Nordic Diet and Inflammation—A Review of Observational and Intervention Studies



Abstract
:1. Introduction
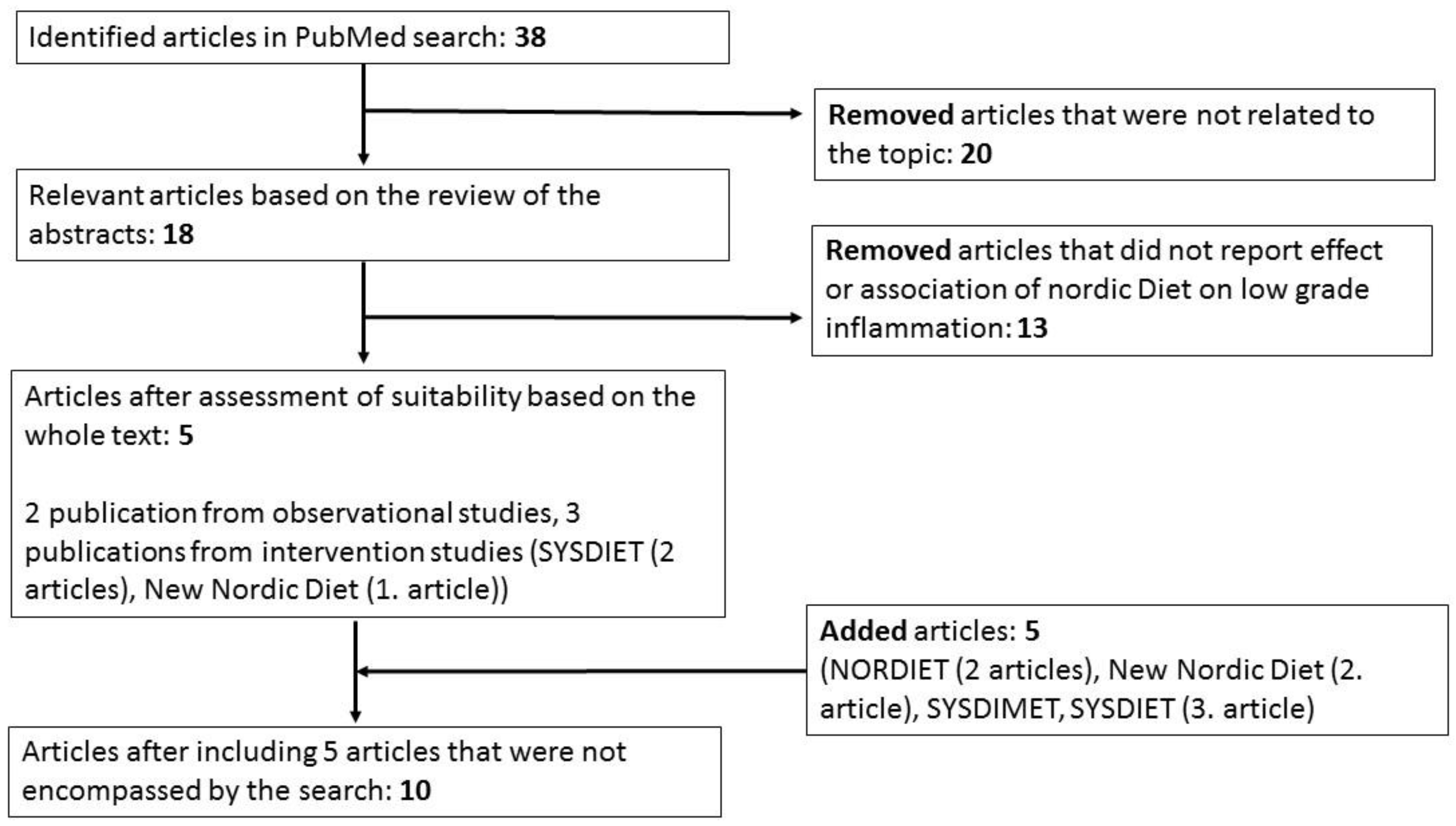
2. Methods
3. HND and LGI in Observational Studies
4. Nordic Diet and LGI in Randomized Dietary Trials
4.1. Studies Including Selected Key Components of the HND
4.2. HND in Controlled Dietary Trials
5. Discussion
6. Concluding Remarks
Author Contributions
Funding
Conflicts of Interest
References
- Hotamisligil, G.S. Inflammation and Metabolic Disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Hansson, G.K. Inflammation, Atherosclerosis, and Coronary Artery Disease. N. Engl. J. Med. 2005, 352, 1685–1695. [Google Scholar] [CrossRef] [PubMed]
- Kern, L.; Mittenbuhler, M.J.; Vesting, A.J.; Ostermann, A.L.; Wunderlich, C.M.; Wunderlich, F.T. Obesity-Induced TNFalpha and IL-6 Signaling: The Missing Link between Obesity and Inflammation-Driven Liver and Colorectal Cancers. Cancers 2018, 11, 24. [Google Scholar] [CrossRef] [PubMed]
- Costantini, E.; D’Angelo, C.; Reale, M. The Role of Immunosenescence in Neurodegenerative Diseases. Mediat. Inflamm. 2018, 2018, 6039171. [Google Scholar] [CrossRef] [PubMed]
- Yudkin, J.S. Adipose Tissue, Insulin Action and Vascular Disease: Inflammatory Signals. Int. J. Obes. Relat. Metab. Disord. 2003, 27 (Suppl. 3), S25–S28. [Google Scholar] [CrossRef]
- Unamuno, X.; Gomez-Ambrosi, J.; Rodriguez, A.; Becerril, S.; Fruhbeck, G.; Catalan, V. Adipokine Dysregulation and Adipose Tissue Inflammation in Human Obesity. Eur. J. Clin. Investig. 2018, 48, e12997. [Google Scholar] [CrossRef]
- Chmelar, J.; Chung, K.J.; Chavakis, T. The Role of Innate Immune Cells in Obese Adipose Tissue Inflammation and Development of Insulin Resistance. Thromb. Haemost. 2013, 109, 399–406. [Google Scholar]
- de Mello, V.D.; Kolehmainen, M.; Pulkkinen, L.; Schwab, U.; Mager, U.; Laaksonen, D.E.; Niskanen, L.; Gylling, H.; Atalay, M.; Rauramaa, R.; et al. Downregulation of Genes Involved in NFkappaB Activation in Peripheral Blood Mononuclear Cells After Weight Loss is Associated with the Improvement of Insulin Sensitivity in Individuals with the Metabolic Syndrome: The GENOBIN Study. Diabetologia 2008, 51, 2060–2067. [Google Scholar] [CrossRef]
- Ferreira, C.M.; Vieira, A.T.; Vinolo, M.A.; Oliveira, F.A.; Curi, R.; Martins Fdos, S. The Central Role of the Gut Microbiota in Chronic Inflammatory Diseases. J. Immunol. Res. 2014, 2014, 689492. [Google Scholar] [CrossRef]
