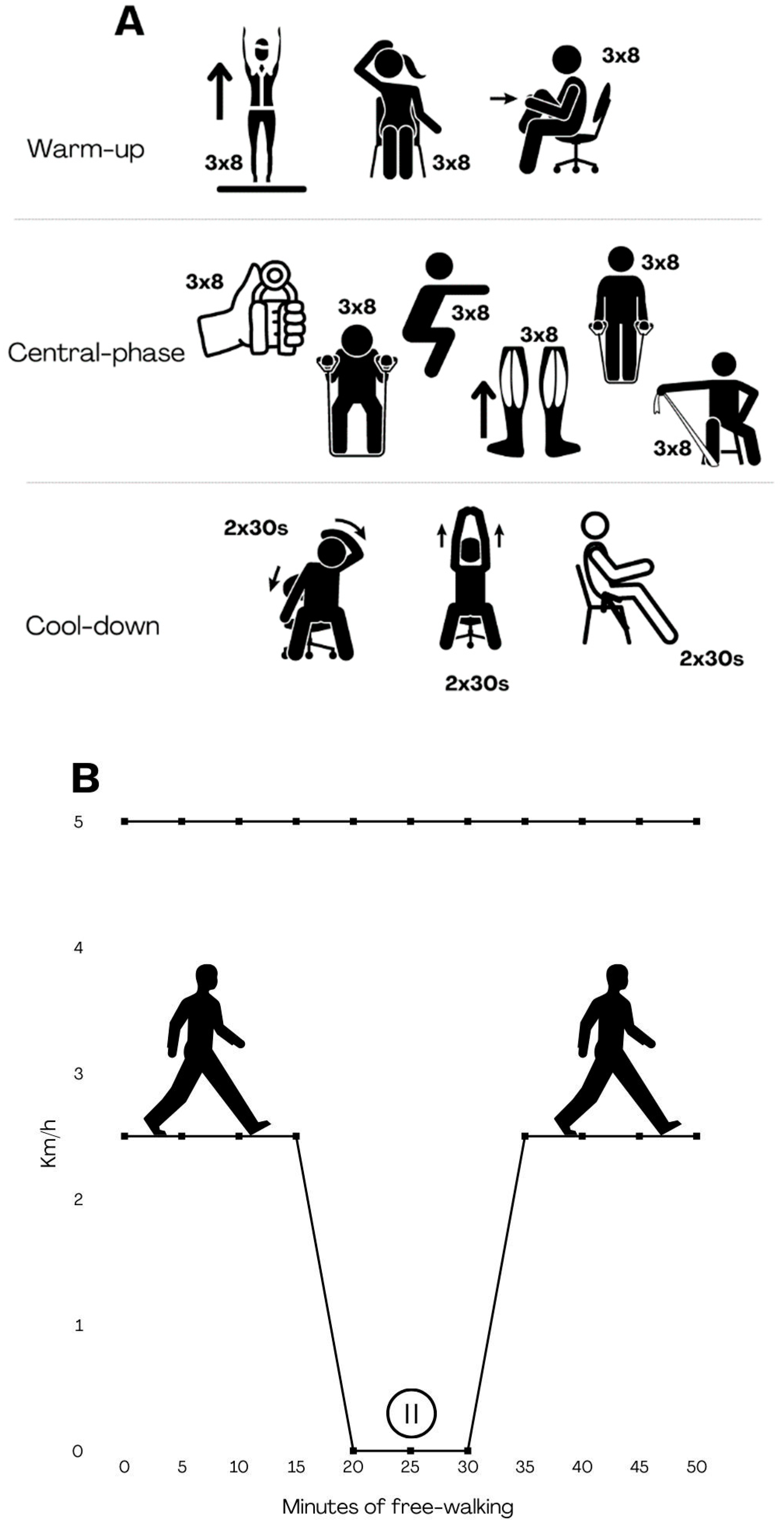
2.4. Training Program
- I.
- Supervised outdoor exercise
- II.
- Telecoaching
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Strengths and Limitations
4.2. Practical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations. World Population Ageing 2019 (ST/ESA/SER. A/444); United Nations, Department of Economic and Social Affairs, Population Division: New York, NY, USA, 2020. [Google Scholar]
- WHO. Ageing and Healt. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 1 October 2022).
