A Provegetarian Food Pattern Emphasizing Preference for Healthy Plant-Derived Foods Reduces the Risk of Overweight/Obesity in the SUN Cohort

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
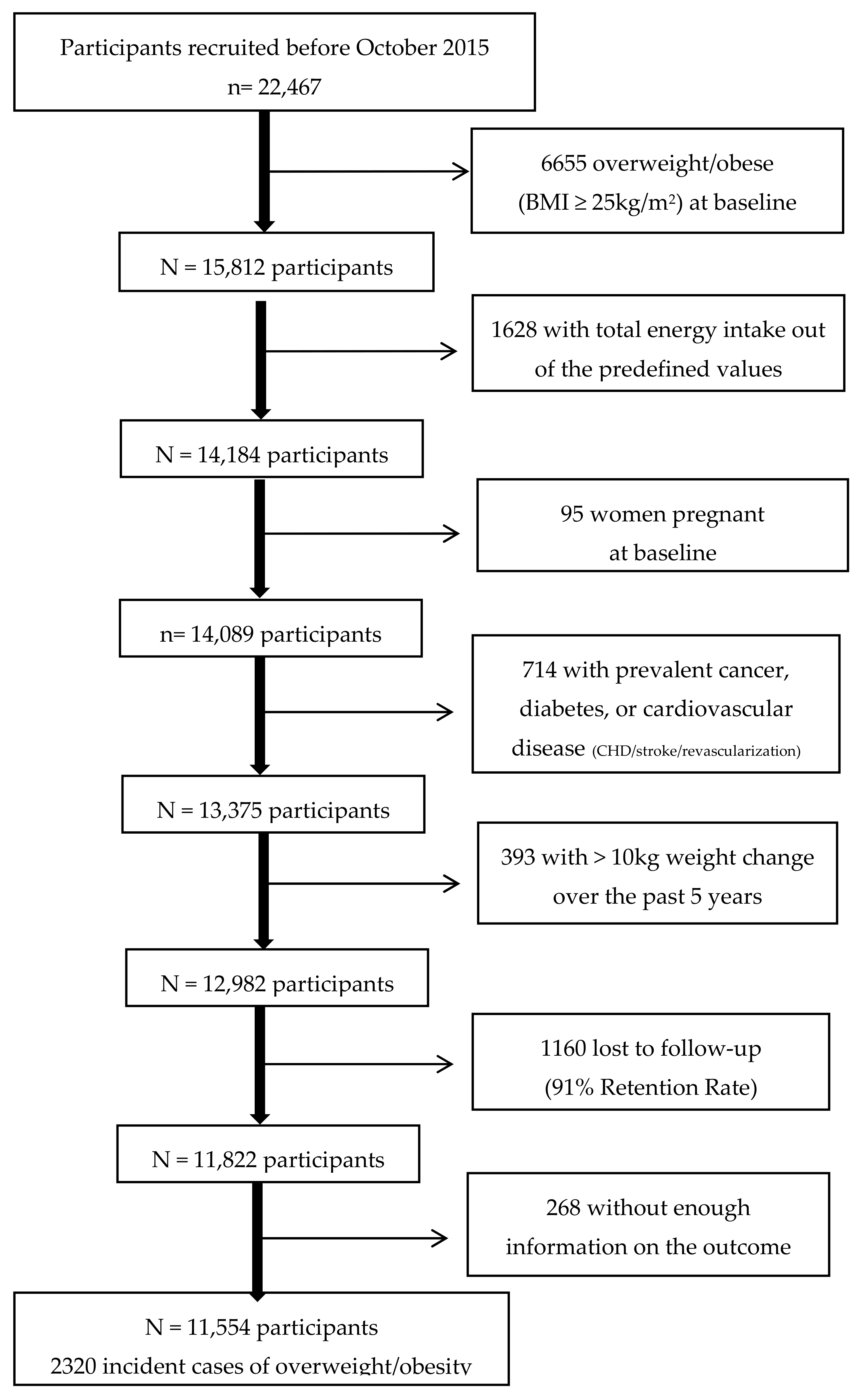
2.1. Study Population
2.2. Dietary Assessment
2.3. Other Covariates Assessment
2.4. Outcome Ascertainment
2.5. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Springmann, M.; Clark, M.; Mason-D’Croz, D.; Wiebe, K.; Bodirsky, B.; Lassaletta, L.; de Vries, W.; Vermeulen, S.; Herrero, M.; Carlson, K.; et al. Options for keeping the food system within environmental limits. Nature 2018, 562, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Godfray, H.C.J.; Aveyard, P.; Garnett, T.; Hall, J.W.; Key, T.J.; Lorimer, J.; Pierrehumber, R.T.; Scarborough, P.; Springmann, M.; Jebb, S.A. Meat consumption, health, and the environment. Science 2018, 361, 5324. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; Declerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT–Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Key, T.; Fraser, G.; Thorogood, M.; Appleby, P.; Beral, V.; Reeves, G.; Burr, M.; Chang-Claude, J.; Frentzel-Beyme, R.; Kuzma, J.; et al. Mortality in Vegetarians and Nonvegetarians: Detailed Findings from A Collaborative Analysis Of 5 Prospective Studies. Am. J. Clin. Nutr. 1999, 70, 516s–524s. [Google Scholar] [CrossRef] [PubMed]
- Fraser, G.E. Vegetarian diets: What do we know of their effects on common chronic diseases? Am. J. Clin. Nutr. 2009, 89, 1607S–1612S. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, C.T.; Temple, N.; Woodside, J.V. Vegetarian diets, low-meat diets and health: A review. Public Health Nutr. 2012, 15, 2287–2294. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Yang, B.; Zheng, J.; Li, G.; Wahlqvist, M.; Li, D. Cardiovascular disease mortality and cancer incidence in vegetarians: A meta-analysis and systematic review. Ann. Nutr. Metab. 2012, 60, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Orlich, M.; Singh, P.; Sabaté, J.; Jaceldo-Siegl, K.; Fan, J.; Knutsen, S.; Beeson, W.; Fraser, G. Vegetarian Dietary Patterns and Mortality in Adventist Health Study 2. JAMA Intern. Med. 2013, 173, 1230–1238. [Google Scholar] [CrossRef]
- Kwok, C.; Umar, S.; Myint, P.; Mamas, M.; Loke, Y. Vegetarian Diet, Seventh Day Adventists and Risk of Cardiovascular Mortality: A Systematic Review and Meta-Analysis. Int. J. Cardiol. 2014, 176, 680–686. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Sanchez-Tainta, A.; Corella, D.; Salas-Salvadó, J.; Ros, E.; Arós, F.; Gómez-Gracia, E.; Fiol, M.; Lamuela-Raventós, R.M.; Schröder, H.; et al. A provegetarian food pattern and reduction in total mortality in the Prevencion con Dieta Mediterranea (PREDIMED) study. Am. J. Clin. Nutr. 2014, 100, 320S–328S. [Google Scholar] [CrossRef]