- Telle-Hansen, V.H.; Holven, K.B.; Ulven, S.M. Impact of a Healthy Dietary Pattern on Gut Microbiota and Systemic Inflammation in Humans. Nutrients 2018, 10, 1786. [Google Scholar] [CrossRef]
- Minihane, A.M.; Vinoy, S.; Russell, W.R.; Baka, A.; Roche, H.M.; Tuohy, K.M.; Teeling, J.L.; Blaak, E.E.; Fenech, M.; Vauzour, D.; et al. Low-Grade Inflammation, Diet Composition and Health: Current Research Evidence and its Translation. Br. J. Nutr. 2015, 114, 999–1012. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Ahluwalia, N.; Brouns, F.; Buetler, T.; Clement, K.; Cunningham, K.; Esposito, K.; Jonsson, L.S.; Kolb, H.; Lansink, M.; et al. Dietary Factors and Low-Grade Inflammation in Relation to Overweight and Obesity. Br. J. Nutr. 2011, 106 (Suppl. 3), S5–S78. [Google Scholar] [CrossRef]
- Madsen, E.L.; Rissanen, A.; Bruun, J.M.; Skogstrand, K.; Tonstad, S.; Hougaard, D.M.; Richelsen, B. Weight Loss Larger than 10% is Needed for General Improvement of Levels of Circulating Adiponectin and Markers of Inflammation in Obese Subjects: A 3-Year Weight Loss Study. Eur. J. Endocrinol. 2008, 158, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Ziccardi, P.; Nappo, F.; Giugliano, G.; Esposito, K.; Marfella, R.; Cioffi, M.; D’Andrea, F.; Molinari, A.M.; Giugliano, D. Reduction of Inflammatory Cytokine Concentrations and Improvement of Endothelial Functions in Obese Women After Weight Loss Over One Year. Circulation 2002, 105, 804–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esposito, K.; Pontillo, A.; Di Palo, C.; Giugliano, G.; Masella, M.; Marfella, R.; Giugliano, D. Effect of Weight Loss and Lifestyle Changes on Vascular Inflammatory Markers in Obese Women: A Randomized Trial. JAMA 2003, 289, 1799–1804. [Google Scholar] [CrossRef] [PubMed]
- Neale, E.P.; Batterham, M.J.; Tapsell, L.C. Consumption of a Healthy Dietary Pattern Results in Significant Reductions in C-Reactive Protein Levels in Adults: A Meta-Analysis. Nutr. Res. 2016, 36, 391–401. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Mediterranean Dietary Pattern, Inflammation and Endothelial Function: A Systematic Review and Meta-Analysis of Intervention Trials. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 929–939. [Google Scholar] [CrossRef]
- Uusitupa, M.; Schwab, U. Diet, Inflammation and Prediabetes-Impact of Quality of Diet. Can. J. Diabetes 2013, 37, 327–331. [Google Scholar] [CrossRef]
