Abstract
Intravenous lipid emulsions (ILEs) have been an integral component of parenteral nutrition for more than 50 years. Numerous formulations are available and are based on vegetable (soybean, olive, coconut) and animal (fish) oils. Therefore, each of these formulations has a unique fatty acid composition that offers both benefits and limitations. As clinical experience and our understanding of the effects of fatty acids on various physiological processes has grown, there is evidence to suggest that some ILEs may have benefits compared with others. Current evidence suggests that olive oil-based ILE may preserve immune, hepatobiliary, and endothelial cell function, and may reduce lipid peroxidation and plasma lipid levels. There is good evidence from a large randomized controlled study to support a benefit of olive oil-based ILE over soybean oil-based ILE on reducing infections in critically ill patients. At present there is limited evidence to demonstrate a benefit of olive oil-based ILE over other ILEs on glucose metabolism, and few data exist to demonstrate a benefit on clinical outcomes such as hospital or intensive care unit stay, duration of mechanical ventilation, or mortality. We review the current research and clinical evidence supporting the potential positive biological and clinical aspects of olive oil-based ILE and conclude that olive oil-based ILE is well tolerated and provides effective nutritional support to various PN-requiring patient populations. Olive oil-based ILE appears to support the innate immune system, is associated with fewer infections, induces less lipid peroxidation, and is not associated with increased hepatobiliary or lipid disturbances. These data would suggest that olive oil-based ILE is a valuable option in various PN-requiring patient populations.
1. Introduction
Parenteral nutrition (PN) is recognized as an important means to provide nutrition for patients who are unable to receive sufficient oral or enteral nutrition [1]. Parenteral nutrition should include a balance between glucose, amino acids, and lipids, as well as vitamins, minerals, and trace elements, in order to meet individual nutritional needs of patients. Lipids are an integral component of PN as they are rich in calories and provide essential fatty acids [1]. Several different formulations of intravenous lipid emulsions (ILEs) are commercially available: soybean oil-based ILEs (e.g., Intralipid®); mixtures of soybean long-chain triglycerides (LCT)/coconut oil medium-chain triglycerides (MCT) (MCT/LCT; e.g., Lipofundin®); olive oil-based ILE (olive oil 80%, soybean oil 20%, e.g., ClinOleic®); and fish oil-based ILEs either as a 100% ILE (e.g., Omegaven®) that is usually mixed with another ILE at the point of care, or preformulated fish oil-based ILEs such as Smoflipid® (soybean oil 30%, MCT 30%, olive oil 25%, fish oil 15%) or Lipoplus/Lipidem® (soybean oil 40%, MCT 50%, fish oil 10%).
Olive oil-based ILE has been commercially available since the 1990s and is widely used in some settings (see Table 1 for summary). The primary fatty acid in olive oil-based ILE is the omega (n)-9 monounsaturated fatty acid (MUFA), oleic acid. MUFAs have been associated with health benefits [2,3], and diets rich in MUFAs have been associated with a lower risk of inflammatory disease [4]. Oleic acid contributes approximately 60% of the total fatty acids in the 80% olive oil-based ILE [5]. Olive oil-based ILE also includes linoleic acid, an essential omega (n)-6 polyunsaturated fatty acid (PUFA), which contributes approximately 20% of the total fatty acids in the olive oil-based ILE [5]. Olive oil-based ILE also includes the essential omega (n)-3 PUFA α-linolenic acid, which contributes approximately 2% of the total fatty acid content [5]. Concerns have emerged regarding excess n-6 PUFAs and their effects on lipid peroxidation, immune function, and inflammation [6,7,8,9,10].

Table 1.
Fatty acid composition of commercially available parenteral nutrition lipid emulsions.
This narrative review summarizes the evidence for the effects of olive oil-based ILE on immune function and lipid peroxidation in vitro, in vivo (animal and human), and in clinical studies. Additionally, the effects of olive oil-based ILE on plasma lipids and glucose metabolism, hepatobiliary and endothelial function, and morbidity and mortality in clinical trials are summarized.
2. Literature Search
2.1. Literature Search Strategy
The Medline and Embase databases (inception to 15 September 2017) were searched using the terms (parenteral nutrition or PN) AND olive AND (lipid* OR oil* OR emulsion* OR ILE OR IVLE). The search was limited to English-language articles. Animal, in vitro, and in vivo studies, as well as prospective clinical studies (randomized and observational) in adult and pediatric patients, were included. Conference abstracts, case studies, and editorials were excluded. Review articles retrieved during the literature search were hand searched to identify any further articles of relevance.
2.2. Literature Search Results
A total of 387 articles were retrieved, of which 115 were included in the review (Figure 1). Most excluded articles were deemed irrelevant, primarily because they did not discuss olive oil-based ILE.
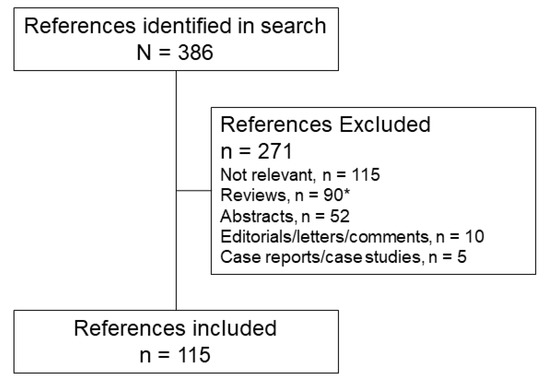
Figure 1.
Flow diagram of the articles identified and included in this review. * Bibliographies of review articles were searched by hand to identify additional relevant articles.
3. Immune Function
Parenteral nutrition is commonly administered to critically ill patients who have inflammation and/or immune dysfunction and are therefore at an increased risk of infection. Fatty acid content of the ILE used for PN may impact immune function, and therefore the risk of infection and of organ damage arising from inflammation. Metabolism of n-6 PUFAs and n-3 PUFAs contributes to the formation of inflammatory mediators such as prostaglandins, leukotrienes, and resolvins (Figure 2), and some of these inflammatory mediators may play a role in increasing inflammation. Lipid emulsions containing high levels of n-6 PUFAs, such as soybean oil, have been reported to suppress the immune system [7], increase inflammation [8,9,10], and may be associated with higher rates of infection [20] compared with other ILEs. In contrast, lipid emulsions containing olive oil, which is high in the n-9 MUFA oleic acid, may preserve immune function [21].

Figure 2.
Metabolic pathways of n-3 and n-6 fatty acids. Adapted from [30], Copyright 2009, with permission from Elsevier.
3.1. Immune Response
Collective evidence from animal studies, in vitro cultured immune cell studies, and clinical studies suggests that olive oil-based ILE appears to preserve immune function (Table 2). Some studies have reported that olive oil-based ILE has no effect or beneficial effects on immune cell proliferation and function and/or immune cell death [7,22,23,24,25,26,27], as well as lesser effects on disruption of bacterial clearing [28,29] compared with other ILEs. Numerous studies have reported that oleic acid has direct effects on both the innate and adaptive immune systems (see review by Carillo et al., 2012) [4]. These include effects on the expression of cellular adhesion molecules, neutrophil aggregation, neutrophil phagocytic activity, neutrophil reactive oxygen species (ROS) production, leukocyte migration, T-cell proliferation, and lymphocyte apoptosis [4].
Table 2.
Effects of olive oil-based intravenous lipid emulsions on inflammation, immune function, and infections.
Analysis of the effects of olive oil-based ILE on isolated human lymphocytes and neutrophils revealed that olive oil-based ILE decreased lymphocyte proliferation, induced lymphocyte necrosis, and did not alter the proportion of viable neutrophils [22]. When these results were compared with a previous study by the same group using soybean oil-based ILE, olive oil-based ILE was less toxic to lymphocytes, increased ROS production by neutrophils, and did not affect neutrophil viability compared with soybean oil-based ILE [22,47]. Similar findings were reported in another study of isolated human immune cells, where olive oil-based ILE had no effect on lymphocyte proliferation, while soybean oil-based ILE inhibited lymphocyte proliferation [23]. With regard to immune cell function, one study reported that olive oil-based ILE did not significantly affect neutrophil function, including intracellular calcium or elastase release, oxidative burst, chemotaxis, adhesion molecule or leukotriene generation, and phagocytic activity [7]. Another study reported that both olive oil-based and soybean oil-based ILEs induced a significant increase in hydrogen peroxide production (respiratory burst) by neutrophils compared with incubation with no ILE or with MCT/LCT ILE [25]. Respiratory burst is a critical component of the killing function of neutrophils; thus, this study demonstrates that olive oil-based ILE does not appear to diminish neutrophil function. Although it is not clear that olive oil-based ILE improves immune function, the evidence available from in vitro and in vivo studies suggests that olive oil-based ILE preserves existing immune function.
In rats, ILEs have been shown to disrupt bacterial clearing by mononuclear phagocytes [28]. Compared with soybean oil-based ILE and MCT/LCT-based ILE, olive oil-based ILE resulted in less disruption of bacterial clearing despite there being no difference between groups in prostaglandin E2 plasma levels [28]. Compared with fish oil-based ILE, structured lipids, MCT/LCT, and soybean oil-based ILE, olive oil-based ILE was the least likely to impair the pneumococcal elimination capacity of isolated human neutrophils [28]. In mouse models of inflammation (trauma-induced cremaster muscle inflammation and lipopolysaccharide-induced inflammation) and lethal endotoxemia, olive oil-based ILE blocked leukocyte recruitment (most likely through modulation of adhesion molecules) and increased survival compared with soybean oil-based ILE and fish oil-based ILE formulations [27].
In a study comparing the effects of olive oil-based ILE to soybean oil-based ILE on leukocyte counts in critically ill adults, olive oil-based ILE was associated with an increase from baseline in leukocyte count, whereas soybean oil-based ILE was associated with a decrease from baseline in leukocyte count [26]. The exact mechanism for this effect was not clear; however, it may be possible that the soybean oil-based ILE suppressed the inflammatory response. Not all studies have reported a difference between olive oil-based ILE and soybean oil-based ILE. Two studies, one in healthy adults and the other in surgical intensive care unit (ICU) patients, reported no significant differences in granulocyte phagocytosis, monocyte phagocytosis, granulocyte ROS generation, and monocyte ROS between the olive oil-based ILE and soybean oil-based ILE groups [24,40]. Similar findings were reported in adult patients in the surgical ICU [40]. Importantly, it cannot be ruled out that the differences between these studies may reflect differences between the immune systems of the subjects (i.e., critically ill patients vs. healthy adults).
