The Effect of a New Sodium Bicarbonate Loading Regimen on Anaerobic Capacity and Wrestling Performance

 ,
,  ,
, 
Abstract
:1. Introduction
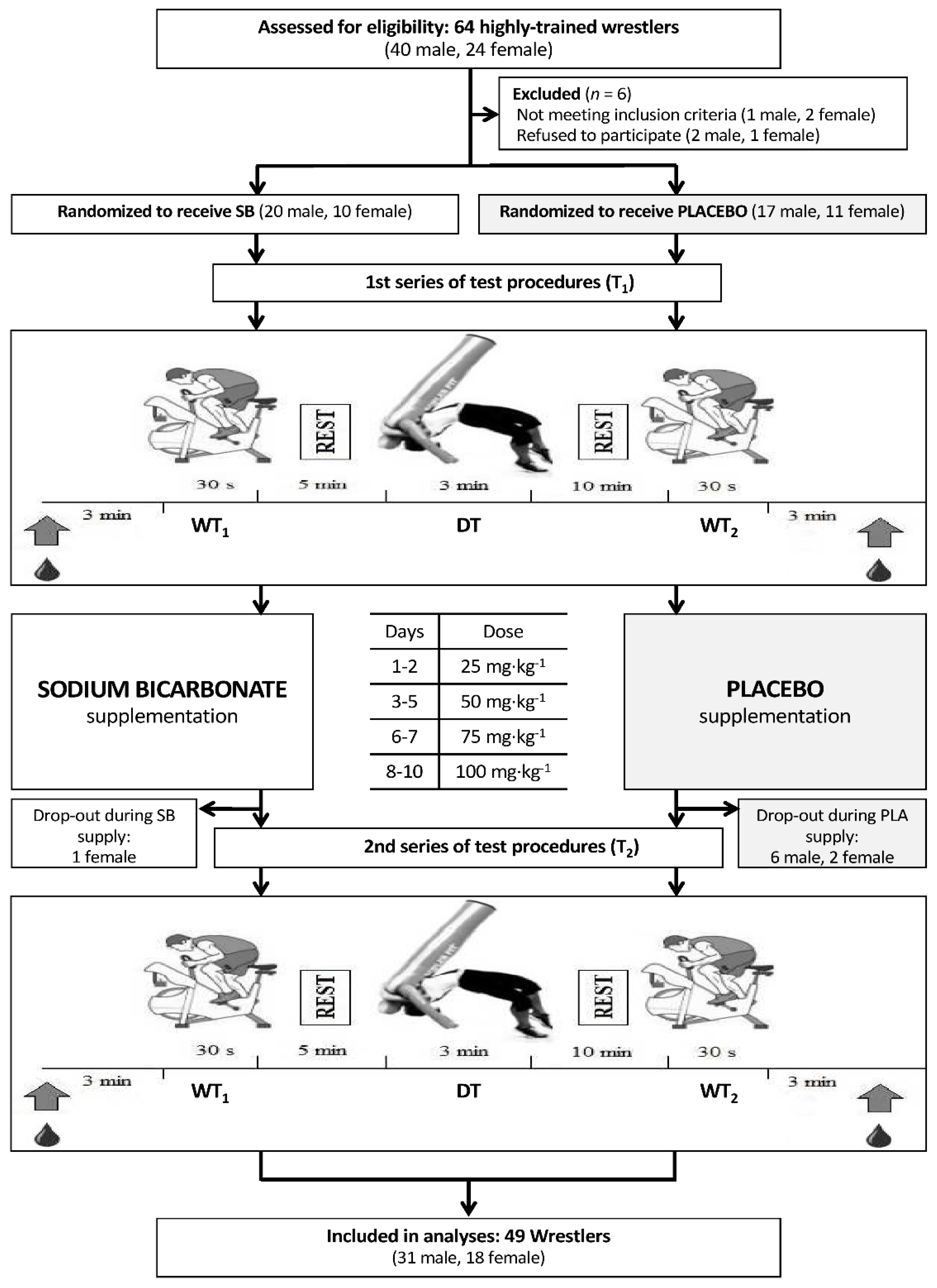
2. Materials and Methods
2.1. Participants
2.2. Experimental Protocol
2.3. Supplementation
2.4. Anthropometric Measurements
2.5. Exercise Tests
- slow mode—four compulsory suplex throws in 30 s
- quick mode—as many suplex throws as possible in 15 s
2.6. Blood Samples Analysis
2.7. Gastrointestinal Side Effects
2.8. Statistical Analysis
3. Results
3.1. Gastrointestinal Side Effects
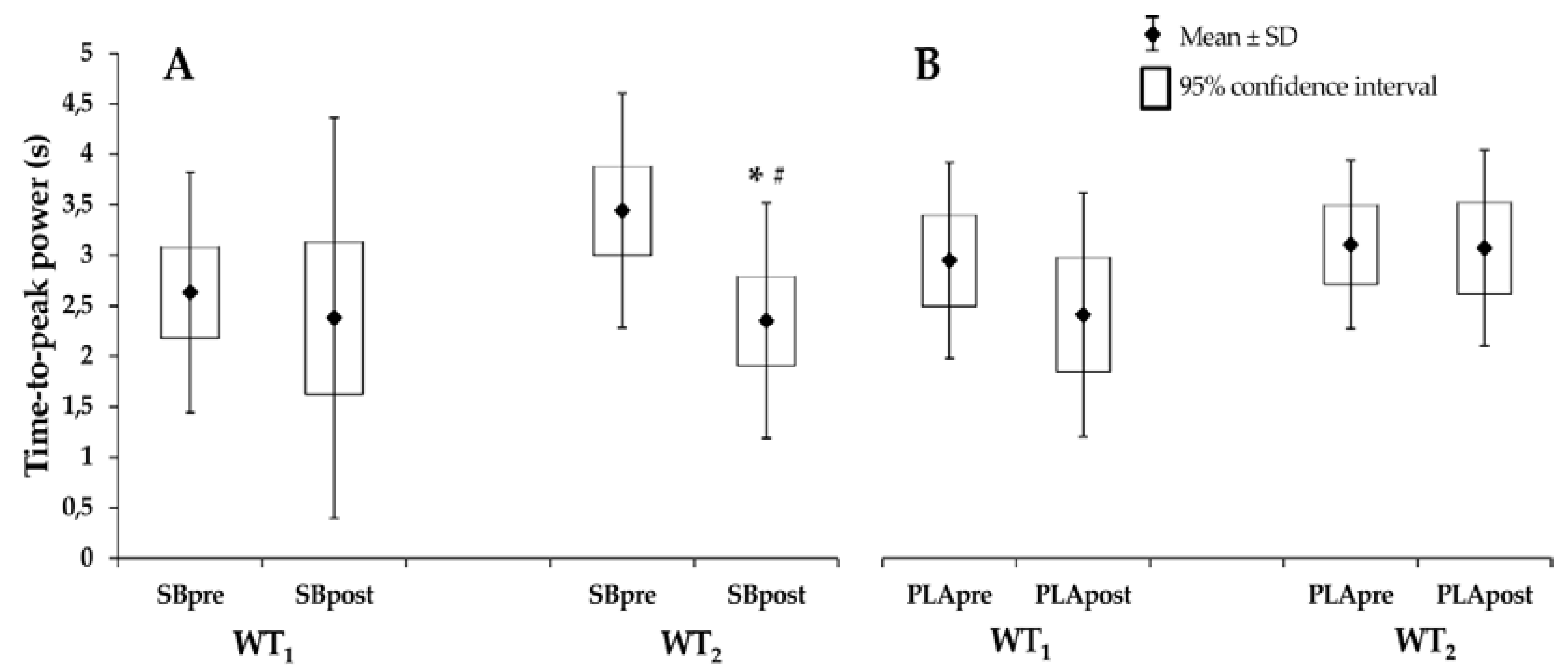
3.2. Anaerobic Power in the Wingate Test
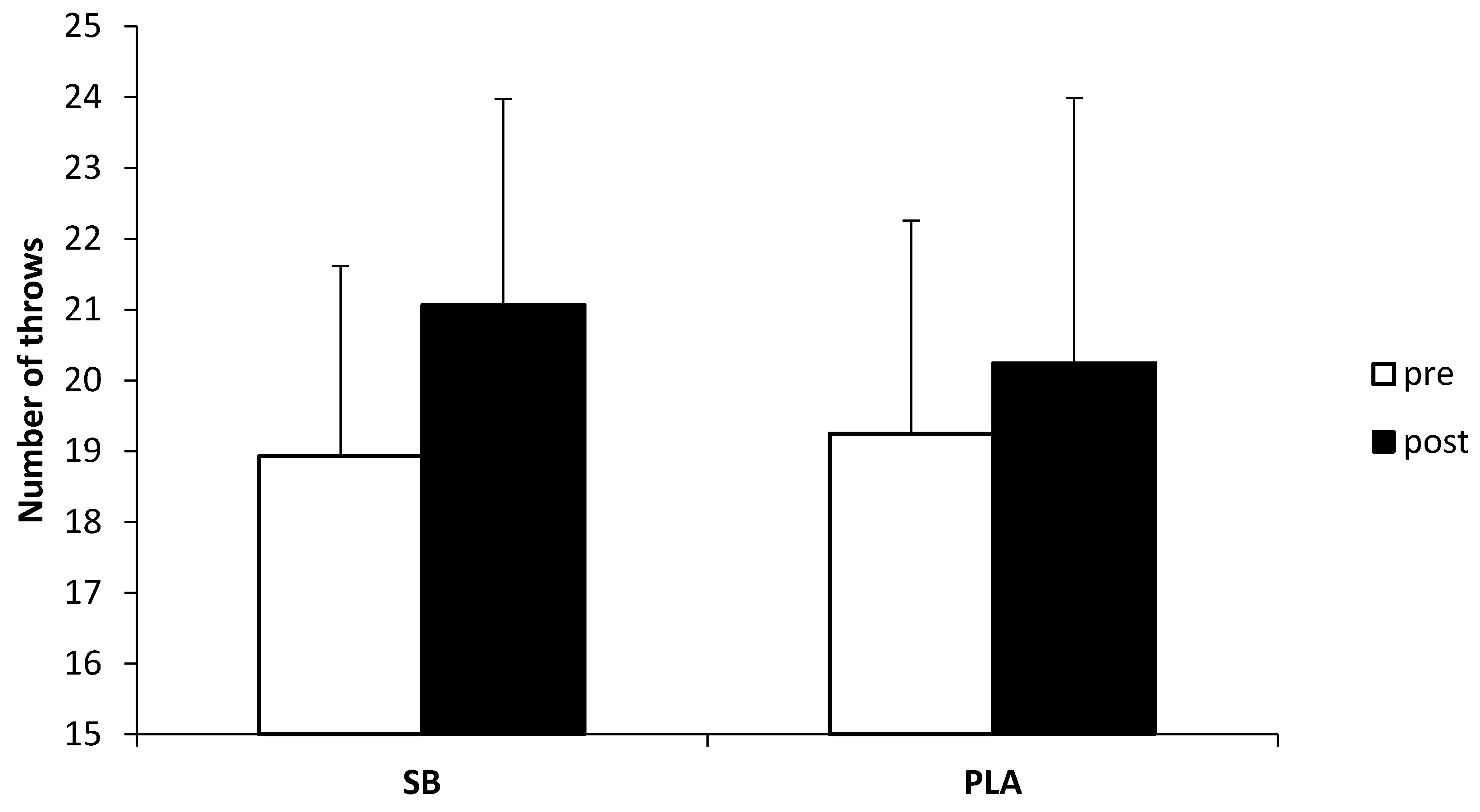
3.3. Dummy Throw Test
3.4. Glucose and Lactate Concentrations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Hübner-Wozniak, E.; Kosmol, A.; Lutoslawska, G.; Bem, E.Z. Anaerobic performance of arms and legs in male and female free style wrestlers. J. Sci. Med. Sport 2004, 7, 473–480. [Google Scholar] [CrossRef]
- Karnincic, H.; Tocilj, Z.; Uljevic, O.; Erceg, M. Lactate profile during Greco-Roman wrestling match. J. Sports Sci. Med. 2009, 8, 17–19. [Google Scholar] [PubMed]
- Demirkan, E.; Koz, M.; Kutlu, M.; Favre, M. Comparison of physical and physiological profiles in elite and amateur young wrestlers. J. Strength Cond. Res. 2015, 29, 1876–1883. [Google Scholar] [CrossRef] [PubMed]
