Abstract
Purpose: Cycling is a popular activity for children aged 5–14 years and has a notable risk of head injuries. Extensive evidence shows that bicycle helmets can reduce the severity of head injuries and prevent fatalities. The current study examines the prevalence of bicycle helmet use among children (aged 5–17 years) in Saudi Arabia, parents’ attitudes and safety perceptions toward children’s bicycle helmets, and factors that influence parents’ decisions regarding their children’s bicycle helmets. Methods: This study used an analytical cross-sectional design via a validated questionnaire to examine parents’ attitudes toward helmet use for their children (aged 5–17 years) in Saudi Arabia. The study, which was carried out from September 2023 to September 2024, involved 492 participants (69.5% mothers and 30.5% fathers), and they were recruited from all regions of Saudi Arabia. A validated and translated questionnaire was used to assess helmet usage attitudes, considering demographic factors and potential confounders. Results: Approximately 60% of children wear helmets while cycling, despite a high mean attitude score of 5.49 (SD = 0.91), with 93.3% of respondents expressing strong support for mandatory helmet laws. While belief (mean (M) = 5.45) and knowledge (M = 4.63) scores were also high, they did not correlate with actual helmet use. Strong helmet regulations significantly increased usage rates (>80%). Helmet ownership and parental helmet-wearing habits were associated with higher usage among children, with mothers showing greater usage rates for younger children than fathers. Regression analyses indicated that parents who wore helmets as children were 5.85 times more likely to have their children wear helmets and parents who wore helmets themselves were 7.98 times more likely to ensure that their oldest child did so. Conclusions: While parents have positive attitudes toward helmet safety, actual helmet usage among children measures at approximately 60%. Sustainable helmet regulations and parental modeling, especially for parents who wear helmets, are crucial for improving safety.
1. Introduction
1.1. The Use of Helmets Worldwide
Cycling is a globally popular activity among 5-year-old to 14-year-old children. In the United States, up to 80% of children and teenagers ride bicycles without wearing helmets [1,2]. In Turkey, 4.4% of children cyclists (8–16 years) wear helmets [3]. A study in the United States revealed that the majority of middle-school students in certain states frequently cycled without helmets as they rarely or never wore helmets (68.6%) [4]. A study in 26 countries assessed helmet usage among school students aged 11–15 years and revealed significant variations in reported helmet use across the countries, from 39.2% to 1.9%. Scandinavian countries, Canada, and England reported the highest rates of helmet use (>25%), while the participating Eastern European countries, along with France, Belgium (Flemish), Portugal, and Greenland, reported rates of <10% [5]. Although there is no specific evidence about helmet use among child cyclists in Saudi Arabia, studies in other countries have highlighted inadequate helmet usage among children and teenagers. This data gap highlights the pressing need to investigate helmet use behaviors among children in Saudi Arabia, given that cycling-related injuries continue to pose a significant public health issue. Gaining insight into parental attitudes and behaviors is essential for creating targeted interventions that encourage helmet use and enhance child safety.
1.2. Importance of Helmet Use
Cycling poses a significant risk of injury, especially head injuries. Each year, approximately 26,000 children require emergency department visits due to cycling-related head injuries [6]. The findings of the study conducted by Gross et al. (2018) demonstrate that e-bike-related trauma may result in significant injuries, particularly among children, who exhibit increased vulnerability to head and facial injuries due to their proportionally larger head-to-body ratio. Additionally, the injury patterns associated with e-bike incidents closely resemble those observed in motorcycle-related injuries, indicating the necessity for the appropriate triage of such cases to medical facilities equipped with sufficient trauma care capabilities [7]. Extensive research has proven the effectiveness of bicycle helmets in reducing the severity of head injuries and saving lives [2]. A 2019 study analyzed 85,187 facial injuries in adults (18–65 years) and found that helmets reduced head fractures by 52% and head soft-tissue injuries by 30%. However, the effectiveness of helmets in preventing facial injuries varies depending on the area of the face [8]. A 2022 report from the American Academy of Pediatrics highlighted that wearing helmets substantially reduces the likelihood of both fatal and nonfatal head injuries in a range of recreational sports, such as cycling, and does not raise the risk of neck injuries [9]. Nearly 90% of children in Los Angeles aged <18 years and who received medical treatment for cycling-related injuries did not wear helmets [10]. Not wearing helmets was also associated with a higher incidence of brain injuries and the need for head X-rays or computed tomography scans [11].
1.3. Factors That Influence Helmet Use
Helmet use among children can be influenced by many factors, including parental attitudes and safety perception, which play a crucial role. Factors such as a child’s age, demographic areas, income, education, parental rules, role modeling, monitoring, peer pressure, helmet design, thoughts, beliefs, and habitual inclination toward safety practices can influence parents’ attitudes [10,11].
Parental consistency in enforcing helmet-wearing rules and positive reinforcement are crucial and effective strategies for encouraging children to wear helmets [12]. Children whose parents wear helmets themselves and have strict helmet rules are more likely to wear helmets more consistently than children whose parents set partial or no rules [13]. The same study shows that parents are aware of their influence on their children’s behavior and recognize the importance of their own actions and rules in promoting helmet use [13].
Other factors, such as the influence of parental role modeling [14], peer pressure, and helmet design [15], play a significant role in helmet use by children [13]. Parents identified the comfort, style, and design of helmets, as well as the fear of being teased, as barriers to helmet use [16]. Moreover, teenagers have indicated that laws requiring helmet use and measures such as parental enforcement can significantly boost helmet usage [17]. Parents may lack awareness regarding whether their cycling-proficient child needs a helmet and the types of helmets available for their children’s activities. For instance, parents suggested that for motorized vehicles, they have specialized helmets for their children, but for other activities, a bicycle helmet or multi-purpose helmet is sufficient. There was common disagreement about whether a child needs a particular helmet for certain non-motorized activities [18]. Parents’ perceptions of safety also influence helmet usage; some parents believe that their children do not always need to wear helmets in “safe” areas where they are supervised by responsible individuals [14].
Age is negatively associated with helmet use [5,12,19], with a noticeable drop in usage among teenagers aged 10–16 years [12]. As children grow older, they are less likely to wear helmets. A study revealed that 89.5% of children (3–6 years) wear helmets while cycling, whereas 11.0% of adolescents (14–17 years) do so. The youngest age group (3–6 years) accounted for 19% of bicycle-related head injuries caused by the absence of helmets, whereas the oldest age group (14–17 years) accounted for 67% of similar injuries [5,19].
Geographical and legislative factors affect helmet usage. Helmet use among child pillion riders is more prevalent in urban areas compared to rural areas [19]. Parents in rural areas have reported that their own rules significantly impact their children’s helmet use [18]. In Canada, parents have shown high support for bicycle helmet legislation [20]. Despite legislation and parents’ attitudes toward the dangers of not wearing helmets, there remain significant barriers to helmet use.
Income and education have a strong influence on helmet use. Lower income and education levels are associated with a higher occurrence of unhelmeted crashes [21]. Lower median incomes and education levels, limited resources, and ineffective outreach efforts aimed at injury prevention may contribute to a higher prevalence of riding without a helmet. The mortality rate of accidents has exhibited a decline (approximately 3.1%) for each unit increase in the percentage of the population with a college education [21].
Evidence highlights the critical role of road infrastructure in promoting economic growth, social development, and environmental sustainability while also addressing the significant risks that can lead to delays and budget overruns in large infrastructure projects. Through a comprehensive literature review and analysis of completed projects, the authors identify and quantify the key risks linked to an increased contract price (ICP) and extension of time (EoT) in future endeavors. They subsequently develop a model that categorizes these risks into clusters, prioritizing those that require immediate funding and proposing specific preventive measures tailored to address each identified risk. These preventive measures include implementing proactive risk management strategies, enhancing stakeholder communication, conducting thorough feasibility studies, and investing in training and resources for project teams. An example of such preventive measures in the context of road safety is the promotion of helmet use among children, which can reduce the risk of severe injuries related to cycling accidents [22]. Additionally, recent research emphasizes the importance of maintaining appropriate lateral distance parameters when vehicles overtake electric bicycles to enhance road safety, further supporting the need for comprehensive safety measures in infrastructure planning [23]. Overall, the aim of these interventions is to minimize the likelihood of risk occurrence and ensure that projects stay within their established timelines and budgets.
