Associations of Vitamin D Deficiency, Parathyroid hormone, Calcium, and Phosphorus with Perinatal Adverse Outcomes. A Prospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants Data
2.2. Clinical and Biochemical Procedures
2.3. Statistical Analysis
3. Results
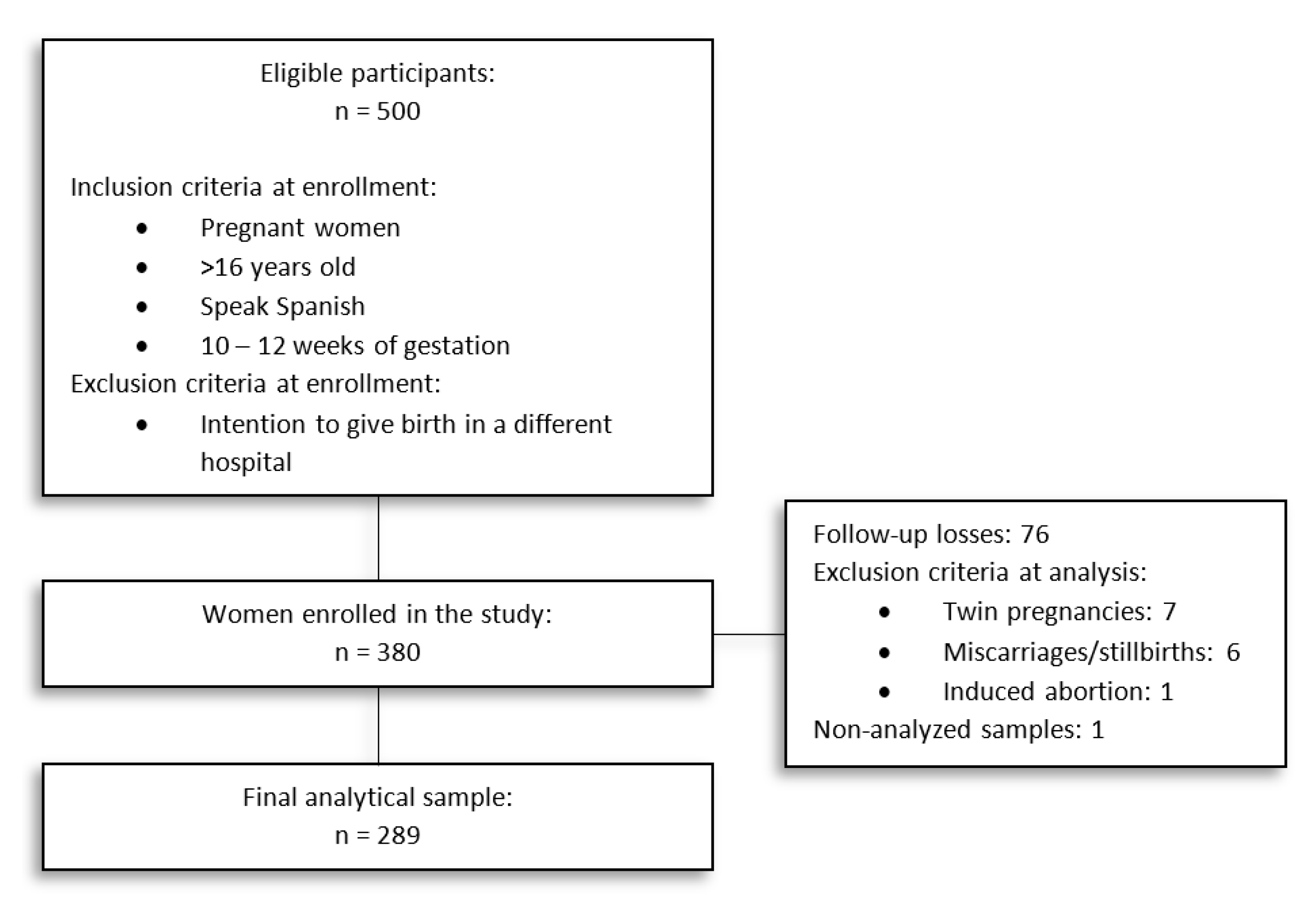
3.1. Cohort of Study
3.2. Characteristics of Participants
3.3. Pregnancy and Perinatal Adverse Outcomes
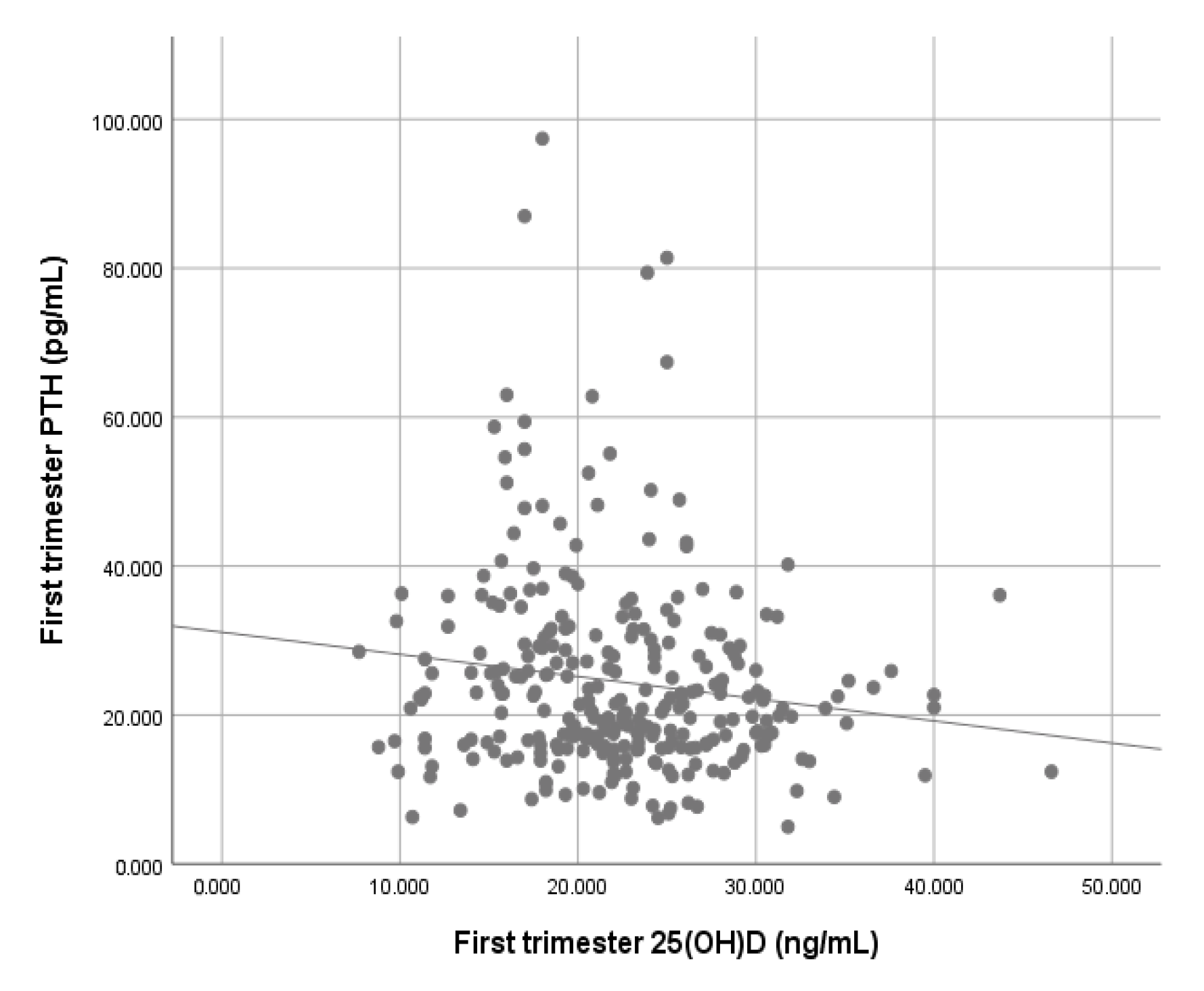
3.4. Associations of Vitamin D Deficiency, PTH, Calcium, and Phosphorus with Perinatal Adverse Outcomes
4. Discussion
4.1. Limitations of the Study
4.2. Deficiency of Vitamin D and Preterm Birth
4.3. Vitamin D Associated Metabolites and Perinatal Outcomes
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Holick, M.F. The Vitamin D Deficiency Pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Roth, D.E.; Abrams, S.A.; Aloia, J.; Bergeron, G.; Bourassa, M.W.; Brown, K.H.; Calvo, M.S.; Cashman, K.D.; Combs, G.; De-Regil, L.M.; et al. Global prevalence and disease burden of vitamin D deficiency: A roadmap for action in low- and middle-income countries. Ann. N. Y. Acad. Sci. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wacker, M.; Holiack, M.F. Vitamin D-effects on skeletal and extraskeletal health and the need for supplementation. Nutrients 2013, 5, 111–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-López, F.R.; Pasupuleti, V.; Mezones-Holguin, E.; Benites-Zapata, V.A.; Thota, P.; Deshpande, A.; Hernandez, A.V. Effect of vitamin D supplementation during pregnancy on maternal and neonatal outcomes: A systematic review and meta-analysis of randomized controlled trials. Fertil. Steril. 2015, 103, 1278–1288. [Google Scholar] [CrossRef]
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.-B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef] [Green Version]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Wei, S.-Q.; Qi, H.-P.; Luo, Z.-C.; Fraser, W.D. Maternal vitamin D status and adverse pregnancy outcomes: A systematic review and meta-analysis. J. Matern. Fetal. Neonatal Med. 2013, 26, 889–899. [Google Scholar] [CrossRef]
- Agarwal, S.; Kovilam, O.; Agrawal, D.K. Vitamin D and its impact on maternal-fetal outcomes in pregnancy: A critical review. Crit. Rev. Food Sci. Nutr. 2018, 58, 755–769. [Google Scholar] [CrossRef]
- Chung, C.; Silwal, P.; Kim, I.; Modlin, R.L.; Jo, E.K. Vitamin D-Cathelicidin axis: At the crossroads between protective immunity and pathological inflammation during infection. Immune Netw. 2020, 20, 1–26. [Google Scholar] [CrossRef]
