Abstract
Vitamin D plays a pivotal role in bone homeostasis and calcium metabolism. However, recent research has indicated additional beneficial effects of vitamin D on the cardiovascular system. This review aims to elucidate if vitamin D can be used as an add-on treatment in coronary artery disease (CAD). Large-scale epidemiological studies have found a significant inverse association between serum 25(OH)-vitamin D levels and the prevalence of essential hypertension. Likewise, epidemiological data have suggested plasma levels of vitamin D to be inversely correlated to cardiac injury after acute myocardial infarction (MI). Remarkably, in vitro trials have showed that vitamin D can actively suppress the intracellular NF-κB pathway to decrease CAD progression. This is suggested as a mechanistic link to explain how vitamin D may decrease vascular inflammation and atherosclerosis. A review of randomized controlled trials with vitamin D supplementation showed ambiguous results. This may partly be explained by heterogeneous study groups. It is suggested that subgroups of diabetic patients may benefit more from vitamin D supplementation. Moreover, some studies have indicated that calcitriol rather than cholecalciferol exerts more potent beneficial effects on atherosclerosis and CAD. Therefore, further studies are required to clarify these assumptions.
1. Introduction
Cardiovascular disease (CVD) is a major concern of global health. According to the World Health Organization (WHO), CVD is the most common cause of mortality worldwide. Approximately 17.9 million people died from CVD in 2015, with 7.3 million of these deaths due to coronary artery disease (CAD) [1]. Although CAD is formerly considered a disease mediated by lipid accumulation, its pathophysiology is complex, and the exact underlying mechanisms are still unknown. More recent investigations have suggested an additional excessive inflammatory response in the subintimal arterial space followed by thrombus formation [2,3]. Furthermore, several studies have found that blood microparticle levels are elevated in individuals with CAD [4,5]. Different molecules on the surface of the microparticles mediate procoagulant properties that may lead to an acute coronary event [6].
In 2016, the prevalence of CAD in Denmark was estimated to be approximately 160,000 people [7]. Interestingly, new data suggest that vitamin D is a potentially cost-effective treatment agent for CAD [8]. This review will focus on relevant studies in order to investigate whether vitamin D supplementation may exert beneficial effects on atherosclerosis and CAD.
2. Literature Search and Investigation
Studies included in this review met the following criteria: participants were adults (>18 years); measured endpoints included risk of myocardial infarction (MI), mortality, plaque burden, CAD events, pulse wave velocity (PWV), adhesion molecules, blood lipids, high-sensitive C-reactive protein (hsCRP) and/or SYNTAX score. Only data from randomized clinical trial (RCT) studies in the publication period from 1 January 2010 to 12 October 2019 were assessed. Only English-language studies that were completed with available results were included. Studies with only stroke or heart failure (HF) as the CVD endpoints were excluded. Moreover, studies with cohorts consisting only of chronic kidney disease (CKD) patients were excluded. The intervention arm was administered calcitriol, cholecalciferol or ergocalciferol.
To prepare the literature review, the following databases were used: PubMed (https://www.ncbi.nlm.nih.gov/pubmed/), Clinicaltrials.gov (https://clinicaltrials.gov/) and Scopus (https://www.scopus.com). Search items were (‘Coronary Artery Disease’[Mesh] OR ‘Myocardial Infarction’[Mesh]) AND (‘Vitamin D’[Mesh] OR ‘Cholecalciferol’[Mesh]) AND (Clinical Trial[ptyp]), or (‘Vitamin D’[Mesh] OR ‘Cholecalciferol’[Mesh] AND ‘Heart Failure’[Mesh]) AND (‘Myocardial Infarction’[Mesh]), which were applied to the databases to identify studies. A search for ‘Vitamin D’ yielded 81,299 items, ‘Coronary artery disease’ yielded 163,605 items and ‘Vitamin D AND coronary artery disease’ yielded 155 items in PubMed (20 October 2019). There were 927 studies identified in Scopus after performing a search for ‘Coronary artery disease’ OR ‘Myocardial infarction’ AND ‘Vitamin D’ within the time period 1 January 2010 until 12 October 2019. Figure 1 illustrates the flowchart of the study selection.
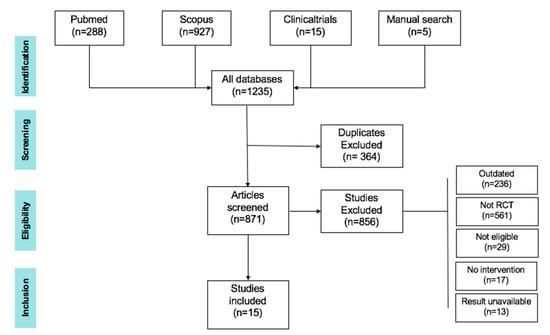
Figure 1.
Flowchart of study selection for this review.
In order to determine whether vitamin D can reduce vascular inflammation and atherosclerosis by suppression of the NF-κB pathway and be used as a potential treatment agent for CAD in patients with hypovitaminosis D, this review will define CAD and its risk factors, pathophysiology, symptoms and treatment. Next, the physiological role of vitamin D will be described. This review will investigate if vitamin D can be used as a prognostic marker of CAD risk. Finally, the potential role of vitamin D in cardiomyocytes after MI and possible cardioprotective mechanisms will be elucidated.
3. Coronary Artery Disease
CAD is an overall group of clinical conditions including stable angina, unstable angina, myocardial infarction (MI) and sudden death [9]. Important complications are heart failure and arrhythmia. The symptoms of CAD are the result of an inadequate blood supply of the heart caused by the obstruction of a coronary artery. MI is the most common manifestation of CAD and is due to the disruption of a vulnerable atherosclerotic plaque or the erosion of the coronary artery endothelium. Upon rupture, the atherosclerotic plaque releases thrombogenic contents, initiating a coagulation cascade. This hypercoagulable state could especially contribute to the rupture of additional vulnerable fibroatheromas leading to more than one culprit lesion. MI finally ends in an irreversible necrosis of myocardial cells that is detectable by an elevation of cardiac biomarkers [10,11].
3.1. Pathophysiology of Atherosclerosis
The underlying mechanisms of atherosclerosis can be divided into two parts: formation of a stable plaque and transition into an unstable plaque. The first process involves endothelial erosion with endothelial activation and denudation [12]. This endothelial dysfunction results in the deposit of low-density lipoprotein (LDL) molecules in the vascular intima [13], which leads to the formation of fatty streaks and eventually stable plaques. Lipoxygenases and myeloperoxidases oxidize the LDL molecules in the vessel wall. This oxidation attracts and stimulates activated macrophages [12]. These macrophages may induce apoptosis of endothelial cells and form a thin fibrous plaque cap that separates the lipid core from the lumen. The plaque consists of degraded smooth muscle cells, endothelial cells, foam cells, cellular debris, lymphocytes and modified lipids [14]. This mechanism is referred to as atherosclerosis and causes a gradual narrowing of the lumen. Atherosclerosis is considered to be a chronic inflammatory process in the vessel wall [15].