- Coso, J.D.; Hamouti, N.; Agudo-Jimenez, R.; Mora-Rodriguez, R. Restoration of blood pH between repeated bouts of high-intensity exercise: Effects of various active-recovery protocols. Eur. J. Appl. Physiol. 2010, 108, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Abramowitz, M.K.; Hostetter, T.H.; Melamed, M.L. Lower serum bicarbonate and a higher anion gap are associated with lower cardiorespiratory fitness in young adults. Kidney Int. 2012, 81, 1033–1042. [Google Scholar] [CrossRef] [PubMed]
- Lancha Junior, A.H.; Painelli Vde, S.; Saunders, B.; Artioli, G.G. Nutritional strategies to modulate intracellular and extracellular buffering capacity during high-intensity exercise. Sports Med. 2015, 45 (Suppl. 1), 71–81. [Google Scholar] [CrossRef] [PubMed]
- Ciechanowski, K. To dialyze or to alkalyze? (Dializować czy alkalizować?). Forum Nefrol. 2012, 5, 347–350. [Google Scholar]
- Heisler, N. Buffering and H+ ion dynamics in muscle tissues. Respir. Physiol. Neurobiol. 2004, 144, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Juel, C. Regulation of pH in human skeletal muscle: Adaptations to physical activity. Acta Physiol. 2008, 193, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Carr, B.M.; Webster, M.J.; Boyd, J.C.; Hudson, G.M.; Scheett, T.P. Sodium bicarbonate supplementation improves hypertrophy-type resistance exercise performance. Eur. J. Appl. Physiol. 2013, 113, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Hollidge-Horvat, M.G.; Parolin, M.L.; Wong, D.; Jones, N.L.; Heigenhauser, G.J. Effect of induced metabolic alkalosis on human skeletal muscle metabolism during exercise. Am. J. Physiol. Endocrinol. Metab. 2000, 278, 316–329. [Google Scholar] [CrossRef] [PubMed]