1.4. Aims and Objectives
Cycling presents a notable safety risk for children, yet readily accessible data on bicycle usage and injury rates in Saudi Arabia are currently lacking. Despite a thorough search of official sources, we were unable to locate comprehensive statistics on this topic. This study directly addresses this data gap by providing a comprehensive assessment of bicycle helmet use among children in Saudi Arabia and identifying factors influencing helmet usage decisions among parents. Thus, this study offers several important contributions. It presents the first thorough analysis of child helmet use prevalence and parental attitudes in Saudi Arabia. Furthermore, it highlights the influence of sociodemographic factors on helmet use behaviors, providing practical insights to inform policy and intervention strategies designed to enhance safety outcomes for child cyclists. This study’s first aim is to measure the prevalence of bicycle helmet use in Saudi Arabia among children aged 5–17 years. It is hypothesized that helmet usage is low, with around 90% not wearing helmets while cycling [24]. The study uses a validated questionnaire to assess parents’ attitudes toward helmet safety, expecting that up to 97% of parents believe that helmets prevent injuries [25]. Despite this belief, a gap is anticipated between belief and actual helmet usage, and this study aims to explore and understand the influencing factors.
Additionally, this study examines influencing factors such as parental sociodemographic characteristics, their own helmet use, and geographic differences in parental decisions about children’s helmet use. It is hypothesized that socioeconomic status affects attitudes, with a 9% decrease in helmet usage for every 10% income decrease [24,25]. Parents who use helmets might expect their children to follow suit [24,25]. The findings will inform policy development for promoting helmet use among children in Saudi Arabia, highlighting the need for sustainable nationwide preventive measures.
2. Material and Methods
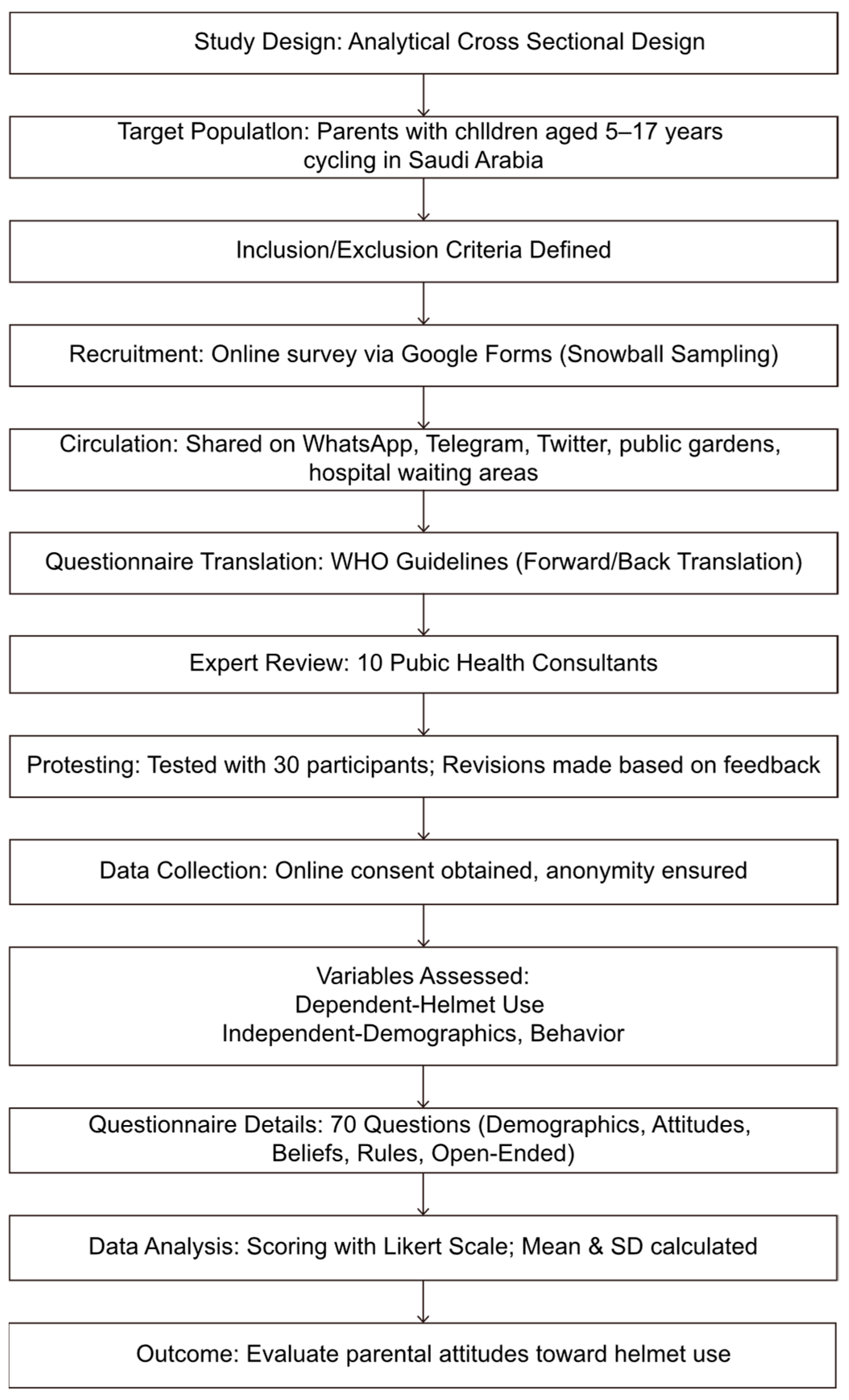
This study used an analytical cross-sectional design questionnaire to investigate the attitudes of parents toward helmet use for their children when cycling. The cross-sectional design provided a comprehensive overview of parental attitudes and behaviors throughout Saudi Arabia during a specific time period. This study was conducted in all 13 regions of Saudi Arabia from September 2023 to September 2024, including 3 months dedicated specifically to data collection (Figure 1).
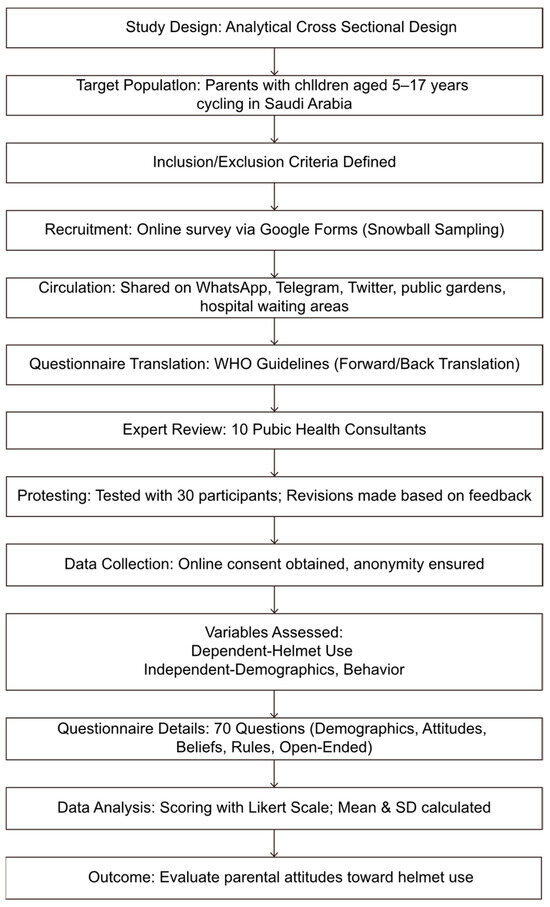
Figure 1.
Flowchart of the methodology of this study.
2.1. Participants
The inclusion criteria were parents with one or more children aged 5–17 years who used a bicycle (bicycle, tricycle, quadricycle, and scooter), lived in Saudi Arabia, and resided with the child in the same home. The exclusion criteria included parents with ≥1 child not in the 5–17-year age group, who did not cycle, and who lived outside Saudi Arabia.
Participant recruitment and selection were executed through the distribution of an online survey via a Google Form (132.0.6834.160) link. This link was strategically circulated using a snowball sampling technique across prominent social media platforms such as WhatsApp, Telegram (Version 11.7), and Twitter within Saudi Arabia over a three-month period, aiming to ensure extensive reach and diverse participant engagement. The survey utilized a pre-validated questionnaire [13], keeping the identities of the participants anonymous [13].
Given constraints—such as potential selection bias inherent in recruiting parents from toy stores and bicycle shops that sell helmets and bicycles, which may not adequately represent the broader population of parents—and the impracticality of accessing a comprehensive list of parents’ names and contact information, a non-probability convenience sampling method was deemed appropriate. This methodology facilitated the inclusion of parents from all 13 regions of Saudi Arabia. While the snowball sampling method facilitated effective recruitment across different regions, it may have resulted in selection bias, which could restrict the generalizability of the results.