- Kaluza, J.; Harris, H.; Melhus, H.; Michaelsson, K.; Wolk, A. Questionnaire-Based Anti-Inflammatory Diet Index as a Predictor of Low-Grade Systemic Inflammation. Antioxid. Redox Signal. 2018, 28, 78–84. [Google Scholar] [CrossRef]
- Kolehmainen, M.; Ulven, S.M.; Paananen, J.; de Mello, V.; Schwab, U.; Carlberg, C.; Myhrstad, M.; Pihlajamaki, J.; Dungner, E.; Sjolin, E.; et al. Healthy Nordic Diet Downregulates the Expression of Genes Involved in Inflammation in Subcutaneous Adipose Tissue in Individuals with Features of the Metabolic Syndrome. Am. J. Clin. Nutr. 2015, 101, 228–239. [Google Scholar] [CrossRef]
- De Mello, V.D.; Kolehmanien, M.; Schwab, U.; Pulkkinen, L.; Uusitupa, M. Gene Expression of Peripheral Blood Mononuclear Cells as a Tool in Dietary Intervention Studies: What do we Know so Far? Mol. Nutr. Food Res. 2012, 56, 1160–1172. [Google Scholar] [CrossRef] [PubMed]
- Kanerva, N.; Kaartinen, N.E.; Rissanen, H.; Knekt, P.; Eriksson, J.G.; Saaksjarvi, K.; Sundvall, J.; Mannisto, S. Associations of the Baltic Sea Diet with Cardiometabolic Risk Factors—A Meta-Analysis of Three Finnish Studies. Br. J. Nutr. 2014, 112, 616–626. [Google Scholar] [CrossRef]
- Kanerva, N.; Loo, B.M.; Eriksson, J.G.; Leiviska, J.; Kaartinen, N.E.; Jula, A.; Mannisto, S. Associations of the Baltic Sea Diet with Obesity-Related Markers of Inflammation. Ann. Med. 2014, 46, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Uusitupa, M.; Hermansen, K.; Savolainen, M.J.; Schwab, U.; Kolehmainen, M.; Brader, L.; Mortensen, L.S.; Cloetens, L.; Johansson-Persson, A.; Onning, G.; et al. Effects of an Isocaloric Healthy Nordic Diet on Insulin Sensitivity, Lipid Profile and Inflammation Markers in Metabolic Syndrome—A Randomized Study (SYSDIET). J. Intern. Med. 2013, 274, 52–66. [Google Scholar] [CrossRef] [PubMed]
- Fritzen, A.M.; Lundsgaard, A.M.; Jordy, A.B.; Poulsen, S.K.; Stender, S.; Pilegaard, H.; Astrup, A.; Larsen, T.M.; Wojtaszewski, J.F.; Richter, E.A.; et al. New Nordic Diet-Induced Weight Loss is Accompanied by Changes in Metabolism and AMPK Signaling in Adipose Tissue. J. Clin. Endocrinol. Metab. 2015, 100, 3509–3519. [Google Scholar] [CrossRef] [PubMed]