- Sostaric, S.M.; Skinner, S.L.; Brown, M.J.; Sangkabutra, T.; Medved, I.; Medley, T.; Selig, S.E.; Fairweather, I.; Rutar, D.; McKenna, M.J. Alkalosis increases muscle K+ release, but lowers plasma [K+] and delays fatigue during dynamic forearm exercise. J. Physiol. 2006, 570 Pt 1, 185–205. [Google Scholar] [CrossRef] [PubMed]
- McNaughton, L.R.; Gough, L.; Deb, S.; Bentley, D.; Sparks, S.A. Recent developments in the use of sodium bicarbonate as an ergogenic aid. Curr. Sports Med. Rep. 2016, 15, 233–244. [Google Scholar] [CrossRef] [PubMed]
- Artioli, G.G.; Gualano, B.; Coelho, D.F.; Benatti, F.B.; Gailey, A.W.; Lancha, A.H. Does sodium-bicarbonate ingestion improve simulated judo performance? Int. J. Sport Nutr. Exerc. Metab. 2007, 17, 206–217. [Google Scholar] [CrossRef] [PubMed]
- Felippe, L.C.; Lopes-Silva, J.P.; Bertuzzi, R.; McGinley, C.; Lima-Silva, A.E. Separate and combined effects of caffeine and sodium-bicarbonate intake on judo performance. Int. J. Sports Physiol. Perform. 2016, 11, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Siegler, J.C.; Hirscher, K. Sodium bicarbonate ingestion and boxing performance. J. Strength Cond. Res. 2010, 24, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Krustrup, P.; Ermidis, G.; Mohr, M. Sodium bicarbonate intake improves high-intensity intermittent exercise performance in trained young men. J. Int. Soc. Sports Nutr. 2015, 12, 25. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.J.; Hopkins, W.G.; Gore, C.J. Effects of acute alkalosis and acidosis on performance: A meta-analysis. Sports Med. 2011, 41, 801–814. [Google Scholar] [CrossRef] [PubMed]
