Probiotic NVP-1703 Alleviates Allergic Rhinitis by Inducing IL-10 Expression: A Four-week Clinical Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Products
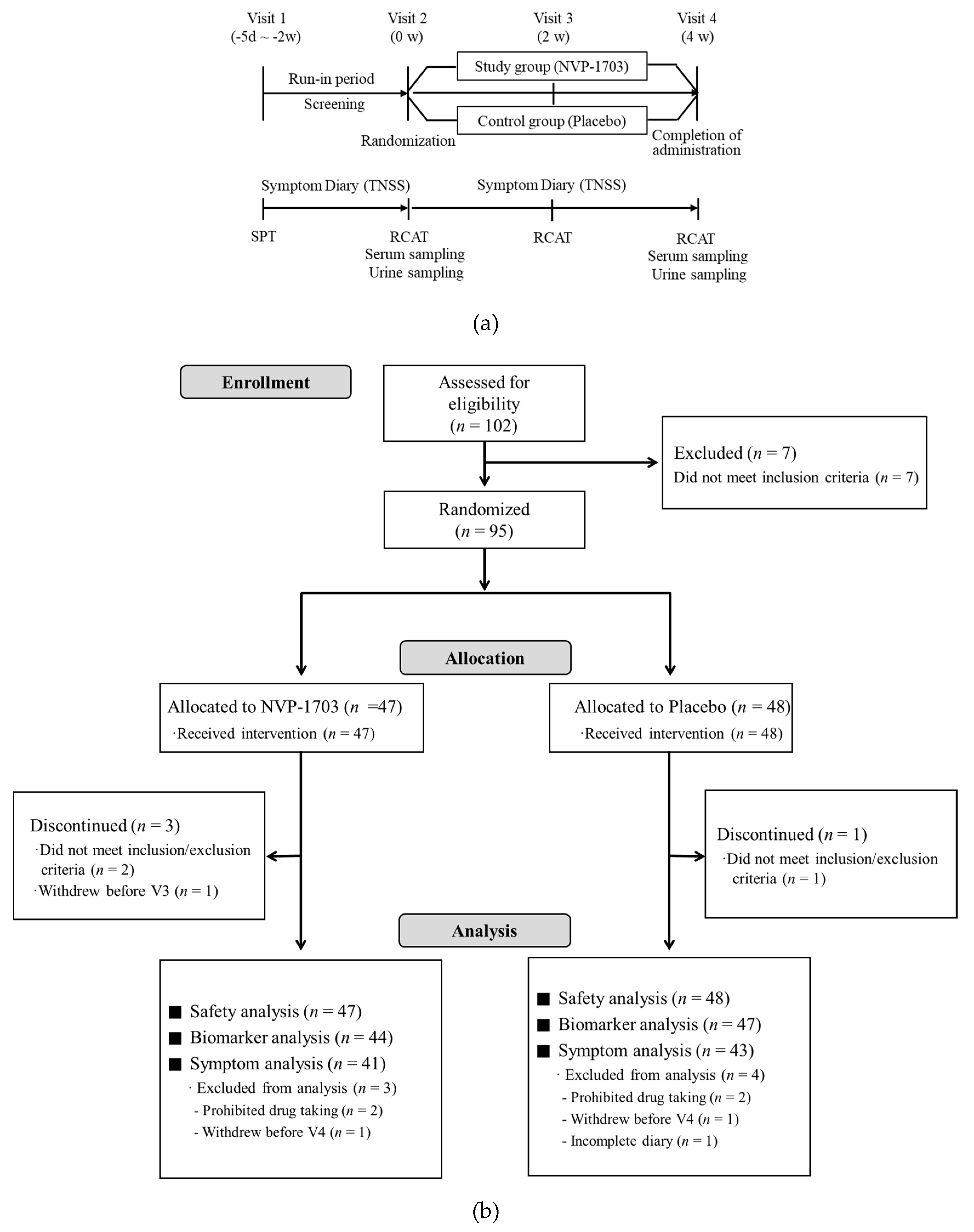