- Chen, Z.; Zuurmond, M.; van der Schaft, N.; Nano, J.; Wijnhoven, H.; Ikram, M.; Franco, O.; Voortman, T. Plant Versus Animal Based Diets and Insulin Resistance, Prediabetes and Type 2 Diabetes: The Rotterdam Study. Eur. J. Epidemiol. 2018, 33, 883–893. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Schoufour, J.; Rivadeneira, F.; Lamballais, S.; Ikram, M.; Franco, O.; Voortman, T. Plant-Based Diet and Adiposity Over Time in A Middle-Aged and Elderly Population. Epidemiology 2018, 30, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Turner-McGrievy, G.M.; Mandes, T.; Crimarco, A. A plant-based diet for overweight and obesity prevention and treatment. J. Geriatr. Cardiol. 2017, 14, 369–374. [Google Scholar] [PubMed]
- Huang, R.Y.; Huang, C.C.; Hu, F.B.; Chavarro, J.E. Vegetarian diets and weight reduction: A meta-analysis of randomized controlled trials. J. Gen. Intern. Med. 2016, 31, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Turner-McGrievy, G.M.; Davidson, C.R.; Wingard, E.E.; Wilcox, S.; Frongillo, E.A. Comparative effectiveness of plant-based diets for weight loss: A randomized controlled trial of five different diets. Nutrition 2015, 31, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Tonstad, S.; Butler, T.; Yan, R.; Fraser, G.E. Type of vegetarian diet, body weight, and prevalence of type 2 diabetes. Diabetes Care 2009, 32, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Rosell, M.; Appleby, P.; Spencer, E.; Key, T. Weight gain over 5 years in 21 966 meat-eating, fish-eating, vegetarian, and vegan men and women in EPIC-Oxford. Int. J. Obes. 2006, 30, 1389–1396. [Google Scholar] [CrossRef] [Green Version]
- Newby, P.; Tucker, K.L.; Wolk, A. Risk of overweight and obesity among semivegetarian, lactovegetarian, and vegan women. Am. J. Clin. Nutr. 2005, 81, 1267–1274. [Google Scholar] [CrossRef]
- Spencer, E.A.; Appleby, P.N.; Davey, G.K.; Key, T.J. Diet and Body Mass Index in 38 000 EPIC-Oxford Meat-Eaters, Fish-Eaters, Vegetarians and Vegans. Int. J. Obes. 2003, 27, 728–734. [Google Scholar] [CrossRef]
- Schulz, M.; Nöthlings, U.; Hoffmann, K.; Bergmann, M.M.; Boeing, H. Identification of a food pattern characterized by high-fiber and low-fat food choices associated with low prospective weight change in the EPIC-Potsdam cohort. J. Nutr. 2005, 135, 1183–1189. [Google Scholar] [CrossRef]
- Hruby, A.; Manson, J.E.; Qi, L.; Malik, V.S.; Rimm, E.B.; Sun, Q.; Willett, W.C.; Hu, F.B. Determinants and consequences of obesity. Am. J. Public Health 2016, 106, 1656–1662. [Google Scholar] [CrossRef]
- Foreman, K.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.; Smith, A.; Tang, K.; Yuan, C.; et al. Forecasting Life Expectancy, Years of Life Lost, And All-Cause and Cause-Specific Mortality For 250 Causes of Death: Reference and Alternative Scenarios For 2016–40 For 195 Countries and Territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef]
- Satija, A.; Bhupathiraju, S.N.; Rimm, E.B.; Spiegelman, D.; Chiuve, S.E.; Borgi, L.; Willett, W.C.; Manson, J.E.; Sun, Q.; Hu, F.B. Plant-Based Dietary Patterns and Incidence of Type 2 Diabetes in US Men and Women: Results from Three Prospective Cohort Studies. PLoS Med. 2016, 13, e1002039. [Google Scholar] [CrossRef] [PubMed]