- Adamsson, V.; Reumark, A.; Fredriksson, I.B.; Hammarstrom, E.; Vessby, B.; Johansson, G.; Riserus, U. Effects of a Healthy Nordic Diet on Cardiovascular Risk Factors in Hypercholesterolaemic Subjects: A Randomized Controlled Trial (NORDIET). J. Intern. Med. 2011, 269, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Jobs, E.; Adamsson, V.; Larsson, A.; Jobs, M.; Nerpin, E.; Ingelsson, E.; Arnlov, J.; Riserus, U. Influence of a Prudent Diet on Circulating Cathepsin S in Humans. Nutr. J. 2014, 13, 84. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, S.K.; Due, A.; Jordy, A.B.; Kiens, B.; Stark, K.D.; Stender, S.; Holst, C.; Astrup, A.; Larsen, T.M. Health Effect of the New Nordic Diet in Adults with Increased Waist Circumference: A 6-Mo Randomized Controlled Trial. Am. J. Clin. Nutr. 2014, 99, 35–45. [Google Scholar] [CrossRef] [PubMed]
- De Mello, V.D.; Schwab, U.; Kolehmainen, M.; Koenig, W.; Siloaho, M.; Poutanen, K.; Mykkanen, H.; Uusitupa, M. A Diet High in Fatty Fish, Bilberries and Wholegrain Products Improves Markers of Endothelial Function and Inflammation in Individuals with Impaired Glucose Metabolism in a Randomised Controlled Trial: The Sysdimet Study. Diabetologia 2011, 54, 2755–2767. [Google Scholar] [CrossRef]
- Myhrstad, M.C.W.; de Mello, V.D.; Dahlman, I.; Kolehmainen, M.; Paananen, J.; Rundblad, A.; Carlberg, C.; Olstad, O.K.; Pihlajamaki, J.; Holven, K.B.; et al. Healthy Nordic Diet Modulates the Expression of Genes Related to Mitochondrial Function and Immune Response in Peripheral Blood Mononuclear Cells from Subjects with Metabolic Syndrome-A SYSDIET Sub-Study. Mol. Nutr. Food Res. 2019, e1801405. [Google Scholar] [CrossRef]
- Joosten, M.M.; Witkamp, R.F.; Hendriks, H.F. Alterations in Total and High-Molecular-Weight Adiponectin After 3 Weeks of Moderate Alcohol Consumption in Premenopausal Women. Metabolism 2011, 60, 1058–1063. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Liimatainen, J.; Alanne, A.L.; Lindstedt, A.; Liu, P.; Sinkkonen, J.; Kallio, H.; Yang, B. Phenolic Compounds Extracted by Acidic Aqueous Ethanol from Berries and Leaves of Different Berry Plants. Food Chem. 2017, 220, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Kolehmainen, M.; Mykkanen, O.; Kirjavainen, P.V.; Leppanen, T.; Moilanen, E.; Adriaens, M.; Laaksonen, D.E.; Hallikainen, M.; Puupponen-Pimia, R.; Pulkkinen, L.; et al. Bilberries Reduce Low-Grade Inflammation in Individuals with Features of Metabolic Syndrome. Mol. Nutr. Food Res. 2012, 56, 1501–1510. [Google Scholar] [CrossRef] [PubMed]