- Morgan, C.; Dodds, L.; Langille, D.B.; Weiler, H.A.; Armson, B.A.; Forest, J.-C.; Giguere, Y.; Woolcott, C.G. Cord blood vitamin D status and neonatal outcomes in a birth cohort in Quebec, Canada. Arch. Gynecol. Obstet. 2016, 293, 731–738. [Google Scholar] [CrossRef]
- Chen, Y.-H.; Fu, L.; Hao, J.-H.; Wang, H.; Zhang, C.; Tao, F.-B.; Xu, D.-X. Influent factors of gestational vitamin D deficiency and its relation to an increased risk of preterm delivery in Chinese population. Sci. Rep. 2018, 8, 3608. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems: Tenth Revision, 2nd ed.; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- WHO Expert Committee on Physical Status. The use and interpretation of anthropometry (1993: Geneva, Switzerland) & World Health Organization. In Physical Status: The Use of and Interpretation of Anthropometry, Report of A WHO Expert Committee; World Health Organization: Geneva, Switzerland, 1995; Available online: https://apps.who.int/iris/handle/10665/37003 (accessed on 20 July 2020).
- Chen, Y.H.; Fu, L.; Hao, J.H.; Yu, Z.; Zhu, P.; Wang, H.; Xu, Y.Y.; Zhang, C.; Tao, F.B.; Xu, D.X. Maternal vitamin D deficiency during pregnancy elevates the risks of small for gestational age and low birth weight infants in Chinese population. J. Clin. Endocrinol. Metab. 2015, 100, 1912–1919. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Xiao, Y.; Zhang, L.; Gao, Q. Maternal early pregnancy vitamin D status in relation to low birth weight and small-for-gestational-age offspring. J. Steroid Biochem. Mol. Biol. 2018, 175, 146–150. [Google Scholar] [CrossRef]
- Monier, I.; Baptiste, A.; Tsatsaris, V.; Senat, M.V.; Jani, J.; Jouannic, J.M.; Winer, N.; Elie, C.; Souberbielle, J.C.; Zeitlin, J.; et al. First trimester maternal vitamin D status and risks of preterm birth and small-for-gestational age. Nutrients 2019, 11, 3042. [Google Scholar] [CrossRef] [Green Version]
- Santorelli, G.; Whitelaw, D.; Farrar, D.; West, J.; Lawlor, D.A. Associations of maternal vitamin D, PTH and calcium with hypertensive disorders of pregnancy and associated adverse perinatal outcomes: Findings from the born in Bradford cohort study. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef]