- Peters, E.; Pritzkuleit, R.; Beske, F.; Katalinic, A. Demographic change and disease rates: A projection until 2050. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2010, 53, 417–426. [Google Scholar] [CrossRef]
- European-Commission. The 2018 Ageing Report: Economic and Budgetary Projections for the EU Member States (2016–2070); European-Commission: Geneva, Switzerland, 2018. [Google Scholar]
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef]
- Merchant, R.A.; Morley, J.E.; Izquierdo, M. Editorial: Exercise, Aging and Frailty: Guidelines for Increasing Function. J. Nutr. Health Aging 2021, 25, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Benavent-Caballer, V.; Rosado-Calatayud, P.; Segura-Ortí, E.; Amer-Cuenca, J.J.; Lisón, J.F. Effects of three different low-intensity exercise interventions on physical performance, muscle CSA and activities of daily living: A randomized controlled trial. Exp. Gerontol. 2014, 58, 159–165. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Daley, M.J.; Spinks, W.L. Exercise, mobility and aging. Sports Med. 2000, 29, 1–12. [Google Scholar] [CrossRef]
- de Oliveira, L.; Souza, E.C.; Rodrigues, R.A.S.; Fett, C.A.; Piva, A.B. The effects of physical activity on anxiety, depression, and quality of life in elderly people living in the community. Trends Psychiatry Psychother. 2019, 41, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Andreescu, C.; Lee, S. Anxiety Disorders in the Elderly. Adv. Exp. Med. Biol. 2020, 1191, 561–576. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Assessing Physical Performance in Independent Older Adults: Issues and Guidelines. J. Aging Phys. Act. 1997, 5, 244–261. [Google Scholar] [CrossRef]
- Seah, B.; Kowitlawakul, Y.; Jiang, Y.; Ang, E.; Chokkanathan, S.; Wang, W. A review on healthy ageing interventions addressing physical, mental and social health of independent community-dwelling older adults. Geriatr. Nurs. 2019, 40, 37–50. [Google Scholar] [CrossRef]
- Furtado, G.E.; Letieri, R.V.; Carballeira, E. Exercise Evaluation and Prescription in Older Adults. Healthcare 2022, 11, 42. [Google Scholar] [CrossRef]
- Patti, A.; Bianco, A.; Karsten, B.; Montalto, M.A.; Battaglia, G.; Bellafiore, M.; Cassata, D.; Scoppa, F.; Paoli, A.; Iovane, A.; et al. The effects of physical training without equipment on pain perception and balance in the elderly: A randomized controlled trial. Work 2017, 57, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, C.; O’ Sullivan, R.; Caserotti, P.; Tully, M.A. Consequences of physical inactivity in older adults: A systematic review of reviews and meta-analyses. Scand. J. Med. Sci. Sports 2020, 30, 816–827. [Google Scholar] [CrossRef] [PubMed]
- Guirguis-Blake, J.M.; Michael, Y.L.; Perdue, L.A.; Coppola, E.L.; Beil, T.L.; Thompson, J.H. U.S. Preventive Services Task Force Evidence Syntheses, formerly Systematic Evidence Reviews. In Interventions to Prevent Falls in Community-Dwelling Older Adults: A Systematic Review for the U.S. Preventive Services Task Force; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2018. [Google Scholar]
- Battaglia, G.; Giustino, V.; Messina, G.; Faraone, M.; Brusa, J.; Bordonali, A.; Barbagallo, M.; Palma, A.; Dominguez, L.-J. Walking in Natural Environments as Geriatrician’s Recommendation for Fall Prevention: Preliminary Outcomes from the “Passiata Day” Model. Sustainability 2020, 12, 2684. [Google Scholar] [CrossRef]
- Battaglia, G.; Bellafiore, M.; Caramazza, G.; Paoli, A.; Bianco, A.; Palma, A. Changes in spinal range of motion after a flexibility training program in elderly women. Clin. Interv. Aging 2014, 9, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, K.; Sobol, N.A.; Frederiksen, K.S.; Beyer, N.; Vogel, A.; Vestergaard, K.; Braendgaard, H.; Gottrup, H.; Lolk, A.; Wermuth, L.; et al. Moderate-to-High Intensity Physical Exercise in Patients with Alzheimer’s Disease: A Randomized Controlled Trial. J. Alzheim. Dis. 2016, 50, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Koevoets, E.W.; Schagen, S.B.; de Ruiter, M.B.; Geerlings, M.I.; Witlox, L.; van der Wall, E.; Stuiver, M.M.; Sonke, G.S.; Velthuis, M.J.; Jobsen, J.J.; et al. Effect of physical exercise on cognitive function after chemotherapy in patients with breast cancer: A randomized controlled trial (PAM study). Breast Cancer Res. 2022, 24, 36. [Google Scholar] [CrossRef]
- Scaturro, D.; Rizzo, S.; Sanfilippo, V.; Giustino, V.; Messina, G.; Martines, F.; Falco, V.; Cuntrera, D.; Moretti, A.; Iolascon, G.; et al. Effectiveness of Rehabilitative Intervention on Pain, Postural Balance, and Quality of Life in Women with Multiple Vertebral Fragility Fractures: A Prospective Cohort Study. J. Funct. Morphol. Kinesiol. 2021, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Hennig, T.; Haehre, L.; Hornburg, V.T.; Mowinckel, P.; Norli, E.S.; Kjeken, I. Effect of home-based hand exercises in women with hand osteoarthritis: A randomised controlled trial. Ann. Rheum. Dis. 2015, 74, 1501–1508. [Google Scholar] [CrossRef]
- Martinez-Velilla, N.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Saez de Asteasu, M.L.; Lucia, A.; Galbete, A.; Garcia-Baztan, A.; Alonso-Renedo, J.; Gonzalez-Glaria, B.; Gonzalo-Lazaro, M.; et al. Effect of Exercise Intervention on Functional Decline in Very Elderly Patients During Acute Hospitalization: A Randomized Clinical Trial. JAMA Intern. Med. 2019, 179, 28–36. [Google Scholar] [CrossRef]
- Sahin, H.; Naz, I.; Karadeniz, G.; Sunecli, O.; Polat, G.; Ediboglu, O. Effects of a home-based pulmonary rehabilitation program with and without telecoaching on health-related outcomes in COVID-19 survivors: A randomized controlled clinical study. J. Bras. Pneumol. 2023, 49, e20220107. [Google Scholar] [CrossRef]