Subsequently, atherosclerosis may be followed by rupture of the vulnerable plaque cap. This exposes the lipid core to the vessel lumen. The atheromatous mass is now thrombogenic and causes platelet activation and finally coronary occlusion [16]. Coronary artery narrowing or occlusion may cause the symptoms of angina due to the onset of ischemia.
3.2. CAD Symptoms
The CAD symptom spectrum of angina can manifest itself in multiple ways. According to the European Society of Cardiology (ESC) [17], the typical symptoms include discomfort, pain, nausea, fatigue, restlessness, burning, shortness of breath and uncomfortable chest pressure. The sensation of discomfort is most often located at the chest or near the sternum. However, this pain may also be localized between shoulder blades, at the jaw, teeth, in either arm or at the wrist and fingers. In most cases, the pain has a duration of ≤ 10 min and is triggered by physical exercise. Table 1 shows the typical characteristics of pain due to CAD.

Table 1.
Characteristics of coronary artery disease (CAD) symptoms, modified from [17].
3.3. CAD Prognosis
A serious complication to acute MI is the progression of heart failure (HF) with reduced function of the left ventricle (LV) [18]. The estimated risk of LV systolic dysfunction after MI is about 40% [19]. Pathogenesis is partly based upon excessive β-adrenergic activation post-MI. This mechanism is complex and promotes cardiomyocyte growth, vasoconstriction and cardiac injury. Subsequently, this might lead to cardiac remodeling and LV dysfunction [20].
3.4. Diagnosis of CAD
A thorough prior diagnosis is crucial. This section gives an overview of basic test procedures in patients with suspected diagnosis of CAD. Table 2 depicts some of the useful procedures in diagnosis of CAD.
Table 2.
Diagnostic tools for the diagnosis of CAD.
3.5. Current Treatment Options of CAD
Treatment of CAD must focus on both acute treatment and secondary prophylaxis. Smoking, physical inactivity, high body mass index (BMI), diabetes mellitus, hypertension, excessive dietary fat and genetic dispositions are some of the known risk factors associated with CAD [26]. They all contribute to the lifelong atherosclerotic process and increase the risk of ischemic events. Thus, public health approaches with a focus on smoking cessation, healthy diet, stress reduction, physical exercise and antihypertensive treatment are of great importance [16]. In addition, Ornish et al. [27] showed a 7.9% relative reduction of coronary artery stenosis after five years with the intensive lifestyle interventions mentioned above.
The pharmaceutical treatment of CAD aims to reduce CVD and improve survival. More drug classes can be included in the treatment regimen. Table 3 illustrates an overview of drugs used in the treatment of CAD.
Table 3.
Overview of medications used for CAD.
Favaloro et al. (1971) [39] were the first to describe surgical techniques with vein grafts in acute MI patients to re-establish blood supply to the myocardium. Since then, great progress has been made in order to improve survival in acute coronary syndrome (ACS) patients.
- Percutaneous coronary intervention (PCI): The PCI procedure is an effective strategy for revascularization in CAD patients with both acute and stable forms. The intervention is performed by inserting a guidewire catheter into the femoral or radial artery. The guidewire is guided to the coronary artery, where the thrombosis is located. Here, a balloon is inflated, and, for example, a metallic stent might be inserted in order to prevent reinfarction. Stents can either be bare metal or drug-eluting (everolimus, zotarolimus, etc.) to minimize restenosis [17,40]. In principle, PCI is the preferred procedure in patients with ST-segment elevation myocardial infarction (STEMI) within 12 h of symptom onset [41]. In addition, patients with non-ST-segment elevation myocardial infarction (NSTEMI) might be offered PCI within 48 h of symptom onset if no relevant comorbidity is present.
- Coronary artery bypass grafting (CABG): The CAGB procedure is considered more invasive compared to PCI. The procedure includes bypassing stenosed coronary arteries [42]. Thus, vein or artery grafts are used to anastomose occluded vessels. According to the SYNTAX study, the CABG strategy is preferable in more complex multivessel occlusions [43].
4. Vitamin D
Vitamin D is mainly synthesized endogenously, when the skin is exposed to ultraviolet radiation from sunlight. Since Askew et al. [44] first isolated vitamin D in 1932, much knowledge has been gained to understand the functions of this vitamin.
4.1. Vitamin D Metabolism
The active form of vitamin D (named 1,25(OH)2D3) is based upon a modified steroid scaffold with lipophilic properties [45]. Its chemical structure contains a secosteroid with an open B-ring. Figure 2 shows a schematic overview of vitamin D metabolism.
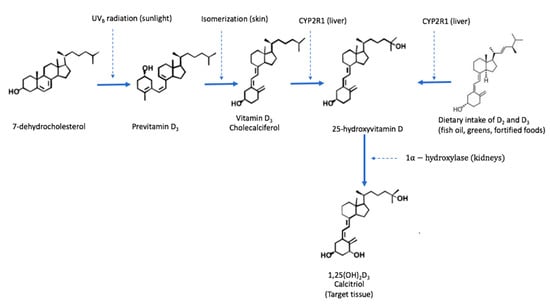
Figure 2.
The metabolism of vitamin D in humans; modified from [46].
Typically, the marker 25-hydroxyvitamin D (25(OH)D) is used as a surrogate endpoint of vitamin D status in plasma [47]. Historically it has been difficult to establish evidence-based recommendations for optimal plasma levels of vitamin D. Several health regulatory agencies have published slightly different definitions of vitamin deficiency based on the serum levels of 25-hydroxyvitamin D. An international consensus on the definition of vitamin D deficiency and sufficiency is lacking. Table 4 summarizes the definitions of selected health organizations and the Mayo Clinic [48,49,50,51,52,53].
Table 4.
Definition of Vitamin D status (25(OH)D concentration) by different health authorities.
Vitamin D is important for bone health and calcium homeostasis in humans. However, recent studies have implied that vitamin D has extraskeletal functions as well. Hewison et al. demonstrated that the enzyme 25(OH)-hydroxyvitamin D3-1α-hydroxylase is present in various extrarenal tissues [54], elucidating the local synthesis of active 1,25(OH)2D3. These findings suggest that vitamin D has autocrine and paracrine functions [54]. This probably exerts a positive impact on cardiovascular health and the immune system and prevents the development of diabetes mellitus [55].