Invitations to participate in the survey were extended to a convenience sample, including colleagues, family members, classmates, friends, and other individuals within the research team’s network. Employing a “snowball” recruitment strategy, participants were encouraged to disseminate the survey among their contacts. The online questionnaire was also distributed through a barcode in public gardens and hospital waiting areas where individuals typically have the time for engagements. This multifaceted approach enabled the efficient collection of responses from readily accessible and willing participants.
2.2. Materials
The questionnaire was professionally translated according to WHO guidelines and adapted to align with the research objectives. The translation process included forward translation, an expert panel review (10 consultants from public health, epidemiology, and preventive medicine), back translation, pretesting, and cognitive interviewing, resulting in the final version (Supplementary Materials). A bilingual health professional fluent in Arabic and English conducted the forward translation, focusing on conveying concepts rather than literal translation. An expert panel reviewed the translation and performed a back translation to ensure accuracy. The translated questionnaire was tested with 30 participants through pretesting and cognitive interviewing to assess comprehension and effectiveness. Based on the feedback, there were further revisions to produce the final questionnaire, and these responses were not included in the final analysis. We consulted with local experts and stakeholders to incorporate cultural differences that may impact the understanding and interpretation of the survey items. Their insights were invaluable in refining the questionnaire to reflect the unique perspectives and experiences of families in Saudi Arabia.
To ensure confidentiality and ethical considerations, access to the collected data was limited to the research supervisor and co-authors and data were used solely for research purposes. The Google Form survey for participants included an informed consent form at the beginning. No incentives were provided for participation in the survey. Participants were informed about their right to withdraw from the survey at any time and their anonymity was protected via the use of participant codes. The results, identified using codes, were entered into a collective database and stored anonymously in accordance with the appropriate guidelines.
The main outcome of the study was to assess parents’ attitudes toward the importance of helmet use for their children’s safety. This was assessed through dependent variables such as children’s helmet use, and independent variables included participants’ demographic information (age, parents’ educational level, gender, income, and geographic area).
Various confounders that could affect the study’s outcome were considered, including existing laws regarding helmet use, history of previous injury due to cycling, socioeconomic status, educational level, cultural beliefs and thoughts, parents’ cycling behavior, access to helmets in terms of availability and accessibility, and media exposure.
2.3. Data Collection
Participant consent and data collection were conducted through an online validated questionnaire. A validated questionnaire and scoring system developed by another researcher were utilized with permission [13]. The questionnaire had 70 questions, including six sections: demographics (number and ages of children), parents’ cycling behavior and attitudes (whether parents used helmets), providing insights into their children’s cycling habits, beliefs and experiences, rules and opinions, a comparison between the oldest and youngest child, and open-ended questions. The scoring system for the questionnaire was based on a Likert scale and it was employed to assess helmet usage. Participants were asked for the frequency they required their child to wear a helmet (1 (never) to 6 (always)). The mean and standard deviation (SD) of the responses to the six questions related to parents’ helmet requirements were calculated. This score provided a quantitative measure of the influences of parental decision-making.
Participants were asked 24 questions about helmet use, behavior, and beliefs. The questions were grouped into subscales: helmet rules, helmet concerns, peer pressure, belief (think), attitude (preference), and knowledge behavior (parents’ actions).
2.3.1. Helmet Rules
This subscale included two questions: “I require my child who is a beginner cyclist to wear a helmet” and “I require my child who is an experienced cyclist to wear a helmet”. Responses ranged from 1 (never or almost never) to 6 (always or almost always).
2.3.2. Peer Pressure
This subscale included six questions: “My child’s friends do not wear helmets”, “Most of the other parents I know do not wear helmets”, “I think other parents might consider me to be too afraid for my children if I forced them to wear a helmet”, “I fear that my child will be upset by other children who do not wear a helmet”, ”People think I would be more stylish if I didn’t wear a helmet”, and “Most of my friends don’t ask their kids to wear a helmet”.
2.3.3. Belief (Think)
This subscale included three questions: “I believe that mandatory helmet laws for bicyclists would significantly reduce the number of cycle-related head injuries and fatalities”, “I believe that a helmet can prevent head injury in a bicycle accident”, and “I think I would be more likely to insist that my child/ren wear a helmet if one of my close friends or family members was killed in a bicycle accident”.
2.3.4. Attitude (Prefer)
This subscale included two questions: “I feel that children are safer when wearing a helmet” and “I will support the idea of issuing a mandatory helmet law for all persons under the age of 16”.
2.3.5. Behavior (What People Really Do)
This subscale included four questions: “I know how to adjust the helmet to fit my child”, “I do not always ask my child to wear a bicycle helmet, especially because of the child’s complaint and insistence on not wearing it” (reverse-coded), “I think I could enforce the helmet rule on my kids if I wanted to”, and “When purchasing a helmet, I look for a certificate of approval for the helmet from an approved body for helmet safety”.
2.3.6. Knowledge
This subscale included four questions: “I remember seeing/hearing information about an adult/child who was seriously injured/killed in a cycle-related accident”, “If my child suffers a serious injury to the head area, this will have a devastating impact on his normal development (socially, intellectually, and physically)”, “Over the past year, I have received advice from a friend or family member that I should wear a helmet”, and “People who wear a cycle helmet when they ride are a good role model”.
Answers to the open-ended questions were grouped into main themes: “My greatest fear regarding my child/ren’s safety are” and “The number one reason I do not require my child to wear a helmet”.
2.4. Data Analysis
The data were analyzed with SPSS software (version 27; IBM Corp; Chicago, IL, USA). Descriptive statistics, including frequencies, percentages, means, and SDs, were employed to summarize the categorical and quantitative variables.
The relationships between parents’ attitudes toward helmet use and demographic and socioeconomic factors, including age, sex, nationality, marital status, and education level, were assessed using bivariate analysis. The Student’s t-test was used for independent samples or a one-way analysis of variance followed by post hoc analysis to test for quantitative outcome variables in order to compare the mean values in relation to the categorical study variables, which have 2 and >2 options, respectively. Pearson’s Chi-square test and odds ratios were used to test and measure the association between the categorical study and outcome variables. If the Chi-square test (for a 2 × 2 table) was not applicable, Fisher’s exact test was used. p < 0.05 and 95% confidence intervals were used to report the statistical significance and precision of the results. Common confounders, such as sociodemographic factors, were adjusted in the regression model.
3. Results
The questionnaires were distributed for three months and were answered by 492 parents; the data were available and collected for analysis. Not all questions on the survey were answered by all participants. The reported percentages are based on the number of participants who responded to each question; 20 (4.1%) respondents were eliminated from the study because they and their children did not live in the same house (Table 1).

Table 1.
Sociodemographic characteristics of parents and children, n = * 492.
Of the 492 participants, 342 (69.5%) were mothers and 150 (30.5%) were fathers. The parents’ ages ranged from 30 to 54 years (average 42.45 years). Most participants (95.3%) were Saudi nationals and 59.3% had at least a bachelor’s degree. Most children (95.9%) lived at home with their parents. The number of children per family varied considerably, from 29 (6.0%) single-child families to 16 (3.3%) families with 8–10 children. Most families had 3–4 children (Table 1). The prevalence of cycle helmet use among children in Saudi Arabia was only around 60% when cycling (Table 2).
Table 2.
Bicycle helmet use.
Out of the 492 respondents, 161 (32.7%) owned a bicycle, and Table 3a shows the cycling behavior of these parents. On average, the parents cycled 1.86 times/week (median 1 time/week). Parents cycled without children a few times per year (40.4%) or a few times per month (21.7%). Most parents did not cycle with their children (37.3%), except for a few times per year (21.7%). Parks or playgrounds were the most common sites where parents cycled with or without children (47.2% and 26.1%, respectively).
Table 3.
(a) Parents’ bicycle riding behavior, n = 161. (b) Helmet use behavior.
Table 3b shows that 81 (50.3%) parents with bicycles owned helmets, although only 59 (36.6%) wore helmets when riding a bicycle. Out of 81 (50.3%) parents who owned helmets, more than half of them usually wore helmets or always wore them when cycling without children (19.8% and 37.0%, respectively) and a higher proportion of parents wore them usually or always wore them when cycling with children (21.0% and 45.7%, respectively). Parents injured during cycling (37.3%) had minor scrapes and bruises (65%). The most common cause of injury was a fall from the bicycle (90%).
Table 4 summarizes various scores expressed on a 1–6 scale. Higher mean values indicate greater levels of the constructs measured. The proportion of responses with scores of ≥4 indicates the percentages of participants with a “high” level of agreement with the statements. There were very high scores for the belief and attitude subscales (mean (M) = 5.45 and M = 5.49, respectively), with over 90% of respondents in the “high” category. The helmet concern subscale had the lowest score (M = 2.84), suggesting that <20% of respondents had high concerns about helmets.