- Fraser, M.; Munoz, S.A.; MacRury, S. Does the Mode of Exercise Influence the Benefits Obtained by Green Exercise? Int. J. Environ. Res. Public Health 2019, 16, 3004. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Liu, H.; Yang, Z.; Bi, S.; Cao, Y.; Zhang, G. The Effects of Green and Urban Walking in Different Time Frames on Physio-Psychological Responses of Middle-Aged and Older People in Chengdu, China. Int. J. Environ. Res. Public Health 2020, 18, 90. [Google Scholar] [CrossRef] [PubMed]
- Greco, G.; Centrone, C.; Poli, L.; Silva, A.F.; Russo, L.; Cataldi, S.; Giustino, V.; Fischetti, F. Impact of Coastal Walking Outdoors and Virtual Reality Indoor Walking on Heart Rate, Enjoyment Levels and Mindfulness Experiences in Healthy Adults. J. Funct. Morphol. Kinesiol. 2023, 9, 11. [Google Scholar] [CrossRef] [PubMed]
- Bullo, V.; Gobbo, S.; Vendramin, B.; Duregon, F.; Cugusi, L.; Di Blasio, A.; Bocalini, D.S.; Zaccaria, M.; Bergamin, M.; Ermolao, A. Nordic Walking Can Be Incorporated in the Exercise Prescription to Increase Aerobic Capacity, Strength, and Quality of Life for Elderly: A Systematic Review and Meta-Analysis. Rejuvenation Res. 2018, 21, 141–161. [Google Scholar] [CrossRef] [PubMed]
- Demeyer, H.; Louvaris, Z.; Frei, A.; Rabinovich, R.A.; de Jong, C.; Gimeno-Santos, E.; Loeckx, M.; Buttery, S.C.; Rubio, N.; Van der Molen, T.; et al. Physical activity is increased by a 12-week semiautomated telecoaching programme in patients with COPD: A multicentre randomised controlled trial. Thorax 2017, 72, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Colorado-State-University. Telecoaching Emerges as Tool in Nutrition and Medicine; Colorado-State-University: Fort Collins, CO, USA, 2016. [Google Scholar]
- Leale, I.; Figlioli, F.; Giustino, V.; Brusa, J.; Barcellona, M.; Nocera, V.; Canzone, A.; Patti, A.; Messina, G.; Barbagallo, M.; et al. Telecoaching as a new training method for elderly people: A systematic review. Aging Clin. Exp. Res. 2024, 36, 18. [Google Scholar] [CrossRef]
- Hume, E.; Muse, H.; Wallace, K.; Wilkinson, M.; Heslop Marshall, K.; Nair, A.; Clark, S.; Vogiatzis, I. Feasibility and acceptability of a physical activity behavioural modification tele-coaching intervention in lung transplant recipients. Chronic Respir. Dis. 2022, 19, 14799731221116588. [Google Scholar] [CrossRef] [PubMed]
- von Storch, K.; Graaf, E.; Wunderlich, M.; Rietz, C.; Polidori, M.C.; Woopen, C. Telemedicine-Assisted Self-Management Program for Type 2 Diabetes Patients. Diabetes Technol. Ther. 2019, 21, 514–521. [Google Scholar] [CrossRef]
- Scura, D.; Munakomi, S. Tinetti Gait and Balance Test. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Spijkerman, D.C.; Snijders, C.J.; Stijnen, T.; Lankhorst, G.J. Standardization of grip strength measurements. Effects on repeatability and peak force. Scand. J. Rehabil. Med. 1991, 23, 203–206. [Google Scholar] [CrossRef]
- Bohannon, R.W. Reference values for the timed up and go test: A descriptive meta-analysis. J. Geriatr. Phys. Ther. 2006, 29, 64–68. [Google Scholar] [CrossRef]
- Welch, S.A.; Ward, R.E.; Beauchamp, M.K.; Leveille, S.G.; Travison, T.; Bean, J.F. The Short Physical Performance Battery (SPPB): A Quick and Useful Tool for Fall Risk Stratification Among Older Primary Care Patients. J. Am. Med. Dir. Assoc. 2021, 22, 1646–1651. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Bolzetta, F.; Toffanello, E.D.; Zambon, S.; De Rui, M.; Perissinotto, E.; Coin, A.; Corti, M.-C.; Baggio, G.; Crepaldi, G.; et al. Association Between Short Physical Performance Battery and Falls in Older People: The Progetto Veneto Anziani Study. Rejuvenation Res. 2014, 17, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Volpato, S.; Cavalieri, M.; Sioulis, F.; Guerra, G.; Maraldi, C.; Zuliani, G.; Fellin, R.; Guralnik, J.M. Predictive Value of the Short Physical Performance Battery Following Hospitalization in Older Patients. J. Gerontol. Ser. A 2011, 66A, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Vasunilashorn, S.; Coppin, A.K.; Patel, K.V.; Lauretani, F.; Ferrucci, L.; Bandinelli, S.; Guralnik, J.M. Use of the Short Physical Performance Battery Score to Predict Loss of Ability to Walk 400 Meters: Analysis from the InCHIANTI Study. J. Gerontol. Ser. A 2009, 64A, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Studenski, S.; Perera, S.; Wallace, D.; Chandler, J.M.; Duncan, P.W.; Rooney, E.; Fox, M.; Guralnik, J.M. Physical Performance Measures in the Clinical Setting. J. Am. Geriatr. Soc. 2003, 51, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E. Performance-oriented assessment of mobility problems in elderly patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Rivolta, M.W.; Aktaruzzaman, M.; Rizzo, G.; Lafortuna, C.L.; Ferrarin, M.; Bovi, G.; Bonardi, D.R.; Caspani, A.; Sassi, R. Evaluation of the Tinetti score and fall risk assessment via accelerometry-based movement analysis. Artif. Intell. Med. 2019, 95, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, G.; Bellafiore, M.; Bianco, A.; Paoli, A.; Palma, A. Effects of a dynamic balance training protocol on podalic support in older women. Pilot Study. Aging Clin. Exp. Res. 2010, 22, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Bellafiore, M.; Battaglia, G.; Bianco, A.; Paoli, A.; Farina, F.; Palma, A. Improved postural control after dynamic balance training in older overweight women. Aging Clin. Exp. Res. 2011, 23, 378–385. [Google Scholar] [CrossRef]
- World-Health-Organization. Physical Activity. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 5 October 2022).