4.2. Cardiovascular Effects of Vitamin D
In a recent review summarizing the current knowledge of the effects of vitamin D on cardiovascular disease, Saponaro et al. [56] demonstrated that this scientific field has drawn considerable attention in recent years. As detailed below, vitamin D deficiency is associated with hypertension [57], which is a risk factor in the atherosclerotic process. Moreover, in vitro models have been used to understand the possible mechanistic effects of vitamin D in CAD progression [58] and the suppression of renin synthesis [59]. Al-Ishaq et al. [60] have stated that vitamin D deficiency activates the renin-angiotensin-aldosterone system, which might lead to cardiac hypertrophy and increased CVD risk. However, RCTs and Mendelian studies have been inconclusive regarding the causality of vitamin D supplementation and improved cardiovascular outcomes [61].
4.2.1. Vitamin D and Essential Hypertension
In a review on vitamin D and essential hypertension [62], it was pointed out that, based on data from the third National Health and Nutrition Examination Survey (NHANES III), vitamin D deficiency is associated with essential hypertension [63,64]. In addition to these epidemiological findings, Yuan et al. demonstrated that vitamin D can suppress renin synthesis in vitro [59]. Nevertheless, RCTs performed to assess the impact of vitamin D supplementation on hypertension showed equivocal results [62]. This can, in part, be attributed to suboptimal study designs.
4.2.2. Association between Serum Vitamin D and Myocardial Injury
Using NHANES III data, Ahmad et al. [65] examined a possible association between serum vitamin D concentration and subclinical myocardial injury. In this cross-sectional study, recruited individuals were sought to be representative of the background population [66]. Hence, 8561 participants underwent a 12-lead ECG to visualize the electrical conduction of the heart. Participants with earlier diagnosed CVD were excluded, and thus 6079 participants were included for this analysis in the period between 1988 and 1994. To evaluate subclinical myocardial injury (SC-MI) in ECG measurements, the objective multivariate tool named the Cardiac Infarction Injury Score (CIIS) [67] was chosen. Participants were divided into three tertiles based on their serum levels of 25(OH)D (<20, 20–30 and >30 ng/mL).
The first group (serum-25(OH)D < 20 ng/mL) showed a prevalence of SC-MI = 23.0%, while the second group (serum-25(OH)D 20–30 ng/mL) had a prevalence of SC-MI = 21.1%. The third group (reference) with serum-25(OH)D > 30 ng/mL had a prevalence of SC-MI = 19.5%. A comparison of groups one and three revealed that SC-MI was inversely associated with 25(OH)D levels with an odds ratio (OR) of 1.27 (95% CI: 1.04–1.55) after adjustments for potential confounders [65]. Hence, the study found a significant incremental increase in SC-MI prevalence associated with vitamin D deficiency (p = 0.04).
Verdoia et al. [68] conducted another cross-sectional study to investigate the relationship between serum 25(OH)D-levels and CAD. The examined cohort comprised 1484 patients, all of whom underwent elective coronary angiography. The results showed that vitamin D deficiency is significantly associated with the severity of CAD. Comparing the odds of CAD in patients with severe hypovitaminosis D (<10 ng/mL) and patients with normal vitamin D status yielded an adjusted OR of 1.73 (95% CI: 1.18–2.52).
The strengths of these studies can be attributed to the large sample size. Moreover, data included in the NHANES III study were derived from a sample group without prior CVD history. So far, the NHANES III survey is the most comprehensive study, where both information on serum 25(OH)D-levels and markers of myocardial injury can be extracted. However, the methodological limitations include potential confounding factors, as the evaluations of exposure and outcomes were not temporally separated. Likewise, seasonal variation in serum 25(OH)D-levels might be a concern. This is due to fact that information is lacking about the time of year at which the participants had blood samples collected [65]. Even though both studies found strong associations between vitamin D status and CAD, this does not necessarily substantiate causality.
4.2.3. Impact of Vitamin D on Cardiac Function after MI
Le et al. [69] conducted an in vivo study to explore the effects of vitamin D on cardiac function in post-MI mice. One group of 1,25(OH)2D3 supplemented mice (n = 5) was compared to non-vitamin D supplemented controls (n = 5). The experimental mice were offered an optimal diet and husbandry conditions. At the start of the study, MI was induced in all mice by ligating the left anterior descending (LAD) artery. Subsequently, the intervention group was administered calcitriol 0.6 μg/day/kg for 14 days and examined by echocardiography and histological analysis. The results showed a significant reduction in the fibrotic scar area in the LV in the intervention arm compared with controls (p < 0.05). Likewise, LV wall thinning after MI was attenuated in calcitriol- supplemented mice versus controls (p < 0.05). Le et al. [69] performed an in vitro experiment to provide a mechanistic explanation for these findings (i.e., that vitamin D suppresses cell cycle progression in cCFU progenitor cells). Thus, cardiac myofibroblast differentiation might be decreased after calcitriol supplementation.
4.2.4. Possible Mechanisms behind Vitamin D Effects on CAD
To clarify possible underlying mechanisms of vitamin D effects on CAD, Chen et al. [58] performed a study in swine. Here, epicardial adipose tissue (EAT) cells were extracted and cultured as preadipocytes in vitro. Interestingly, this study indicated that vitamin D suppresses the nuclear factor ‘kappa-light-chain-enhancer’ of the activated B-cells (NF-κB) pathway and thereby attenuates the progression of CAD. Figure 3 depicts how vitamin D interferes with the NF-κB pathway.
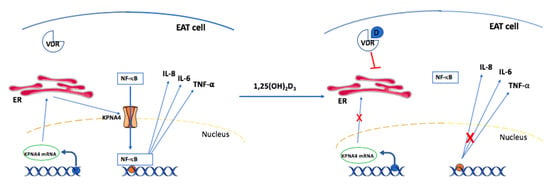
Figure 3.
Suppression of NF-κB pathways by vitamin D supplementation (modified from [53]). EAT cell: epicardial adipose tissue cell; VDR: vitamin D receptor; KPNA4: karyopherin α4; mRNA: messenger ribonucleic acid; NF-κB: nuclear factor kappa B; D: 1,25(OH)2-vitamin D3; IL-6: interleukin 6; IL-8: interleukin 8; TNF-α: tumor necrosis factor-α; ER: endoplasmic reticulum.
EAT cells are deeply involved in the progression of coronary atherogenesis mediated through the synthesis of local inflammatory cytokines [70]. First, KPNA4 mRNA is transcribed in the nucleus and transported to the endoplasmic reticulum in the cytosol, where translation takes place. Subsequently, the nascent KPNA4 protein is released and incorporated in the nuclear membrane. KPNA4 is a membrane transporter that is responsible for shuttling NF-κB from the cytosol to the nucleus [71]. NF-κB acts as a transcription factor in the nucleus via binding to different κB elements [72], which promote the transcription of proinflammatory cytokines such as IL-6, IL-8 and TNF-α. These cytokines are involved in the progression of atherogenesis in coronary arteries [73,74].