- Peart, D.J.; Siegler, J.C.; Vince, R.V. Practical recommendations for coaches and athletes: A meta-analysis of sodium bicarbonate use for athletic performance. J. Strength Cond. Res. 2012, 26, 1975–1983. [Google Scholar] [CrossRef] [PubMed]
- Maughan, R.J.; Burke, L.M.; Dvorak, J.; Larson-Meyer, D.E.; Peeling, P.; Phillips, S.M.; Rawson, E.S.; Walsh, N.P.; Garthe, I.; Geyer, H.; et al. IOC consensus statement: Dietary supplements and the high-performance athlete. Br. J. Sports Med. 2018, 52, 439–455. [Google Scholar] [CrossRef]
- Douroudos, I.I.; Fatouros, I.G.; Gourgoulis, V.; Jamurtas, A.Z.; Tsitsios, T.; Hatzinikolaou, A.; Margonis, K.; Mavromatidis, K.; Taxildaris, K. Dose-related effects of prolonged NaHCO3 ingestion during high-intensity exercise. Med. Sci. Sports Exerc. 2006, 38, 1746–1753. [Google Scholar] [CrossRef] [PubMed]
- Horswill, C.A.; Costill, D.L.; Fink, W.J.; Flynn, M.G.; Kirwan, J.P.; Mitchell, J.B.; Houmard, J.A. Influence of sodium bicarbonate on sprint performance: Relationship to dosage. Med. Sci. Sports Exerc. 1988, 20, 566–569. [Google Scholar] [CrossRef] [PubMed]
- Browman, S.A. The Effect of Different Dosing Strategies of Sodium Bicarbonate upon Collegiate Swimmers. MS in Exercise and Sports Science—Human Performance, University of Wisconsin-La Crosse. 2002. Available online: https://minds.wisconsin.edu/bitstream/handle/1793/48658/Obowmansteven2002.PDF?sequence=1 (accessed on 10 May 2018).