- Adamsson, V.; Reumark, A.; Marklund, M.; Larsson, A.; Riserus, U. Role of a Prudent Breakfast in Improving Cardiometabolic Risk Factors in Subjects with Hypercholesterolemia: A Randomized Controlled Trial. Clin. Nutr. 2015, 34, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Mithril, C.; Dragsted, L.O.; Meyer, C.; Tetens, I.; Biltoft-Jensen, A.; Astrup, A. Dietary Composition and Nutrient Content of the New Nordic Diet. Public Health Nutr. 2013, 16, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, S.K.; Crone, C.; Astrup, A.; Larsen, T.M. Long-Term Adherence to the New Nordic Diet and the Effects on Body Weight, Anthropometry and Blood Pressure: A 12-Month Follow-Up Study. Eur. J. Nutr. 2015, 54, 67–76. [Google Scholar] [CrossRef]
- Gupta, S.; Singh, R.K.; Dastidar, S.; Ray, A. Cysteine Cathepsin S as an Immunomodulatory Target: Present and Future Trends. Expert Opin. Ther. Targets 2008, 12, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Jobs, E.; Riserus, U.; Ingelsson, E.; Helmersson, J.; Nerpin, E.; Jobs, M.; Sundstrom, J.; Lind, L.; Larsson, A.; Basu, S.; et al. Serum Cathepsin S is Associated with Serum C-Reactive Protein and Interleukin-6 Independently of Obesity in Elderly Men. J. Clin. Endocrinol. Metab. 2010, 95, 4460–4464. [Google Scholar] [CrossRef]
- Marklund, M.; Magnusdottir, O.K.; Rosqvist, F.; Cloetens, L.; Landberg, R.; Kolehmainen, M.; Brader, L.; Hermansen, K.; Poutanen, K.S.; Herzig, K.H.; et al. A Dietary Biomarker Approach Captures Compliance and Cardiometabolic Effects of a Healthy Nordic Diet in Individuals with Metabolic Syndrome. J. Nutr. 2014, 144, 1642–1649. [Google Scholar] [CrossRef] [Green Version]
- Herder, C.; Brunner, E.J.; Rathmann, W.; Strassburger, K.; Tabak, A.G.; Schloot, N.C.; Witte, D.R. Elevated Levels of the Anti-Inflammatory Interleukin-1 Receptor Antagonist Precede the Onset of Type 2 Diabetes: The Whitehall II Study. Diabetes Care 2009, 32, 421–423. [Google Scholar] [CrossRef]
- Lankinen, M.; Schwab, U.; Kolehmainen, M.; Paananen, J.; Nygren, H.; Seppanen-Laakso, T.; Poutanen, K.; Hyotylainen, T.; Riserus, U.; Savolainen, M.J.; et al. A Healthy Nordic Diet Alters the Plasma Lipidomic Profile in Adults with Features of Metabolic Syndrome in a Multicenter Randomized Dietary Intervention. J. Nutr. 2016, 146, 662–672. [Google Scholar] [CrossRef] [PubMed]
- de Mello, V.D.; Paananen, J.; Lindstrom, J.; Lankinen, M.A.; Shi, L.; Kuusisto, J.; Pihlajamaki, J.; Auriola, S.; Lehtonen, M.; Rolandsson, O.; et al. Indolepropionic Acid and Novel Lipid Metabolites are Associated with a Lower Risk of Type 2 Diabetes in the Finnish Diabetes Prevention Study. Sci. Rep. 2017, 7, 46337. [Google Scholar] [CrossRef] [PubMed]