3.2. Inflammation
Compared with other ILEs, there is limited and conflicting evidence to support the benefits of olive oil-based ILE on inflammatory marker profiles. In vitro studies using isolated human peripheral blood mononuclear cells (PBMCs) or polymorphonuclear cells (PMNs) from healthy volunteers revealed that olive oil-based ILE appeared to be more neutral in its effects on inflammatory eicosanoid or cytokine production compared with soybean oil-based, MCT/LCT, or fish oil-based ILEs [7,31,32]. Olive oil-based ILE was not associated with increases in leukotriene B4 or prostaglandin-E2 production [7,31], or with suppression of tumor necrosis factor α (TNFα), interleukin (IL)-1β, or IL-8 [7,32] levels. These properties of olive oil-based ILE may be advantageous in patients where immune suppression may be detrimental (e.g., ICU patients) [39].
3.2.1. Inflammation Marker Profiles in Adult Clinical Studies
Most adult clinical studies were small and have reported no significant differences between the effects of olive oil and other ILEs on inflammatory marker profiles. In healthy adults, no differences between OO, SO, lipid-free PN, and saline were noted for TNFα, IL-6, or C-reactive protein (CRP).
In surgical patients, most studies have not reported differences in inflammatory marker profiles between ILEs. In a recent study comparing soybean oil-based + MCT/LCT (75% soybean oil-based + 25% MCT/LCT) ILE, olive oil-based ILE, and olive oil + fish oil (85% olive oil-based ILE + 15% fish oil) ILE in patients with cancer who had undergone abdominal surgery, TNFα and IL-6 levels were similar between groups at baseline; however, the postoperative increases in TNFα and IL-6 were lower in the olive oil-based ILE group compared with the other groups (Figure 3) [34]. Another study in patients undergoing abdominal surgery reported no differences between groups in CRP [33]. In a study of surgical patients, there was no difference in plasma TNFα, CRP, or IL-6 levels between the olive oil-based ILE and soybean oil-based ILE groups [40]. Similar findings for CRP were reported in another study [20]. In a large randomized controlled trial of surgical patients (N = 458), olive oil was associated with a significant decrease in IL-6 levels compared with soybean oil [20]. Thus, the lack of differences noted in earlier studies may reflect a lack of statistical power.
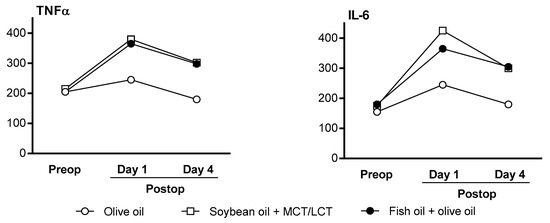
Figure 3.
TNFα and IL-6 levels in adult patients undergoing major abdominal surgery (N = 52). Reprinted from Demirer, S.; et al. Effects of postoperative parenteral nutrition with different lipid emulsions in patients undergoing major abdominal surgery. Annals Surg Treat Res 2016, 91, 309–315. CC BY 4.0 [34]. IL-6—interleukin 6; MCT/LCT—medium-chain triglycerides/long-chain triglycerides; postop—postoperative; preop—pre-operative; TNFα—tumor necrosis factor α.
In adults with severe burns receiving an olive oil-based ILE versus a MCT/LCT-based ILE, TNFα decreased significantly from baseline in the olive oil group but not in the MCT/LCT group. IL-6 and IL-10 also decreased from baseline in the olive oil group; however, the decrease was not significant [35]. No between-group differences were noted.
In a study of patients receiving long-term olive oil-based ILE, no differences in TNFα or IL-6 levels between baseline and 3 months were observed [39]. Another study of patients receiving long-term olive oil-based ILE reported that TNFα was 3.6-fold higher in patients compared with healthy controls (likely reflective of the disease), but no differences in IL-10 between groups were noted [37]. The authors also reported that no differences in leukocyte activation, adhesion molecule expression, degranulation markers, or ROS production were noted between the patient and control groups [37]. Further, another study of patients receiving long-term PN with olive oil-based ILE reported that there were no differences in CRP levels between healthy controls and those receiving PN [36].
3.2.2. Inflammation Marker Profiles in Pediatric Clinical Studies
Only one study has examined the effects of ILE on inflammatory marker profiles in pediatric patients [42]. Premature neonates (<32 weeks gestational age and <1500 g) were randomized to either an olive oil-based ILE or a soybean oil-based ILE within the first 48 h of life. Blood samples were collected at baseline and at 14 days, and the PBMCs were isolated and cultured for 48 h in medium only or in the presence of anti-CD3 antibodies. Anti-CD3-stimulated IL-6 increased significantly in the soybean oil group compared with the olive oil group [42]. TNFα and IL-10 were not different between groups.
3.3. Infections
Infections in patients receiving PN remain a significant concern. Duration of total PN has been identified as one of the strongest predictors of nosocomial infections in adult [48] and pediatric patients [49] receiving PN. Currently it remains unclear as to whether or not olive oil-based ILE is associated with lower infection rates, with small studies showing no difference between groups. However, in a large randomized controlled trial, olive oil-based ILE was clearly associated with fewer infections compared with a soybean oil-based ILE [20].
3.3.1. Infection Rates in Adult Clinical Studies
Only one study has reported the effects of ILE on sepsis rates [33]. No significant differences in sepsis rates between olive oil and olive + fish oil groups were noted; however, a significantly lower rate of infections was noted for the olive + fish oil group [33]. In the olive oil group, infection types included respiratory (n = 3), abdominal (n = 3), urinary tract (n = 4), and surgical incision (n = 1), while in the olive + fish oil group, infections included abdominal (n = 1), surgical wound (n = 1), and blood stream infection (n = 1) [33]. In several studies, no significant difference between olive oil and soybean oil groups in infection rates was noted; however, these studies were likely underpowered to detect significant differences [26,38,39,40]. In the largest study to date, Jia and colleagues reported that olive oil-based ILE was associated with a significantly lower infection rate compared with soybean oil-based ILE (Figure 4) [20].
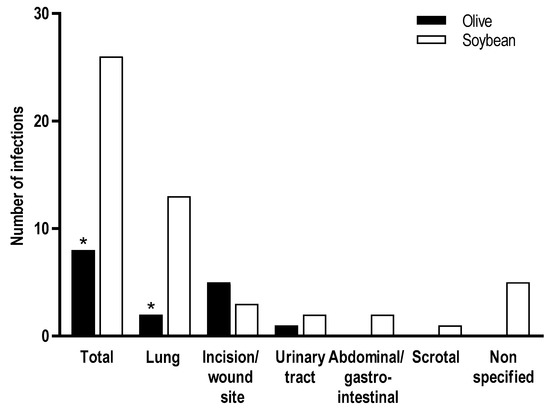
Figure 4.
Infection rates in adult surgical patients (N = 458) [20]. * p < 0.05.
3.3.2. Infection Rates in Pediatric Clinical Studies
Several studies, predominantly in preterm neonates, have reported no significant differences in sepsis rates between olive oil-based and soybean oil-based ILEs [41,43,44,45,46].
4. Lipid Peroxidation
Oxidative stress is an important mechanism that may contribute to the pathogenesis of inflammation [6]. The fatty acid composition of ILEs (saturated, monounsaturated, and polyunsaturated) results in differential lipid peroxidation; therefore, it has been proposed that ILEs that are high in saturated fatty acids or MUFAs (like olive oil) may be at lower risk of lipid peroxidation [6]. Increased numbers of double bonds, as found in PUFAs, may increase the risk of lipid peroxidation [50]. Additionally, ILEs with higher levels of α-tocopherol may also be more resistant to lipid peroxidation [51,52]. However, paradoxically, excessive/high levels of α-tocopherol may be pro-oxidant [53], thus it is important to ensure that the appropriate amount of α-tocopherol is present in the ILE. Notably, Xu and colleagues found no correlation between the amount of vitamin E present in lipid emulsions and lipid peroxidation [54]; however, the production of hydroperoxides was lowest with olive oil-based ILE and highest with 100% fish oil-based ILE [54].
Studies examining the effects of different ILEs or their main fatty acid constituents suggest that olive oil and its primary constituent, oleic acid, is associated with less lipid peroxidation compared with other ILEs (Table 3) [31,50,55,56,57]. In an in vitro study comparing the effects of fatty acids on ROS production in cultured human colonic cells, docosahexaenoic acid, an important constituent of fish oil, induced a 429% increase in ROS production compared with 6% induced by oleic acid [55]. In mice fed fatty acids (docosahexaenoic acid, oleic acid, or linoleic acid) or oils (fish, olive, or soy), fish oil and docosahexaenoic acid induced ~3-fold increases in postprandial thiobarbituric acid reactive substances (TBARS), a marker of lipid peroxidation [56]. In contrast, olive oil and oleic acid induced modest increases (~0.5-fold) in postprandial TBARS levels [56]. Furthermore, linoleic acid, the primary constituent in soybean oil, resulted in a ~2-fold increase in TBARS levels, while soybean oil induced a ~0.5-fold increase [58]. Lastly, an in vitro study using PBMCs harvested from healthy, fasted volunteers revealed that incubation with olive oil-based or soybean oil-based ILE did not significantly affect lipid peroxide production in mononuclear cells or neutrophils compared with no ILE (control) [31]. However, both Smoflipid and Omegaven induced significant increases in lipid peroxide production in mononuclear cells (2.5-fold and >5-fold, respectively) and neutrophils (2.5-fold and >5-fold, respectively) compared with control [31].
Table 3.
Effects of olive oil-based intravenous lipid emulsions on lipid peroxidation.
In contrast, numerous clinical studies have investigated markers of oxidative stress including total antioxidant status (TAS), total antioxidant capacity, TBARS, F2-isoprostane, vitamin Eα-tocopherol levels, pentane, or malondialdehyde (MDA). Most studies have reported no differences in oxidative stress markers between olive oil-based and soybean oil-based [20,38,40,43,59,60,61], MCT/LCT [60,62,63], or fish oil-based [64,65] ILE (Table 3). Furthermore, a systematic review of studies in hospitalized pediatric patients suggested that available studies do not support one ILE over another with regard to benefits on oxidative stress [66].
In adult patients after abdominal surgery, TBARS were significantly lower in the olive oil group compared with MCT/LCT + LCT and olive oil + fish oil groups, an effect that was maintained after adjusting for multiplicity [34]. In adults receiving long-term PN with an olive oil-based ILE, malondialdehyde levels did not increase from baseline to 3 months, suggesting that long-term exposure to olive oil-based ILE does not increase oxidative stress [39]. Similarly, another study reported that although adult patients receiving long-term PN with an olive oil-based ILE had increases in oxidized glutathione compared with healthy control subjects, no differences between groups were noted for lipid peroxidation markers and protein carbonyls [36]. Similarly, in children requiring long-term PN, olive oil-based ILE was associated with significantly lower peroxidation products compared with soybean oil-based ILE [51].