- Bodnar, L.M.; Catov, J.M.; Zmuda, J.M.; Cooper, M.E.; Parrott, M.S.; Roberts, J.M.; Marazita, M.L.; Simhan, H.N. Maternal serum 25-hydroxyvitamin D concentrations are associated with small-for-gestational age births in white women. J. Nutr. 2010, 21, 999–1006. [Google Scholar] [CrossRef] [Green Version]
- Qin, L.-L.; Lu, F.-G.; Yang, S.-H.; Xu, H.-L.; Luo, B.-A. Does maternal vitamin D deficiency increase the risk of preterm birth: A meta-analysis of observational studies. Nutrients 2016, 8, 301. [Google Scholar] [CrossRef]
- Zhou, S.-S.; Tao, Y.-H.; Huang, K.; Zhu, B.-B.; Tao, F.-B. Vitamin D and risk of preterm birth: Up-to-date meta-analysis of randomized controlled trials and observational studies. J. Obstet. Gynaecol. Res. 2017, 43, 247–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Zhu, B.; Wu, X.; Li, S.; Tao, F. Association between maternal vitamin D deficiency and small for gestational age: Evidence from a meta-analysis of prospective cohort studies. BMJ Open 2017, 7, e016404. [Google Scholar] [CrossRef] [Green Version]
- Aguilar-cordero, M.J.; Lasserrot-cuadrado, A.; Mur-villar, N.; León-ríos, X.A. Vitamin D, preeclampsia and prematurity: A systematic review and meta-analysis of observational and interventional studies. Midwifery 2020, 87, 102707. [Google Scholar] [CrossRef] [PubMed]
- Maugeri, A.; Barchitta, M.; Blanco, I.; Agodi, A. Effects of vitamin D supplementation during pregnancy on birth size: A systematic review and meta-analysis of randomized controlled trials. Nutrients 2019, 11, 442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalmar, A.; Raff, H.; Chauhan, S.P.; Singh, M.; Siddiqui, D.S. Serum 25-hydroxyvitamin D, calcium, and calcium-regulating hormones in preeclamptics and controls during first day postpartum. Endocrine 2015, 48, 287–292. [Google Scholar] [CrossRef]
- Meng, D.H.; Zhang, Y.; Hu, H.L.; Li, J.J.; Yin, W.J.; Ma, S.S.; Tao, R.X.; Zhu, P. The role of PTH during pregnancy on the relationship between maternal vitamin D deficiency and fetal growth restriction: A prospective birth cohort study. Br. J. Nutr. 2020, 124, 432–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemmingway, A.; Kenny, L.C.; Malvisi, L.; Kiely, M.E. Exploring the concept of functional vitamin D deficiency in pregnancy: Impact of the interaction between 25-hydroxyvitamin D and parathyroid hormone on perinatal outcomes. Am. J. Clin. Nutr. 2018, 108, 821–829. [Google Scholar] [CrossRef]