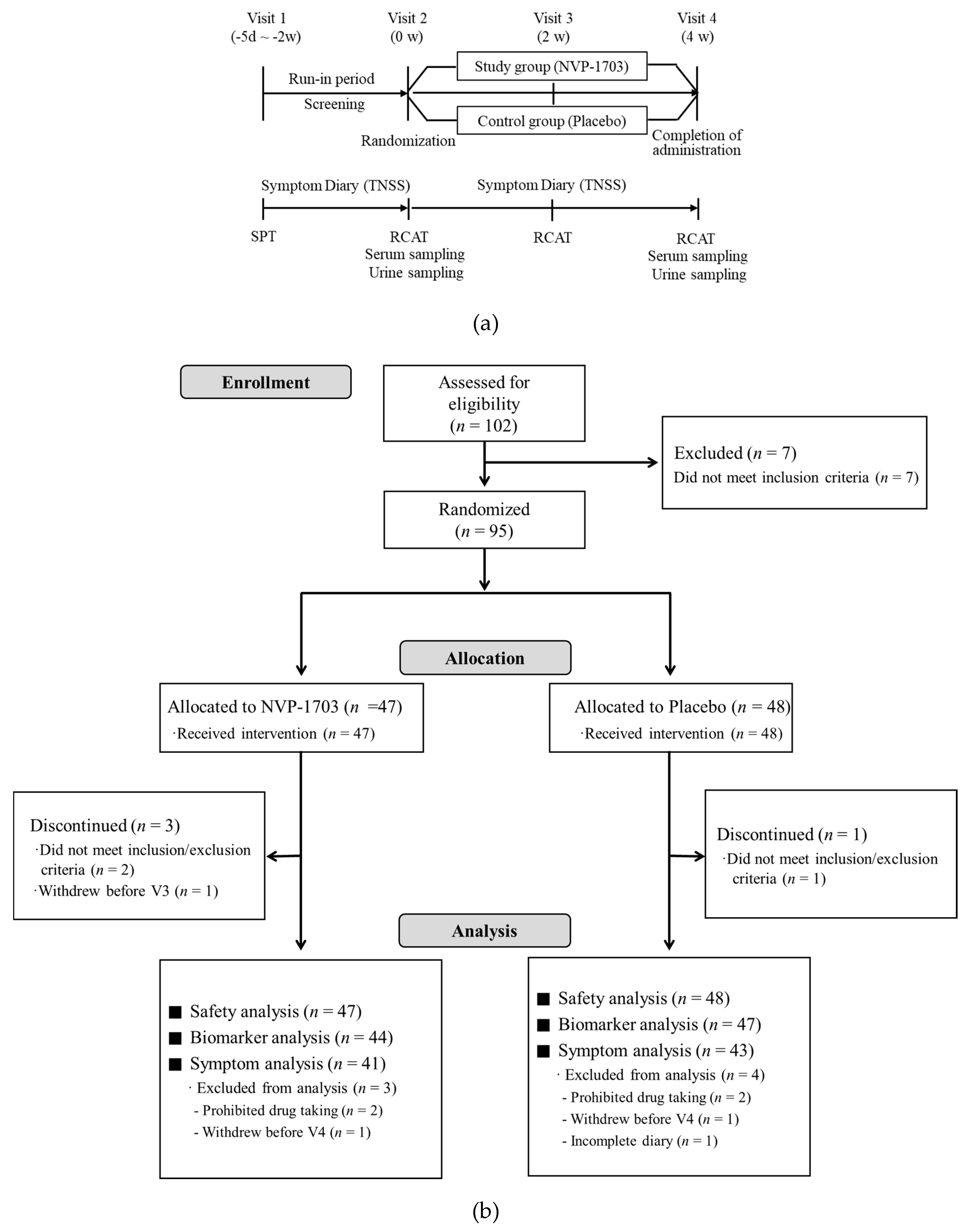
2.3. Study Design
2.4. TNSS
2.5. RCAT
2.6. Skin Prick Test
2.7. Measurement of Inflammatory Mediators in Serum and Urine
2.8. Statistical Analysis
3. Results