5. Metabolic Effects
5.1. Lipid Metabolism
Administration of PN is associated with increases in plasma cholesterol and triglyceride levels [67]. In the short-term, this transient increase in serum lipid parameters is of less concern than for patients receiving long-term PN. There is evidence to suggest that olive oil-based ILE may have beneficial effects on cholesterol levels, whereas the relationship between olive oil-based ILE and serum triglyceride levels is less clear (Table 4). In guinea pigs, chronic administration of ILEs (10 days) resulted in increased triglyceride levels; however, the levels were significantly lower in soybean oil-based, olive oil-based, and 100% fish oil ILE groups compared with Smoflipid or control (diet) groups [5]. Furthermore, small clinical studies in pediatric and adult populations have shown that olive oil-based ILEs are safe and have limited effects on lipid profiles when used for long-term PN [39,51].
Table 4.
Effects of olive oil-based intravenous lipid emulsions on plasma cholesterol and triglyceride levels.
Notably, most studies failed to report the normal reference ranges for lipid markers; however, using the National Cholesterol Education Program Adult Treatment Panel (NCEP-ATP) as a general guide (fasted state), most lipid profiles remained within normal ranges [68]. However, it should be noted that lipid levels measured in patients receiving PN represent the “fed” and not “fasting” state. Therefore, increases in lipid levels above the NCEP-ATP ranges may not represent a true elevation in lipid levels.
5.1.1. Plasma Lipid Levels in Adult Clinical Studies
In healthy adults, plasma triglyceride levels increased significantly in both the olive oil-based and soybean oil-based groups compared with the lipid-free PN and saline treatment groups [24]. In contrast, no differences between treatment groups were noted for total cholesterol (TC), high-density lipoprotein (HDL), or low-density lipoprotein (LDL) between the groups [24]. Despite these significant differences, all plasma lipid values remained largely within normal ranges (fasted state). In this particular study, it should also be noted that the no lipid and saline groups would represent a fasted state; and therefore, comparisons between the ILE groups (fed state) and the no lipid and saline groups (fasted state) should take this into consideration.
In adult patients with severe burns, TC levels increased significantly in response to olive oil-based ILE but remained within the normal range [35]. Triglyceride levels also increased significantly in response to both olive oil-based and soybean oil-based ILEs, exceeding the normal range, with no between-group differences noted.
In adult patients with sepsis or septic shock, both TC and triglyceride levels remained within the normal range after administration of olive oil-based ILE [69]. Further, in adult trauma patients, triglyceride levels were not different between patients receiving olive oil-based ILE and patients receiving no lipid or soybean-based ILE [70].
In adult patients after abdominal surgery, one study reported that in the olive oil group, TC, HDL, LDL, and very low-density lipoprotein (VLDL) levels decreased from baseline, while in the soybean oil group these same parameters increased, with no significant differences between olive oil-based and soybean oil-based ILEs [38]. Another study reported no change from baseline in TC, HDL, LDL, or triglyceride levels after administration of olive oil-based ILE [71]. All lipid levels remained within the normal range [71]. In contrast, another study reported that triglyceride levels increased significantly in both the olive oil-based and fish oil-based ILE groups [72]. Triglyceride levels were higher in the olive oil group and exceeded the normal ranges by Day 2, and the difference between groups was significant [72].
Lastly, in studies of malnourished adult patients, fewer patients receiving olive oil-based ILE experienced deterioration of triglyceride levels compared with patients receiving soybean oil-based ILE [73]. Deterioration was defined as a patient who moved to a more abnormal category after starting PN (categories: within normal limits, elevation up to 2 × upper limit of normal [ULN], and elevation > 2 × ULN), while in adult patients receiving long-term PN, no changes from baseline in TC, HDL, LDL, or triglyceride levels after administration of olive oil-based ILE were noted [36,39].
5.1.2. Plasma Lipid Levels in Pediatric Studies
In children receiving long-term (mean 34 months) PN, olive oil-based ILE was associated with reductions in TC, HDL, LDL, and triglycerides compared with soybean oil, which increased these lipid levels [51]. The differences between groups were significant for TC and LDL. In children with intestinal failure, TC remained within normal limits after administration of olive oil ILE [75].
In preterm neonates, one study reported that olive oil and MCT/LCT were associated with significant increases in triglyceride levels [63]; however, the levels remained within the normal range. Another study reported that olive oil-based ILE maintained HDL levels compared with MCT/LCT; nevertheless, LDL levels were significantly higher for olive oil-based than for soybean oil-based or MCT/LCT ILEs [46]. A third study reported no significant differences in triglycerides, TC, HDL, or LDL between olive oil-based and soybean oil-based ILE; however, VLDL levels were significantly lower in the olive oil-based ILE group [41]. All levels were within normal ranges. Lastly, a fourth study reported no significant differences between olive oil-based ILE and soybean oil-based ILE for TC and triglycerides, and all levels were within normal ranges [43]. Investigation of the metabolism of fatty acids to acylcarnitines indicated that free carnitine, hexanoyl carnitine, and medium-chain fatty acid carnitine levels were significantly lower in the olive oil-based ILE group compared with the soybean oil-based ILE group [41]. These findings suggest that soybean oil-based ILE may impair intramitochondrial metabolism of fatty acids.
5.2. Glucose Metabolism
Disturbances of glucose metabolism are common in critically ill patients receiving PN, and this reflects both the dextrose load and possibly the fatty acid composition of the ILE. However, few studies have investigated the direct effects of ILE on glucose metabolism. In normal healthy adults, significant increases in plasma glucose, insulin, and C-peptide were observed after infusion of lipid-free PN, olive oil-based ILE, and soybean oil-based ILE compared with infusion of saline [24]. No significant differences between the lipid-free, olive oil-based ILE, and soybean oil-based ILE groups were noted. These results would suggest that the changes in glucose metabolism likely reflect the dextrose load rather than specific effects of the ILE. In contrast, in preterm infants, soybean oil-based ILE significantly increased gluconeogenesis and glucose production and significantly decreased glycogenolysis compared with glucose, glycerol, and olive oil-based ILE [76]. Olive oil-based ILE did not significantly affect any of these measures. Furthermore, the lack of effect of glycerol on these measures suggests that the fatty acids contained in soybean oil-based ILE may play a role in regulating these processes. The authors suggested that the differences between the ILEs may be useful clinically in that soybean oil-based ILE may be valuable in treating/preventing the hypoglycemia observed during the first few days after birth, while olive oil-based ILE may be beneficial in preventing/treating hyperglycemia [76].
5.3. Emerging Issues Associated with the Fatty Acid Composition of ILEs
The unique fatty acid compositions of different ILEs impact fatty acid metabolism and as a result may have unintended consequences. As shown in Figure 2, metabolism of fatty acids relies on a few key enzymes, and therefore competition between the fatty acids for these enzymes can impact the fatty acids available for key physiological processes. In preterm neonates, who have no or limited stores of fatty acids, this may be a significant issue as docosahexaenoic acid and arachidonic acid are important for normal brain development. Supplementation with docosahexaenoic acid downregulates the production of both arachidonic acid and docosahexaenoic acid [77,78], and there is evidence to suggest that the ratio of docosahexaenoic acid to arachidonic acid is a key determinant of ensuring adequate supply of both fatty acids [78,79]. Similar to the ratio in breast milk, the appropriate ratio in enteral formulations is approximately 1:2 (docosahexaenoic:arachidonic acid) [78,79]. More recently it has been shown that fish oil-based ILEs (docosahexaenoic:arachidonic acid ratio 1:1) may cause increased rates of retinopathy of prematurity (ROP) compared with olive oil-based ILE (docosahexaenoic:arachidonic acid ratio 1:1.7) [80]. Further studies are needed to elucidate the optimal ratio and concentration of fatty acids in ILE utilized in the preterm neonate population.
In the past 40 years, PN has been infrequently linked to the development of essential fatty acid deficiency (EFAD) and, in the setting of malnutrition, EFAD can occur quickly owing to the lack of essential fatty acid stores. Essential fatty acids are found in high levels in soybean oil, and thus the use of soybean oil-based ILE has been effective in preventing EFAD. With the advent of newer ILEs, such as olive oil-based and fish oil-based ILEs, the potential for EFAD has increased.
Olthof and colleagues recently published their findings regarding the use of an olive oil-based ILE in patients requiring long-term PN [37]. The study reported that there was no clinical or biochemical evidence of EFAD in patients who had received olive oil-based ILE at least 5 times per week for a period of at least 3 months [37]. The results of this study confirm that, if used daily at the recommended lipid dose, olive oil-based ILE provides sufficient essential fatty acids to prevent EFAD; however, in patients who are receiving lower than recommended doses, e.g., twice-weekly infusions instead of daily, patients may be at risk of EFAD.
6. Liver Function
Liver function in patients receiving PN remains a clinical concern for physicians [81,82,83]. Some patients receiving PN may develop liver dysfunction characterized by steatosis and cholestasis. This liver disease is referred to as PN-associated liver disease (PNALD) or intestinal failure-associated liver disease (IFALD) and may progress to steatohepatitis (nonalcoholic-associated steatohepatitis [NASH]), cirrhosis, and liver failure. The etiology of liver dysfunction remains elusive; however, several mechanisms have been proposed [5,44,84,85]:
- Impaired hepatic secretion of fatty acids and triglycerides as VLDL
- Increased synthesis of hepatic triglycerides due to increased intake of n-6 PUFAs and low intake of n-3 PUFAs
- Impaired hepatobiliary secretion leading to cholestasis, possibly resulting from phytosterols present in lipid emulsions and competition of transport owing to differences in phytosterol content
- Impaired hepatobiliary function due to endotoxin entry into the portal circulation or sepsis
- Modulation of oxidative stress and inflammation by peroxidation of PUFAs, increased intake of n-6 PUFAs, and differences in α-tocopherol content
- Lack of enteral nutrition and enteral-stimulated gut growth factors, which may in turn lead to alterations in the gut microbiome.
Although liver disease can occur in adults, children and especially infants are most at risk of developing cholestasis and overt liver disease [82]. The increased risk of IFALD in infants may result from the immature liver development/function along with the use of PN incorporating high lipid doses. In infants, risk factors for IFALD relate to both patient characteristics and management of the intestinal failure. Patient-dependent risk factors include age, degree of liver maturation (prematurity), cause of intestinal failure, site and frequency of infection (gastrointestinal tract, central venous catheter), small-bowel bacterial overgrowth, and enteral feed tolerance [86]. Treatment-related risk factors include the composition of PN [86], its mode of administration (continuous/cyclical) [86], the duration of PN dependency [57,86], the surgical interventions and their anatomical consequences (intestinal obstruction, disruption of the enterohepatic circulation, resection of the terminal ileum or the ileocecal valve) [86], and the use of antibiotics (liver/renal toxicity) [86]. Imbalance (deficiency/excess) of parenteral nutrients has also been implicated in IFALD, and almost all of the components may be possible causative or aggravating agents [86].