- Tuomainen, M.; Lindstrom, J.; Lehtonen, M.; Auriola, S.; Pihlajamaki, J.; Peltonen, M.; Tuomilehto, J.; Uusitupa, M.; de Mello, V.D.; Hanhineva, K. Associations of Serum Indolepropionic Acid, a Gut Microbiota Metabolite, with Type 2 Diabetes and Low-Grade Inflammation in High-Risk Individuals. Nutr. Diabetes 2018, 8, 35. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, A.; Scott, J.A. The Impact on Eating Habits of Temporary Translocation from a Mediterranean to a Northern European Environment. Eur. J. Clin. Nutr. 2002, 56, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Valsta, L.; Kaartinen, N.; Tapanainen, H.; Männistö, S.; Sääksjärvi, K. Nutrition in Finland—The National FinDiet 2017 Survey; Julkari: Helsinki, Finland, 2018; ISBN 978-952-343-238-3. [Google Scholar]
- Sakhaei, R.; Ramezani-Jolfaie, N.; Mohammadi, M.; Salehi-Abargouei, A. The Healthy Nordic Dietary Pattern has no Effect on Inflammatory Markers: A Systematic Review and Meta-Analysis of Randomized Controlled Clinical Trials. Nutrition 2019, 58, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Mellberg, C.; Sandberg, S.; Ryberg, M.; Eriksson, M.; Brage, S.; Larsson, C.; Olsson, T.; Lindahl, B. Long-Term Effects of a Palaeolithic-Type Diet in Obese Postmenopausal Women: A 2-Year Randomized Trial. Eur. J. Clin. Nutr. 2014, 68, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Blomquist, C.; Alvehus, M.; Buren, J.; Ryberg, M.; Larsson, C.; Lindahl, B.; Mellberg, C.; Soderstrom, I.; Chorell, E.; Olsson, T. Attenuated Low-Grade Inflammation Following Long-Term Dietary Intervention in Postmenopausal Women with Obesity. Obesity 2017, 25, 892–900. [Google Scholar] [CrossRef] [PubMed]
- Nordic Council of Ministers. Nordic Nutrition Recommendations 2012. In Integrating Nutrition and Physical Activity, Nord 2014:002 ed.; Nordic Council of Ministers: Copenhagen, Denmark, 2014. [Google Scholar]



{kind=link}
{kind=link}
| References | Years of Data Collection | Study Design | Name of the Study | Country | Population |
|---|---|---|---|---|---|
| [22,23] | 2007 | Observational study | DILGOM | Finland | n = 4579 A representative sample of the Finnish population in 5 large study areas |
| [22,23] | 2001–2004 | Observational study | the Helsinki Birth Cohort Study | Finland | n = 1911 Helsinki University Central Hospital area |
| [22] | 2000–2001 | Observational study | Health 2000 Survey | Finland | n = 5180 A representative sample of the Finnish population from 80 health service districts |