Interestingly, it appears that liganded 1,25(OH)2-vitamin D3-VDR actively suppresses the transcription and translation of KPNA4 in EAT cells. The reduced expression of KPNA4 leads to compromised shuttling of NF-κB into the nucleus. Hence, sufficient levels of intracellular 1,25(OH)2-vitamin D3 are capable of reducing the inflammatory response in the atherosclerotic process. This might to some extent be a mechanistic explanation as to how vitamin D deficiency is linked to CAD. However, it still remains to be elucidated how vitamin D3 indirectly or directly suppresses KPNA4 transcription [58].
4.3. Vitamin D Supplementation and CAD
A comprehensive review of relevant studies has been prepared in order to investigate whether vitamin D supplementation may exert beneficial effects on atherosclerosis and CAD. All eligible RCTs for this review are listed in Table 5.
Table 5.
Reviewed studies examining the effects of vitamin D supplementation on CAD and atherosclerosis.
5. Discussion
Overall, this review attempted to elucidate whether vitamin D supplementation could be beneficial as a treatment agent in CAD patients. A possible mechanistic link was provided by Chen et al. [58], who explained how vitamin D alters the inflammatory response of CAD through suppression of the NF-κB pathway. Likewise, Le et al. [69] suggested that calcitriol might decrease fibroblast differentiation in progenitor cCFU cells after MI. However, this study was conducted in mice, which might make it problematic to directly transfer these findings to the human organism. Overall, these results are consistent with epidemiological studies reporting serum 25(OH)D to be inversely correlated with CAD and myocardial injury [65,68]. However, the possibility of unknown confounding factors in these cross-sectional studies cannot be excluded. Hence, randomized prospective studies are in high demand.
Table 5 shows recent the RCTs that have attempted to address this issue. Nevertheless, the results are ambiguous. The two large scale studies [75,78] failed to demonstrate a beneficial effect of vitamin D on MI risk and CVD events. These studies must be given greater weight due to the large sample size. Interestingly, Scragg et al. [75] used monthly bolus doses of 100,000 IU in their study. One consideration worth following with this study design is the bioavailability of vitamin D. A high-dose intervention with a long dosage interval might be a suboptimal study design [90]. All RCTs that used this study design failed to demonstrate major benefits of vitamin D supplementation, even though plasma levels were restored [75,79,80,82,86].
Hin et al. [76] found no cardiovascular benefits of daily cholecalciferol therapy. Remarkably, plasma levels of 25(OH)D were above 50 nmol/L at baseline and 12 months after the intervention in both the intervention arm and controls. According to the Danish Health Authority [52], the threshold of vitamin D sufficiency is achieved at plasma concentrations between 50–160 nmol/L. Thus, possible additional cardiovascular benefits might be difficult to detect in this sample group.
The two studies by Seibert et al. [77] and Sokol et al. [84] have more similarities. Both studies had a study period of 12 weeks and did not show significant changes in endothelial markers, BP, inflammation or blood lipids. Perhaps a longer duration of follow-up in these studies would have clarified the effect of this intervention.
Only four small RCTs succeeded in showing major cardiovascular improvements following vitamin D supplementation. Wu et al. [81] examined whether daily supplementation of 0.5 μg calcitriol for six months could improve CAD. The results revealed a significantly decreased SYNTAX score (−3.9; p < 0.001) and reduced vascular inflammation. This was the only RCT to employ the administration of calcitriol (1α, 25-(OH)2D3), which is the active form of vitamin D. This vitamin D analogue is more potent compared to cholecalciferol and might be more suitable treating vitamin D insufficiency [91]. Therefore, it could be speculated as to whether this analogue is more effective in exerting positive effects on atherosclerosis and CAD. Nevertheless, further studies are needed to investigate if calcitriol is a better treatment agent in cardiovascular disease.
In a sub-study of the Women’s Health Initiative, Manson et al. [87] did not find evidence for reduced coronary calcification after seven years of cholecalciferol treatment. It is important to state that this RCT did not obtain information about vitamin D status in participants.
In a small study by Arnson et al. [85], five days of cholecalciferol treatment attenuated some inflammatory and endothelial markers (CRP, VCAM-1 and IL-6). Likewise, Raygan et al. found reduced vascular inflammation (hsCRP) and metabolic improvements in diabetic patients supplemented with 12 weeks of vitamin D [88,89]. Low calcium intake and low vitamin D status have been associated with obesity and diabetes mellitus [92,93]. This hints towards a tendency for better cardiovascular outcomes with vitamin D supplementation in certain patient subgroups, such as type 2 diabetics. Nevertheless, other studies in diabetic type 2 patients failed to demonstrate any effects on vascular inflammation [80,82,83]. In addition, the role of vitamin D in Ca2+-mediated apoptosis in obesity indirectly supports the recommendation to reach an optimal vitamin D status [94].
In general, the results in this field are conflicting. A comprehensive 2019 meta-analysis by Barbarawi et al. [95] including 83,000 participants did not find beneficial cardiovascular outcomes following vitamin D supplementation. However, further studies are needed to clarify if special subgroups could benefit from this intervention.
6. Conclusions
CAD is one of the most prevalent cardiovascular diseases. This disease is mainly caused by the progression of atherosclerosis. Predisposing factors represent a complex interaction between lifestyle, environmental and genetic contributors. Recent large-scale observational studies have demonstrated a strong inverse correlation between plasma levels of 25(OH)D and coronary atherosclerosis. Interestingly, in vitro studies suggest that vitamin D may attenuate CAD through the downregulation of the NF-κB pathway. However, the results obtained from a review of relevant RCTs presented here did not clearly show cardiovascular improvements following cholecalciferol supplementation.
Only a few RCTs have supported the hypothesis of the benefits of vitamin D in the treatment of CAD. In one study that employed calcitriol as the intervention, the results indicated a significant reduction in CAD and vascular inflammation. Hence, future studies could focus on the effects of more potent vitamin D analogues, such as calcitriol. Likewise, considerations of sufficient doses are important to conducting optimally designed studies. Finally, future studies may consider if certain subgroups such as type 2 diabetics with vitamin D insufficiency are more suitable for vitamin D supplementation.
Author Contributions
Conceptualization, C.L. and D.G.; methodology, C.L.; software, C.L.; validation, D.G., M.K. and M.W.; formal analysis, C.L., and M.W.; investigation, C.L.; resources, M.I.; writing—original draft preparation, C.L., M.K., D.G., and M.W.; writing—review and editing, D.G., M.K., and M.W.; project administration, D.G.; funding acquisition, D.G. and M.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Deutsches Zentrum für Luft- und Raumfahrt, grant number 50WB1924.