- Kahlea, L.E.; Kellyb, P.V.; Eliota, K.A.; Weissa, E.P. Acute sodium bicarbonate loading has negligible effects on resting and exercise blood pressure but causes gastrointestinal distress. Nutr. Res. 2013, 33, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Saunders, B.; Sale, C.; Harris, R.C.; Sunderland, C. Sodium bicarbonate and high-intensity-cycling capacity: Variability in responses. Int. J. Sports Physiol. Perform. 2014, 9, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Bentzur, K.M.; Kravitz, L.; Lockner, D.W. Evaluation of the BOD POD for estimating percent body fat in collegiate track and field female athletes: A comparison of four methods. J. Strength Cond. Res. 2008, 22, 1985–1991. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical impedance analysis-part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef] [PubMed]
- Starosta, W.; Baić, M. Battery of tests for evaluation level of motor abilities in high advanced wrestlers from perspective of 32 years of using in practice. Arch. Budo Sci. Martial Art Extreme Sport 2015, 11, 213–222. [Google Scholar]
- Anioł-Strzyżewska, K.; Starosta, W. The evaluation of specific effort of the highly advanced wrestlers in the many years training cycle [Ocena specyficznej wydolności wysoko zaawansowanych zapaśników w wieloletnim cyklu treningowym]. Sci. J. Grad. Sch. Phys. Educ. Tour. Bialystok 2012, 8, 110–112. [Google Scholar]
- Bar-Or, O. The Wingate anaerobic test: An update on methodology, reliability and validity. Sports Med. 1987, 4, 381–394. [Google Scholar] [CrossRef] [PubMed]
- Maughan, R.J. A simple, rapid method for the determination of glucose, lactate, pyruvate, alanine, 3- hydroxybutyrate and acetoacetate on a single 20-mL blood sample. Clin. Chim. Acta 1982, 122, 231–240. [Google Scholar] [CrossRef]
- Jeukendrup, A.E.; Vet-Joop, K.; Sturk, A.; Stegen, J.H.; Senden, J.; Saris, W.H.; Wagenmakers, A.J. Relationship between gastro-intestinal complaints and endotoxaemia, cytokine release and the acute-phase reaction during and after a long-distance triathlon in highly trained men. Clin. Sci. 2000, 98, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; Turk, D.C.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Katz, N.P.; Kerns, R.D.; Stucki, G.; Allen, R.R.; Bellamy, N.; et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain 2005, 113, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Zabala, M.; Requena, B.; Sánchez-Muñoz, C.; González-Badillo, J.J.; García, I.; Oöpik, V.; Pääsuke, M. Effects of sodium bicarbonate ingestion on performance and perceptual responses in a laboratory-simulated BMX cycling qualification series. J. Strength Cond. Res. 2008, 22, 1645–1653. [Google Scholar] [CrossRef] [PubMed]
- Griffen, C.; Rogerson, D.; Ranchordas, M.; Ruddock, A. Effects of creatine and sodium bicarbonate congestion on multiple indices of mechanical power output during repeated Wingate tests in trained men. Int. J. Sport Nutr. Exerc. Metab. 2015, 25, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Tobias, G.; Benatti, F.B.; de Salles Painelli, V.; Roschel, H.; Gualano, B.; Sale, C.; Harris, R.C.; Lancha, A.H., Jr.; Artioli, G.G. Additive effects of beta-alanine and sodium bicarbonate on upper-body intermittent performance. Amino Acids 2013, 45, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, L.F.; de Salles Painelli, V.; Nemezio, K.; Gonçalves, L.S.; Yamaguchi, G.; Saunders, B. Gualano, B.; Artioli, G.G. Chronic lactate supplementation does not improve blood buffering capacity and repeated high-intensity exercise. Scand. J. Med. Sci. Sports 2017, 27, 1231–1239. [Google Scholar] [CrossRef] [PubMed]