We identified 24 studies [20,33,35,38,39,41,43,44,45,46,51,61,64,71,72,73,75,85,87,88,89,90,91,92,93] and three meta-analyses [66,81,83] that investigated the effects of olive oil-based ILE on liver function (Table 5). Findings have varied across studies, and no clear pattern of effect of olive oil-based ILE on markers of liver function (sometimes called liver function tests) such as alanine aminotransferase (ALT), aspartate aminotransferase (AST), and bilirubin (total or conjugated) or on biliary tract function markers such as alkaline phosphatase (ALP) and gamma-glutamyl transpeptidase (GGT) have been discerned. Importantly, while statistically significant differences between olive oil-based ILE and other ILEs were noted in many studies (Table 5), the majority of studies reported hepatobiliary functional marker levels that were within the normal ranges or within 1.5 × ULN [94]. Slight elevations (up to 1.5 × ULN) do not necessarily indicate the presence of liver disease [94]. Thus, these statistically significant differences between ILEs need to be interpreted with caution as they may not be clinically important. Most studies in adults, preterm neonates, and children suggest that olive oil-based ILE is safe and not associated with adverse effects on hepatobiliary function.
Table 5.
Effects of olive oil-based intravenous lipid emulsions on markers of liver function.
6.1. Hepatobiliary Function in Adult Studies
Most studies of adult patients have demonstrated that, in general, olive oil-based ILE is not associated with adverse effects on the hepatobiliary system. In adults post-abdominal surgery, four small studies reported that ALP, AST, and ALT levels remained or decreased to normal ranges (or less than 1.5 × ULN), suggesting that olive oil-based ILE preserved liver function in these patients [33,38,71,72]. Two of three studies reported that GGT was within the normal range (or less than 1.5 × ULN) [33,38], while the third study reported that although GGT levels were higher than the normal range, they did not change from baseline [71], i.e., olive oil-based ILE did not worsen pre-existing biliary dysfunction. Of two studies reporting on total bilirubin, one reported that olive oil-based ILE significantly decreased total bilirubin levels from baseline, whereas the other reported no change; however, the levels were within normal limits [38,71]. Similar findings for liver function tests have been reported for severely malnourished adult patients [73], adult patients receiving long-term PN [39,90], adult patients with esophageal cancer [92], and adult patients with severe burns [35].
In another study of adult patients receiving PN for longer than 6 months, transitioning patients from soybean oil-based ILE to olive oil-based ILE did not result in changes to biliary outflow efficiency, and imaging revealed no abnormalities at baseline or at the end of the study [90].
In the largest study to date (n = 458), adult surgical patients were randomized to either olive oil-based ILE (n = 226) or soybean oil-based ILE (n = 232) for a minimum of 5 and a maximum of 14 days [20]. In this large randomized controlled trial, liver enzymes were generally within normal limits (Figure 5). No incidences of clinically relevant liver disease were observed and no lipid dose reductions were required [20].
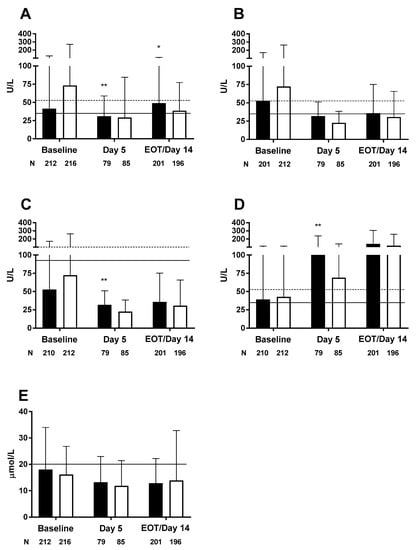
Figure 5.
Liver enzymes in adult surgical patients; (A) alanine aminotransferase, (B) aspartate aminotransferase, (C) alkaline phosphatase, (D) gamma-glutamyl transpeptidase, and (E) total bilirubin. Black bars denote olive oil-based ILE, white bars denote soybean oil-based ILE, solid horizontal line denotes upper limit of normal range, dotted horizontal line denotes 1.5 × ULN. Values up to 1.5 × ULN are not considered clinically meaningful [20]. * p < 0.05, ** p < 0.005. EOT—end of therapy; ILE—intravenous lipid emulsion; ULN—upper limit of normal range.
Most recently, a study of adult patients receiving PN for >12 months due to intestinal failure reported that olive oil-based ILE significantly reduced bilirubin levels compared with soybean oil-based, MCT/LCT, and fish oil-based ILE [93]. No differences between the soybean oil-based, MCT/LCT, or fish oil-based ILE were observed for any marker of hepatobiliary function [93].
Few studies have directly compared the effects of olive oil-based ILE with fish oil-based ILE; of those that have, most reported no significant differences between groups in most LFT results [33,44,64]. Only one study reported significant differences in LFTs between olive oil-based and fish oil-based ILE; however, levels in both groups were within the normal range [74]. Additionally, long-term PN (1 year) with olive oil-based ILE significantly reduced bilirubin and GGT levels [93]. In contrast, fish oil-based ILE had no effect on bilirubin or any other LFTs [93].
6.2. Hepatobiliary Function in Pediatric Studies
In preterm neonates, most studies have reported no adverse effects of olive oil-based ILE on liver function. Most studies reported that conjugated bilirubin, currently the best marker of cholestasis, was within the normal range [41,43,44,45,46,64,87].
One study reported that conjugated bilirubin levels were substantially above the normal range in preterm neonates (<30 weeks gestational age) [64]. Notably, no differences between groups were observed at Day 8 (olive: 6.85 ± 5.12 µmol/L vs. fish: 5.53 ± 3.04 µmol/L) [64]. ALT and AST were within the normal range in all studies that assessed these liver enzymes [43,44,45,46,61,64,87]. In contrast, ALP and GGT were well above the normal range after PN administration in all but one study [44] that assessed these biliary tract function markers [43,45,46,64,87].
In children aged greater than 1 year, olive oil-based ILE has not been associated with adverse effects on liver function. In children undergoing bone marrow transplantation, small elevations in ALT, AST, ALP, and GGT were reported; however, none of the changes were statistically significant and values were within normal ranges [62]. Total bilirubin decreased slightly from baseline; however, this effect was not statistically significant. In children with intestinal failure who were stabilized on long-term PN, liver function tests remained within normal ranges (or within 1.5 × ULN); however, liver biopsies revealed some degree of fibrosis in five of eight patients [75].
Another study of children receiving long-term PN (with olive oil-based ILE or soybean oil-based ILE) reported that liver enzymes increased from baseline to Day 60; ALP and total bilirubin levels were substantially greater than normal, while ALT, AST, and GGT were within normal or 1.5 × ULN [51].
Lastly, meta-analyses and systematic literature reviews have reported that there is no evidence to suggest that there are benefits of one lipid emulsion over another in terms of effects on liver enzymes or total bilirubin [66,81,83].
7. Endothelial Function
Endothelial cells play a critical and multifunctional role in the maintenance of vascular function, including necessary actions such as preserving vascular tone, blood fluidity, and vascular permeability [95,96]. Endothelial cells also regulate inflammatory responses as well as modulating hemostasis/thrombosis, fibrinolysis, and angiogenesis [97]. Endothelial cells are critical to an effective immune response as they regulate the migration of leukocytes and their transition from the blood to the site(s) of infection [98]. In the setting of cardiovascular disease as well as metabolic disorders, significant research has demonstrated that free fatty acids may directly contribute to endothelial dysfunction [97]. In the setting of PN, this may have important implications for patients who are already hyperinflamed or immunocompromised.
There is limited evidence to suggest that ILEs may exert direct effects on endothelial function [52,99,100,101]. In porcine coronary artery rings, soybean oil-based and olive oil-based ILEs did not reduce bradykinin-induced relaxation of endothelial cells, while MCT/LCT and Smoflipid did [101]. In normotensive, healthy adults, soybean oil-based ILE induced a rapid and sustained increase in blood pressure and decreased endothelial function compared with olive oil-based ILE and lipid-free ILE [24]. Infusion of olive oil-based ILE did not alter flow-mediated dilatation, while infusion of soybean oil-based ILE significantly decreased flow-mediated dilatation from baseline to 4 h and 24 h [24].
In cultured human aortic endothelial cells, the effects of different ILEs on fatty acid uptake and incorporation, integrity, and inflammatory activation varied depending on the ILE used [102]. Fatty acid uptake by endothelial cells was shown to be dose dependent and was lowest in the soybean oil-based ILE group and highest in the olive oil-based ILE group. Regarding endothelial cell apoptosis/necrosis, olive oil-based ILE increased endothelial cell viability, fish oil-based ILE reduced cell viability, and soybean oil-based ILE had no effect. The effect of ILEs on the proinflammatory response in endothelial cells was assessed by their effect on lipopolysaccharide-induced surface expression of intracellular adhesion molecule-1. Although all three ILEs suppressed the endothelial cell inflammatory response, the fish oil-based ILE may be the most potent, and its inhibitory effects were consistent with other studies using fish oil-based ILEs and omega-3 fatty acids [102].
Transmigration of leukocytes from the blood to infected/inflamed tissues is regulated by the endothelial cells through the expression of cytokines and adhesion molecules [103]. An in vitro/in vivo study investigating the effects of olive oil-based, soybean oil-based, and MCT/LCT ILEs revealed that only the olive oil-based ILE preserved adhesion and emigration of leukocytes, thereby maintaining transmigration, compared with soybean oil-based and MCT/LCT ILEs (Figure 6) [7].
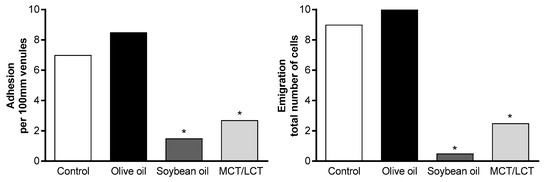
Figure 6.
Adhesion and emigration of LPS-induced leukocytes in a rat model. Reprinted from Demirer, S.; et al. Effects of postoperative parenteral nutrition with different lipid emulsions in patients undergoing major abdominal surgery. Annals Surg Treat Res 2016, 91, 309–315. CC BY 4.0. * p < 0.05. LPS—lipopolysaccharide; MCT/LCT—medium-chain triglycerides/long-chain triglycerides.
8. Clinical Outcomes
The goal of PN is to provide nutrition to patients who would otherwise not receive their daily calories and nutrients. In addition to their effects on cellular, metabolic, and liver function markers, some studies have evaluated the effects of ILEs on morbidity and mortality. Currently there is limited evidence that olive oil-based ILE offers any significant benefit over other ILEs on morbidity or mortality outcomes. However, it should also be noted that other, newer ILEs such as those containing fish oil also have not been shown to consistently confer benefits on these important outcomes [104,105].