- An, H.Y.; Chen, W.; Wang, C.W.; Yang, H.F.; Huang, W.T.; Fan, S.Y. The Relationships between Physical Activity and Life Satisfaction and Happiness among Young, Middle-Aged, and Older Adults. Int. J. Environ. Res. Public Health 2020, 17, 4817. [Google Scholar] [CrossRef]
- Silva, F.M.; Petrica, J.; Serrano, J.; Paulo, R.; Ramalho, A.; Lucas, D.; Ferreira, J.P.; Duarte-Mendes, P. The Sedentary Time and Physical Activity Levels on Physical Fitness in the Elderly: A Comparative Cross Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 3697. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, P.L.; Castillo-García, A.; Morales, J.S.; Izquierdo, M.; Serra-Rexach, J.A.; Santos-Lozano, A.; Lucia, A. Physical Exercise in the Oldest Old. Compr. Physiol. 2019, 9, 1281–1304. [Google Scholar] [CrossRef] [PubMed]
- Low, D.C.; Walsh, G.S.; Arkesteijn, M. Effectiveness of Exercise Interventions to Improve Postural Control in Older Adults: A Systematic Review and Meta-Analyses of Centre of Pressure Measurements. Sports Med. 2017, 47, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Eckardt, N. Lower-extremity resistance training on unstable surfaces improves proxies of muscle strength, power and balance in healthy older adults: A randomised control trial. BMC Geriatr. 2016, 16, 191. [Google Scholar] [CrossRef] [PubMed]
- Watson, S.L.; Weeks, B.K.; Weis, L.J.; Harding, A.T.; Horan, S.A.; Beck, B.R. High-Intensity Resistance and Impact Training Improves Bone Mineral Density and Physical Function in Postmenopausal Women with Osteopenia and Osteoporosis: The LIFTMOR Randomized Controlled Trial. J. Bone Miner. Res. 2018, 33, 211–220. [Google Scholar] [CrossRef]
- Pinheiro, M.B.; Oliveira, J.; Bauman, A.; Fairhall, N.; Kwok, W.; Sherrington, C. Evidence on physical activity and osteoporosis prevention for people aged 65+ years: A systematic review to inform the WHO guidelines on physical activity and sedentary behaviour. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 150. [Google Scholar] [CrossRef] [PubMed]