- McNaughton, L.R. Bicarbonate ingestion: Effects of dosage on 60 s cycle ergometry. J. Sports Sci. 1992, 10, 415–423. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, D.C.; Coutts, K.D.; Stirling, D.R.; Hoeben, H.H.; Kuzara, G. Maximal work production following two levels of artificially induced metabolic alkalosis. J. Sports Sci. 1986, 4, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Mc Naughton, L.; Thompson, D. Acute versus chronic sodium bicarbonate ingestion and anaerobic work and power output. J. Sports Med. Phys. Fitness 2001, 41, 456–462. [Google Scholar] [PubMed]
- Carr, A.J.; Slater, G.J.; Gore, C.J.; Dawson, B.; Burke, L.M. Reliability and effect of sodium bicarbonate: Buffering and 2000-m rowing performance. Int. J. Sports Physiol. Perform. 2012, 7, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Joyce, S.; Minahan, C.; Anderson, M.; Osborne, M. Acute and chronic loading of sodium bicarbonate in highly trained swimmers. Eur. J. Appl. Physiol. 2012, 112, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Sant’Ana, J.; Franchini, E.; da Silva, V.; Diefenthaeler, F. Effect of fatigue on reaction time, response time, performance time, and kick impact in taekwondo roundhouse kick. Sports Biomech. 2017, 16, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Lima, E.V.; Tortoza, C.; Rosa, L.C.L.; Lopes-Martins, R.A.B. Study of the correlation between the velocity of motor reaction and blood lactate in different times of combat in judo. Rev. Bras. Med. Esporte 2004, 10, 339–343. [Google Scholar] [CrossRef]
- Bouhlel, E.; Jouini, A.; Gmada, N.; Nefzi, A.; Ben Abdallah, K.; Tabka, Z. Heart rate and blood lactate responses during taekwondo training and competition. Sci. Sports 2006, 21, 285–290. [Google Scholar] [CrossRef]
- Özdemir, R.A.; Kirazcı, S.; Ugras, A. Simple reaction time and decision making performance after different physical workloads: An examination with elite athletes. IJHS 2010, 7, 655–670. [Google Scholar]
- Lopes-Silva, J.P.; Da Silva Santos, J.F.; Artioli, G.G.; Loturco, I.; Abbiss, C.; Franchini, E. Sodium bicarbonate ingestion increases glycolytic contribution and improves performance during simulated taekwondo combat. Eur. J. Sport Sci. 2018, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.; Bishop, D.J.; Lambert, K.; Mercier, J.; Brooks, G.A. Effects of acute and chronic exercise on sarcolemmal MCT1 and MCT4 contents in human skeletal muscles: Current status. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2012, 302, R1–R14. [Google Scholar] [CrossRef] [PubMed]
- Siegler, J.C.; Marshall, P.W.; Bishop, D.; Shaw, G.; Green, S. Mechanistic insights into the efficacy of sodium bicarbonate supplementation to improve athletic performance. Sports Med. Open 2016, 2, 41. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Sodium Bicarbonate Group | Placebo Group |
|---|---|---|
| Mean ± SD | Mean ± SD | |