- Satija, A.; Bhupathiraju, S.; Spiegelman, D.; Chiuve, S.; Manson, J.; Willett, W.; Rexrode, K.; Rimm, E.; Hu, F.B. Healthful and Unhealthful Plant-Based Diets and The Risk of Coronary Heart Disease In, U.S. Adults. J. Am. Coll. Cardiol. 2017, 70, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Satija, A.; Malik, V.; Rimm, E.B.; Sacks, F.; Willett, W.; Hu, F.B. Changes in intake of plant-based diets and weight change: Results from 3 prospective cohort studies. Am. J. Clin. Nutr. 2019. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Caulfield, L.E.; Rebholz, C.M. Healthy Plant-Based Diets Are Associated with Lower Risk of All-Cause Mortality in US Adults. J. Nutr. 2018, 148, 624–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Caulfield, L.E.; Garcia-Larsen, V.; Steffen, L.M.; Grams, M.E.; Coresh, J.; Rebholz, C.M. Plant-Based Diets and Incident CKD and Kidney Function. Clin. J. Am. Soc. Nephrol. 2019, 14, 682–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKeown, N.; Jacobs, D. In Defence Of Phytochemical-Rich Dietary Patterns. Br. J. Nutr. 2010, 104, 1–3. [Google Scholar] [CrossRef]
- Liang, N.; Kitts, D.D. Role of Chlorogenic Acids in Controlling Oxidative and Inflammatory Stress Conditions. Nutrients 2015, 8, 16. [Google Scholar] [CrossRef]
- Cuevas-Sierra, A.; Ramos-Lopez, O.; Riezu-Boj, J.I.; Milagro, F.I.; Martinez, J.A. Diet, Gut Microbiota, and Obesity: Links with Host Genetics and Epigenetics and Potential Applications. Adv. Nutr. 2019, 10, S17–S30. [Google Scholar] [Green Version]
- Song, M.; Fung, T.; Hu, F.; Willett, W.; Longo, V.; Chan, A.; Giovannucci, E. Association of Animal and Plant Protein Intake with All-Cause and Cause-Specific Mortality. JAMA Intern. Med. 2016, 176, 1453–1463. [Google Scholar] [CrossRef] [PubMed]
- Westerterp-Plantenga, M.; Nieuwenhuizen, A.; Tomé, D.; Soenen, S.; Westerterp, K. Dietary Protein, Weight Loss, and Weight Maintenance. Annu. Rev. Nutr. 2009, 29, 21–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez-Garcia, E.; Schulze, M.; Fung, T.; Meigs, J.; Rifai, N.; Manson, J.; Hu, F. Major Dietary Patterns Are Related to Plasma Concentrations of Markers of Inflammation and Endothelial Dysfunction. Am. J. Clin. Nutr. 2004, 80, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- Watzl, B.; Kulling, S.; Möseneder, J.; Barth, S.; Bub, A. A 4-Wk Intervention with High Intake of Carotenoid-Rich Vegetables and Fruit Reduces Plasma C-Reactive Protein in Healthy, Nonsmoking Men. Am. J. Clin. Nutr. 2005, 82, 1052–1058. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Griffith, J.A.; Chasan-Taber, L.; Olendzki, B.C.; Jackson, E.; Stanek, E.J.; Li, W.; Pagoto, S.L.; Hafner, A.R.; Ockene, I.S. Association between dietary fiber and serum C-reactive protein. Am. J. Clin. Nutr. 2006, 83, 760–766. [Google Scholar] [CrossRef]