- Vikberg, S.; Sörlén, N.; Brandén, L.; Johansson, J.; Nordström, A.; Hult, A.; Nordström, P. Effects of Resistance Training on Functional Strength and Muscle Mass in 70-Year-Old Individuals with Pre-sarcopenia: A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2019, 20, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Osuka, Y.; Fujita, S.; Kitano, N.; Kosaki, K.; Seol, J.; Sawano, Y.; Shi, H.; Fujii, Y.; Maeda, S.; Okura, T.; et al. Effects of Aerobic and Resistance Training Combined with Fortified Milk on Muscle Mass, Muscle Strength, and Physical Performance in Older Adults: A Randomized Controlled Trial. J. Nutr. Health Aging 2017, 21, 1349–1357. [Google Scholar] [CrossRef] [PubMed]
- Harwood, R.H.; Conroy, S.P. Slow walking speed in elderly people. BMJ 2009, 339, b4236. [Google Scholar] [CrossRef]
- Bai, X.; Soh, K.G.; Omar Dev, R.D.; Talib, O.; Xiao, W.; Cai, H. Effect of Brisk Walking on Health-Related Physical Fitness Balance and Life Satisfaction Among the Elderly: A Systematic Review. Front. Public Health 2021, 9, 829367. [Google Scholar] [CrossRef]
- Fan, Y.; Li, Z.; Han, S.; Lv, C.; Zhang, B. The influence of gait speed on the stability of walking among the elderly. Gait Posture 2016, 47, 31–36. [Google Scholar] [CrossRef]
- Chatutain, A.; Pattana, J.; Parinsarum, T.; Lapanantasin, S. Walking meditation promotes ankle proprioception and balance performance among elderly women. J. Bodyw. Mov. Ther. 2019, 23, 652–657. [Google Scholar] [CrossRef]
- Little, C.; Moore, C.; Bean, E.; Peters, D.M.; McGinnis, R.S.; Kasser, S.L. Acute effects of axial loading on postural control during walking and turning in people with multiple sclerosis: A pilot study. Gait Posture 2022, 94, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Madureira, M.M.; Takayama, L.; Gallinaro, A.L.; Caparbo, V.F.; Costa, R.A.; Pereira, R.M.R. Balance training program is highly effective in improving functional status and reducing the risk of falls in elderly women with osteoporosis: A randomized controlled trial. Osteoporos. Int. 2007, 18, 419–425. [Google Scholar] [CrossRef]