Acknowledgments
We would like to thank Proof-Reading-Service.com, Hertfordshire, United Kingdom for English editing of this review.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Thomas, H.; Diamond, J.; Vieco, A.; Chaudhuri, S.; Shinnar, E.; Cromer, S.; Perel, P.; Mensah, G.A.; Narula, J.; Johnson, C.O.; et al. Global atlas of cardiovascular disease 2000–2016: The path to prevention and control. Glob. Heart 2018, 13, 143–163. [Google Scholar] [CrossRef]
- Fioranelli, M.; Bottaccioli, A.G.; Bottaccioli, F.; Bianchi, M.; Rovesti, M.; Roccia, M.G. Stress and inflammation in coronary artery disease: A review psychoneuroendocrineimmunology-based. Front. Immunol. 2018, 9, 2031. [Google Scholar] [CrossRef] [PubMed]
- Christodoulidis, G.; Vittorio, T.J.; Fudim, M.; Lerakis, S.; Kosmas, C.E. Inflammation in coronary artery disease. Cardiol. Rev. 2014, 22, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Suades, R.; Padro, T.; Vilahur, G.; Badimon, L. Circulating and platelet-derived microparticles in human blood enhance thrombosis on atherosclerotic plaques. Thromb. Haemost. 2012, 108, 1208–1219. [Google Scholar] [CrossRef] [PubMed]
- Badimon, L.; Suades, R.; Arderiu, G.; Pena, E.; Chiva-Blanch, G.; Padro, T. Microvesicles in atherosclerosis and angiogenesis: From bench to bedside and reverse. Front. Cardiovasc. Med. 2017, 4, 77. [Google Scholar] [CrossRef] [PubMed]
- Slomka, A.; Piekus, A.; Kowalewski, M.; Pawliszak, W.; Anisimowicz, L.; Zekanowska, E. Assessment of the procoagulant activity of microparticles and the protein z system in patients undergoing off-pump coronary artery bypass surgery. Angiology 2018, 69, 347–357. [Google Scholar] [CrossRef]
- Hjerte. Available online: http://hjerteforeningen.dk/alt-om-dit-hjerte/hjertetal/hjertetaldk/ (accessed on 22 November 2019).
- Rai, V.; Agrawal, D.K. Role of vitamin D in cardiovascular diseases. Endocrinol. Metab. Clin. N. Am. 2017, 46, 1039–1059. [Google Scholar] [CrossRef]
- Mendis, S.; Thygesen, K.; Kuulasmaa, K.; Giampaoli, S.; Mahonen, M.; Ngu Blackett, K.; Lisheng, L. World health organization definition of myocardial infarction: 2008-09 revision. Int. J. Epidemiol. 2011, 40, 139–146. [Google Scholar] [CrossRef]
- Reed, G.W.; Rossi, J.E.; Cannon, C.P. Acute myocardial infarction. Lancet 2017, 389, 197–210. [Google Scholar] [CrossRef]
- George, J. Pathophysiology of coronary artery disease. In Interventional Cardiology Imaging: An Essential Guide; Abbas, A.E., Ed.; Springer: London, UK, 2015; pp. 29–46. [Google Scholar]
- Libby, P.; Ridker, P.M.; Hansson, G.K. Progress and challenges in translating the biology of atherosclerosis. Nature 2011, 473, 317–325. [Google Scholar] [CrossRef]
- Cochain, C.; Zernecke, A. Macrophages in vascular inflammation and atherosclerosis. Pflüg. Arch. 2017, 469, 485–499. [Google Scholar] [CrossRef] [PubMed]
- Rognoni, A.; Cavallino, C.; Veia, A.; Bacchini, S.; Rosso, R.; Facchini, M.; Secco, G.G.; Lupi, A.; Nardi, F.; Rametta, F.; et al. Pathophysiology of atherosclerotic plaque development. Cardiovasc. Hematol. Agents Med. Chem. 2015, 13, 10–13. [Google Scholar] [CrossRef]
- Gistera, A.; Hansson, G.K. The immunology of atherosclerosis. Nat. Rev. Nephrol. 2017, 13, 368–380. [Google Scholar] [CrossRef]
- Bentzon, J.F.; Otsuka, F.; Virmani, R.; Falk, E. Mechanisms of plaque formation and rupture. Circ. Res. 2014, 114, 1852–1866. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2019. [Google Scholar] [CrossRef]
- Oeing, C.U.; Tschope, C.; Pieske, B. [The new ESC Guidelines for acute and chronic heart failure 2016]. Herz 2016, 41, 655–663. [Google Scholar] [CrossRef]
- Albert, N.M.; Lewis, C. Recognizing and managing asymptomatic left ventricular dysfunction after myocardial infarction. Crit. Care Nurse 2008, 28, 20–37, quiz 38. [Google Scholar]
- Philippides, G.J. Managing the post-myocardial infarction patient with asymptomatic left ventricular dysfunction. Cardiology 2006, 105, 95–107. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef]
- Bakker, A.J.; Gorgels, J.P.; van Vlies, B.; Koelemay, M.J.; Smits, R.; Tijssen, J.G.; Haagen, F.D. Contribution of creatine kinase mb mass concentration at admission to early diagnosis of acute myocardial infarction. Br. Heart J. 1994, 72, 112–118. [Google Scholar] [CrossRef][Green Version]
- Rumbinaite, E.; Zaliaduonyte-Peksiene, D.; Viezelis, M.; Ceponiene, I.; Lapinskas, T.; Zvirblyte, R.; Vencloviene, J.; Morkunaite, K.; Bielinis, A.; Slapikas, R.; et al. Dobutamine-stress echocardiography speckle-tracking imaging in the assessment of hemodynamic significance of coronary artery stenosis in patients with moderate and high probability of coronary artery disease. Medicina (Kaunas.) 2016, 52, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, J.P.; Ripley, D.P.; Berry, C.; McCann, G.P.; Plein, S.; Bucciarelli-Ducci, C.; Dall’Armellina, E.; Prasad, A.; Bijsterveld, P.; Foley, J.R.; et al. Effect of care guided by cardiovascular magnetic resonance, myocardial perfusion scintigraphy, or nice guidelines on subsequent unnecessary angiography rates: The ce-marc 2 randomized clinical trial. JAMA 2016, 316, 1051–1060. [Google Scholar] [CrossRef]
- Gotschy, A.; Niemann, M.; Kozerke, S.; Luscher, T.F.; Manka, R. Cardiovascular magnetic resonance for the assessment of coronary artery disease. Int. J. Cardiol. 2015, 193, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Flora, G.D.; Nayak, M.K. A brief review of cardiovascular diseases, associated risk factors and current treatment regimes. Curr. Pharm. Des. 2019. [Google Scholar] [CrossRef] [PubMed]