Table 4.
Subscale scores, n = 492.
Table 5 shows the descriptive statistics for bicycle riding and helmet use among children. Only 45.1% of the youngest children and 48.2% of the oldest children owned a bicycle. The majority of those who owned a bicycle never rode without their parent’s supervision or rode without supervision only 10–20% of the time. In these two categories, the youngest children were 27.1% and 27.1%, respectively, and the oldest children accounted for 20.7% and 31.0%, respectively.
Table 5.
Bicycle riding and helmet use by children.
The majority of parents required their child to wear a helmet (59.8% for the oldest children and 62.4% for the youngest children) and 60–70% of parents required their children to wear helmets for other activities such as rollerblading, skateboarding, cycling, and riding scooters.
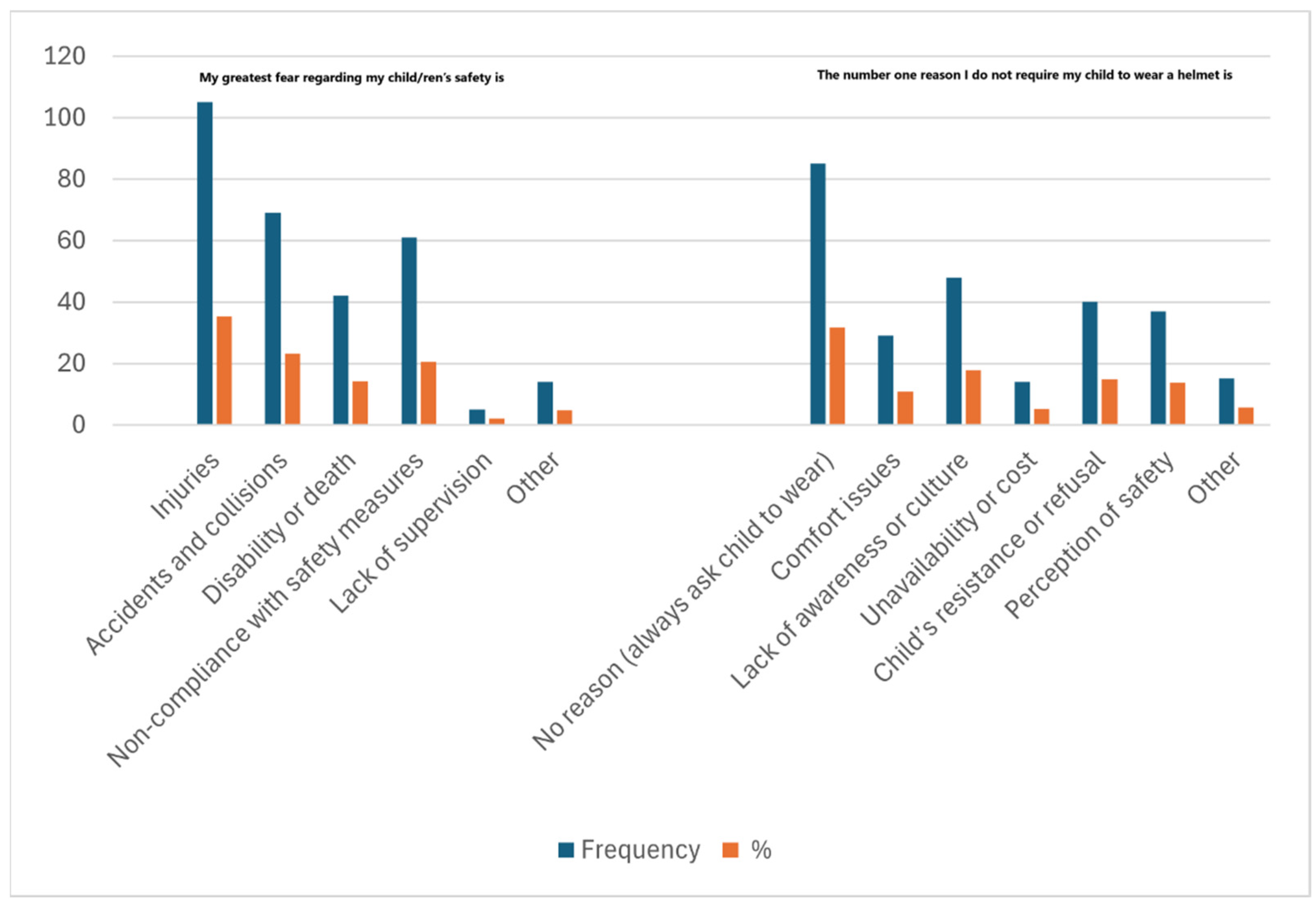
The main themes for responses to the open-ended question “My greatest fear regarding my child/ren’s safety” were as follows (Figure 2):
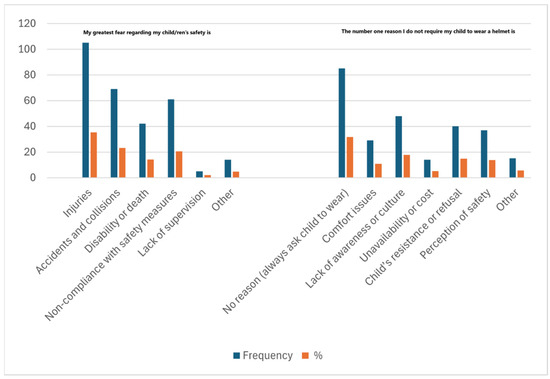
Figure 2.
Parental insight about child safety and helmet usage.
- Injuries: A prevalent concern among parents was their children experiencing a head injury or other injuries, especially from falls without helmets.
- Accidents and collisions: Many parents expressed fears of accidents, particularly involving cars or other vehicles, and collisions while riding a bicycle.
- Disability or death: There was significant anxiety about severe injuries leading to permanent disability or death.
- Non-compliance with safety measures: Parents worried about their children not following safety rules, such as not wearing helmets or cycling at high speeds.
- Lack of supervision: Parents often mentioned their inability to always supervise their children, fearing that this leads to accidents and injuries.
The main themes for responses to the open-ended question, “The number one reason I do not require my child to wear a helmet” were as follows (Figure 2):
- Comfort issues: Many responses mentioned that helmets are uncomfortable, too tight, or cause discomfort such as sweating, choking, or dispensing weight.
- Lack of awareness or culture: A recurring theme was the lack of awareness about the importance of wearing helmets or a cultural lack of emphasis on helmet use. Several responses mentioned that helmet wearing was not common practice and there was no strong helmet-wearing culture.
- Unavailability or cost: Some respondents stated that helmets were either not available or too expensive; therefore, the children did not wear them.
- Child’s resistance or refusal: Children’s refusal or stubbornness was frequently mentioned as a reason. They either outright rejected wearing helmets or found them annoying.
Perception of safety: Many parents said they did not enforce helmet use because their child was playing in safe places, such as at home or in the backyard, and they did not see helmets as necessary in these situations.
Belief and attitude had no significant association with actual helmet usage. Helmet rules, behavior, and knowledge were associated with a statistically significant increase in helmet usage among children. Strong helmet rules by parents were associated with the highest rate of helmet use among children (>80%) (Table 6).
Table 6.
Association between belief and helmet usage.
Parents who owned and wore helmets (p ≤ 0.001 for the youngest and oldest child); those who wore helmets (p ≤ 0.003 for the youngest child, and p ≤ 0.001 for the oldest child); and gender (p = 0.049 for the youngest child) were associated with a statistically significant increase in helmet usage among children. Owning a helmet and parents who wore helmets themselves were associated with the highest rate of helmet use among children (over 80%). Mothers had higher helmet use rates for their younger children than fathers (Table 7). Mothers had a more significant impact on their children’s helmet use than fathers. They were more inclined to establish rules about wearing helmets, irrespective of the child’s wishes, and engaged in stricter monitoring behaviors, such as promoting seatbelt usage. As a result, children were more likely to comply with helmet wearing. In contrast, while fathers tended to wear helmets themselves while cycling, they were less focused on ensuring their children wore them. These results highlight a distinct difference in how mothers and fathers approached safety enforcement, as indicated by the logistic regression analysis.
Table 7.
Association between parents’ demographic factors and helmet use for children.
Most factors related to cycle accidents and helmet regulation had a statistically significant association with helmet usage among children (Table 8). The analysis revealed several significant factors associated with helmet use among children. Knowing someone killed in a cycle accident correlated with higher helmet usage with p-values of 0.030 and 0.049 for the youngest and oldest children, respectively. A strong parental requirement for helmet use was associated with high compliance rates (86.5% for the youngest child and 85.7% for the oldest child) and significant p-values (<0.001). Community promotions of helmet use also showed a positive impact, with p-values of 0.014 and 0.003. An awareness of helmet laws in Saudi Arabia significantly contributed to helmet use, with p-values of 0.001 and 0.002.