- Buppasiri, P.; Lumbiganon, P.; Thinkhamrop, J.; Ngamjarus, C.; Laopaiboon, M.; Medley, N. Calcium supplementation (other than for preventing or treating hypertension) for improving pregnancy and infant outcomes. Cochrane Database Syst. Rev. 2015, 2, CD007079. [Google Scholar] [CrossRef] [PubMed]
- Hofmeyr, G.J.; Lawrie, T.A.; Atallah, A.N.; Duley, L.; Torloni, M.R. Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane Database Syst. Rev. 2014, 6, CD001059. [Google Scholar] [CrossRef]
- Scholl, T.O.; Chen, X.; Stein, T.P. Maternal calcium metabolic stress and fetal growth. Am. J. Clin. Nutr. 2014, 99, 918–925. [Google Scholar] [CrossRef] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbrouckef, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Bull. World Health Organ. 2007, 85, 867–872. [Google Scholar] [CrossRef]
- Perez-Ferre, N.; Torrejon, M.J.; Fuentes, M.; Fernandez, M.D.; Ramos, A.; Bordiu, E.; Del Valle, L.; Rubio, M.A.; Bedia, A.R.; Montañez, C.; et al. Association of low serum 25-hydroxyvitamin D levels in pregnancy with glucose homeostasis and obstetric and newborn outcomes. Endocr. Pract. 2012, 18, 676–684. [Google Scholar] [CrossRef]
- Oliver, E.M.; Grimshaw, K.E.C.; Schoemaker, A.A.; Keil, T.; McBride, D.; Sprikkelman, A.B.; Ragnarsdottir, H.S.; Trendelenburg, V.; Emmanouil, E.; Reche, M.; et al. Dietary habits and supplement use in relation to national pregnancy recommendations: Data from the EuroPrevall birth cohort. Matern. Child Health J. 2014, 18, 2408–2425. [Google Scholar] [CrossRef]
- IOM (Institute of Medicine). Dietary Reference Intakes for Calcium and Vitamin D; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Giustina, A.; Adler, R.A.; Binkley, N.; Bollerslev, J.; Bouillon, R.; Dawson-Hughes, B.; Ebeling, P.R.; Feldman, D.; Formenti, A.M.; Lazaretti-Castro, M.; et al. Consensus Statement from 2nd International Conference on Controversies in Vitamin D. Rev. Endocr. Metab. Disord. 2020, 21, 89–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karras, S.N.; Fakhoury, H.; Muscogiuri, G.; Grant, W.B.; van den Ouweland, J.M.; Colao, A.M.; Kotsa, K. Maternal vitamin D levels during pregnancy and neonatal health: Evidence to date and clinical implications. Ther. Adv. Musculoskelet. Dis. 2016, 8, 124–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.P.; Saito, S.; Hall, D.R.; Warren, C.E.; Adoyi, G.; Ishaku, S. The hypertensive disorders of pregnancy: ISSHP classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. 2018, 13, 291–310. [Google Scholar] [CrossRef] [PubMed]