| [20,24,30] | 2009–2010 | RCT multicenter 18–24 weeks | SYSDIET | Denmark Finland Iceland Sweden | n = 166 men and women with features of MetS mean age 55 years mean BMI 31.6 kg/m2 |
| [25,28] | 2010–2011 | RCT 26 weeks | New Nordic Diet | Denmark | n = 147 centrally obese men and women mean age 42 years mean BMI 30.2 kg/m2 |
| [26,27] | 2007–2008 | RCT 6 weeks | NORDIET | Sweden | n = 86 mildly hypercholesterolaemic men and women mean age 53 years mean BMI 26.5 kg/m2 |
| [29] | 2008–2009 | RCT 12 weeks | SYSDIMET | Finland | n = 104 men and women with features of MetS mean age 59 years mean BMI 31.1 kg/m2 |
| Reference | Study Name | Dietary Intake | Inflammatory Markers/Measurements Related to Inflammation | Main Results | |
| (A) | [23] | DILGOM study (n = 4 579); Helsinki Birth Cohort Study (n = 1911) | FFQ was used to measure dietary intake over the past year and to calculate the BSDS. | leptin, HMW-adiponectin, TNF-alfa, IL-6, and hsCRP. | An inverse association between the BSDS and hsCRP concentration in both studies (p < 0.01). No association with other inflammatory markers. In the DILGOM study HMW-adiponectin had inverse association with BSDS. |
| [22] | DILGOM (n = 4776); Health 2000 Survey (n = 5180); Helsinki Birth Cohort Study (n = 1972) | FFQ was used to measure dietary intake over the past year and to calculate the BSDS. | hsCRP | The risk of elevated hsCRP concentration was lower among men (OR 0.58, p = 0.004) and women (OR 0.73, p = 0.001) in the highest BSDS quintile than among those in the lowest BSDS quintile. | |
| Reference | Study Name | Study Groups (n) and Duration of the Intervention | Inflammatory Markers/Measurements Related to Inflammation | Main Results | |
| (B) | [24] | SYSDIET 6 study centers in Nordic countries | (1) HND (n = 96) (2) Control (average Nordic diet) (n = 70) 18–24 weeks | IL-1Ra, IL-1β, IL10, TNF RII, hsCRP | IL-1 Ra increased in the Control group. No differences between the groups in the other markers. |
| [20] | SYSDIET (3 centers out of 6) | (1) HND (n = 31) (2) Control (n = 25) 18–24 weeks | Gene expression in subcutaneous adipose tissue | Gene expression of inflammation related genes was reduced in the HND group compared with the Control group. | |
| [30] | SYSDIET (3 centers out of 6) | (1) HND (n = 42) (2) Control (n = 26) 18–24 weeks | Gene expression in peripheral blood mononuclear cells | Pathways and processes involved in the immune response were down-regulated in the HND group. | |