Table 8.
Association between parents’ knowledge of injuries and helmet regulations and helmet use in children.
Multivariable logistic regression models were constructed to examine the simultaneous effect of multiple predictors (and covariates) (Table 9). Out of seven potential predictors of the likelihood of helmet use among the youngest children included in regression model 1, only one (“Did your parents require you to wear a helmet as a young child”) remained statistically significant. Parents who wore helmets as young children were 5.85 times more likely to have their youngest child wear a helmet compared to parents who did not wear a helmet as children. Out of seven potential predictors of the likelihood of helmet use among the youngest children included in regression model 2, only one (helmet use by parents) remained statistically significant (p < 0.002). Parents who wore helmets were 7.98 times more likely to have their oldest child wear a helmet compared to non-helmet-wearing parents.
Table 9.
Binary logistic regression results.
A statistically significant association was found between being injured when cycling and owning a helmet. Study participants who were injured when cycling were significantly more likely to own a helmet (61.7%) compared to those who were uninjured (43.6%), p = 0.026 (Table S1).
Table S2 summarizes responses to cycle accidents and helmet regulation questions. Most participants (58.9%) personally knew someone injured while cycling and about 19.9% personally knew someone who was killed in a cycling accident.
As children, 19.5% of the respondents’ parents required them to wear helmets. Some respondents (27.8%) recalled helmet promotion within their community during the past year and 49.8% were aware of helmet laws in Saudi Arabia (Table S2). Most parents (55.9%) always encouraged their children to wear seatbelts when riding in the car (Table S3). When combining the responses of “fairly often”, “frequently”, and “always”, a total of 78.6% of parents were classified in the “high” category for encouraging children to wear a seatbelt when riding in the car (Table S3).
Parents who wore helmets had stronger expectations for their children to do so and reported their children as wearing helmets more often (p < 0.001) (Table S4). Perceived peer pressure had a negative influence on helmet rules and helmet use by children (Table S4). The effect of peer pressure and parents without strong helmet rules showed that most parents did not wear helmets and believed their child’s friends also did not wear them, with significant p-values of 0.013 and <0.001, respectively (Table S5). They also expressed concerns about being judged by other parents for enforcing helmet use (p = 0.003). Fears about upsetting children when peers did not wear helmets and perceptions about style showed no significant difference. The belief that parents’ friends did not require helmet use was significantly higher among parents with weak rules (p = 0.004). This study’s findings are closely aligned with its objectives, offering valuable insights into helmet use behaviors, attitudes, and influencing factors. Helmet ownership among children was relatively low, with only 45.1% of the youngest and 48.2% of the oldest owning bicycles, and helmet-wearing rates were notably inconsistent, especially during unsupervised cycling. These results fulfill the objective of measuring helmet use prevalence while revealing gaps in protective behaviors. Parental attitudes toward helmet use were strong, with over 90% of parents scoring high on the “Belief” and “Attitude” subscales, meeting the goal of assessing how much importance parents place on helmets for safety. However, a disconnect was noted between these strong beliefs and actual helmet use among children, highlighting barriers to compliance. Sociodemographic factors, including parental education, gender, and income, significantly impacted helmet use, with mothers more frequently enforcing helmet rules and fathers demonstrating higher personal helmet usage. These findings address the objective of examining how sociodemographic factors influence parental decisions, providing a detailed understanding of the challenges and opportunities for enhancing helmet use behaviors in Saudi Arabia.
4. Discussion
This study offers important insights into bicycle helmet use among children in Saudi Arabia and factors that influence parental decisions regarding helmet use. The initial hypothesis posited cycle helmet usage among children in Saudi Arabia is low, with approximately 90% of children not wearing helmets [24]. However, our findings indicate that the percentage of children wearing helmets is 59.8% for the youngest child and 62.4% for the oldest child, which is higher than the expected rate of 30% [19] and very close to another study that reported 58% of children wore helmets [26]. Another study reported that 43% of children never wore a helmet when cycling [27]. The relatively high prevalence of helmet use could reflect a growing awareness of helmet safety in Saudi Arabia, possibly due to recent public health initiatives or changing safety norms among parents.
The finding that parents exhibit positive attitudes toward helmet use yet fail to align these attitudes with corresponding behaviors raises significant concerns regarding the effectiveness of public health messaging and intervention strategies in promoting safety practices. In our study, 93.7% of parents acknowledged that helmets can prevent head injuries; however, only 60–70% reported consistently enforcing helmet use for their children. This disconnect highlights a critical gap between parental beliefs and actual behaviors, reinforcing that mere awareness is insufficient for driving behavioral change. Our hypothesis anticipated an even greater gap, with the expectation that up to 97% of parents would recognize the protective benefits of helmets against injuries [25]. The observed discrepancy suggests that while parents understand the importance of helmet safety, various barriers [24,28] may hinder their ability to implement this critical safety measure consistently.
These barriers could include practical challenges, such as a limited access to helmets or perceived inconvenience in ensuring their children wear them during activities such as cycling or scootering [26]. Furthermore, parents may lack the necessary resources or support systems to reinforce helmet use consistently. Social norms and peer influences could also play a pivotal role, with parents potentially underestimating the importance of modeling safe practices in front of their children or feeling pressure to conform to behaviors observed in their communities [26,28].
A study showed that a 10% decrease in household income would result in a 9% reduction in helmet usage [24,25]. Our study found no significant link between socioeconomic status and actual helmet use, contradicting previous research indicating that helmet use declines with lower household income and helmet use [24,25]. This challenges the notion that financial barriers are the primary factors affecting helmet usage in Saudi Arabia. The finding that helmet affordability is not perceived as a significant factor influencing helmet use in Saudi Arabia necessitates further investigation, particularly among families of lower socioeconomic statuses. While our study indicates that cost may not be a primary barrier for many, it is crucial to recognize that families with limited financial resources could face distinct challenges that impact their ability to purchase helmets. Additional research should explore these nuances and examine the availability and effectiveness of state subsidies for helmets, as such initiatives might alleviate financial barriers for underserved families.
Moreover, understanding the perceptions of parents from lower socioeconomic backgrounds regarding helmet safety and affordability could reveal important attitudes affecting helmet use behaviors. Qualitative research focusing on the experiences of these families may uncover obstacles and motivations often overlooked in quantitative studies [24,25]. Ultimately, to validate our findings on affordability and its relation to helmet usage, a comprehensive examination of socioeconomic factors and the broader context of public health initiatives is necessary. Addressing these gaps can enhance strategies to promote helmet use and improve child safety across all population segments in Saudi Arabia.
Parental helmet ownership and use emerged as the strongest predictors for children’s helmet use, and >80% of children wear helmets if their parents do so. We confirmed a statistically significant relationship, indicating that parents who wear helmets themselves are more likely to expect their children to do the same [24,25]. This emphasizes the importance of parental role modeling in safety practices, suggesting that initiatives aimed toward encouraging helmet use among parents could positively influence children’s behaviors. Having adult companions greatly lowers the chances of children using helmets incorrectly, highlighting the important role of parental involvement in promoting helmet use [28].
Another significant finding is the impact of parental supervision on helmet use. Younger children are more likely to be supervised while riding, and parents, especially mothers, are more likely to promote helmet use for younger children than older ones. This may stem from a perceived decrease in risk as children age, which does not accurately reflect their ongoing vulnerability to head injuries. Educational programs emphasizing the importance of helmet use for all age groups could help mitigate this issue.
This study did not find substantial differences in helmet use based on geographic location or parental attitudes, which were initially expected to influence outcomes. This may indicate that the factors affecting helmet use in Saudi Arabia are less regionally specific and more broadly applicable, suggesting a nationwide cultural or social attitude toward helmet use. However, further investigation is necessary to uncover potential nuances not addressed in this analysis. The mean attitude score was 5.49 (SD = 0.91), with a substantial majority of respondents (93.3%) reporting a “high” score (≥4), indicating that parents are generally aware of the importance of helmet use. This is consistent with studies showing a significant percentage of parents recognize the protective benefits of helmets [24,25,28].
A study indicated that 85% of bicycle-related head injuries could be prevented by wearing helmets, highlighting the critical role of parental awareness in promoting helmet use among children [29]. Bicycle helmets decrease the likelihood of head injuries by 48%, serious head injuries by 60%, fatal head injuries by 71%, and traumatic brain injuries by 53%, emphasizing the vital role of helmets in preventing serious injuries and further supporting the need for broader helmet usage [30].