- Gavin, J.R.; Alberti, K.G.M.M.; Davidson, M.B.; DeFronzo, R.A.; Drash, A.; Gabbe, S.G.; Genuth, S.; Harris, M.I.; Kahn, R.; Keen, H.; et al. Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 2002, 25, 5–20. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO: Recommended definitions, terminology and format for statistical tables related to the perinatal period and use of a new certificate for cause of perinatal deaths. Acta Obstet. Gynecol. Scand. 1977, 56, 247–253.
- Terán, J.M.; Varea, C.; Bernis, C.; Bogin, B.; González-González, A. Nuevas curvas de peso al nacer por paridad y tipo de parto para la población Española. Gac. Sanit. 2017, 31, 116–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosmer, D.W.; Lemeshow, S. Aplied Logistic Regression, 2nd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2000. [Google Scholar]
- Zhang, Z. Model building strategy for logistic regression: Purposeful selection. Ann. Transl. Med. 2016, 4, 4–10. [Google Scholar] [CrossRef] [Green Version]
- Abalos, E.; Cuesta, C.; Grosso, A.L.; Chou, D.; Say, L. Global and regional estimates of preeclampsia and eclampsia: A systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 170, 1–7. [Google Scholar] [CrossRef]
- Guariguata, L.; Linnenkamp, U.; Beagley, J.; Whiting, D.R.; Cho, N.H. Global estimates of the prevalence of hyperglycaemia in pregnancy. Diabetes Res. Clin. Pract. 2014, 103, 176–185. [Google Scholar] [CrossRef]
- DeSisto, C.L.; Kim, S.Y.; Sharma, A.J. Prevalence estimates of gestational diabetes mellitus in the United States, pregnancy risk assessment monitoring system (PRAMS), 2007–2010. Prev. Chronic Dis. 2014, 11, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Vogel, J.P.; Betrán, A.P.; Vindevoghel, N.; Souza, J.P.; Torloni, M.R.; Zhang, J.; Tunçalp, Ö.; Mori, R.; Morisaki, N.; Ortiz-Panozo, E.; et al. Use of the Robson classification to assess caesarean section trends in 21 countries: A secondary analysis of two WHO multicountry surveys. Lancet Glob. Health 2015, 3, e260–e270. [Google Scholar] [CrossRef] [Green Version]
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.K.; Driscoll, A.K. Births: Final data for 2018. Natl. Vital Stat. Rep. 2019, 68, 1980–2018. [Google Scholar]
- EURO-PERISTAT Project with SCPE and EUROCAT. European Perinatal Health Report. The Health and Care of Pregnant Women and Babies in Europe in 2010. Available online: www.europeristat.com (accessed on 20 July 2020).