- Ornish, D.; Scherwitz, L.W.; Billings, J.H.; Brown, S.E.; Gould, K.L.; Merritt, T.A.; Sparler, S.; Armstrong, W.T.; Ports, T.A.; Kirkeeide, R.L.; et al. Intensive lifestyle changes for reversal of coronary heart disease. JAMA 1998, 280, 2001–2007. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, S.R.; Wanstall, J.C. Beta-1 and beta-2 adrenoceptor-mediated responses in preparations of pulmonary artery and aorta from young and aged rats. J. Pharmacol. Exp. Ther. 1984, 228, 733–738. [Google Scholar] [PubMed]
- Patrono, C.; Morais, J.; Baigent, C.; Collet, J.P.; Fitzgerald, D.; Halvorsen, S.; Rocca, B.; Siegbahn, A.; Storey, R.F.; Vilahur, G. Antiplatelet agents for the treatment and prevention of coronary atherothrombosis. J. Am. Coll. Cardiol. 2017, 70, 1760–1776. [Google Scholar] [CrossRef] [PubMed]
- Stancu, C.; Sima, A. Statins: Mechanism of action and effects. J. Cell. Mol. Med. 2001, 5, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Oesterle, A.; Laufs, U.; Liao, J.K. Pleiotropic effects of statins on the cardiovascular system. Circ. Res. 2017, 120, 229–243. [Google Scholar] [CrossRef]
- Tarkin, J.M.; Kaski, J.C. Vasodilator therapy: Nitrates and nicorandil. Cardiovasc. Drugs Ther. 2016, 30, 367–378. [Google Scholar] [CrossRef]
- Iachini Bellisarii, F.; Radico, F.; Muscente, F.; Horowitz, J.; De Caterina, R. Nitrates and other nitric oxide donors in cardiology: Current positioning and perspectives. Cardiovasc. Drugs Ther. 2012, 26, 55–69. [Google Scholar] [CrossRef] [PubMed]
- Brown, N.J.; Vaughan, D.E. Angiotensin-converting enzyme inhibitors. Circulation 1998, 97, 1411–1420. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.K.; Griendling, K.K. Angiotensin ii cell signaling: Physiological and pathological effects in the cardiovascular system. Am. J. Physiol. Cell Physiol. 2007, 292, C82–C97. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Shi, G. How cav1.2-bound verapamil blocks ca(2+) influx into cardiomyocyte: Atomic level views. Pharmacol. Res. 2019, 139, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Rayner-Hartley, E.; Sedlak, T. Ranolazine: A contemporary review. J. Am. Heart. Assoc. 2016, 5, e003196. [Google Scholar] [CrossRef]
- Fisch, A.S.; Perry, C.G.; Stephens, S.H.; Horenstein, R.B.; Shuldiner, A.R. Pharmacogenomics of anti-platelet and anti-coagulation therapy. Curr. Cardiol. Rep. 2013, 15, 381. [Google Scholar] [CrossRef][Green Version]
- Favaloro, R.G.; Effler, D.B.; Cheanvechai, C.; Quint, R.A.; Sones, F.M., Jr. Acute coronary insufficiency (impending myocardial infarction and myocardial infarction): Surgical treatment by the saphenous vein graft technique. Am. J. Cardiol. 1971, 28, 598–607. [Google Scholar] [CrossRef]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Steg, P.G.; James, S.K.; Atar, D.; Badano, L.P.; Blomstrom-Lundqvist, C.; Borger, M.A.; Di Mario, C.; Dickstein, K.; Ducrocq, G.; Fernandez-Aviles, F.; et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur. Heart J. 2012, 33, 2569–2619. [Google Scholar] [CrossRef]
- Melly, L.; Torregrossa, G.; Lee, T.; Jansens, J.L.; Puskas, J.D. Fifty years of coronary artery bypass grafting. J. Thorac. Dis. 2018, 10, 1960–1967. [Google Scholar] [CrossRef]
- Mohr, F.W.; Morice, M.C.; Kappetein, A.P.; Feldman, T.E.; Stahle, E.; Colombo, A.; Mack, M.J.; Holmes, D.R., Jr.; Morel, M.A.; Van Dyck, N.; et al. Coronary artery bypass graft surgery versus percutaneous coronary intervention in patients with three-vessel disease and left main coronary disease: 5-year follow-up of the randomised, clinical syntax trial. Lancet 2013, 381, 629–638. [Google Scholar] [CrossRef]
- Deluca, H.F. History of the discovery of vitamin D and its active metabolites. Bonekey Rep. 2014, 3, 479. [Google Scholar] [CrossRef] [PubMed]
- Macintyre, I.; Evans, I.M.; Larkins, R.G. Vitamin D. Clin. Endocrinol. (Oxf.) 1977, 6, 65–79. [Google Scholar] [CrossRef] [PubMed]
- Al Mheid, I.; Patel, R.S.; Tangpricha, V.; Quyyumi, A.A. Vitamin D and cardiovascular disease: Is the evidence solid? Eur. Heart J. 2013, 34, 3691–3698. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the institute of medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef]
- IOM (Institute of Medicine). Dietary Reference Intakes for Calcium and Vitamin D; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Camacho, P.M.; Petak, S.M.; Binkley, N.; Clarke, B.; Harris, S.T.; Hurley, D.L.; Kleerekoper, M.; Lewiecki, E.M.; Miller, P.D.; Narula, H.S.; et al. American association of clinical endocrinologists and American College of Endocrinology clinical practice guidelines for the diagnosis and treatment of postmenopausal osteoporosis—2016. Endocr. Pract. 2016, 22, 1–42. [Google Scholar] [CrossRef]
- Thacher, T.D.; Clarke, B.L. Vitamin D insufficiency. Mayo Clin. Proc. 2011, 86, 50–60. [Google Scholar] [CrossRef]
- Mosekilde, L.; Nielsen, R.; Larsen, E.R.; Moosgaard, B.; Heickendorff, L. [Vitamin D deficiency. Definition and prevalence in denmark]. Ugeskr Laeger 2005, 167, 29–33. [Google Scholar]
- Lips, P.; Cashman, K.D.; Lamberg-Allardt, C.; Bischoff-Ferrari, H.A.; Obermayer-Pietsch, B.R.; Bianchi, M.; Stepan, J.; El-Hajj Fuleihan, G.; Bouillon, R. MANAGEMENT OF ENDOCRINE DISEASE: Current vitamin D status in European and Middle East countries and strategies to prevent vitamin D deficiency; a position statement of the European Calcified Tissue Society. Eur. J. Endocrinol. 2019, 180, 23–54. [Google Scholar] [CrossRef]