| [28] | New Nordic Diet | (1) NND (n = 91) (2) ADD (n = 56) 26 weeks | CRP | CRP decreased in the NND group (p = 0.007). The decrease of CRP attenuated, but remained significant after adjusting for the weight loss (p = 0.043). The loss of body weight during the intervention was greater (p < 0.001) in the NND group (~4.74 ± 0.48 kg) than in the ADD group (~1.52 ± 0.45 kg). | |
| [25] | Subset of New Nordic Diet | (1) NND (n = 43) (2) ADD (n = 21) 26 weeks | CRP, TNF-α | No significant changes in the whole population, but in women CRP concentration decreased 40% in the NDD group (p < 0.01). The model was not adjusted by weight loss. The loss of body weight during the intervention was greater in NDD than ADD (p < 0.01). | |
| [26,27] | NORDIET | (1) HND (n = 44) (2) Control (n = 42) 6 weeks | CRP, Cathepsin S | No change in CRP. Level of Cathepsin S was decreased in the HND group compared with the Control group (p = 0.003). The difference remained significant after adjusting for baseline Cathepsin S level, but not after adjusting for change in weight or LDL cholesterol concentration. | |
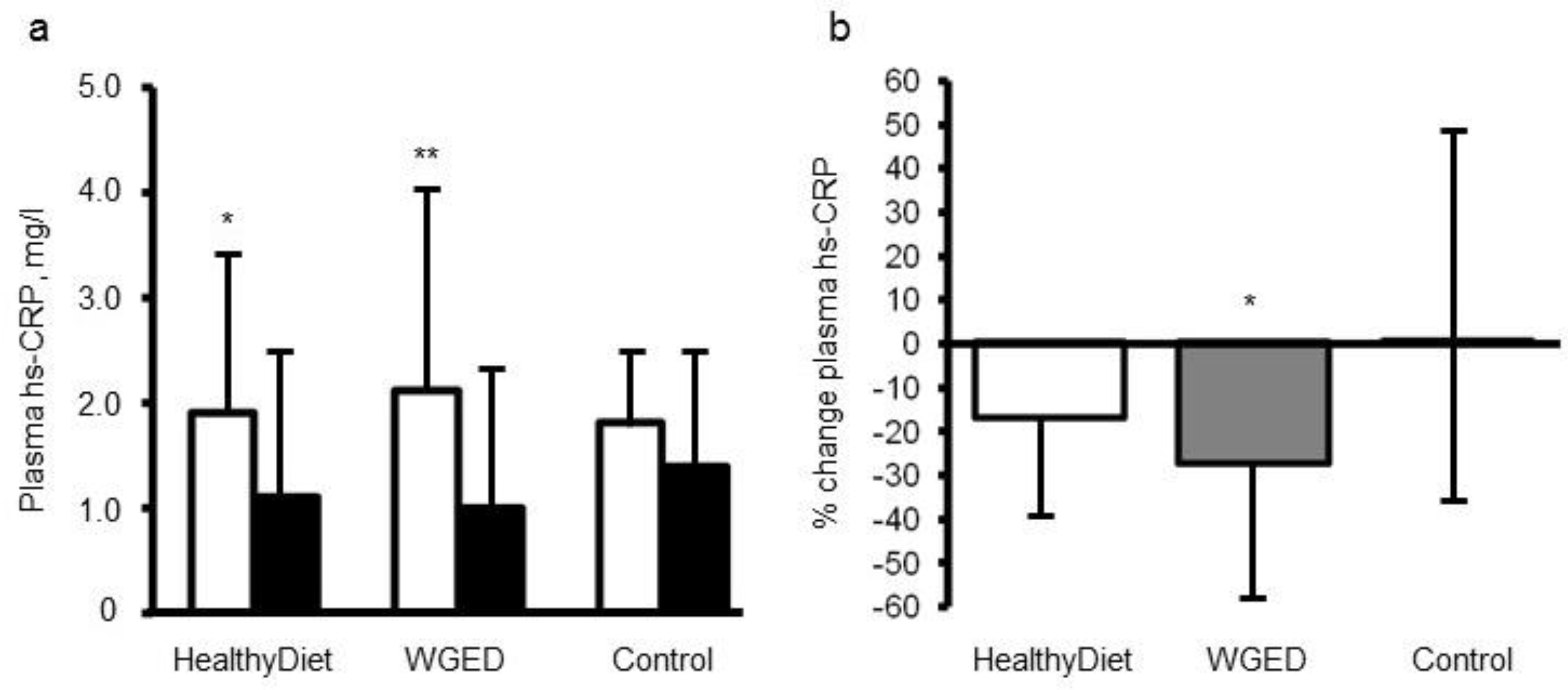
| [29] | SYSDIMET | (1) Healthy Diet rich in whole grain, fatty fish and bilberries (2) Whole Grain Enriched Diet (WGED) (3) Control Diet 12 weeks | hsCRP, TNF-α, IL-6, IL1Ra, SAA, CCL5, sICAM-1 and MIF | Plasma hsCRP concentration decreased in the WGED and Healthy Diet groups (p < 0.01 and p < 0.05, respectively) and the change in hsCRP in the WGED group was significantly different from that in the control group (p < 0.05). No changes in other inflammatory markers. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lankinen, M.; Uusitupa, M.; Schwab, U. Nordic Diet and Inflammation—A Review of Observational and Intervention Studies. Nutrients 2019, 11, 1369. https://doi.org/10.3390/nu11061369
Lankinen M, Uusitupa M, Schwab U. Nordic Diet and Inflammation—A Review of Observational and Intervention Studies. Nutrients. 2019; 11(6):1369. https://doi.org/10.3390/nu11061369
Chicago/Turabian StyleLankinen, Maria, Matti Uusitupa, and Ursula Schwab. 2019. "Nordic Diet and Inflammation—A Review of Observational and Intervention Studies" Nutrients 11, no. 6: 1369. https://doi.org/10.3390/nu11061369
APA StyleLankinen, M., Uusitupa, M., & Schwab, U. (2019). Nordic Diet and Inflammation—A Review of Observational and Intervention Studies. Nutrients, 11(6), 1369. https://doi.org/10.3390/nu11061369