- Blencowe, H.; Krasevec, J.; de Onis, M.; Black, R.E.; An, X.; Stevens, G.A.; Borghi, E.; Hayashi, C.; Estevez, D.; Cegolon, L.; et al. National, regional, and worldwide estimates of low birthweight in 2015, with trends from 2000: A systematic analysis. Lancet Glob. Health 2019, 7, e849–e860. [Google Scholar] [CrossRef] [Green Version]
- Jeyabalan, A. Epidemiology of preeclampsia: Impact of obesity. Nutr. Rev. 2013, 71, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Dehli, A.C.; Galán, I.R.; Fernández-Somoano, A.; Navarrete-Muñoz, E.M.; Espada, M.; Vioque, J.; Tardón, A. Prevalencia de deficiencia e insuficiencia de vitamina D y factores asociados en mujeres embarazadas del norte de España. Nutr. Hosp. 2015, 31, 1633–1640. [Google Scholar] [CrossRef]
- Karras, S.; Paschou, S.A.; Kandaraki, E.; Anagnostis, P.; Annweiler, C.; Tarlatzis, B.C.; Hollis, B.W.; Grant, W.B.; Goulis, D.G. Hypovitaminosis D in pregnancy in the mediterranean region: A systematic review. Eur. J. Clin. Nutr. 2016, 70, 979–986. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, A.; García-Esteban, R.; Basterretxea, M.; Lertxundi, A.; Rodríguez-Bernal, C.; Iñiguez, C.; Rodriguez-Dehli, C.; Tardõn, A.; Espada, M.; Sunyer, J.; et al. Associations of maternal circulating 25-hydroxyvitamin D3 concentration with pregnancy and birth outcomes. BJOG Int. J. Obstet. Gynaecol. 2015, 122, 1695–1704. [Google Scholar] [CrossRef] [Green Version]
- Choi, R.; Kim, S.; Yoo, H.; Cho, Y.Y.; Kim, S.W.; Chung, J.H.; Oh, S.; Lee, S.-Y. High Prevalence of Vitamin D Deficiency in Pregnant Korean Women: The First trimester and the winter season as risk factors for vitamin D deficiency. Nutrients 2015, 7, 3427–3448. [Google Scholar] [CrossRef]
- Miliku, K.; Vinkhuyzen, A.; Blanken, L.M.; McGrath, J.J.; Eyles, D.W.; Burne, T.H.; Hofman, A.; Tiemeier, H.; Steegers, E.A.; Gaillard, R.; et al. Maternal vitamin D concentrations during pregnancy, fetal growth patterns, and risks of adverse birth outcomes. Am. J. Clin. Nutr. 2016, 103, 1514–1522. [Google Scholar] [CrossRef]
- Palacios, C.; Kostiuk, L.K.; Peñas-Rosas, J.P. Vitamin D supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2019, 7, CD008873. [Google Scholar] [CrossRef]
- Wagner, C.L.; Hollis, B.W. The implications of vitamin D Status during pregnancy on mother and her developing child. Front. Endocrinol. (Lausanne) 2018, 9, 500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heaney, R.P. Guidelines for optimizing design and analysis of clinical studies of nutrient effects. Nutr. Rev. 2014, 72, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Barrera, D.; Díaz, L.; Noyola-Martínez, N.; Halhali, A. Vitamin D and inflammatory cytokines in healthy and preeclamptic pregnancies. Nutrients 2015, 7, 6465–6490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tao, R.X.; Meng, D.H.; Li, J.J.; Tong, S.L.; Hao, J.H.; Huang, K.; Tao, F.B.; Zhu, P. Current recommended vitamin D prenatal supplementation and fetal growth: Results from the China-Anhui birth cohort study. J. Clin. Endocrinol. Metab. 2018, 103, 244–252. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | All Participants (n = 289) | Vitamin D < 20 ng/mL (n = 105) | Vitamin D ≥ 20 ng/mL (n = 184) | p-Value |