A significant predictor is parental helmet usage; parents who wear helmets themselves are 7.98 times more likely to have their children wear helmets. Parents who wore helmets as children are 5.85 times more likely to ensure their youngest child wears one, demonstrating the lasting impact of early safety education. Our findings indicate helmet ownership and use by parents significantly correlate with increased helmet usage among children. The highest rates (where 90% of children wore helmets) were observed when parents owned helmets and wore them regularly, compared to only 38% when parents did not. Mothers enforced higher helmet usage (64.3%) among their younger children compared to fathers (50.7%). This trend aligns with other studies that highlight the positive relationship between parent and child helmet use, suggesting that parental behavior and practices are crucial in promoting safety measures among children [24,31].
Direct comparisons indicated that children’s safety behaviors are more strongly influenced by their parents’ safety practices than by how parents communicate safety information [32]. A rural focus group study found that some parents might be encouraged to model helmet use if they believed it was important to align their own behavior with the expectations they set for their children [18].
High scores were observed in related domains that influence helmet use: beliefs about helmet use (M = 5.45; 95.9% of respondents had a “high” score), knowledge about helmet safety (M = 4.63; 80.9% had “high” scores), and self-reported behavior (M = 4.56; 71.1% had “high” scores). The related domain scores, particularly the belief score of M = 5.45, suggest that parents understand the importance of helmets and believe in their efficacy. This belief is crucial as it influences parents’ and children’s behaviors. Research has shown that when parents have strong beliefs about helmet safety, they are more likely to enforce helmet use among their children [14,33]. The knowledge score of 4.63 indicates that while many parents are informed about helmet safety, there is still room for improvement. Educational interventions targeting parents can enhance their knowledge and, consequently, their children’s safety practices. Previous studies have demonstrated that increased knowledge about helmet safety correlates with higher rates of helmet use among children [29].
The results also suggest potential inconsistencies in the enforcement of helmet use and personal adherence to helmet-wearing practices. This study highlights a notable gap between parents’ beliefs about helmet safety and children’s helmet use. Although most parents (93.7%) think helmets help prevent head injuries, this belief does not translate into consistent helmet use. Parents who do not enforce strict helmet rules report much lower usage rates (24.0% for their youngest child and 25.3% for their oldest) compared to those who implement such rules (77.3% and 81.5%, respectively, p < 0.001). The absence of family role models negatively impacts helmet use. A qualitative study found that children were less inclined to wear helmets if their parents did not demonstrate this behavior [34].
Research on road safety education indicates that although parents recognize the importance of safety practices, this understanding does not always lead to appropriate actions. For example, many parents acknowledge the dangers of speeding and helmet use, yet a considerable number permit their children to engage in unsafe behaviors, such as riding without helmets. This discrepancy between knowledge and action highlights the necessity of not only raising parental awareness but also ensuring the consistent enforcement of safety regulations [35].
The challenge of translating parents’ beliefs about helmet safety into actual behavior, specifically the consistent use of helmets by children, is affected by several factors. For example, the knowledge gap among parents regarding the importance of consistent helmet use and their lack of enforcement of safety rules act as significant obstacles that ultimately affect children’s helmet usage. Insufficient knowledge about helmet safety posed a significant obstacle. This highlights the need to focus on educational programs for children and parents in order to enhance helmet use by increasing awareness and promoting positive safety practices [34]. This suggests that merely believing in helmet safety is insufficient; enforcing rules is essential for increasing helmet use.
Parents’ actions, such as monitoring and knowledge of safety, significantly influence helmet usage. Children whose parents actively promote other safety practices, such as seatbelt use, tend to wear helmets more often (41.2% for low monitoring versus 65.1% for high monitoring, p = 0.002). Parents with better knowledge about helmet safety are more likely to enforce helmet use (46.5% for low knowledge compared to 62.9% for high knowledge, p = 0.048). These results emphasize the need to convert beliefs into actions by enforcing safety practices to boost helmet usage.
Parents aware of helmet safety laws in Saudi Arabia are more likely to enforce helmet use, at 69.7% among those aware of the regulations with respect to compliance versus 49.1% among those unaware of the regulations. Public safety campaigns positively influence behavior; 72.1% of parents who remember helmet safety promotions enforce helmet use compared to only 54.7% of parents who do not recall such campaigns but enforce helmet use. This highlights the importance of community and public awareness efforts in fostering safer behaviors. Children (51%) consistently wore helmets while cycling [14], while our study showed around 60% of children using helmets, indicating an improvement in helmet use among children in Saudi Arabia.
Parents who did not enforce helmet rules experienced greater peer pressure, often agreeing that their peers did not require helmets for their children, and they noticed that their children’s friends also did not wear helmets [13,36]. Our study found that peer pressure has a negative effect on helmet rules and usage among children. This pressure is perceived in children and parents with their own peers. Regarding sociodemographic factors, one study in the United States found that children of single parents were less likely to own helmets [25]. However, in our study, there was no significant relationship between socioeconomic status and helmet use, possibly reflecting cultural or contextual differences influencing helmet ownership and usage.
In open-ended questions, when parents were asked their top reasons for not requiring their children to wear helmets, a commonly reported answer was comfort issues (10% of parents). Studies examined attitudes from a child’s perspective and found the major factors relative to helmet-wearing resistance were appearance and comfort [24,37].
To effectively address the gap between positive attitudes toward helmet use and actual behaviors, targeted interventions are essential [25,26,38,39,40]. First and foremost, community education programs should aim to inform parents not only about the critical role of helmets in preventing injuries but also about strategies to overcome specific barriers to consistent helmet use. Recommended initiatives include providing affordable helmet distribution, hosting educational workshops that demonstrate the proper usage of helmets, and organizing community events that promote safe cycling habits. Additionally, creating environments where helmet use is normalized among peers can further reinforce positive behavioral change within families.
By bridging this gap, we can cultivate a culture of safety that encourages consistent helmet use among children. This, in turn, has the potential to significantly reduce the incidence of head injuries associated with cycling and related activities, ultimately supporting the broader goal of improving public health outcomes in our communities. Addressing the disconnect between parental beliefs and behaviors is a crucial step in enhancing the efficacy of injury prevention initiatives aimed at protecting children.
Our findings highlight the impact of safety campaigns and highlight the potential for even greater improvements in helmet use through parental modeling and community awareness [38,39,40]. Public health initiatives should prioritize increasing helmet ownership and promoting the benefits of helmet use, particularly targeting families with lower compliance rates. Awareness campaigns must not only emphasize the protective advantages of helmets but also address concerns related to comfort and appearance.
Collaboration between policymakers, public health authorities, schools, sports organizations, and community centers is essential to integrate helmet safety into broader safety education programs [38]. Educational programs aimed at parents can enhance their understanding of helmet safety and encourage the consistent enforcement of helmet use among their children. Engaging the community in discussions about cycling safety is crucial, as it can help identify barriers and foster a safety-oriented culture.
Furthermore, leveraging digital platforms presents an opportunity for intervention. Social media campaigns, influencer partnerships, and interactive online content can reach a wider audience, particularly younger parents. These efforts can be amplified by sharing personal stories and testimonials from other parents who prioritize helmet safety, thus creating a peer-driven movement [10,26,28]. To effectively bridge the gap between parental beliefs and actions, organizations can develop tools and resources—such as checklists or reminders—to support parents in consistently enforcing helmet use at home.
Interventions should also account for the differing influences of mothers and fathers on helmet usage, ensuring that both parents are involved in safety advocacy [26,28]. Additional research is needed to explore the underlying reasons for neutral attitudes toward helmet use, with the aim of shifting perceptions toward more positive views. Strategies to enhance bicycle ownership and improve access to helmets may also help mitigate barriers to safe cycling practices.
The ongoing monitoring of helmet usage trends and parental attitudes is essential to evaluate the effectiveness of interventions and policies over time, ultimately contributing to enhanced cycling safety for children in Saudi Arabia. To bridge the gap between parental awareness and the consistent enforcement of helmet use among children, robust public health policies in Saudi Arabia are needed. These policies should focus on raising awareness, encouraging role modeling, and strengthening the enforcement of helmet-wearing regulations. Given that socioeconomic status does not significantly affect helmet use, interventions should specifically target behavioral and cultural factors. National campaigns should promote helmet safety across urban and rural areas, emphasizing the importance of parental supervision and involvement and addressing concerns related to comfort and appearance. By aligning public health policies with these findings, Saudi Arabia can foster a culture of cycling safety, significantly reducing head injuries and promoting healthier practices for children.