- Hermsdorff, H.H.; Zulet, M.; Puchau, B.; Martínez, J.A. Fruit and vegetable consumption and proinflammatory gene expression from peripheral blood mononuclear cells in young adults: A translational study. Nutr. Metab. 2010, 7, 42. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Legarrea, P.; Iglesia, R.D.L.; Abete, I.; Navas-Carretero, S.; Martinez, J.A.; Zulet, M.A. The protein type within a hypocaloric diet affects obesity-related inflammation: The RESMENA project. Nutrition 2014, 30, 424–429. [Google Scholar] [CrossRef]
- Carlos, S.; Fuente-Arrillaga, C.; Bes-Rastrollo, M.; Razquin, C.; Rico-Campà, A.; Martínez-González, M.A.; Ruiz-Canela, M. Mediterranean Diet and Health Outcomes in the SUN Cohort. Nutrients 2018, 10, 439. [Google Scholar] [CrossRef]
- De la Fuente-Arrillaga, C.; Ruiz, Z.V.; Bes-Rastrollo, M.; Sampson, L.; Martinez-González, M.A. Reproducibility of an FFQ validated in Spain. Public Health Nutr. 2010, 13, 1364–1372. [Google Scholar] [CrossRef]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and validation of a food frequency questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef]
- Mataix, J. Tabla de Composición de Alimentos, 5th ed.; Universidad de Granada: Granada, Spain, 2009. [Google Scholar]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Los Alimentos; de Prácticas, G., Ed.; Pirámide: Madrid, Spain, 2015. [Google Scholar]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2595–2596. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; López-Fontana, C.; Varo, J.J.; Sánchez-Villegas, A.; Martinez, J.A. Validation of the Spanish version of the physical activity questionnaire used in the Nurses’ Health Study and the Health Professionals’ Follow-up Study. Public Health Nutr. 2005, 8, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Zazpe, I.; Sánchez-Taínta, A.; Santiago, S.; Fuente-Arrillaga, C.D.L.; Bes-Rastrollo, M.; Martínez, J.A.; Martínez-González, M.A. Association between dietary carbohydrate intake quality and micronutrient intake adequacy in a Mediterranean cohort: The SUN (Seguimiento Universidad de Navarra) Project. Br. J. Nutr. 2014, 111, 2000–2009. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Tainta, A.; Zazpe, I.; Bes-Rastrollo, M.; Salas-Salvado, J.; Bullo, M.; Sorli, J.V.; Corella, D.; Covas, M.I.; Arós, F.; Gutierrez-Bedmar, M.; et al. Nutritional adequacy according to carbohydrates and fat quality. Eur. J. Nutr. 2016, 55, 93–106. [Google Scholar] [CrossRef] [PubMed]
- Bes-Rastrollo, M.; Pérez, J.R.; Sánchez-Villegas, A.; Alonso, A.; Martínez-González, M.A. Validation of self-reported weight and body mass index in a cohort of university graduates in Spain. Rev. Esp. Obes. 2005, 3, 352–358. [Google Scholar]
- Mozaffarian, D. Dietary and Policy Priorities for Cardiovascular Disease, Diabetes, and Obesity: A Comprehensive Review. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef]
- Silveira, J.A.C.D.; Meneses, S.S.; Quintana, P.T.; Santos, V.D.S. Association between Overweight and Consumption of Ultra-Processed Food and Sugar-Sweetened Beverages among Vegetarians. Rev. Nutr. 2017, 30, 431–441. [Google Scholar] [CrossRef]