|---|---|---|---|---|
| Age | 33 (29–36) | 34 (30–35.5) | 32 (28–36) | 0.358 |
| Seasonality | 0.159 | |||
| Spring | 42 (14.5%) | 12 (11.4%) | 30 (16.3%) | |
| Summer | 21 (7.3%) | 5 (4.8%) | 16 (8.7%) | |
| Autumn | 216 (74.7%) | 82 (78.1%) | 134 (72.83%) | |
| Winter | 10 (3.5%) | 6 (5.7%) | 4 (2.17%) | |
| Smoking | 0.976 | |||
| Yes | 36 (12.5%) | 13 (12.4%) | 23 (12.5%) | |
| No | 253 (87.5%) | 92 (87.6%) | 161 (87.5%) | |
| Obesity | 0.01 * | |||
| BMI ≥ 30 | 52 (18%) | 27 (25.7%) | 25 (13.59%) | |
| BMI < 30 | 237 (82%) | 78 (74.3%) | 159 (86.41%) | |
| Parity | 0.198 | |||
| Nulliparity | 163 (56.4%) | 54 (51.4%) | 75 (40.76%) | |
| Multiparity | 126 (43.6%) | 51 (48.6%) | 109 (59.24%) | |
| Preterm birth | 17 (5.9%) | 10 (9.5%) | 7(3.8%) | 0.047 * |
| Low birth weight | 24 (8.3%) | 13 (12.4%) | 11 (6%) | 0.058 |
| Small for gestational age | 27 (9.3%) | 14 (13.3%) | 13 (7.1%) | 0.078 |
| Metabolite | All Participants (n = 289) | Vitamin D < 20 ng/mL (n = 105) | Vitamin D ≥ 20 ng/mL (n = 184) | p-Value |
|---|---|---|---|---|
| Parathyroid hormone | 21 (16–29.3) pg/mL | 25.50 (16.6–34.6) pg/mL | 19.6 (15.8–26.4) pg/mL | 0.002 * |
| Calcium | 9.2 (8.9–9.4) mg/dL | 9.2 (9–9.4) mg/dL | 9.2 (8.9–9.4) mg/dL | 0.914 |
| Phosphorus | 3.6 (3.4–3.9) mg/dL | 3.6 (3.4–3.9) mg/dL | 3.6 (3.4–3.9) mg/dL | 0.899 |
| Outcome | Frequency | Estimated Global Frequency | Estimated Frequency in the USA | Estimated Frequency in Europe |
|---|---|---|---|---|
| Preeclampsia | 1.7% | 4.6% (2010) [42] | 3% (2010) [42] | 5.3% (2010) [42] |
| Gestational diabetes mellitus | 5.6% | 16.9% (2013) [43] | 4.6–9.2% (2010) [44] | 15.2% (2013) [43] |
| Cesarean section | 21.5% | 31% (2011) [45] | 31.9% (2018) [46] | 25.2% (2010) [47] |
| Preterm birth | 5.9% | 10.6% (2014) [5] | 10.2% (2018) [46] | 8.7% (2014) [5] |
| Low birthweight | 8.3% | 14.6% (2015) [48] | 8.28% (2018) [46] | 6.5% (2015) [48] |
| Outcome | Vitamin D Deficiency | p-Value | Parathyroid Hormone | p-Value | Calcium | p-Value | Phosphorus | p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| Preterm Birth | Unadjusted OR | 2.662 (0.982–7.217) | 0.054 | 1.030 (1.002–1.058) | 0.035 * | 2.024 (0.581–7.048) | 0.268 | 1.021 (0.630–1.652) | 0.934 |
| Adjusted OR 1 | 3.529 (1.159–10.741) | 0.026 * | 1.027 (0.997–1.059) | 0.083 | 1.814 (0.513–6.413) | 0.355 | 0.764 (0.240–2.431) | 0.648 | |
| Low Birth Weight | Unadjusted OR | 2.222 (0.958–5.157) | 0.063 | 1.019 (0.993–1.046) | 0.156 | 1.572 (0.566–4.366) | 0.386 | 0.738 (0.282–1.927) | 0.535 |
| Adjusted OR 2 | 1.586 (0.586–4.336) | 0.361 | 1.009 (0.977–1.041) | 0.597 | 1.212 (0.355–4.144) | 0.758 | 0.568 (0.189–1.711) | 0.315 | |