In most studies of adult patients, no differences between ILEs were reported for mortality, length of hospital stay, length of ICU stay, termination of mechanical ventilation, or duration of mechanical ventilation [33,40,69,106]. However, one study did report a significant benefit of olive oil-based ILE on length of ICU stay and duration of mechanical ventilation compared with patients receiving no ILE [70]. A meta-analysis reported that olive oil-based ILE was not associated with significant reductions in mortality or length of ICU stay compared with soybean oil-based or MCT/LCT ILEs [107]. In contrast, olive oil-based ILE was found to significantly reduce the duration of mechanical ventilation (risk ratio −6.47; 95% confidence interval −11.41, −1.53; p = 0.01) compared with soybean oil-based or MCT/LCT ILEs [107]. The findings from this meta-analysis should be interpreted with caution as they are based on the results of only two studies.
In pediatric patients, the evidence is less clear, with conflicting results across studies. One study of preterm, very low birth weight neonates (<1500 g) reported no differences between olive oil-based and soybean oil-based ILEs in duration of mechanical ventilation, bronchopulmonary dysplasia, necrotizing enterocolitis, or retinopathy of prematurity [42]. Another study of preterm neonates (≤34 weeks) reported a significant benefit of olive oil-based ILE compared with soybean oil-based ILE on bronchopulmonary dysplasia and duration of mechanical ventilation [43]. In a study of preterm very low birth weight (<1250 g) neonates, the combination of olive oil-based ILE plus fish oil (50% + 50%) was associated with a significant reduction in the incidence of ROP that required laser therapy compared with olive oil-based ILE alone; however, there was no difference between treatment groups in ROP grades 1–3, bronchopulmonary dysplasia, necrotizing enterocolitis, sepsis, or length of hospitalization [108]. Lastly, one study of preterm, very low birth weight neonates (500–1249 g) compared five different ILEs [44]. No statistically significant differences between groups (soybean oil-based, olive oil-based, MCT/LCT, MCT/LCT + soybean oil + fish oil, or Smoflipid ILEs) for bronchopulmonary dysplasia, necrotizing enterocolitis, sepsis, or patent ductus arteriosus were observed [44].
9. Stability
The physicochemical stability of PN solutions is an important consideration as destabilization can lead to catastrophic consequences such as pulmonary emboli. Physical destabilization of a PN solution includes the formation of precipitates as well as an increase in fat globule size to greater than the industry-established 5 micron limit [109]. Physical instability occurs due to the loss of the net negative charge upon the lipid droplets. This primarily results from the introduction of positively charged cations in the form of electrolytes, minerals, or amino acids [110].
The United States Pharmacopeia sets the maximum percentage of fat globules greater than 5 microns (PFAT5) as 0.05% for ILEs, and all commercially available ILEs must meet this standard at the time of manufacture. However, the PFAT5 can increase above the industry standard during the standard hang time of 24 h [111]. Importantly, destabilization of the PN solution cannot be determined in most cases by visual inspection [112].
Several studies have reported that olive oil-based ILE better maintains its physicochemical stability compared with other currently available ILEs [111,113]. Compared with three soybean oil-based ILEs, olive oil-based ILE had the smallest globule size distribution, with the least variation in size between globules [2]. Another study showed that the physicochemical stability deteriorated substantially over time for soybean and soybean/safflower oils compared with MCT/LCT and olive oil-based ILEs [111].
More recently, there has been the development of multi-chamber bag (MCB) formulations of PN that combine dextrose, amino acids, and lipids that allow the mixing of the constituents at the time of use. The benefits of MCBs include the potential for reduced risk of infections occurring during compounding as well as ease of use [20,114]. Furthermore, the use of MCBs eliminates the risk of precipitation or destabilization of the PN solution, which can occur when Y-site administration is used [115]. The stability of the ILE in MCBs was assessed and revealed that no fat particles over 5 microns were observed for either olive oil-based or soybean oil-based ILE [113]. Notably, the tendency for separation of large diameter droplets in the two emulsion systems was different, with the large droplets being located at the top of the bag in the olive oil-based ILE and at the bottom of the bag in the soybean oil-based ILE independent of the calcium content of the PN admixtures. This observation may have important clinical implications, as the large droplets at the top of the bags are less likely to be infused than those at the bottom of the bag. The difference between the two types of PN mixtures could be partly explained by the different glucose content and its effect on the osmolarity, and by the slightly different density of the two emulsions. Another study investigated the stability of a fish oil-containing ILE (Smoflipid) in MCBs and reported that PFAT5 values of all the tested samples were below the USP-specified limits (0.05%) [116]. This was consistent across all study conditions (12 months of storage at 25 or 30 °C, or 6 months of storage at 40 °C) and the maximum value never exceeded 0.016% [116].
10. Conclusions
Olive oil-based ILE has been available for clinical use for over 20 years and during that time has proven to be effective at meeting the nutritional needs (including energy and essential fatty acid requirements) of, as well as being well tolerated in, numerous PN-requiring populations. There is evidence to suggest that olive oil-based ILE preserves immune function by supporting the innate immune system, and this is borne out by the lower infection rates seen in a large randomized controlled trial in critically ill patients [20]. Similarly, olive oil-based ILE appears to result in less lipid peroxidation compared with soybean oil-based ILEs, most likely due to its high MUFA and low PUFA content. In most studies, olive oil-based ILE maintained hepatobiliary marker and plasma lipid levels within normal or near normal ranges, and in patients receiving long-term PN, olive oil-based ILE was not associated with increased hepatobiliary or lipid disturbances. No clear differentiation between ILE formulations has been observed for sepsis rates, morbidity, mortality, or for prevention of liver damage. These data would suggest that olive oil-based ILE is a valuable option in various PN-requiring patient populations.
Author Contributions
All authors contributed equally to the drafting, critical revision, and approval of the final version of the manuscript.
Funding
Medical writing assistance was provided by Tania Dickson, PhD, CMPP and Rebecca Lew, PhD, CMPP of ProScribe—Envision Pharma Group, and was funded by Baxter Healthcare Corporation. ProScribe’s services complied with international guidelines for Good Publication Practice (GPP3).
Acknowledgments
Baxter Healthcare Corporation was involved in the preparation of the manuscript.
Conflicts of Interest
P.C.C. has served as a consultant for Fresenius Kabi Ltd., B. Braun Medical, and Baxter Healthcare Corporation. M.F.C.-B. has served as a consultant for Baxter Healthcare Corporation. E.D.W. and W.C. have no relevant conflicts of interest to declare. J.J. is an employee of Baxter Healthcare Corporation. G.Z. is a former employee and has also served as a consultant for Baxter Healthcare Corporation.
References
- Singer, P.; Berger, M.M.; Van den Berghe, G.; Biolo, G.; Calder, P.; Forbes, A.; Griffiths, R.; Kreyman, G.; Leverve, X.; Pichard, C. ESPEN Guidelines on Parenteral Nutrition: Intensive care. Clin. Nutr. 2009, 28, 387–400. [Google Scholar] [CrossRef] [PubMed]
- Pontes-Arruda, A. Biological benefits of an oleic acid-rich lipid emulsion for parenteral nutrition. Clin. Nutr. Suppl. 2009, 4, 19–23. [Google Scholar] [CrossRef]
- Abdullah, M.M.; Jew, S.; Jones, P.J. Health benefits and evaluation of healthcare cost savings if oils rich in monounsaturated fatty acids were substituted for conventional dietary oils in the United States. Nutr. Rev. 2017. [Google Scholar] [CrossRef] [PubMed]
- Carrillo, C.; Cavia Mdel, M.; Alonso-Torre, S. Role of oleic acid in immune system; mechanism of action: A review. Nutr. Hosp. 2012, 27, 978–990. [Google Scholar] [CrossRef] [PubMed]
- Harvey, K.; Xu, Z.; Walker, C.; Pavlina, T.; McGrath, S.; Zaloga, G.; Siddiqui, R. Parenteral lipid emulsions in guinea pigs differentially influence plasma and tissue levels of fatty acids, squalene, cholesterol, and phytosterols. Lipids 2014, 49, 777–793. [Google Scholar] [CrossRef] [PubMed]
- Eritsland, J. Safety considerations of polyunsaturated fatty acids. Am. J. Clin. Nutr. 2000, 71, 197S–201S. [Google Scholar] [CrossRef] [PubMed]
- Buenestado, A.; Cortijo, J.; Sanz, M.-J.; Naim-Abu-Nabah, Y.; Martinez-Losa, M.; Mata, M.; Issekutz, A.C.; Marti-Bonmati, E.; Morcillo, E.J. Olive oil-based lipid emulsion’s neutral effects on neutrophil functions and leukocyte-endothelial cell interactions. JPEN J. Parenter. Enter. Nutr. 2006, 30, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Grimble, R.F. Polyunsaturated fatty acids, inflammation and immunity. Eur. J. Clin. Nutr. 2002, 56 (Suppl. 3), S14–S19. [Google Scholar] [CrossRef] [PubMed]
- Wanten, G.J.; Calder, P.C. Immune modulation by parenteral lipid emulsions. Am. J. Clin. Nutr. 2007, 85, 1171–1184. [Google Scholar] [CrossRef] [PubMed]
- Wanten, G.J.A. Parenteral lipids in nutritional support and immune modulation. Clin. Nutr. Suppl. 2009, 4, 13–17. [Google Scholar] [CrossRef]