- Bertoia, M.L.; Rimm, E.B.; Mukamal, K.J.; Hu, F.B.; Willett, W.C.; Cassidy, A. Dietary Flavonoid Intake and Weight Maintenance: Three Prospective Cohorts of 124 086 US Men and Women Followed for up to 24 Years. BMJ 2016, 352, i17. [Google Scholar] [CrossRef]
- Santiago, S.; Zazpe, I.; Bes-Rastrollo, M.; Sánchez-Tainta, A.; Sayón-Orea, C.; Fuente-Arrillaga, C.D.L.; Benito, S.; Martínez, J.A.; Martínez-González, M.Á. Carbohydrate Quality, Weight Change and Incident Obesity in a Mediterranean Cohort: The SUN Project. Eur. J. Clin. Nutr. 2014, 69, 297–302. [Google Scholar] [CrossRef]
- Barbaresko, J.; Koch, M.; Schulze, M.B.; Nöthlings, U. Dietary Pattern Analysis and Biomarkers of Low-Grade Inflammation: A Systematic Literature Review. Nutr. Rev. 2013, 71, 511–527. [Google Scholar] [CrossRef] [PubMed]
- Ramallal, R.; Toledo, E.; Martínez, J.A.; Shivappa, N.; Hébert, J.R.; Martínez-González, M.A.; Ruiz-Canela, M. Inflammatory Potential of Diet, Weight Gain, and Incidence of Overweight/Obesity: The SUN Cohort. Obesity 2017, 25, 997–1005. [Google Scholar] [CrossRef] [PubMed]
- Fresán, U.; Martínez-González, M.A.; Sabaté, J.; Bes-Rastrollo, M. Global Sustainability (Health, Environment and Monetary Costs) of Three Dietary Patterns: Results from a Spanish Cohort (the SUN Project). BMJ Open 2019, 9, e021541. [Google Scholar] [CrossRef] [PubMed]
- Hekler, E.B.; Gardner, C.D.; Robinson, T.N. Effects of a College Course About Food and Society on Students Eating Behaviors. Am. J. Prev. Med. 2010, 38, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.A.; Kraak, V.I.; Allender, S.; Atkins, V.J.; Baker, P.I.; Bogard, J.R.; Brinsden, H.; Calvillo, A.; Schutter, O.D.; Devarajan, R.; et al. The Global Syndemic of Obesity, Undernutrition, and Climate Change: The Lancet Commission Report. Lancet 2019, 393, 791–846. [Google Scholar] [CrossRef]
- Rothman, K.J. Epidemiology: An Introduction, 2nd ed.; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Rothman, K.J.; Gallacher, J.E.; Hatch, E.E. Why representativeness should be avoided. Int. J. Epidemiol. 2013, 42, 1012–1014. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Provegetarian Food Pattern (Potential Range of 12–60) | Healthful/Unhealthful Provegetarian Food Patterns (Potential Range of 18–90) | |||
|---|---|---|---|---|
| Component | Criteria | Component | Criteria | |
| Plant food Groups | Energy-Adjusted Quintiles | Plant Food Groups | Energy-Adjusted Quintiles | |
| Healthy | Healthful | Unhealthful | ||
| 1. Vegetables | Positive | 1. Vegetables | Positive | Reverse |
| 2. Fruits | Positive | 2. Fruits | Positive | Reverse |
| 3. Legumes | Positive | 3. Legumes | Positive | Reverse |
| 4. Cereal grains | Positive | 4. Whole grains | Positive | Reverse |
| 5. Potatoes | Positive | 5. Nuts | Positive | Reverse |
| 6. Nuts | Positive | 6. Olive oil | Positive | Reverse |
| 7. Olive oil | Positive | 7. Coffee | Positive | Reverse |
| Less-healthy | ||||
| Animal Food Groups | 8. Fruit juices | Reverse | Positive | |
| 8. Dairy | Reverse | 9. Potatoes | Reverse | Positive |
| 9. Eggs | Reverse | 10. Refined grains | Reverse | Positive |