- Okubo, Y.; Osuka, Y.; Jung, S.; Figueroa, R.; Tsujimoto, T.; Aiba, T.; Kim, T.; Tanaka, K. Effects of walking on physical and psychological fall-related factors in community-dwelling older adults: Walking versus balance program. J. Phys. Fit. Sports Med. 2014, 3, 515–524. [Google Scholar] [CrossRef]
- Okubo, Y.; Osuka, Y.; Jung, S.; Rafael, F.; Tsujimoto, T.; Aiba, T.; Kim, T.; Tanaka, K. Walking can be more effective than balance training in fall prevention among community-dwelling older adults. Geriatr. Gerontol. Int. 2016, 16, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, L.D.; Gillespie, W.J.; Robertson, M.C.; Lamb, S.E.; Cumming, R.G.; Rowe, B.H. Interventions for preventing falls in elderly people. Cochrane Database Syst. Rev. 2003, 4, Cd000340. [Google Scholar] [CrossRef]
- Lopez, P.; Pinto, R.S.; Radaelli, R.; Rech, A.; Grazioli, R.; Izquierdo, M.; Cadore, E.L. Benefits of resistance training in physically frail elderly: A systematic review. Aging Clin. Exp. Res. 2018, 30, 889–899. [Google Scholar] [CrossRef]
- Borde, R.; Hortobágyi, T.; Granacher, U. Dose-Response Relationships of Resistance Training in Healthy Old Adults: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 1693–1720. [Google Scholar] [CrossRef]
- Otsuka, Y.; Yamada, Y.; Maeda, A.; Izumo, T.; Rogi, T.; Shibata, H.; Fukuda, M.; Arimitsu, T.; Miyamoto, N.; Hashimoto, T. Effects of resistance training intensity on muscle quantity/quality in middle-aged and older people: A randomized controlled trial. J. Cachexia Sarcopenia Muscle 2022, 13, 894–908. [Google Scholar] [CrossRef]
- Seo, M.W.; Jung, S.W.; Kim, S.W.; Lee, J.M.; Jung, H.C.; Song, J.K. Effects of 16 Weeks of Resistance Training on Muscle Quality and Muscle Growth Factors in Older Adult Women with Sarcopenia: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 6762. [Google Scholar] [CrossRef] [PubMed]
- Wagner, L.I.; Tooze, J.A.; Hall, D.L.; Levine, B.J.; Beaumont, J.; Duffecy, J.; Victorson, D.; Gradishar, W.; Leach, J.; Saphner, T.; et al. Targeted eHealth Intervention to Reduce Breast Cancer Survivors’ Fear of Recurrence: Results from the FoRtitude Randomized Trial. J. Natl. Cancer Inst. 2021, 113, 1495–1505. [Google Scholar] [CrossRef] [PubMed]