- Xu, Z.; Harvey, K.; Pavlina, T.; Dutot, G.; Zaloga, G.; Siddiqui, R. An improved method for determining medium- and long-chain FAMEs using gas chromatography. Lipids 2010, 45, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Harvey, K.A.; Pavlina, T.; Dutot, G.; Hise, M.; Zaloga, G.P.; Siddiqui, R.A. Steroidal compounds in commercial parenteral lipid emulsions. Nutrients 2012, 4, 904–921. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Harvey, K.A.; Pavlina, T.M.; Zaloga, G.P.; Siddiqui, R.A. Tocopherol and tocotrienol homologs in parenteral lipid emulsions. Eur. J. Lipid Sci. Technol. 2015, 117, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Linseisen, J.; Hoffmann, J.; Lienhard, S.; Jauch, K.W.; Wolfram, G. Liver function and plasma patients receiving TPN with an omega-3-fatty acid-containing lipid emulsion supplemented with alpha-tocopherol. Clin. Nutr. 2000, 19, 177–184. [Google Scholar] [CrossRef] [PubMed]
- D’Ascenzo, R.; Savini, S.; Biagetti, C.; Bellagamba, M.P.; Marchionni, P.; Pompilio, A.; Cogo, P.E.; Carnielli, V.P. Higher docosahexaenoic acid, lower arachidonic acid and reduced lipid tolerance with high doses of a lipid emulsion containing 15% fish oil: A randomized clinical trial. Clin. Nutr. 2014, 33, 1002–1009. [Google Scholar] [CrossRef] [PubMed]
- Driscoll, D.F.; Ling, P.R.; Andersson, C.; Bistrian, B.R. Hepatic indicators of oxidative stress and tissue damage accompanied by systemic inflammation in rats following a 24-hour infusion of an unstable lipid emulsion admixture. JPEN J. Parenter. Enter. Nutr. 2009, 33, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Goulet, O.; Antebi, H.; Wolf, C.; Talbotec, C.; Alcindor, L.G.; Corriol, O.; Lamor, M.; Colomb-Jung, V. A new intravenous fat emulsion containing soybean oil, medium-chain triglycerides, olive oil, and fish oil: A single-center, double-blind randomized study on efficacy and safety in pediatric patients receiving home parenteral nutrition. JPEN J. Parenter. Enter. Nutr. 2010, 34, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Grimm, H.; Mertes, N.; Goeters, C.; Schlotzer, E.; Mayer, K.; Grimminger, F.; Furst, P. Improved fatty acid and leukotriene pattern with a novel lipid emulsion in surgical patients. Eur. J. Nutr. 2006, 45, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Antebi, H.; Mansoor, O.; Ferrier, C.; Tetegan, M.; Morvan, C.; Rangaraj, J.; Alcindor, L.G. Liver function and plasma antioxidant status in intensive care unit patients requiring total parenteral nutrition: Comparison of 2 fat emulsions. JPEN J. Parenter. Enter. Nutr. 2004, 28, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Jia, Z.Y.; Yang, J.; Xia, Y.; Tong, D.N.; Zaloga, G.P.; Qin, H.L.; Qiu, Z.; Li, W.; Jiang, X.; Peng, B.; et al. Safety and efficacy of an olive oil-based triple-chamber bag for parenteral nutrition: A prospective, randomized, multi-center clinical trial in China. Nutr. J. 2015, 14, 119. [Google Scholar] [CrossRef] [PubMed]
- Yaqoob, P. Monounsaturated fatty acids in parenteral nutrition; evaluation of risks and benefits. Br. J. Nutr. 2005, 94, 867–868. [Google Scholar] [CrossRef] [PubMed]
- Cury-Boaventura, M.F.; Gorjao, R.; de Lima, T.M.; Fiamoncini, J.; Torres, R.P.; Mancini-Filho, J.; Soriano, F.G.; Curi, R. Effect of olive oil-based emulsion on human lymphocyte and neutrophil death. JPEN J. Parenter. Enter. Nutr. 2008, 32, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Granato, D.; Blum, S.; Rossle, C.; Le Boucher, J.; Malnoe, A.; Dutot, G. Effects of parenteral lipid emulsions with different fatty acid composition on immune cell functions in vitro. JPEN J. Parenter. Enter. Nutr. 2000, 24, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.; Smiley, D.; Newton, C.; Le, N.-A.; Gosmanov, A.R.; Spiegelman, R.; Peng, L.; Osteen, S.J.; Jones, D.P.; Quyyumi, A.A.; et al. Substitution of standard soybean oil with olive oil-based lipid emulsion in parenteral nutrition: Comparison of vascular, metabolic, and inflammatory effects. J. Clin. Endocrinol. Metab. 2011, 96, 3207–3216. [Google Scholar] [CrossRef] [PubMed]
- Juttner, B.; Kroplin, J.; Coldewey, S.M.; Witt, L.; Osthaus, W.A.; Weilbach, C.; Scheinichen, D. Unsaturated long-chain fatty acids induce the respiratory burst of human neutrophils and monocytes in whole blood. Nutr. Metab. 2008, 5, 19. [Google Scholar] [CrossRef] [PubMed]
- Mateu-de Antonio, J.; Grau, S.; Luque, S.; Marin-Casino, M.; Albert, I.; Ribes, E. Comparative effects of olive oil-based and soyabean oil-based emulsions on infection rate and leucocyte count in critically ill patients receiving parenteral nutrition. Br. J. Nutr. 2008, 99, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Buschmann, K.; Poeschl, J.; Braach, N.; Hudalla, H.; Kuss, N.; Frommhold, D. The olive oil-based lipid clinoleic blocks leukocyte recruitment and improves survival during systemic inflammation: A comparative in vivo study of different parenteral lipid emulsions. Mediat. Inflamm. 2015, 2015, 757059. [Google Scholar] [CrossRef] [PubMed]
- Garnacho-Montero, J.; Ortiz-Leyba, C.; Garnacho-Montero, M.C.; Garcia-Garmendia, J.L.; Perez-Paredes, C.; Moyano-Del Estad, M.R.; Barrero-Almodovar, A.; Jimenez-Jimenez, F.J. Effects of three intravenous lipid emulsions on the survival and mononuclear phagocyte function of septic rats. Nutrition 2002, 18, 751–754. [Google Scholar] [CrossRef]
- Versleijen, M.W.; Roelofs, H.M.; te Morsche, R.H.; Simonetti, E.R.; Hermans, P.W.; Wanten, G.J. Parenteral lipids impair pneumococcal elimination by human neutrophils. Eur. J. Clin. Investig. 2010, 40, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Le, H.D.; Meisel, J.A.; de Meijer, V.E.; Gura, K.M.; Puder, M. The essentiality of arachidonic acid and docosahexaenoic acid. Prostaglandins Leukot. Essent. Fatty Acids. 2009, 81, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Nanhuck, R.M.; Doublet, A.; Yaqoob, P. Effects of lipid emulsions on lipid body formation and eicosanoid production by human peripheral blood mononuclear and polymorphonuclear cells. Clin. Nutr. 2009, 28, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Reimund, J.-M.; Scheer, O.; Muller, C.D.; Pinna, G.; Duclos, B.; Baumann, R. In vitro modulation of inflammatory cytokine production by three lipid emulsions with different fatty acid compositions. Clin. Nutr. 2004, 23, 1324–1332. [Google Scholar] [CrossRef] [PubMed]
- Badía-Tahull, M.B.; Llop-Talaveron, J.M.; Leiva-Badosa, E.; Biondo, S.; Farran-Teixido, L.; Ramon-Torrell, J.M.; Jodar-Masanes, R. A randomised study on the clinical progress of high-risk elective major gastrointestinal surgery patients treated with olive oil-based parenteral nutrition with or without a fish oil supplement. Br. J. Nutr. 2010, 104, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Demirer, S.; Sapmaz, A.; Karaca, A.S.; Kepenekci, I.; Aydintug, S.; Balci, D.; Sonyurek, P.; Kose, K. Effects of postoperative parenteral nutrition with different lipid emulsions in patients undergoing major abdominal surgery. Ann. Surg. Treat. Res. 2016, 91, 309–315. [Google Scholar] [CrossRef] [PubMed]
- García-de-Lorenzo, A.; Denia, R.; Atlan, P.; Martinez-Ratero, S.; Le Brun, A.; Evard, D.; Bereziat, G. Parenteral nutrition providing a restricted amount of linoleic acid in severely burned patients: A randomised double-blind study of an olive oil-based lipid emulsion v. medium/long-chain triacylglycerols. Br. J. Nutr. 2005, 94, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Olthof, E.D.; Roelofs, H.M.J.; Versleijen, M.W.J.; Te Morsche, R.H.M.; Simonetti, E.R.; Hermans, P.W.M.; Wanten, G.J.A. Long-term olive oil-based parenteral nutrition sustains innate immune function in home patients without active underlying disease. Clin. Nutr. 2013, 32, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Olthof, E.D.; Roelofs, H.M.J.; Fisk, H.L.; Calder, P.C.; Wanten, G.J.A. No clinical or biochemical evidence for essential fatty acid deficiency in home patients who depend on long-term mixed olive oil- and soybean oil-based parenteral nutrition. JPEN J. Parenter. Enter. Nutr. 2016, 40, 982–988. [Google Scholar] [CrossRef] [PubMed]
- Onar, P.; Yildiz, B.D.; Yildiz, E.A.; Besler, T.; Abbasoglu, O. Olive oil-based fat emulsion versus soy oil-based fat emulsion in abdominal oncologic surgery. Nutr. Clin. Pract. 2011, 26, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Reimund, J.M.; Rahmi, G.; Escalin, G.; Pinna, G.; Finck, G.; Muller, C.D.; Duclos, B.; Baumann, R. Efficacy and safety of an olive oil-based intravenous fat emulsion in adult patients on home parenteral nutrition. Aliment. Pharmacol. Ther. 2005, 21, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Umpierrez, G.E.; Spiegelman, R.; Zhao, V.; Smiley, D.D.; Pinzon, I.; Griffith, D.P.; Peng, L.; Morris, T.; Luo, M.; Garcia, H.; et al. A double-blind, randomized clinical trial comparing soybean oil-based versus olive oil-based lipid emulsions in adult medical-surgical intensive care unit patients requiring parenteral nutrition. Crit. Care Med. 2012, 40, 1792–1798. [Google Scholar] [CrossRef] [PubMed]
- Demirel, G.; Oguz, S.S.; Celik, I.H.; Erdeve, O.; Uras, N.; Dilmen, U. The metabolic effects of two different lipid emulsions used in parenterally fed premature infants—A randomized comparative study. Early Hum. Dev. 2012, 88, 499–501. [Google Scholar] [CrossRef] [PubMed]