| Number of subjects (n) | 29 | 20 |
| Age (years) | 19 ± 4 | 18 ± 4 |
| Height (cm) | 173 ± 9 | 171 ± 7 |
| Training types [the number of training sessions during one week]: | ||
| Wrestling training | 5 ± 1 | 5 ± 1 |
| Running training | 1 ± 1 | 2 ± 1 |
| Resistance training | 1 ± 1 | 1 ± 0 |
| Variable | Sodium Bicarbonate Trial | Placebo Trial | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Day 1 | Day 3 | Day 5 | Day 8 | Day 10 | Day 1 | Day 3 | Day 5 | Day 8 | Day 10 | |
| Stomach problems | 1.0 ± 1.0 | 0.8 ± 0.9 | 0.6 ± 1.0 | 0.5 ± 0.8 | 0.3 ± 0.6 | 0.8 ± 1.2 | 0.3 ± 0.6 | 0.6 ± 0.8 | 0.8 ± 1.0 | 0.6 ± 0.9 |
| Nausea | 0.3 ± 0.6 | 0.4 ± 0.6 | 0.2 ± 0.6 | 0.2 ± 0.5 | 0.1 ± 0.4 | 0.3 ± 0.5 | 0.3 ± 0.7 | 0.3 ± 0.4 | 0.3 ± 0.6 | 0.2 ± 0.5 |
| Dizziness | 0.1 ± 0.3 | 0.1 ± 0.4 | 0.3 ± 0.8 | 0.1 ± 0.3 | 0.1 ± 0.3 | 0.2 ± 0.4 | 0.2 ± 0.7 | 0.3 ± 0.4 | 0.1 ± 0.3 | 0.0 ± 0.0 |
| Headache | 0.6 ± 0.5 | 0.6 ± 0.9 | 0.2 ± 0.8 | 0.2 ± 0.6 | 0.4 ± 0.8 | 0.5 ± 0.9 | 0.6 ± 1.0 | 0.7 ± 1.0 | 0.4 ± 0.8 | 0.3 ± 0.8 |
| Flatulence | 0.3 ± 0.6 | 0.2 ± 0.4 | 0.3 ± 0.5 | 0.2 ± 0.4 | 0.2 ± 0.4 | 0.2 ± 0.5 | 0.2 ± 0.5 | 0.2 ± 0.4 | 0.1 ± 0.3 | 0.1 ± 0.3 |
| Urge to urinate | 0.3 ± 0.6 | 0.2 ± 0.5 | 0.3 ± 0.5 | 0.1 ± 0.4 | 0.1 ± 0.3 | 0.3 ± 0.6 | 0.2 ± 0.4 | 0.4 ± 0.6 | 0.2 ± 0.4 | 0.2 ± 0.4 |
| Urge to defecate | 0.3 ± 0.7 | 0.2 ± 0.5 | 0.1 ± 0.6 | 0.4 ± 0.8 | 0.4 ± 0.8 | 0.3 ± 0.6 | 0.3 ± 0.7 | 0.6 ± 1.0 | 0.3 ± 0.6 | 0.2 ± 0.4 |
| Belching | 0.4 ± 0.9 | 0.3 ± 0.7 | 0.2 ± 0.5 | 0.3 ± 0.7 | 0.2 ± 0.5 | 0.1 ± 0.3 | 0.3 ± 0.7 | 0.2 ± 0.4 | 0.3 ± 0.7 | 0.2 ± 0.5 |
| Heartburn | 0.3 ± 0.7 | 0.2 ± 0.6 | 0.2 ± 0.6 | 0.1 ± 0.4 | 0.2 ± 0.6 | 0.1 ± 0.3 | 0.0 ± 0.0 | 0.1 ± 0.4 | 0.3 ± 0.6 | 0.2 ± 0.4 |
| Bloating | 0.2 ± 0.6 | 0.2 ± 0.6 | 0.3 ± 0.7 | 0.4 ± 0.8 | 0.3 ± 0.8 | 0.4 ± 0.9 | 0.2 ± 0.4 | 0.4 ± 0.8 | 0.3 ± 0.6 | 0.5 ± 0.8 |
| Stomach cramps | 0.0 ± 0.0 | 0.1 ± 0.4 | 0.3 ± 0.6 | 0.3 ± 0.8 | 0.3 ± 0.9 | 0.3 ± 0.5 | 0.3 ± 0.7 | 0.4 ± 0.7 | 0.4 ± 0.7 | 0.1 ± 0.3 |
| Intestinal cramps | 0.2 ± 0.7 | 0.2 ± 0.4 | 0.1 ± 0.3 | 0.1 ± 0.3 | 0.2 ± 0.5 | 0.2 ± 0.5 | 0.6 ± 0.9 | 0.1 ± 0.3 | 0.1 ± 0.3 | 0.1 ± 0.2 |
| Urge to vomit | 0.0 ± 0.0 | 0.1 ± 0.4 | 0.0 ± 0.2 | 0.0 ± 0.2 | 0.0 ± 0.2 | 0.0 ± 0.0 | 0.1 ± 0.3 | 0.3 ± 0.6 | 0.1 ± 0.2 | 0.1 ± 0.3 |
| Vomiting | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.2 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.3 ± 0.8 | 0.1 ± 0.2 | 0.0 ± 0.0 | 0.0 ± 0.0 |
| Diarrhea | 0.2 ± 0.5 | 0.2 ± 0.5 | 0.2 ± 0.6 | 0.3 ± 0.7 | 0.2 ± 0.4 | 0.5 ± 0.9 | 0.0 ± 0.0 | 0.2 ± 0.4 | 0.2 ± 0.6 | 0.3 ± 0.7 |
| Side ache left | 0.2 ± 0.5 | 0.0 ± 0.2 | 0.0 ± 0.2 | 0.0 ± 0.2 | 0.0 ± 0.2 | 0.0 ± 0.0 | 0.5 ± 0.8 | 0.4 ± 0.7 | 0.1 ± 0.2 | 0.1 ± 0.2 |
| Side ache right | 0.0 ± 0.2 | 0.0 ± 0.2 | 0.0 ± 0.2 | 0.0 ± 0.0 | 0.0 ± 0.2 | 0.0 ± 0.0 | 0.2 ± 0.4 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.2 ± 0.5 |
| Muscle cramps | 0.1 ± 0.3 | 0.3 ± 0.7 | 0.1 ± 0.4 | 0.3 ± 0.6 | 0.2 ± 0.6 | 0.6 ± 1.0 | 0.3 ± 0.6 | 0.2 ± 0.6 | 0.2 ± 0.6 | 0.1 ± 0.3 |
| Cold shivering | 0.1 ± 0.6 | 0.2 ± 0.7 | 0.1 ± 0.3 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.3 ± 0.7 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.1 ± 0.2 |