- Maggi, G.; Monti Bragadin, M.; Padua, L.; Fiorina, E.; Bellone, E.; Grandis, M.; Reni, L.; Bennicelli, A.; Grosso, M.; Saporiti, R.; et al. Outcome measures and rehabilitation treatment in patients affected by Charcot-Marie-Tooth neuropathy: A pilot study. Am. J. Phys. Med. Rehabil. 2011, 90, 628–637. [Google Scholar] [CrossRef] [PubMed]
- de Vasconcelos, H.C.A.; Lira Neto, J.C.G.; de Araújo, M.F.M.; Carvalho, G.C.N.; de Souza Teixeira, C.R.; de Freitas, R.W.J.F.; Damasceno, M.M.C. Telecoaching programme for type 2 diabetes control: A randomised clinical trial. Br. J. Nurs. 2018, 27, 1115–1120. [Google Scholar] [CrossRef]
- Chetlin, R.D.; Gutmann, L.; Tarnopolsky, M.; Ullrich, I.H.; Yeater, R.A. Resistance training effectiveness in patients with Charcot-Marie-Tooth disease: Recommendations for exercise prescription. Arch. Phys. Med. Rehabil. 2004, 85, 1217–1223. [Google Scholar] [CrossRef]
- Ramdharry, G.M.; Pollard, A.; Anderson, C.; Laura, M.; Murphy, S.M.; Dudziec, M.; Dewar, E.L.; Hutton, E.; Grant, R.; Reilly, M.M. A pilot study of proximal strength training in Charcot-Marie-Tooth disease. J. Peripher. Nerv. Syst. 2014, 19, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Furtado, G.E.; Reis, A.S.; Braga-Pereira, R.; Caldo-Silva, A.; Teques, P.; Sampaio, A.R.; Santos, C.A.; Bachi, A.L.; Campos, F.; Borges, G.F.; et al. Impact of Exercise Interventions on Sustained Brain Health Outcomes in Frail Older Individuals: A Comprehensive Review of Systematic Reviews. Healthcare 2023, 11, 3160. [Google Scholar] [CrossRef]
- Trott, M.; Smith, L. What are the associations between extroversion, enjoyment, and wellness in group vs non-group physical activity? A pilot study. Atena J. Sports Sci. 2019, 1, 3. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Sample (Mean ± SD) | TG (n = 49) (Mean ± SD) | UG (n = 11) (Mean ± SD) | |
|---|---|---|---|
| Male/Female | 28/32 | 23/26 | 5/6 |
| Age (years) | 71.20 ± 6.01 | 71.32 ± 5.98 | 70.64 ± 6.38 |
| BMI | 27.31 ± 5.48 | 27.22 ± 5.70 | 27.70 ± 4.61 |