- Gawecka, A.; Michalkiewicz, J.; Kornacka, M.K.; Luckiewicz, B.; Kubiszewska, I. Immunologic properties differ in preterm infants fed olive oil vs. soy-based lipid emulsions during parenteral nutrition. JPEN J. Parenter. Enter. Nutr. 2008, 32, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Koksal, N.; Kavurt, A.V.; Cetinkaya, M.; Ozarda, Y.; Ozkan, H. Comparison of lipid emulsions on antioxidant capacity in preterm infants receiving parenteral nutrition. Pediatr. Int. 2011, 53, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Savini, S.; D’Ascenzo, R.; Biagetti, C.; Serpentini, G.; Pompilio, A.; Bartoli, A.; Cogo, P.E.; Carnielli, V.P. The effect of 5 intravenous lipid emulsions on plasma phytosterols in preterm infants receiving parenteral nutrition: A randomized clinical trial. Am. J. Clin. Nutr. 2013, 98, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhou, K.-J.; Tang, Q.-Y.; Hong, L.; Feng, Y.; Lu, L.-N.; Wang, W.-P.; Cai, W. Effect of an olive oil-based lipid emulsion compared with a soybean oil-based lipid emulsion on liver chemistry and bile acid composition in preterm infants receiving parenteral nutrition: A double-blind, randomized trial. JPEN J. Parenter. Enter. Nutr. 2016, 40, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Feng, Y.; Lu, L.-N.; Wang, W.-P.; He, Z.-J.; Xie, L.-J.; Hong, L.; Tang, Q.-Y.; Cai, W. The effects of different lipid emulsions on the lipid profile, fatty acid composition, and antioxidant capacity of preterm infants: A double-blind, randomized clinical trial. Clin. Nutr. 2016, 35, 1023–1031. [Google Scholar] [CrossRef] [PubMed]
- Cury-Boaventura, M.F.; Gorjao, R.; de Lima, T.M.; Piva, T.M.; Peres, C.M.; Soriano, F.G.; Curi, R. Toxicity of a soybean oil emulsion on human lymphocytes and neutrophils. JPEN J. Parenter. Enter. Nutr. 2006, 30, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Luzzati, R.; Cavinato, S.; Giangreco, M.; Grana, G.; Centonze, S.; Deiana, M.L.; Biolo, G.; Barbone, F. Peripheral and total parenteral nutrition as the strongest risk factors for nosocomial candidemia in elderly patients: A matched case-control study. Mycoses 2013, 56, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Netto, R.; Mondini, M.; Pezzella, C.; Romani, L.; Lucignano, B.; Pansani, L.; D’Argenio, P.; Cogo, P. Parenteral nutrition is one of the most significant risk factors for nosocomial infections in a pediatric cardiac intensive care unit. JPEN J. Parenter. Enter. Nutr. 2017, 41, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Bruna, E.; Petit, E.; Beljean-Leymarie, M.; Huynh, S.; Nouveloto, A. Specific susceptibility of docosahexaenoic acid and eicosapentaenoic acid to peroxidation in aqueous solution. Lipids 1989, 24, 970–975. [Google Scholar] [CrossRef]
- Goulet, O.; de Potter, S.; Antebi, H.; Driss, F.; Colomb, V.; Bereziat, G.; Alcindor, L.G.; Corriol, O.; Le Brun, A.; Dutot, G.; et al. Long-term efficacy and safety of a new olive oil-based intravenous fat emulsion in pediatric patients: A double-blind randomized study. Am. J. Clin. Nutr. 1999, 70, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Sala-Vila, A.; Barbosa, V.M.; Calder, P.C. Olive oil in parenteral nutrition. Curr. Opin. Clin. Nutr. Metab. Care 2007, 10, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Witting, P.K.; Upston, J.M.; Stocker, R. The molecular action of alpha-tocopherol in lipoprotein lipid peroxidation. Pro- and antioxidant activity of vitamin E in complex heterogeneous lipid emulsions. Subcell. Biochem. 1998, 30, 345–390. [Google Scholar] [PubMed]
- Xu, Z.; Harvey, K.A.; Pavlina, T.M.; Zaloga, G.P.; Siddiqui, R.A. Distribution of tocopherols and tocotrienols in guinea pig tissues following parenteral lipid emulsion infusion. JPEN J. Parenter. Enter. Nutr. 2016, 40, 672–681. [Google Scholar] [CrossRef] [PubMed]
- Watkins, S.M.; Carter, L.C.; German, J.B. Docosahexaenoic acid accumulates in cardiolipin and enhances HT-29 cell oxidant production. J. Lipid Res. 1998, 39, 1583–1588. [Google Scholar] [PubMed]
- Fuhrman, B.; Volkova, N.; Aviram, M. Postprandial serum triacylglycerols and oxidative stress in mice after consumption of fish oil, soy oil or olive oil: Possible role for paraoxonase-1 triacylglycerol lipase-like activity. Nutrition 2006, 22, 922–930. [Google Scholar] [CrossRef] [PubMed]
- Lauriti, G.; Zani, A.; Aufieri, R.; Cananzi, M.; Chiesa, P.L.; Eaton, S.; Pierro, A. Incidence, prevention, and treatment of parenteral nutrition-associated cholestasis and intestinal failure-associated liver disease in infants and children: A systematic review. JPEN J. Parenter. Enter. Nutr. 2014, 38, 70–85. [Google Scholar] [CrossRef] [PubMed]
- Antebi, H.; Zimmermann, L.; Bourcier, C.; Le Brun, A.; Giudicelli, A.; Dutot, G.; Colomb, V.; Corriol, O.; Goulet, O.; Ricour, C.; et al. Peroxydation in vitro et effet de l’administration en nutrition parenterale totale d’une emulsion lipidique a base d’huile d’olive sur la peroxydabilite des lipoproteines de dasse densite chez l’enfant. Nutr. Clin. Metab. 1996, 10, 41S–43S. [Google Scholar] [CrossRef]
- Deshpande, G.C.; Simmer, K.; Mori, T.; Croft, K. Parenteral lipid emulsions based on olive oil compared with soybean oil in preterm (<28 weeks’ gestation) neonates: A randomised controlled trial. J. Pediatr. Gastroenterol. Nutr. 2009, 49, 619–625. [Google Scholar] [PubMed]
- Roggero, P.; Mosca, F.; Gianni, M.L.; Orsi, A.; Amato, O.; Migliorisi, E.; Longini, M.; Buonocore, G. F2-isoprostanes and total radical-trapping antioxidant potential in preterm infants receiving parenteral lipid emulsions. Nutrition 2010, 26, 551–555. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.N.; Hardy, P.; Peterkin, M.; Lee, O.; Shalley, H.; Croft, K.D.; Mori, T.A.; Heine, R.G.; Bines, J.E. Tolerability and safety of olive oil-based lipid emulsion in critically ill neonates: A blinded randomized trial. Nutrition 2008, 24, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Hartman, C.; Ben-Artzi, E.; Berkowitz, D.; Elhasid, R.; Lajterer, N.; Postovski, S.; Hadad, S.; Shamir, R. Olive oil-based intravenous lipid emulsion in pediatric patients undergoing bone marrow transplantation: A short-term prospective controlled trial. Clin. Nutr. 2009, 28, 631–635. [Google Scholar] [CrossRef] [PubMed]
- Pitkanen, O.M.; Luukkainen, P.; Andersson, S. Attenuated lipid peroxidation in preterm infants during subsequent doses of intravenous lipids. Biol. Neonate 2004, 85, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, G.; Simmer, K.; Deshmukh, M.; Mori, T.A.; Croft, K.D.; Kristensen, J. Fish Oil (SMOFlipid) and olive oil lipid (Clinoleic) in very preterm neonates. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Unal, S.; Demirel, N.; Erol, S.; Isik, D.U.; Kulali, F.; Iyigun, F.; Bas, A.Y. Effects of two different lipid emulsions on morbidities and oxidant stress statuses in preterm infants: An observational study. J. Matern. Fetal Neonatal Med. 2018, 31, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Edward, R.R.; Innes, J.K.; Marino, L.V.; Calder, P.C. Influence of different intravenous lipid emulsions on growth, development and laboratory and clinical outcomes in hospitalised paediatric patients: A systematic review. Clin. Nutr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Nghiem-Rao, T.H.; Dahlgren, A.F.; Kalluri, D.; Cao, Y.; Simpson, P.M.; Patel, S.B. Influence of gestational age and birth weight in neonatal cholesterol response to total parenteral nutrition. J. Clin. Lipidol. 2016, 10, 891–897. [Google Scholar] [CrossRef] [PubMed]
- NCEP. National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar]
- Gultekin, G.; Sahin, H.; Inanc, N.; Uyanik, F.; Ok, E. Impact of omega-3 and omega-9 fatty acids enriched total parenteral nutrition on blood chemistry and inflammatory markers in septic patients. Pak. J. Med. Sci. 2014, 30, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Huschak, G.; Zur Nieden, K.; Hoell, T.; Riemann, D.; Mast, H.; Stuttmann, R. Olive oil based nutrition in multiple trauma patients: A pilot study. Intensive Care Med. 2005, 31, 1202–1208. [Google Scholar] [CrossRef] [PubMed]
- Puiggròs, C.; Sanchez, J.; Chacon, P.; Sabin, P.; Rosello, J.; Bou, R.; Planas, M. Evolution of lipid profile, liver function, and pattern of plasma fatty acids according to the type of lipid emulsion administered in parenteral nutrition in the early postoperative period after digestive surgery. JPEN J. Parenter. Enter. Nutr. 2009, 33, 501–512. [Google Scholar] [CrossRef] [PubMed]
- Piper, S.N.; Schade, I.; Beschmann, R.B.; Maleck, W.H.; Boldt, J.; Rohm, K.D. Hepatocellular integrity after parenteral nutrition: Comparison of a fish-oil-containing lipid emulsion with an olive-soybean oil-based lipid emulsion. Eur. J. Anaesthesiol. 2009, 26, 1076–1082. [Google Scholar] [CrossRef] [PubMed]
- Pálová, S.; Charvat, J.; Kvapil, M. Comparison of soybean oil- and olive oil-based lipid emulsions on hepatobiliary function and serum triacylglycerols level during realimentation. J. Int. Med. Res. 2008, 36, 587–593. [Google Scholar] [CrossRef] [PubMed]
- Piper, S.; Schollhorn, T.; Schade, I.; Beschmann, R.; Rohm, K. Modulation of lipid utilisation by parenteral administration of a fish-oil-enriched new lipid formula (SMOFlipid) in surgical ICU patients: Comparison with a lipid emulsion based on olive and soybean oil. Crit. Care 2009, 13, S57. [Google Scholar] [CrossRef]
- Kurvinen, A.; Nissinen, M.J.; Gylling, H.; Miettinen, T.A.; Lampela, H.; Koivusalo, A.I.; Rintala, R.J.; Pakarinen, M.P. Effects of long-term parenteral nutrition on serum lipids, plant sterols, cholesterol metabolism, and liver histology in pediatric intestinal failure. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Van Kempen, A.A.; van der Crabben, S.N.; Ackermans, M.T.; Endert, E.; Kok, J.H.; Sauerwein, H.P. Stimulation of gluconeogenesis by intravenous lipids in preterm infants: Response depends on fatty acid profile. Am. J. Physiol. Endocrinol. Metab. 2006, 290, E723–E730. [Google Scholar] [CrossRef] [PubMed]
- Hadley, K.B.; Ryan, A.S.; Forsyth, S.; Gautier, S.; Salem, N., Jr. The essentiality of arachidonic acid in infant development. Nutrients 2016, 8, 216. [Google Scholar] [CrossRef] [PubMed]