| Variable | p-Value Anova (Effect Size f2%) | p-Value (SBPRE vs. PLAPRE) | SBPRE | SBPOST | p-Value (SBPRE vs. SBPOST) | PLAPRE | PLAPOST | p-Value (PLAPRE vs. PLAPOST) | p-Value (SBPOST vs. PLAPOST) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Peak power (W) | WT1 | 0.6021 (0.5%) | 1.0000 | 834 ± 316 (714–954) | 903 ± 330 (777–1028) | 0.1826 | 802 ± 310 (657–947) | 837 ± 288 (702–972) | 1.0000 | 1.0000 |
| WT2 | 1.0000 | 791 ± 173 (678–903) | 886 ± 172 (769–1003) | 0.0032 | 751 ± 147 (631–870) | 801 ± 142 (676–927) | 1.0000 | 1.0000 | ||
| Average power (W) | WT1 | 0.0862 (2.6%) | 1.0000 | 548 ± 102 (482–613) | 553 ± 108 (487–618) | 1.0000 | 526 ± 80 (457–595) | 530 ± 90 (464–596) | 1.0000 | 1.0000 |
| WT2 | 1.0000 | 517 ± 296 (452–582) | 543 ± 309 (479–607) | 0.0097 | 507 ± 255 (440–574) | 511 ± 268 (444–579) | 1.0000 | 1.0000 | ||
| Minimum power (W) | WT1 | 0.3575 (1.1%) | 1.0000 | 336 ± 171 (297–375) | 327 ± 168 (286–368) | 1.0000 | 319 ± 143 (282–357) | 307 ± 144 (265–349) | 1.0000 | 1.0000 |
| WT2 | 1.0000 | 297 ± 97 (260–334) | 298 ± 110 (256–340) | 1.0000 | 301 ± 87 (261–342) | 290 ± 85 (250–330) | 1.0000 | 1.0000 |
| p-Value Anova (Effect Size f2%) | p-Value (SBPRE vs. PLAPRE) | SBPRE | SBPOST | p-Value (SBPRE vs. SBPOST) | PLAPRE | PLAPOST | p-Value (PLAPRE vs. PLAPOST) | p-Value (SBPOST vs. PLAPOST) | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Glucose (mg∙dL−1) | Pre-exercise | 0.4848 (0.7%) | 1.0000 | 118.3 ± 16.6 (110.3–125.9) | 102.6 ± 20.5 (96.3–115.5) | 0.1060 | 124.2 ± 19.9 (114.9–133.6) | 113.0 ± 14.9 (106.0–119.9) | 1.0000 | 1.0000 |
| Post-exercise | 1.0000 | 139.3 ± 24.0 (125.6–146.9) | 130.9 ± 25.7 (109.1–133.8) | 1.0000 | 135.0 ± 24.1 (123.7–146.3) | 131.4 ± 22.5 (120.9–142.0) | 1.0000 | 1.0000 | ||
| Lactate (mmol∙L−1) | Pre-exercise | 0.2044 (1.4%) | 1.0000 | 1.56 ± 0.42 (1.40–1.73) | 1.51 ± 0.40 (1.30–1.75) | 1.0000 | 1.68 ± 0.46 (1.56–2.40) | 1.67 ± 0.57 (1.44–2.19) | 1.0000 | 1.0000 |
| Post-exercise | 1.0000 | 16.37 ± 2.25 (15.57–17.62) | 16.82 ± 2.82 (13.72–16.98) | 1.0000 | 15.98 ± 2.73 (14.58–17.19) | 15.77 ± 2.65 (14.12–17.02) | 1.0000 | 1.0000 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Durkalec-Michalski, K.; Zawieja, E.E.; Podgórski, T.; Zawieja, B.E.; Michałowska, P.; Łoniewski, I.; Jeszka, J. The Effect of a New Sodium Bicarbonate Loading Regimen on Anaerobic Capacity and Wrestling Performance. Nutrients 2018, 10, 697. https://doi.org/10.3390/nu10060697
Durkalec-Michalski K, Zawieja EE, Podgórski T, Zawieja BE, Michałowska P, Łoniewski I, Jeszka J. The Effect of a New Sodium Bicarbonate Loading Regimen on Anaerobic Capacity and Wrestling Performance. Nutrients. 2018; 10(6):697. https://doi.org/10.3390/nu10060697
Chicago/Turabian StyleDurkalec-Michalski, Krzysztof, Emilia Ewa Zawieja, Tomasz Podgórski, Bogna Ewa Zawieja, Patrycja Michałowska, Igor Łoniewski, and Jan Jeszka. 2018. "The Effect of a New Sodium Bicarbonate Loading Regimen on Anaerobic Capacity and Wrestling Performance" Nutrients 10, no. 6: 697. https://doi.org/10.3390/nu10060697
APA StyleDurkalec-Michalski, K., Zawieja, E. E., Podgórski, T., Zawieja, B. E., Michałowska, P., Łoniewski, I., & Jeszka, J. (2018). The Effect of a New Sodium Bicarbonate Loading Regimen on Anaerobic Capacity and Wrestling Performance. Nutrients, 10(6), 697. https://doi.org/10.3390/nu10060697