5. Conclusions
This study highlights the need for improved helmet use among children in Saudi Arabia, revealing significant gaps between parental beliefs and actual behaviors, which remains a critical challenge. If these issues are not addressed, the risk of bicycle-related injuries among children is likely to persist. The findings underline the importance of targeted public health initiatives and community engagement in promoting helmet safety.
This study serves as a foundation for informing policy changes and educational programs aimed at enhancing helmet safety and introduces new insights into the discussion surrounding helmet safety, emphasizing the importance of the gender difference—mothers being more likely to enforce helmet use for children—and community engagement. Future initiatives should incorporate these dimensions to foster a more robust culture of safety regarding helmet use.
This study is subject to several limitations that affect the generalizability of its findings regarding helmet use among children in Saudi Arabia, thereby influencing its external validity. The attitudes toward helmet use are significantly shaped by cultural norms and practices, suggesting that the unique context of Saudi Arabia may differ markedly from that of other countries, which could restrict the applicability of the results. Despite the inclusion of a diverse sample from all 13 regions of the country, local variations in demographics, attitudes, and cycling behaviors—particularly between urban and rural areas—could impact the findings.
Furthermore, the reliance on convenience sampling introduces additional constraints with respect to generalizability, as the resultant sample may not accurately represent the broader population in terms of helmet use behaviors and parental attitudes. Variations in awareness and education concerning helmet safety across different communities can also contribute to disparities in compliance rates, complicating the extrapolation of our results. Additionally, temporal factors must be considered; shifts in public health policies, safety campaigns, and societal attitudes may influence helmet usage patterns over time, thereby affecting the relevance of the findings.
Overall, the reliance on convenience sampling may have introduced selection bias, which limits the generalizability of the findings. Convenience sampling involves selecting participants who are readily available and willing to participate rather than employing a random sampling method that provides a more representative cross-section of the population; as a result, our sample may not accurately reflect the characteristics and behaviors of the broader population concerning helmet use among children.
This susceptibility to selection bias could limit the generalizability of our findings, as the attitudes and behaviors observed in our sample may differ from those in the general population. For instance, participants who volunteered for the study may have had a greater interest in safety or may have been influenced by their demographics—such as age, socioeconomic status, or geographic location—in ways that are not representative of all families in Saudi Arabia. Consequently, while our study provides valuable insights, it is essential to interpret the results with caution, acknowledging that they may not fully extend to all children in the country. Future research utilizing more robust sampling methods will be crucial for validating our findings and improving their applicability to the wider population. Self-reported population data can result in response bias, as parents may overstate their children’s helmet use or their compliance with safety measures due to social desirability. To mitigate potential biases and enhance the robustness of our findings, we implemented adjustments for the key confounding variables, including socioeconomic status and educational attainment, both of which are known to influence helmet use behaviors. While our results are consistent with those of similar studies, it is important to note that the specific factors influencing helmet use may not be universally applicable, underscoring the need for comparative research across diverse cultural and geographic contexts. The cross-sectional design further constrains the ability to draw causal inferences regarding the observed relationships, necessitating caution in interpretation. Thus, the direction and magnitude of bias may lean toward overestimating helmet usage rates and parental attitudes.
Our findings reveal a helmet use prevalence of approximately 60% among children in Saudi Arabia, a figure that is notably higher than the rates reported in some other regions. Studies in the United States, for instance, have consistently documented significantly lower helmet use prevalence among children and adolescents [1,2,31]. This disparity may reflect differences in cultural norms [25], the enforcement of safety regulations, or the availability and affordability of helmets. Further research is needed to pinpoint the exact contributing factors and ascertain whether this higher prevalence is a unique characteristic of Saudi Arabia or whether broader trends are reflected within specific sociocultural contexts. Further exploration is needed to understand the underlying reasons for neutral attitudes toward helmet use. It is essential to investigate the specific beliefs, perceptions, and cultural attitudes that contribute to these neutral stances. Identifying whether factors such as a lack of awareness about the benefits of helmet use, perceived stigma, or whether social norms play a role can provide valuable insights into why families may not prioritize this important safety measure.
Additionally, it is crucial to examine the barriers that hinder compliance with helmet-wearing practices. These barriers may include economic factors, accessibility issues, or a lack of enforcement of safety regulations. We acknowledge the observed differences in approaches between mothers and fathers in our study and recommend that future research incorporates qualitative investigations to explore the underlying factors influencing these discrepancies regarding helmet use. Understanding these challenges can inform the design of interventions that specifically target the obstacles families face in adopting helmet use for their children.
Moreover, assessing the long-term effectiveness of implemented safety campaigns is vital. It is important to evaluate whether these initiatives successfully change attitudes and behaviors over time and whether they continue to resonate with the community. Longitudinal studies could provide insight into the sustainability of any behavioral changes and help identify the key elements that contribute to the success or failure of these campaigns.
Through ongoing research, we can ensure that strategies are continually adapted to meet the evolving needs of families and communities. By engaging with local stakeholders, conducting focus groups, and implementing community feedback, we can create evidence-based interventions that are more likely to resonate with the target populations. This iterative approach will help to foster a culture of safety that prioritizes helmet use and enhances overall public health outcomes.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/su17041468/s1. Table S1: Association between being injured and helmet ownership, n = 161. Table S2: Cycle accidents and helmet regulation, n = 492. Table S3: Children wear seatbelts while riding in the car. Table S4: Role modeling hypothesis. Table S5: Peer pressure hypothesis.
Author Contributions
Conceptualization, L.R.B.; Methodology, L.R.B., R.A.A. (Razan A. Alotaibi), L.A.A., W.M.A., R.A.A. (Roaa A. Alharbi) and A.H.A.; Software, R.A.A. (Razan A. Alotaibi), L.A.A. and W.M.A.; Validation, L.R.B.; Formal analysis, L.R.B., R.A.A. (Razan A. Alotaibi), L.A.A., W.M.A., R.A.A. (Roaa A. Alharbi) and A.H.A.; Investigation, L.R.B., R.A.A. (Razan A. Alotaibi) and L.A.A.; Resources, L.R.B.; Data curation, R.A.A. (Razan A. Alotaibi), L.A.A., W.M.A., R.A.A. (Roaa A. Alharbi) and A.H.A.; Writing—original draft, L.R.B., R.A.A. (Razan A. Alotaibi), L.A.A., W.M.A., R.A.A. (Roaa A. Alharbi) and A.H.A.; Writing—review & editing, L.R.B., R.A.A. (Razan A. Alotaibi), L.A.A., W.M.A., R.A.A. (Roaa A. Alharbi) and A.H.A.; Visualization, L.R.B.; Supervision, L.R.B.; Project administration, L.R.B.; Funding acquisition, L.R.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board. The Committee of King Saud University provided ethical approval before initiating the study (reference no. E-24-8498, on 15 January 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author L.R.B. upon request.
Acknowledgments
Special thanks are given for the support provided by the College of Medicine Research Center, Deanship of Scientific Research, King Saud University Riyadh, Saudi Arabia.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
DV, dependent variable; KKUH, King Khalid University Hospital; M, mean; OR, odds ratio; SD, standard deviation.
References
- Vittetoe, K.L.; Allen, J.H.; Unni, P.; McKay, K.G.; Yengo-Kahn, A.M.; Ghani, O.; Mummidi, P.; Greeno, A.L.; Bonfield, C.M.; Lovvorn, H.N.B. Socioeconomic factors associated with helmet use in pediatric ATV and dirt bike trauma. Trauma Surg. Acute Care Open 2022, 7, e000876. [Google Scholar] [CrossRef]
- World Health Organization. Helmets: A Road Safety Manual for Decision-Makers and Practitioners, 2nd ed.; World Health Organization: Geneva, Switzerland, 2023. [Google Scholar]
- Secginli, S.; Cosansu, G.; Nahcivan, N.O. Factors associated with bicycle-helmet use among 8–16 years aged Turkish children: A questionnaire survey. Int. J. Inj. Control Saf. Promot. 2014, 21, 367–375. [Google Scholar] [CrossRef]
- Waltzman, D.; Sarmiento, K.; Zhang, X.; Miller, G.F. Estimated prevalence of helmet use while bicycling, rollerblading, and skateboarding among middle school students in selected US States—Youth Behavior Risk Survey, 2013–2019. J. Saf. Res. 2023, 87, 367–374. [Google Scholar] [CrossRef]
- Klein, K.S.; Thompson, D.; Scheidt, P.C.; Overpeck, M.D.; Gross, L.A. Factors associated with bicycle helmet use among young adolescents in a multinational sample. Inj. Prev. 2005, 11, 288–293. [Google Scholar] [CrossRef]
- American Academy of Pediatrics. AAP: Helmets Save Lives & Reduce Risk of Traumatic Brain Injury; American Academy of Pediatrics: Itasca, IL, USA, 2022; Available online: https://www.healthychildren.org/ (accessed on 17 March 2024).