| 10. Meat | Reverse | 11. Sugary beverages | Reverse | Positive |
| 11. Fish & seafood | Reverse | 12. Pastries | Reverse | Positive |
| 12. Animal fat | Reverse | Animal Food Groups | ||
| 13. Dairy | Reverse | Reverse | ||
| 14. Eggs | Reverse | Reverse | ||
| 15. Meat | Reverse | Reverse | ||
| 16. Fish & seafood | Reverse | Reverse | ||
| 17. Miscellaneous food | Reverse | Reverse | ||
| 18. Animal fat | Reverse | Reverse | ||
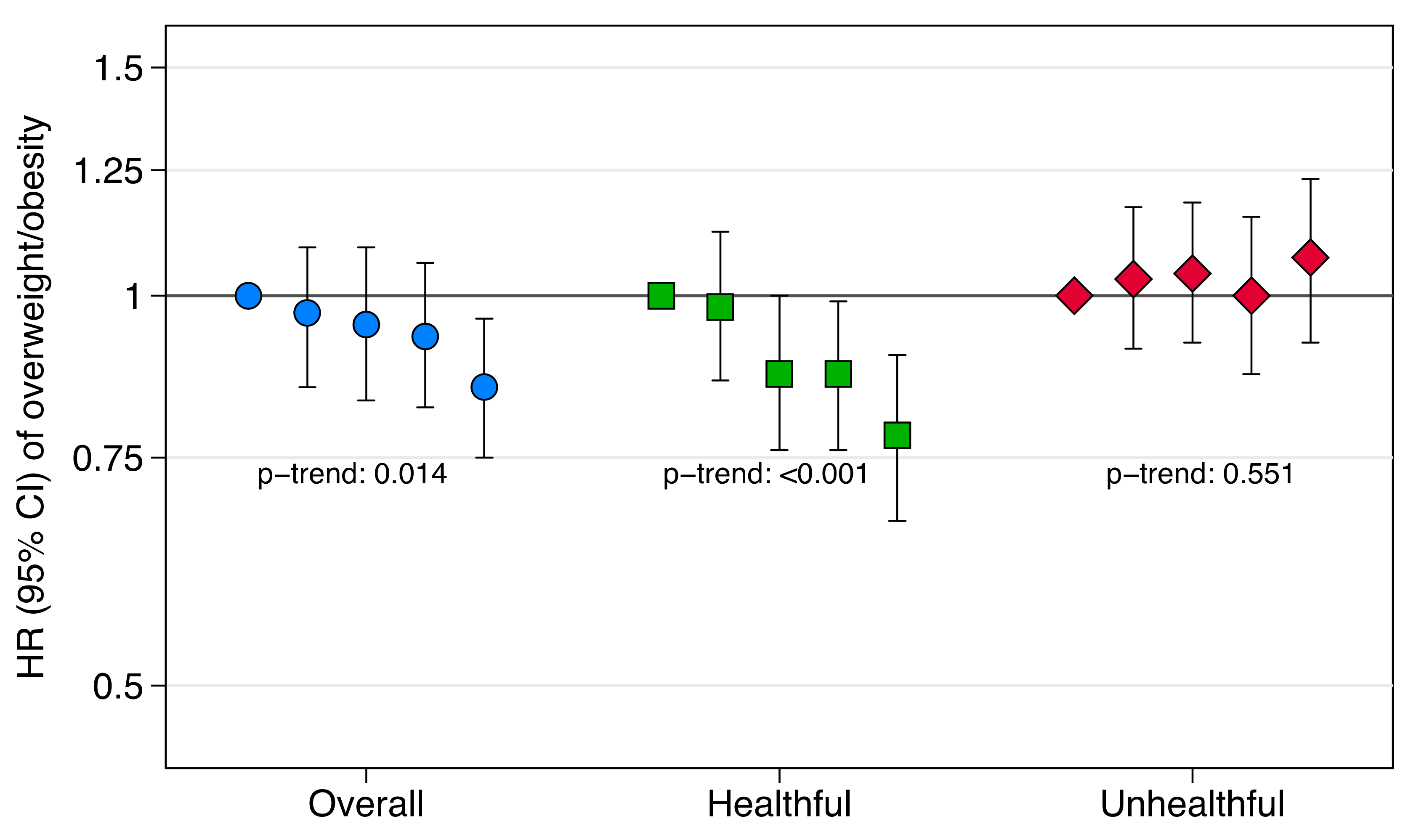
| Provegetarian FP | Q1 | Q2 | Q3 | Q4 | Q5 | p-Trend | z-Continuous 2 |
|---|---|---|---|---|---|---|---|
| Cases/Person-years | 622/29,366 | 494/24,015 | 358/17,697 | 429/20,395 | 417/21,740 | 2320/113,213 | |
| Age-and sex-adjusted | 1 (ref) | 0.97 (0.86 to 1.10) | 0.93 (0.82 to 1.06) | 0.94 (0.83 to 1.06) | 0.77 (0.68 to 0.88) | <0.001 | 0.83 (0.77 to 0.90) |
| Repeated measures | 1 (ref) | 0.98 (0.87 to 1.10) | 0.92 (0.81 to 1.05) | 0.94 (0.83 to 1.07) | 0.76 (0.67 to 0.86) | <0.001 | 0.82 (0.75 to 0.88) |
| Multivariable-adjusted 1 | 1 (ref) | 0.97 (0.85 to 1.09) | 0.95 (0.83 to 1.09) | 0.93 (0. 82 to1.06) | 0.85 (0.75 to 0.96) | 0.014 | 0.89 (0.82 to 0.97) |
| Repeated measures | 1 (ref) | 0.98 (0.87 to 1.11) | 0.94 (0.83 to 1.08) | 0.94 (0. 83 to1.06) | 0.83 (0.73 to 0.95) | 0.005 | 0.88 (0.81 to 0.95) |
| Healthful Provegetarian FP | |||||||
| Cases/Person-years | 490/24,576 | 52 8/24,878 | 413/19,903 | 516/25,293 | 373/18,563 | 2320/113,213 | |
| Age-and sex-adjusted | 1 (ref) | 0.99 (0.87 to 1.12) | 0.95 (0.84 to 1.09) | 0.89 (0.79 to 1.01) | 0.81 (0.71 to 0.93) | 0.001 | 0.87 (0.80 to 0.94) |
| Repeated measures | 1 (ref) | 0.99 (0.88 to 1.12) | 0.94 (0.82 to 1.07) | 0.92 (0.81 to 1.04) | 0.80 (0.70 to 0.92) | 0.001 | 0.87 (0.80 to 0.94) |
| Multivariable-adjusted 1 | 1 (ref) | 0.98 (0.86 to 1.12) | 0.87 (0.76 to 1.00) | 0.87 (0.76 to 0.99) | 0.78 (0.67 to 0.90) | <0.001 | 0.84 (0.77 to 0.92) |
| Repeated measures | 1 (ref) | 0.98 (0.86 to 1.11) | 0.85 (0.74 to 0.97) | 0.89 (0.78 to 1.01) | 0.76 (0.66 to 0.88) | <0.001 | 0.84 (0.77 to 0.92) |
| Unhealthful Provegetarian FP | |||||||
| Cases/Person-years | 544/23,243 | 516/24,135 | 514/25,004 | 388/20,549 | 358/20,282 | 2320/113,213 | |
| Age-and sex-adjusted | 1 (ref) | 0.94 (0.83 to 1.06) | 0.93 (0.82 to 1.05) | 0.88 (0.77 to 1.00) | 0.84 (0.73 to 0.96) | 0.006 | 0.88 (0.81 to 0.96) |
| Repeated measures | 1 (ref) | 0.95 (0.85 to 1.08) | 0.92 (0.81 to 1.04) | 0.87 (0.76 to 0.99) | 0.86 (0.75 to 0.99) | 0.012 | 0.88 (0.81 to 0.96) |
| Multivariable-adjusted 1 | 1 (ref) | 1.03 (0.91 to 1.17) | 1.04 (0.92 to 1.18) | 1.00 (0.87 to 1.15) | 1.07 (0.92 to 1.23) | 0.551 | 1.00 (0.91 to 1.10) |
| Repeated measures | 1 (ref) | 1.04 (0.92 to 1.17) | 1.03 (0.91 to 1.16) | 0.99 (0.86 to 1.13) | 1.09 (0.94 to 1.26) | 0.416 | 1.01 (0.92 to 1.10) |
| Provegetarian FP | ||||||
|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | p-Trend | |
| Absolute Yearly Weight Change (g), Adjusted Mean 1 | 401 (343 to 460) | 413 (344 to 481) | 343 (280 to 405) | 274 (212 to 336) | ||