- Hewison, M.; Burke, F.; Evans, K.N.; Lammas, D.A.; Sansom, D.M.; Liu, P.; Modlin, R.L.; Adams, J.S. Extra-renal 25-hydroxyvitamin D3-1alpha-hydroxylase in human health and disease. J. Steroid Biochem. Mol. Biol. 2007, 103, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Lockau, L.; Atkinson, S.A. Vitamin D’s role in health and disease: How does the present inform our understanding of the past? Int. J. Paleopathol. 2018, 23, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Saponaro, F.; Marcocci, C.; Zucchi, R. Vitamin D status and cardiovascular outcome. J. Endocrinol. Investig. 2019, 42, 1285–1290. [Google Scholar] [CrossRef] [PubMed]
- Norman, P.E.; Powell, J.T. Vitamin D and cardiovascular disease. Circ. Res. 2014, 114, 379–393. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Swier, V.J.; Boosani, C.S.; Radwan, M.M.; Agrawal, D.K. Vitamin D deficiency accelerates coronary artery disease progression in swine. Arterioscler. Thromb. Vasc. Biol. 2016, 36, 1651–1659. [Google Scholar] [CrossRef] [PubMed]
- Yuan, W.; Pan, W.; Kong, J.; Zheng, W.; Szeto, F.L.; Wong, K.E.; Cohen, R.; Klopot, A.; Zhang, Z.; Li, Y.C. 1,25-dihydroxyvitamin D3 suppresses renin gene transcription by blocking the activity of the cyclic AMP response element in the renin gene promoter. J. Biol. Chem. 2007, 282, 29821–29830. [Google Scholar] [CrossRef]
- Al-Ishaq, R.K.; Kubatka, P.; Brozmanova, M.; Gazdikova, K.; Caprnda, M.; Busselberg, D. Health implication of vitamin D on the cardiovascular and the renal system. Arch. Physiol. Biochem. 2019, 1–15. [Google Scholar] [CrossRef]
- Pilz, S.; Verheyen, N.; Grubler, M.R.; Tomaschitz, A.; Marz, W. Vitamin D and cardiovascular disease prevention. Nat. Rev. Cardiol. 2016, 13, 404–417. [Google Scholar] [CrossRef] [PubMed]
- Legarth, C.; Grimm, D.; Wehland, M.; Bauer, J.; Kruger, M. The impact of vitamin D in the treatment of essential hypertension. Int. J. Mol. Sci. 2018, 19, 455. [Google Scholar] [CrossRef]
- Martins, D.; Wolf, M.; Pan, D.; Zadshir, A.; Tareen, N.; Thadhani, R.; Felsenfeld, A.; Levine, B.; Mehrotra, R.; Norris, K. Prevalence of cardiovascular risk factors and the serum levels of 25-hydroxyvitamin D in the united states: Data from the third national health and nutrition examination survey. Arch. Intern. Med. 2007, 167, 1159–1165. [Google Scholar] [CrossRef]
- Scragg, R.; Sowers, M.; Bell, C. Serum 25-hydroxyvitamin D, ethnicity, and blood pressure in the third national health and nutrition examination survey. Am. J. Hypertens. 2007, 20, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.I.; Chevli, P.A.; Li, Y.; Soliman, E.Z. Vitamin D deficiency and electrocardiographic subclinical myocardial injury: Results from national health and nutrition examination survey-iii. Clin. Cardiol. 2018, 41, 1468–1473. [Google Scholar] [CrossRef] [PubMed]
- Burt, V.L.; Harris, T. The third national health and nutrition examination survey: Contributing data on aging and health. Gerontologist 1994, 34, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Rautaharju, P.M.; Warren, J.W.; Jain, U.; Wolf, H.K.; Nielsen, C.L. Cardiac infarction injury score: An electrocardiographic coding scheme for ischemic heart disease. Circulation 1981, 64, 249–256. [Google Scholar] [CrossRef]
- Verdoia, M.; Schaffer, A.; Sartori, C.; Barbieri, L.; Cassetti, E.; Marino, P.; Galasso, G.; De Luca, G. Vitamin D deficiency is independently associated with the extent of coronary artery disease. Eur. J. Clin. Investig. 2014, 44, 634–642. [Google Scholar] [CrossRef]
- Le, T.Y.L.; Ogawa, M.; Kizana, E.; Gunton, J.E.; Chong, J.J.H. Vitamin D improves cardiac function after myocardial infarction through modulation of resident cardiac progenitor cells. Heart Lung Circ. 2018, 27, 967–975. [Google Scholar] [CrossRef]
- Owen, M.K.; Noblet, J.N.; Sassoon, D.J.; Conteh, A.M.; Goodwill, A.G.; Tune, J.D. Perivascular adipose tissue and coronary vascular disease. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1643–1649. [Google Scholar] [CrossRef]
- Leonard, A.; Rahman, A.; Fazal, F. Importins alpha and beta signaling mediates endothelial cell inflammation and barrier disruption. Cell. Signal. 2018, 44, 103–117. [Google Scholar] [CrossRef]
- Sun, X.; Icli, B.; Wara, A.K.; Belkin, N.; He, S.; Kobzik, L.; Hunninghake, G.M.; Vera, M.P.; Blackwell, T.S.; Baron, R.M.; et al. Microrna-181b regulates nf-kappab-mediated vascular inflammation. J. Clin. Investig. 2012, 122, 1973–1990. [Google Scholar] [CrossRef]
- Boisvert, W.A.; Curtiss, L.K.; Terkeltaub, R.A. Interleukin-8 and its receptor cxcr2 in atherosclerosis. Immunol. Res. 2000, 21, 129–137. [Google Scholar] [CrossRef]
- Fatkhullina, A.R.; Peshkova, I.O.; Koltsova, E.K. The role of cytokines in the development of atherosclerosis. Biochemistry (Mosc.) 2016, 81, 1358–1370. [Google Scholar] [CrossRef] [PubMed]
- Scragg, R.; Stewart, A.W.; Waayer, D.; Lawes, C.M.M.; Toop, L.; Sluyter, J.; Murphy, J.; Khaw, K.T.; Camargo, C.A., Jr. Effect of monthly high-dose vitamin D supplementation on cardiovascular disease in the vitamin D assessment study: A randomized clinical trial. JAMA Cardiol. 2017, 2, 608–616. [Google Scholar] [CrossRef] [PubMed]
- Hin, H.; Tomson, J.; Newman, C.; Kurien, R.; Lay, M.; Cox, J.; Sayer, J.; Hill, M.; Emberson, J.; Armitage, J.; et al. Optimum dose of vitamin D for disease prevention in older people: BEST-D trial of vitamin D in primary care. Osteoporos. Int. 2017, 28, 841–851. [Google Scholar] [CrossRef] [PubMed]