- Gross, I.; Weiss, D.J.; Eliasi, E.; Bala, M.; Hashavya, S. E-Bike-Related Trauma in Children and Adults. J. Emerg. Med. 2018, 54, 793–798. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, T.; Hills, N.K.; Knott, P.D.; Murr, A.H.; Seth, R. Association between conventional bicycle helmet use and facial injuries after bicycle crashes. JAMA Otolaryngol. Head. Neck Surg. 2019, 145, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.K.; Flaherty, M.R.; Blanchard, A.M.; Agarwal, M. Helmet use in preventing head injuries in bicycling, snow sports, and other recreational activities and sports. Pediatrics 2022, 150, e2022058878. [Google Scholar] [CrossRef]
- Sullins, V.F.; Yaghoubian, A.; Nguyen, J.; Kaji, A.H.; Lee, S.L. Racial/ethnic and socioeconomic disparities in the use of helmets in children involved in bicycle accidents. J. Pediatr. Surg. 2014, 49, 1000–1003. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, R.; Krisch, I.M.; Schroeder, D.R.; Flick, R.; Nemergut, M.E. Pediatric bicycle-related head injuries: A population-based study in a county without a helmet law. Inj. Epidemiol. 2015, 2, 16. [Google Scholar] [CrossRef]
- Williams, C.; Weston, R.; Feinglass, J.; Crandall, M. Pediatric bicycle helmet legislation and crash-related traumatic brain injury in Illinois, 1999–2009. J. Surg. Res. 2018, 222, 231–237. [Google Scholar] [CrossRef]
- Ross, L.T.; Brinson, M.K.; Ross, T.P. Parenting influences on bicycle helmet rules and estimations of children’s helmet use. J. Psychol. 2014, 148, 197–213. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.L.; Koepplinger, M.E.; Mehlman, C.T.; Gittelman, M.; Garcia, V.F. All-terrain vehicle and bicycle crashes in children: Epidemiology and comparison of injury severity. J Pediatr Surg. 2002, 37, 375–380. [Google Scholar] [CrossRef]
- Lajunen, T. Barriers and facilitators of bicycle helmet use among children and their parents. Transp. Res. Part F Traffic Psychol. Behav. 2016, 41, 294–301. [Google Scholar] [CrossRef]
- Piotrowski, C.C.; Warda, L.; Pankratz, C.; Dubberley, K.; Russell, K.; Assam, H.; Carevic, M. A comparison of parent and child perspectives about barriers to and facilitators of bicycle helmet and booster seat use. Int. J. Inj. Control Saf. Promot. 2020, 27, 276–285. [Google Scholar] [CrossRef]
- Verlinde, L.; Verlinde, F.; Van Doren, S.; De Coninc, D.; Toelen, J. Cycle safe or cycle cool? Adolescents’ views on bicycle helmet use and injury prevention campaigns in Belgium. Inj. Prev. 2024, 6, 2023–2227. [Google Scholar] [CrossRef]
- Robertson, D.W.; Lang, B.D.; Schaefer, J.M. Parental attitudes and behaviours concerning helmet use in childhood activities: Rural focus group interviews. Accid. Anal. Prev. 2014, 70, 314–319. [Google Scholar] [CrossRef]
- Wymore, C.; Denning, G.; Hoogerwerf, P.; Wetjen, K.; Jennissen, C. Parental attitudes and family helmet use for all-terrain vehicles and bicycles. Inj. Epidemiol. 2020, 7, 23. [Google Scholar] [CrossRef]
- Kulanthayan, K.M.; Teow, H.F.; Selvan, H.K.; Yellappan, K.; Ulaganathan, V. Determinants of standard motorcycle safety helmet usage among child pillion riders. Transp. Res. Part F Traffic Psychol. Behav. 2020, 74, 408–417. [Google Scholar] [CrossRef]
- Parkin, P.C.; Degroot, J.; Macpherson, A.; Fuselli, P.; Macarthur, C. Canadian parents’ attitudes and beliefs about bicycle helmet legislation in provinces with and without legislation. Chronic Dis. Inj. Can. 2014, 34, 8–11. [Google Scholar] [CrossRef]
- Senić, A.; Dobrodolac, M.; Stojadinović, Z. Development of Risk Quantification Models in Road Infrastructure Projects. Sustainability. 2024, 16, 7694. [Google Scholar] [CrossRef]
- Ivanišević, T.; Trifunović, A.; Čičević, S.; Pešić, D.; Simović, S.; Zunjic, A.; Duplakova, D.; Duplak, J.; Manojlovic, U. Analysis and Determination of the Lateral Distance Parameters of Vehicles When Overtaking an Electric Bicycle from the Point of View of Road Safety. Appl. Sci. 2023, 13, 1621. [Google Scholar] [CrossRef]
- Berg, P.; Westerling, R. Bicycle helmet use among schoolchildren—The influence of parental involvement and children’s attitudes. Inj. Prev. 2001, 7, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, J.D.; Harper, M.A.; Pardi, L.A.; Christopher, N.C. Parental knowledge and children’s use of bicycle helmets. Clin. Pediatr. 2003, 42, 673–677. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.S.; Soundappan, S.V.; Adams, S.; Adams, S. Helmet use in bicycles and non-motorised wheeled recreational vehicles in children. J. Paediatr. Child Health 2018, 54, 968–974. [Google Scholar] [CrossRef] [PubMed]
- Stead, T.S.; Daneshvar, Y.; Ayala, S.; Ganti, L. Knowledge, Awareness, and Attitudes Regarding Concussion Among Middle Schoolers. Cureus 2019, 11, e4863. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hagel, B.E.; Lee, R.S.; Karkhaneh, M.; Voaklander, D.; Rowe, B.H. Factors associated with incorrect bicycle helmet use. Inj. Prev. 2010, 16, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Strotmeyer, S.J.; Behr, C.; Fabio, A.; Gaines, B.A. Bike helmets prevent pediatric head injury in serious bicycle crashes with motor vehicles. Inj. Epidemiol. 2020, 7 (Suppl. S1), 24. [Google Scholar] [CrossRef]
- Høye, A. Bicycle helmets—To wear or not to wear? A meta-analyses of the effects of bicycle helmets on injuries. Accid. Anal. Prev. 2018, 117, 85–97. [Google Scholar] [CrossRef]
- Jewett, A.; Beck, L.F.; Taylor, C.; Baldwin, G. Bicycle helmet use among persons 5 years and older in the United States, 2012. J. Saf. Res. 2016, 59, 1–7. [Google Scholar] [CrossRef]
- Pierce, S.R.; Palombaro, K.M.; Black, J.D. Barriers to bicycle helmet use in young children in an urban elementary school. Health Promot. Pract. 2013, 15, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Morrongiello, B.A.; Corbett, M.; Bellissimo, A. “Do as I say, not as I do”: Family influences on children’s safety and risk behaviors. Health Psychol. 2008, 27, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Büth, C.M.; Barbour, N.; Abdel-Aty, M. Effectiveness of bicycle helmets and injury prevention: A systematic review of meta-analyses. Sci. Rep. 2023, 13, 8540. [Google Scholar] [CrossRef] [PubMed]
- Muir, C.; O’Hern, S.; Oxley, J.; Devlin, A.; Koppel, S.; Charlton, J.L. Parental role in children’s road safety experiences. Transp. Res. Part F Traffic Psychol. Behav. 2017, 46, 195–204. [Google Scholar] [CrossRef]
- McNicholas, C. Adolescents’ Perceptions of Helmet-Wearing Peers. Published Online 2010. Available online: https://ecommons.udayton.edu/graduate_theses/301/ (accessed on 24 October 2024).
- Finch, C.F. Teenagers’ attitudes towards bicycle helmets three years after the introduction of mandatory wearing. Inj. Prev. 1996, 2, 126–130. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ratanavaraha, V.; Jomnonkwao, S. Community participation and behavioral changes of helmet use in Thailand. Transp. Policy 2013, 25, 111–118. [Google Scholar] [CrossRef]
- Hoekstra, T.; Wegman, F. Improving the effectiveness of road safety campaigns: Current and new practices. Lancet 2011, 34, 80–86. [Google Scholar] [CrossRef]
- Wakefield, M.A.; Loken, B.; Hornik, R.C. Use of mass media campaigns to change health behaviour. Lancet 2010, 376, 1261–1271. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).