| Age-and Sex-Adjusted Differences Versus Q1 | 0 (ref) | −52 (−132 to 27) | -43 (-131 to 44) | −112 (−195 to −30) | −164 (−246 to −81) | <0.001 |
| Multivariable-Adjusted Differences Versus Q1 1 | 0 (ref) | −39 (−118 to 39) | −28 (−115 to 58) | −98 (−181 to −16) | −167 (−249 to −84) | <0.001 |
| Updated Provegetarian FP (repeated measures) | ||||||
| Absolute Yearly Weight Change (g), Adjusted Mean 1 | 367 (321 to 413) | 361 (310 to 411) | 342 (282 to 402) | 302 (251 to 352) | 221 (168 to 274) | |
| Multivariable-Adjusted Differences Versus Q1 (GEE) 2 | 0 (ref) | −6 (−70 to 57) | −26 (−96 to 45) | −65 (−133 to 2) | −146 (−214 to -78) | <0.001 |
| Healthful Provegetarian FP | ||||||
| Absolute Yearly Weight Change (g), Adjusted Mean 1 | 472 (413 to 531) | 416 (359 to 473) | 347 (283 to 411) | 355 (297 to 411) | 270 (203 to 338) | |
| Age-and Sex-Adjusted Differences Versus Q1 | 0 (ref) | −69 (−151 to 13) | −134 (−221 to −46) | −123 (−206 to −40) | −198 (−289 to −107) | <0.001 |
| Multivariable-adjusted differences versus Q1 1 | 0 (ref) | −56 (−138 to 26) | −125 (−212 to −38) | −117 (−200 to −35) | −202 (−294 to −110) | <0.001 |
| Updated Healthful Provegetarian FP (repeated measures) | ||||||
| Absolute Yearly Weight Change (g), Adjusted Mean 1 | 416 (367 to 465) | 342 (295 to 390) | 285 (233 to 337) | 321 (273 to 370) | 216 (160 to 271) | |
| Multivariable-Adjusted Differences versus Q1 (GEE) 2 | 0 (ref) | −73 (−139 to−7) | −130 (−201 to−61) | −94 (−163 to −26) | −200 (−275 to −125) | <0.001 |
| Unhealthful Provegetarian FP | ||||||
| Absolute Yearly Weight Change (g), Adjusted Mean 1 | 365 (306 to 425) | 346 (288 to 404) | 401 (343 to 458) | 393 (330 to 457) | 387 (320 to 455) | |
| Age-and Sex-Adjusted Differences Versus Q1 | 0 (ref) | −11 (−93 to 71) | 50 (−32 to 133) | 38 (−49 to 124) | 51 (−37 to 139) | 0.149 |
| Multivariable-Adjusted Differences Versus Q1 1 | 0 (ref) | −19 (−101 to 62) | 35 (−47 to 118) | 28 (−60 to 116) | 22 (−70 to 114) | 0.434 |
| Updated Unhealthful Provegetarian FP (repeated measures) | ||||||
| Absolute Yearly Weight Change (g), Adjusted Mean 1 | 306 (256 to 355) | 303 (254 to 351) | 334 (287 to 381) | 330 (278 to 382) | 338 (283 to 393) | |
| Multivariable-Adjusted Differences Versus Q1 (GEE) 2 | 0 (ref) | −3 (−70 to 64) | 28 (−39 to 96) | 24 (−47 to 96) | 32 (−43 to 108) | 0.324 |
| Provegetarian FP | Q1 | Q2 | Q3 | Q4 | Q5 | p-Trend | z-Continuous 2 |
|---|---|---|---|---|---|---|---|
| Cases/Person-years | 178/9650 | 162/8178 | 96/5655 | 126/7693 | 107/8288 | 2320/113,213 | |
| Age-and sex-adjusted | 1 (ref) | 1.06 (0.86 to 1.32) | 0.93 (0.72 to 1.20) | 0.90 (0.72 to 1.14) | 0.71 (0.55 to 0.90) | 0.003 | 0.78 (0.67 to 0.91) |
| Repeated measures | 1 (ref) | 1.06 (0.86 to 1.32) | 0.86 (0.67 to 1.12) | 0.92 (0.73 to 1.16) | 0.74 (0.58 to 0.94) | 0.007 | 0.80 (0.68 to 0.93) |
| Multivariable-adjusted 1 | 1 (ref) | 1.09 (0.87 to 1.36) | 0.91 (0.70 to 1.18) | 0.96 (0.75 to 1.23) | 0.79 (0.61 to 1.02) | 0.056 | 0.82 (0.69 to 0.98) |