- Colombo, J.; Jill Shaddy, D.; Kerling, E.H.; Gustafson, K.M.; Carlson, S.E. Docosahexaenoic acid (DHA) and arachidonic acid (ARA) balance in developmental outcomes. Prostaglandins Leukot. Essent. Fatty Acids 2017, 121, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Alshweki, A.; Munuzuri, A.P.; Bana, A.M.; de Castro, M.J.; Andrade, F.; Aldamiz-Echevarria, L.; de Pipaon, M.S.; Fraga, J.M.; Couce, M.L. Effects of different arachidonic acid supplementation on psychomotor development in very preterm infants; a randomized controlled trial. Nutr. J. 2015, 14, 101. [Google Scholar] [CrossRef] [PubMed]
- Najm, S.; Lofqvist, C.; Hellgren, G.; Engstrom, E.; Lundgren, P.; Hard, A.L.; Lapillonne, A.; Savman, K.; Nilsson, A.K.; Andersson, M.X.; et al. Effects of a lipid emulsion containing fish oil on polyunsaturated fatty acid profiles, growth and morbidities in extremely premature infants: A randomized controlled trial. Clin. Nutr. ESPEN 2017, 20, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Hojsak, I.; Colomb, V.; Braegger, C.; Bronsky, J.; Campoy, C.; Domellof, M.; Embleton, N.; Fidler Mis, N.; Hulst, J.M.; Indrio, F.; et al. ESPGHAN Committee on Nutrition position paper. Intravenous lipid emulsions and risk of hepatotoxicity in infants and children: A systematic review and meta-analysis. J. Pediatr. Gastroenterol. Nutr. 2016, 62, 776–792. [Google Scholar] [CrossRef] [PubMed]
- Beath, S.V.; Kelly, D.A. Total parenteral nutrition-induced cholestasis: Prevention and management. Clin. Liver Dis. 2016, 20, 159–176. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.-J.; Sun, L.-L.; Li, M.-Y.; Ding, C.-L.; Su, Y.-C.; Sun, L.-J.; Xue, S.-H.; Yan, F.; Zhao, C.-H.; Wang, W. Comparison of formulas based on lipid emulsions of olive oil, soybean oil, or several oils for parenteral nutrition: A systematic review and meta-analysis. Adv. Nutr. 2016, 7, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Zaloga, G.P. Phytosterols, lipid administration, and liver disease during parenteral nutrition. JPEN J. Parenter. Enter. Nutr. 2015, 39, 39S–60S. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, C.B.; De Bruin, T.W.A.; Jansen, H.; Erkelens, D.W. Different clearance of intravenously administered olive oil and soybean oil emulsions: Role of hepatic lipase. Am. J. Clin. Nutr. 1993, 57, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Lacaille, F.; Gupte, G.; Colomb, V.; D’Antiga, L.; Hartman, C.; Hojsak, I.; Kolacek, S.; Puntis, J.; Shamir, R. Intestinal failure-associated liver disease: A position paper of the ESPGHAN working group of intestinal failure and intestinal transplantation. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Gobel, Y.; Koletzko, B.; Bohles, H.-J.; Engelsberger, I.; Forget, D.; Le Brun, A.; Peters, J.; Zimmermann, A. Parenteral fat emulsions based on olive and soybean oils: A randomized clinical trial in preterm infants. J. Pediatr. Gastroenterol. Nutr. 2003, 37, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Grau, T.; Bonet, A.; Rubio, M.; Mateo, D.; Farre, M.; Acosta, J.A.; Blesa, A.; Montejo, J.C.; de Lorenzo, A.G.; Mesejo, A.; et al. Liver dysfunction associated with artificial nutrition in critically ill patients. Crit. Care 2007, 11, R10. [Google Scholar] [CrossRef] [PubMed]
- Hartman, C.; Berkowitz, D.; Elhasid, R.; Ben Harush, M.; Hadad, S.; Shamir, R. Tolerability and safety of short-term olive oil-based intravenous lipid emulsion in pediatric patients undergoing bone marrow transplantation. J. Pediatr. Gastroenterol. Nutr. 2009, 48, E139–E140. [Google Scholar]
- Thomas-Gibson, S.; Jawhari, A.; Atlan, P.; Brun, A.L.A.L.; Farthing, M.; Forbes, A. Safe and efficacious prolonged use of an olive oil-based lipid emulsion (ClinOleic) in chronic intestinal failure. Clin. Nutr. 2004, 23, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Vahedi, K.; Atlan, P.; Joly, F.; Le Brun, A.; Evard, D.; Perennec, V.; Roux-Haguenau, D.; Bereziat, G.; Messing, B. A 3-month double-blind randomised study comparing an olive oil- with a soyabean oil-based intravenous lipid emulsion in home parenteral nutrition patients. Br. J. Nutr. 2005, 94, 909–916. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.-P.; Yan, X.-L.; Ni, Y.-F.; Guo, K.; Ke, C.-K.; Cheng, Q.-S.; Lu, Q.; Zhang, L.-J.; Li, X.-F. Effects of lipid emulsions in parenteral nutrition of esophageal cancer surgical patients receiving enteral nutrition: A comparative analysis. Nutrients 2013, 6, 111–123. [Google Scholar] [CrossRef] [PubMed]
- Klek, S.; Szczepanek, K.; Scislo, L.; Walewska, E.; Pietka, M.; Pisarska, M.; Pedziwiatr, M. Intravenous lipid emulsions and liver function in adult chronic intestinal failure patients: Results from a randomized clinical trial. Nutrition 2017. [Google Scholar] [CrossRef]
- Johnston, D.E. Special considerations in interpreting liver function tests. Am. Fam. Phys. 1999, 59, 2223–2230. [Google Scholar]
- Chlopicki, S. Perspectives in pharmacology of endothelium: From bench to bedside. Pharmacol. Rep. 2015, 67, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Aird, W.C. Endothelial cell heterogeneity. Crit. Care Med. 2003, 31, S221–S230. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A.; Gao, L.; Thakur, A.; Siu, P.M.; Lai, C.W.K. Role of free fatty acids in endothelial dysfunction. J. Biomed. Sci. 2017, 24, 50. [Google Scholar] [CrossRef] [PubMed]
- Goswami, D.; Vestweber, D. How leukocytes trigger opening and sealing of gaps in the endothelial barrier. F1000Res 2016, 5. [Google Scholar] [CrossRef] [PubMed]
- Waitzberg, D.L.; Torrinhas, R.S.; Jacintho, T.M. New parenteral lipid emulsions for clinical use. JPEN J. Parenter. Enter. Nutr. 2006, 30, 351–367. [Google Scholar] [CrossRef] [PubMed]
- Umpierrez, G.E.; Smiley, D.; Robalino, G.; Peng, L.; Kitabchi, A.E.; Khan, B.; Le, A.; Quyyumi, A.; Brown, V.; Phillips, L.S. Intravenous intralipid-induced blood pressure elevation and endothelial dysfunction in obese African-Americans with type 2 diabetes. J. Clin. Endocrinol. Metab. 2009, 94, 609–614. [Google Scholar] [CrossRef] [PubMed]
- Amissi, S.; Boisrame-Helms, J.; Burban, M.; Rashid, S.K.; Leon-Gonzalez, A.J.; Auger, C.; Toti, F.; Meziani, F.; Schini-Kerth, V.B. Lipid emulsions containing medium chain triacylglycerols blunt bradykinin-induced endothelium-dependent relaxation in porcine coronary artery rings. Lipids 2017, 52, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Harvey, K.A.; Xu, Z.; Pavlina, T.M.; Zaloga, G.P.; Siddiqui, R.A. Modulation of endothelial cell integrity and inflammatory activation by commercial lipid emulsions. Lipid Health Dis. 2015, 14, 9. [Google Scholar] [CrossRef] [PubMed]
- Talbott, G.A.; Sharar, S.R.; Harlan, J.M.; Winn, R.K. Leukocyte-endothelial interactions and organ injury: The role of adhesion molecules. New Horiz. 1994, 2, 545–554. [Google Scholar] [PubMed]
- Abbasoglu, O.; Hardy, G.; Manzanares, W.; Pontes-Arruda, A. Fish oil-containing lipid emulsions in adult parenteral nutrition: A review of the evidence. JPEN J. Parenter. Enter. Nutr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Adolph, M.; Deutz, N.E.; Grau, T.; Innes, J.K.; Klek, S.; Lev, S.; Mayer, K.; Michael-Titus, A.T.; Pradelli, L.; et al. Lipids in the intensive care unit: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2018, 37, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Edmunds, C.E.; Brody, R.A.; Parrott, J.S.; Stankorb, S.M.; Heyland, D.K. The effects of different IV fat emulsions on clinical outcomes in critically ill patients. Crit. Care Med. 2014, 42, 1168–1177. [Google Scholar] [CrossRef] [PubMed]
- Manzanares, W.; Dhaliwal, R.; Jurewitsch, B.; Stapleton, R.D.; Jeejeebhoy, K.N.; Heyland, D.K. Alternative lipid emulsions in the critically ill: A systematic review of the evidence. Intensive Care Med. 2013, 39, 1683–1694. [Google Scholar] [CrossRef] [PubMed]
- Pawlik, D.; Lauterbach, R.; Walczak, M.; Hurkala, J.; Sherman, M.P. Fish-oil fat emulsion supplementation reduces the risk of retinopathy in very low birth weight infants: A prospective, randomized study. JPEN J. Parenter. Enter. Nutr. 2014, 38, 711–716. [Google Scholar] [CrossRef] [PubMed]
- United States Pharmacopeia. Globule Size Distribution in Lipid Injectable Emulsions; USP37/NF32; United States Pharmacopeia: Rockville, MD, USA, 2014; Chapter 729; pp. 360–363. [Google Scholar]
- Mirtallo, J.; Canada, T.; Johnson, D.; Kumpf, V.; Petersen, C.; Sacks, G.; Seres, D.; Guenter, P. Safe practices for parenteral nutrition. JPEN J. Parenter. Enter. Nutr. 2004, 28, S39–S70. [Google Scholar] [CrossRef]
- Driscoll, D.F.; Giampietro, K.; Wichelhaus, D.P.; Peterss, H.; Nehne, J.; Niemann, W.; Bistrian, B.R. Physicochemical stability assessments of lipid emulsions of varying oil composition. Clin. Nutr. 2001, 20, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Driscoll, D.F.; Bhargava, H.N.; Li, L.; Zaim, R.H.; Babayan, V.K.; Bistrian, B.R. Physicochemical stability of total nutrient admixtures. Am. J. Health Syst. Pharm. 1995, 52, 623–634. [Google Scholar] [PubMed]
- Telessy, I.G.; Balogh, J.; Szaba, B.; Csempesz, F.; Zelka, R. Kinetic stability of all-in-one parenteral nutrition admixtures in the presence of high dose Ca2+ additive under clinical application circumstances. Nutr. J. 2012, 11, 32. [Google Scholar] [CrossRef] [PubMed]
- Alfonso, J.E.; Berlana, D.; Ukleja, A.; Boullata, J. Clinical, ergonomic, and economic outcomes with multichamber bags compared with (Hospital) pharmacy compounded bags and multibottle systems: A systematic literature review. JPEN J. Parenter. Enter. Nutr. 2017, 41, 1162–1177. [Google Scholar] [CrossRef] [PubMed]
- Staven, V.; Wang, S.; Gronlie, I.; Tho, I. Development and evaluation of a test program for Y-site compatibility testing of total parenteral nutrition and intravenous drugs. Nutr. J. 2016, 15, 29. [Google Scholar] [CrossRef] [PubMed]
- Gallegos, C.; Valencia, C.; Partal, P.; Franco, J.M.; Maglio, O.; Abrahamsson, M.; Brito-de la Fuente, E. Droplet-size distribution and stability of commercial injectable lipid emulsions containing fish oil. Am. J. Health Syst. Pharm. 2012, 69, 1332–1335. [Google Scholar] [CrossRef] [PubMed]






© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).