| Weight (kg) | 70.24 ± 16.29 | 71.01 ± 14.41 | 72.38 ± 14.23 |
| Height (m) | 1.60 ± 0.09 | 1.60 ± 0.09 | 1.61 ± 0.08 |
| Shapiro–Wilk | T0 (Mean ± SD) | T1 (Mean ± SD) | p-Value | ||
|---|---|---|---|---|---|
| W | p-Value | ||||
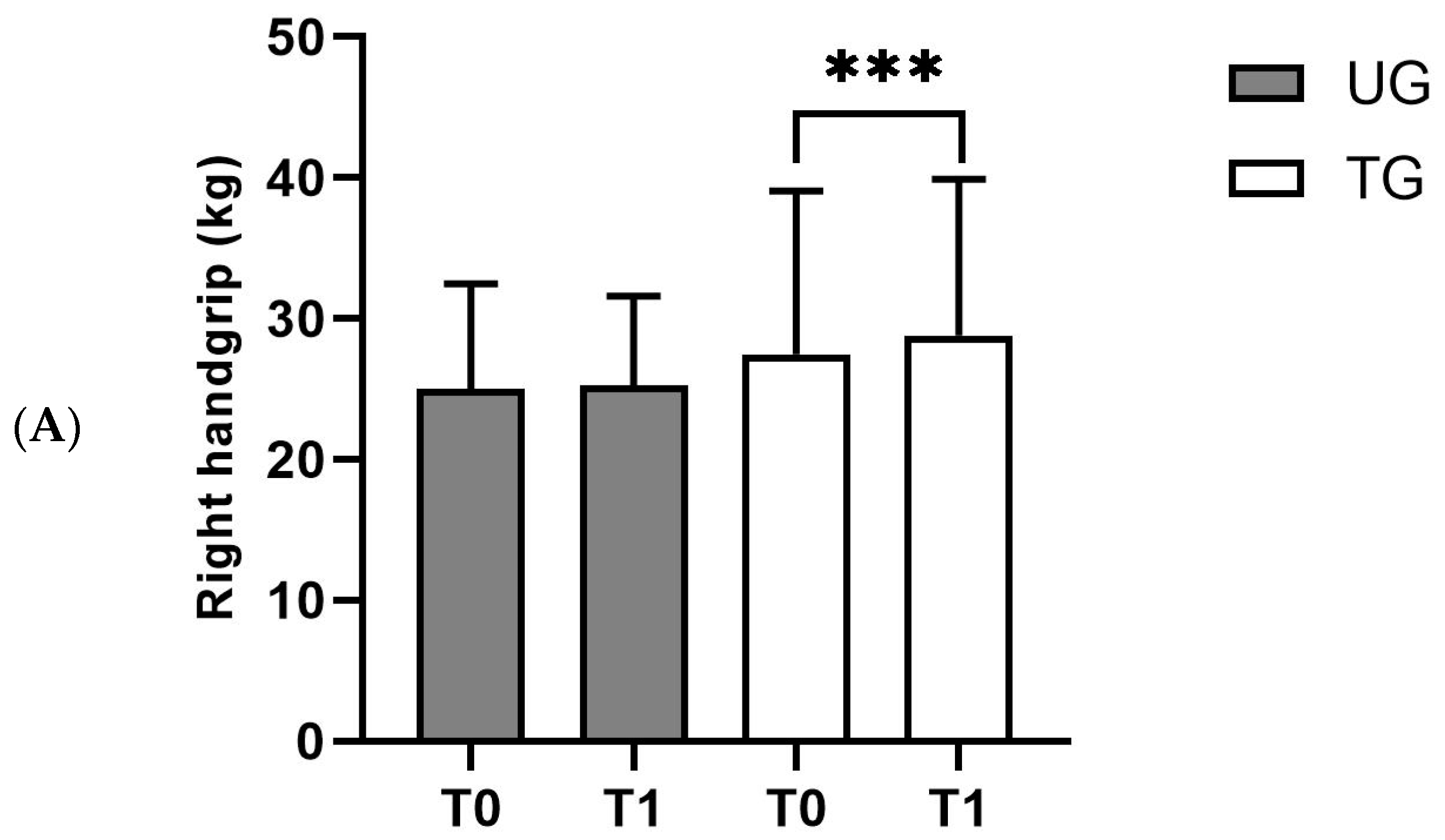
| Right handgrip ° | 0.94 | 0.015 | 27.47 ± 11.58 | 28.82 ± 11.06 | <0.001 *** |
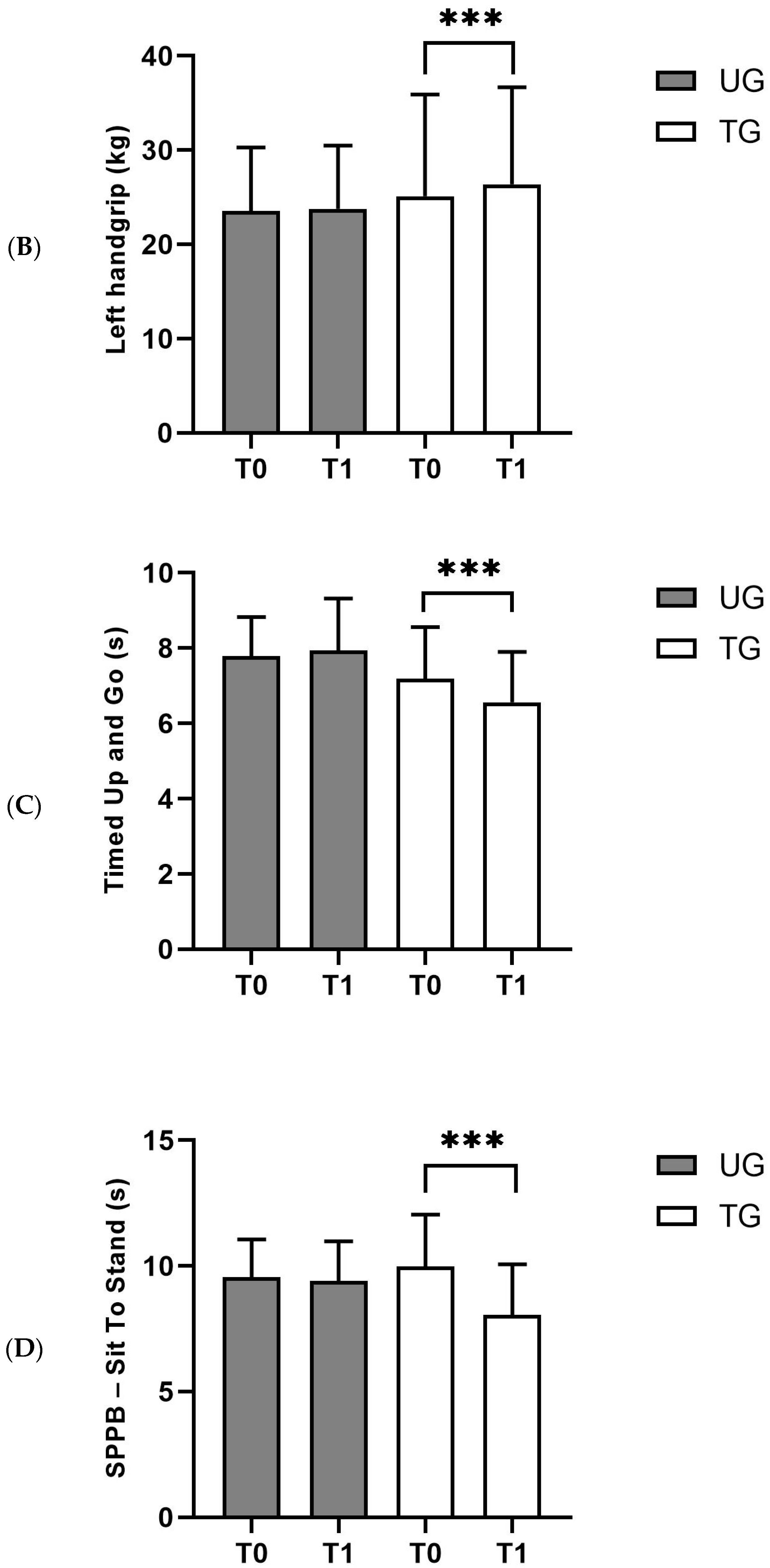
| Left handgrip × | 0.967 | 0.176 | 25.11 ± 10.80 | 26.39 ± 10.30 | <0.001 *** |
| TUG ° | 0.918 | 0.002 | 7.19 ± 1.37 | 6.56 ± 1.36 | <0.001 *** |
| SPPB ° | 0.759 | <0.001 | 11.22 ± 0.98 | 11.5 ± 0.82 | 0.012 * |
| Gait Speed ° | 0.838 | <0.001 | 4.90 ± 1.66 | 4.67 ± 1.43 | 0.194 |
| Sit To Stand ° | 0.946 | 0.025 | 9.98 ± 2.07 | 8.05 ± 2.02 | <0.001 *** |
| Tinetti Scale ° | 0.871 | <0.001 | 24.92 ± 2.74 | 26.20 ± 1.38 | 0.002 ** |
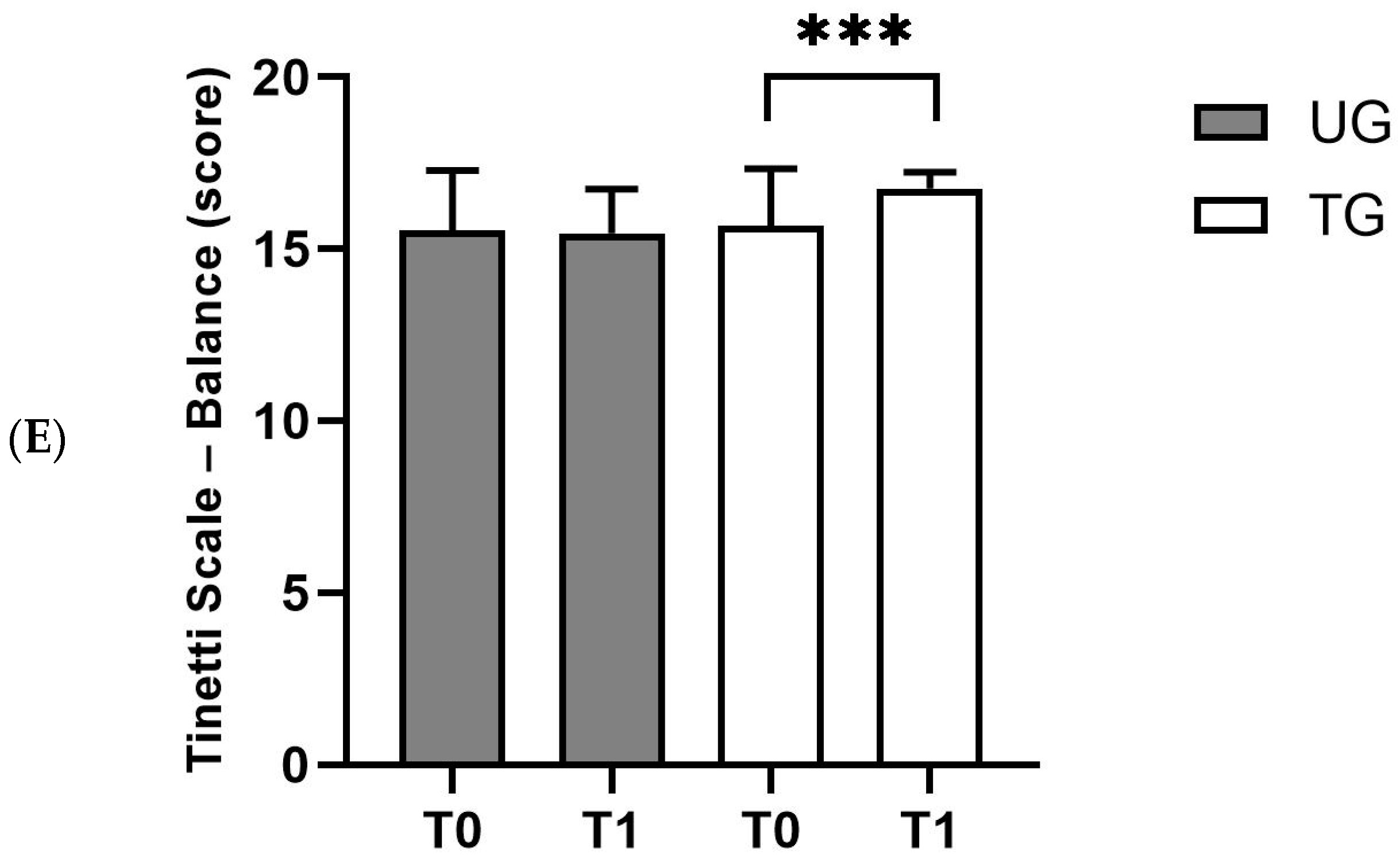
| Balance ° | 0.741 | <0.001 | 15.78 ± 1.53 | 16.76 ± 0.48 | <0.001 *** |
| Gait ° | 0.948 | 0.03 | 9.14 ± 1.63 | 9.45 ± 1.26 | 0.359 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leale, I.; Giustino, V.; Brusa, J.; Barcellona, M.; Barbagallo, M.; Palma, A.; Messina, G.; Dominguez, L.J.; Battaglia, G. Effectiveness of a Sustainable Training Program Combining Supervised Outdoor Exercise with Telecoaching on Physical Performance in Elderly People. Sustainability 2024, 16, 3254. https://doi.org/10.3390/su16083254
Leale I, Giustino V, Brusa J, Barcellona M, Barbagallo M, Palma A, Messina G, Dominguez LJ, Battaglia G. Effectiveness of a Sustainable Training Program Combining Supervised Outdoor Exercise with Telecoaching on Physical Performance in Elderly People. Sustainability. 2024; 16(8):3254. https://doi.org/10.3390/su16083254
Chicago/Turabian StyleLeale, Ignazio, Valerio Giustino, Jessica Brusa, Matteo Barcellona, Mario Barbagallo, Antonio Palma, Giuseppe Messina, Ligia J. Dominguez, and Giuseppe Battaglia. 2024. "Effectiveness of a Sustainable Training Program Combining Supervised Outdoor Exercise with Telecoaching on Physical Performance in Elderly People" Sustainability 16, no. 8: 3254. https://doi.org/10.3390/su16083254