| Small for Gestational Age | Unadjusted OR | 2.024 (0.912–4.488) | 0.083 | 0.985 (0.951–1.020) | 0.399 | 1.215 (0.488–3.022) | 0.676 | 0.735 (0.296–1.913) | 0.551 |
| Adjusted OR 3 | 1.794 (0.786–4.093) | 0.165 | 0.978 (0.939–1.018) | 0.276 | 1.127 (0.435–2.923) | 0.805 | 0.699 (0.269–1.818) | 0.463 | |
| Preterm Birth | Low Birth Weight | Small for GESTATIONAL Age | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n (%) | OR | aOR 1 | n (%) | OR | aOR 2 | n (%) | OR | aOR 3 | |
| 25[OH]D ≥ 20 ng/mL (≥50 nmol/L) | |||||||||
| PTH > 80th | 0/26 (0%) | -- | -- | 0/26 0% | -- | -- | 0/26 0% | -- | -- |
| PTH ≤ 80th | 7/158 (4.4%) | 0.561 (0.207–1.517) | 0.581 (0.203–1.667) | 11/158 (7%) | 0.679 (0.294–1.571) | 0.899 (0.333–2.432) | 13/158 (8.2%) | 0.749 (0.339–1.656) | 0.857 (0.376–1.954) |
| 25[OH]D < 20 ng/mL (<50 nmol/L) | |||||||||
| PTH > 80th | 6/31 (19.4%) | 5.389 (1.837–15.812) * | 6.223 (1.939–19.970) * | 7/31 (19.4%) | 4.135 (1.560–10.963) * | 2.653 (0.766–9.188) | 4/31 (12.9%) | 1.514 (0.487–4.705) | 1.356 [0.407–4.518] |
| PTH ≤ 80th | 4/74 (5.4%) | 0.888 (0.280–2.813) | 1.057 (0.313–1.357) | 6/74 (8.1%) | 0.966 (0.368–2.533) | 0.877 (0.268–2.868) | 10/74 (13.5%) | 1.820 (0.793–4.175) | 1.663 (0.705–3.919) |
| 25[OH]D ≥ 30 ng/mL (≥75 nmol/L) | |||||||||
| PTH > 80th | 0/4 (0%) | -- | -- | 0/4 0% | -- | -- | 0/4 0% | -- | -- |
| PTH ≤ 80th | 2/30 (6.7%) | 1.162 (0.253–5.346) | 1.480 (0.310–7.065) | 1/30 (3.3%) | 0.354 (0.460–2.718) | 0.257 (0.024–2.787) | 1/30 (3.3%) | 0.309 (0.040–2.363) | 0.324 (0.041–2.548) |
| 25[OH]D < 30 ng/mL (<75 nmol/L) | |||||||||
| PTH > 80th | 6/53 (11.3%) | 2.611 (0.920–7.411) | 2.109 (0.673–6.611) | 7/53 (13.2%) | 1.960 (0.769–4.998) | 1.402 (0.442–4.441) | 4/53 (7.5%) | 0.756 (0.250–2.285) | 0.713 (0.226–2.251) |
| PTH ≤ 80th | 9/202 (4.5%) | 0.460 (0.172–1.236) | 0.492 (0.171–1.419) | 16/202 (7.9%) | 0.849 (0.349–2.066) | 1.188 (0.391–3.615) | 22/202 (10.9%) | 2.004 (0.733–5.479) | 2.202 (0.772–6.181) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Castillo, Í.M.; Rivero-Blanco, T.; León-Ríos, X.A.; Expósito-Ruiz, M.; López-Criado, M.S.; Aguilar-Cordero, M.J. Associations of Vitamin D Deficiency, Parathyroid hormone, Calcium, and Phosphorus with Perinatal Adverse Outcomes. A Prospective Cohort Study. Nutrients 2020, 12, 3279. https://doi.org/10.3390/nu12113279
Pérez-Castillo ÍM, Rivero-Blanco T, León-Ríos XA, Expósito-Ruiz M, López-Criado MS, Aguilar-Cordero MJ. Associations of Vitamin D Deficiency, Parathyroid hormone, Calcium, and Phosphorus with Perinatal Adverse Outcomes. A Prospective Cohort Study. Nutrients. 2020; 12(11):3279. https://doi.org/10.3390/nu12113279
Chicago/Turabian StylePérez-Castillo, Íñigo María, Tania Rivero-Blanco, Ximena Alejandra León-Ríos, Manuela Expósito-Ruiz, María Setefilla López-Criado, and María José Aguilar-Cordero. 2020. "Associations of Vitamin D Deficiency, Parathyroid hormone, Calcium, and Phosphorus with Perinatal Adverse Outcomes. A Prospective Cohort Study" Nutrients 12, no. 11: 3279. https://doi.org/10.3390/nu12113279