| Repeated measures | 1 (ref) | 1.03 (0.83 to 1.29) | 0.83 (0.64 to 1.08) | 0.97 (0.77 to 1.24) | 0.83 (0.65 to 1.07) | 0.123 | 0.85 (0.72 to 1.01) |
| Healthful Provegetarian FP | |||||||
| Cases/Person-years | 141/7423 | 139/7876 | 135/6808 | 149/9846 | 105/7510 | 2320/113,213 | |
| Age-and sex-adjusted | 1 (ref) | 0.95 (0.75 to 1.20) | 1.04 (0.82 to 1.32) | 0.80 (0.63 to 1.01) | 0.73 (0.56 to 0.95) | 0.006 | 0.79 (0.68 to 0.93) |
| Repeated measures | 1 (ref) | 0.98 (0.77 to 1.23) | 1.05 (0.83 to 1.33) | 0.78 (0.62 to 0.99) | 0.74 (0.57 to 0.96) | 0.004 | 0.79 (0.68 to 0.92) |
| Multivariable-adjusted 1 | 1 (ref) | 0.93 (0.73 to 1.20) | 1.03 (0.80 to 1.33) | 0.86 (0.67 to 1.10) | 0.79 (0.59 to 1.05) | 0.066 | 0.87 (0.73 to 1.04) |
| Repeated measures | 1 (ref) | 0.94 (0.74 to 1.21) | 1.04 (0.81 to 1.34) | 0.82 (0.64 to 1.05) | 0.79 (0.60 to 1.03) | 0.036 | 0.86 (0.73 to 1.02) |
| Unhealthful Provegetarian FP | |||||||
| Cases/Person-years | 179/9930 | 143/8761 | 144/8338 | 108/6443 | 95/5991 | 2320/113,213 | |
| Age-and sex-adjusted | 1 (ref) | 0.93 (0.74 to 1.16) | 0.99 (0.79 to 1.24) | 0.93 (0.73 to 1.19) | 0.87 (0.68 to 1.11) | 0.305 | 0.92 (0.78 to 1.07) |
| Repeated measures | 1 (ref) | 0.92 (0.74 to 1.14) | 0.97 (0.78 to 1.21) | 0.90 (0.70 to 1.15) | 0.86 (0.67 to 1.11) | 0.256 | 0.92 (0.78 to 1.08) |
| Multivariable-adjusted 1 | 1 (ref) | 1.12 (0.90 to 1.40) | 1.05 (0.83 to 1.32) | 1.03 (0.80 to 1.33) | 0.96 (0.73 to 1.26) | 0.763 | 0.96 (0.81 to 1.14) |
| Repeated measures | 1 (ref) | 1.12 (0.90 to 1.39) | 1.04 (0.83 to 1.31) | 1.02 (0.79 to 1.30) | 0.95 (0.73 to 1.25) | 0.698 | 0.97 (0.82 to 1.15) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Donoso, C.; Martínez-González, M.Á.; Martínez, J.A.; Gea, A.; Sanz-Serrano, J.; Perez-Cueto, F.J.A.; Bes-Rastrollo, M. A Provegetarian Food Pattern Emphasizing Preference for Healthy Plant-Derived Foods Reduces the Risk of Overweight/Obesity in the SUN Cohort. Nutrients 2019, 11, 1553. https://doi.org/10.3390/nu11071553
Gómez-Donoso C, Martínez-González MÁ, Martínez JA, Gea A, Sanz-Serrano J, Perez-Cueto FJA, Bes-Rastrollo M. A Provegetarian Food Pattern Emphasizing Preference for Healthy Plant-Derived Foods Reduces the Risk of Overweight/Obesity in the SUN Cohort. Nutrients. 2019; 11(7):1553. https://doi.org/10.3390/nu11071553
Chicago/Turabian StyleGómez-Donoso, Clara, Miguel Ángel Martínez-González, J. Alfredo Martínez, Alfredo Gea, Julen Sanz-Serrano, Federico J. A. Perez-Cueto, and Maira Bes-Rastrollo. 2019. "A Provegetarian Food Pattern Emphasizing Preference for Healthy Plant-Derived Foods Reduces the Risk of Overweight/Obesity in the SUN Cohort" Nutrients 11, no. 7: 1553. https://doi.org/10.3390/nu11071553
APA StyleGómez-Donoso, C., Martínez-González, M. Á., Martínez, J. A., Gea, A., Sanz-Serrano, J., Perez-Cueto, F. J. A., & Bes-Rastrollo, M. (2019). A Provegetarian Food Pattern Emphasizing Preference for Healthy Plant-Derived Foods Reduces the Risk of Overweight/Obesity in the SUN Cohort. Nutrients, 11(7), 1553. https://doi.org/10.3390/nu11071553