- Seibert, E.; Lehmann, U.; Riedel, A.; Ulrich, C.; Hirche, F.; Brandsch, C.; Dierkes, J.; Girndt, M.; Stangl, G.I. Vitamin D3 supplementation does not modify cardiovascular risk profile of adults with inadequate vitamin D status. Eur. J. Nutr. 2017, 56, 621–634. [Google Scholar] [CrossRef] [PubMed]
- Manson, J.E.; Bassuk, S.S.; Lee, I.M.; Cook, N.R.; Albert, M.A.; Gordon, D.; Zaharris, E.; Macfadyen, J.G.; Danielson, E.; Lin, J.; et al. The vitamin D and omega-3 trial (vital): Rationale and design of a large randomized controlled trial of vitamin D and marine omega-3 fatty acid supplements for the primary prevention of cancer and cardiovascular disease. Contemp. Clin. Trials 2012, 33, 159–171. [Google Scholar] [CrossRef]
- Aslanabadi, N.; Jafaripor, I.; Sadeghi, S.; Hamishehkar, H.; Ghaffari, S.; Toluey, M.; Azizi, H.; Entezari-Maleki, T. Effect of vitamin D in the prevention of myocardial injury following elective percutaneous coronary intervention: A pilot randomized clinical trial. J. Clin. Pharmacol. 2018, 58, 144–151. [Google Scholar] [CrossRef]
- Forouhi, N.G.; Menon, R.K.; Sharp, S.J.; Mannan, N.; Timms, P.M.; Martineau, A.R.; Rickard, A.P.; Boucher, B.J.; Chowdhury, T.A.; Griffiths, C.J.; et al. Effects of vitamin D2 or D3 supplementation on glycaemic control and cardiometabolic risk among people at risk of type 2 diabetes: Results of a randomized double-blind placebo-controlled trial. Diabetes Obes. Metab. 2016, 18, 392–400. [Google Scholar] [CrossRef]
- Wu, Z.; Wang, T.; Zhu, S.; Li, L. Effects of vitamin D supplementation as an adjuvant therapy in coronary artery disease patients. Scand. Cardiovasc. J. 2016, 50, 9–16. [Google Scholar] [CrossRef]
- Shaseb, E.; Tohidi, M.; Abbasinazari, M.; Khalili, D.; Talasaz, A.H.; Omrani, H.; Hadaegh, F. The effect of a single dose of vitamin D on glycemic status and C-reactive protein levels in type 2 diabetic patients with ischemic heart disease: A randomized clinical trial. Acta Diabetol. 2016, 53, 575–582. [Google Scholar] [CrossRef]
- Dalan, R.; Liew, H.; Assam, P.N.; Chan, E.S.; Siddiqui, F.J.; Tan, A.W.; Chew, D.E.; Boehm, B.O.; Leow, M.K. A randomised controlled trial evaluating the impact of targeted vitamin D supplementation on endothelial function in type 2 diabetes mellitus: The dimension trial. Diabetes Vasc. Dis. Res. 2016, 13, 192–200. [Google Scholar] [CrossRef]
- Sokol, S.I.; Srinivas, V.; Crandall, J.P.; Kim, M.; Tellides, G.; Lebastchi, A.H.; Yu, Y.; Gupta, A.K.; Alderman, M.H. The effects of vitamin D repletion on endothelial function and inflammation in patients with coronary artery disease. Vasc. Med. 2012, 17, 394–404. [Google Scholar] [CrossRef] [PubMed]
- Arnson, Y.; Itzhaky, D.; Mosseri, M.; Barak, V.; Tzur, B.; Agmon-Levin, N.; Amital, H. Vitamin D inflammatory cytokines and coronary events: A comprehensive review. Clin. Rev. Allergy Immunol. 2013, 45, 236–247. [Google Scholar] [CrossRef] [PubMed]
- Witham, M.D.; Dove, F.J.; Khan, F.; Lang, C.C.; Belch, J.J.; Struthers, A.D. Effects of vitamin D supplementation on markers of vascular function after myocardial infarction—a randomised controlled trial. Int. J. Cardiol. 2013, 167, 745–749. [Google Scholar] [CrossRef] [PubMed]
- Manson, J.E.; Allison, M.A.; Carr, J.J.; Langer, R.D.; Cochrane, B.B.; Hendrix, S.L.; Hsia, J.; Hunt, J.R.; Lewis, C.E.; Margolis, K.L.; et al. Calcium/vitamin D supplementation and coronary artery calcification in the women’s health initiative. Menopause 2010, 17, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Farrokhian, A.; Raygan, F.; Bahmani, F.; Talari, H.R.; Esfandiari, R.; Esmaillzadeh, A.; Asemi, Z. Long-term vitamin D supplementation affects metabolic status in vitamin D-deficient type 2 diabetic patients with coronary artery disease. J. Nutr. 2017, 147, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Raygan, F.; Ostadmohammadi, V.; Bahmani, F.; Asemi, Z. The effects of vitamin D and probiotic co-supplementation on mental health parameters and metabolic status in type 2 diabetic patients with coronary heart disease: A randomized, double-blind, placebo-controlled trial. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 84, 50–55. [Google Scholar] [CrossRef]
- Dalle Carbonare, L.; Valenti, M.T.; Del Forno, F.; Caneva, E.; Pietrobelli, A. Vitamin D: Daily vs. Monthly use in children and elderly—what is going on? Nutrients 2017, 9, 652. [Google Scholar] [CrossRef]
- Tanakol, R.; Gul, N.; Uzum, A.K.; Aral, F. Calcitriol treatment in patients with low vitamin D levels. Arch. Osteoporos. 2018, 13, 114. [Google Scholar] [CrossRef]
- Song, Q.; Sergeev, I. Calcium and vitamin D in obesity. Nutr. Res. Rev. 2012, 25, 130–141. [Google Scholar] [CrossRef]
- Sergeev, I.N. Vitamin D—Cellular Ca2+ link to obesity and diabetes. J. Steroid Biochem. Mol. Biol. 2016, 164, 326–330. [Google Scholar] [CrossRef]
- Sergeev, I.N. Vitamin D-mediated apoptosis in cancer and obesity. Horm. Mol. Biol. Clin. Investig. 2014, 20, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Barbarawi, M.; Kheiri, B.; Zayed, Y.; Barbarawi, O.; Dhillon, H.; Swaid, B.; Yelangi, A.; Sundus, S.; Bachuwa, G.; Alkotob, M.L.; et al. Vitamin D supplementation and cardiovascular disease risks in more than 83000 individuals in 21 randomized clinical trials: A meta-analysis. JAMA Cardiol. 2019. [Google Scholar] [CrossRef] [PubMed]



© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).