3.1. Study Subject Characteristics
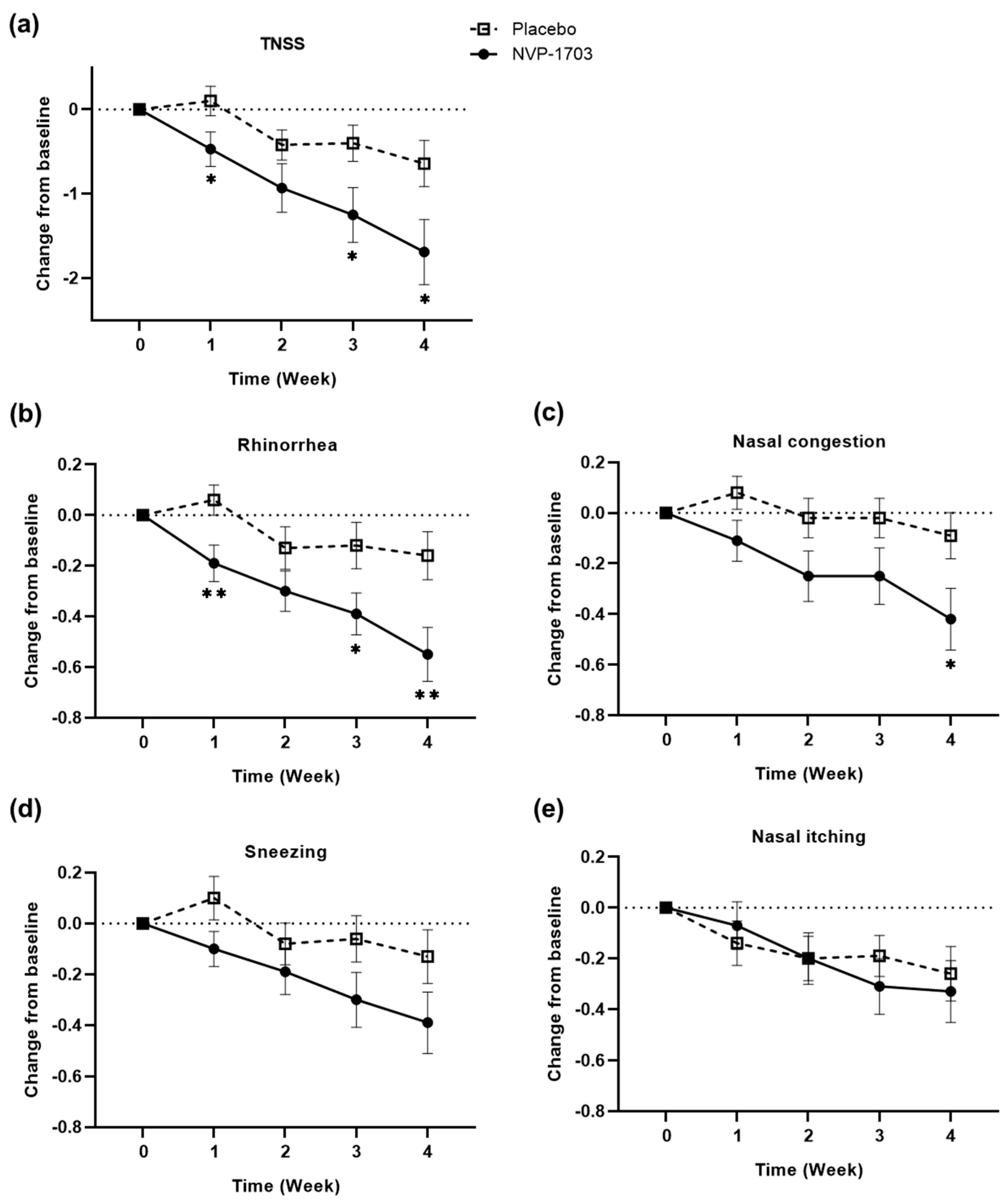
3.2. Changes from Baseline in TNSS
3.3. Changes from Baseline in RCAT
3.4. Effect of NVP-1703 on Blood Eosinophil Count and Serum Specific IgE
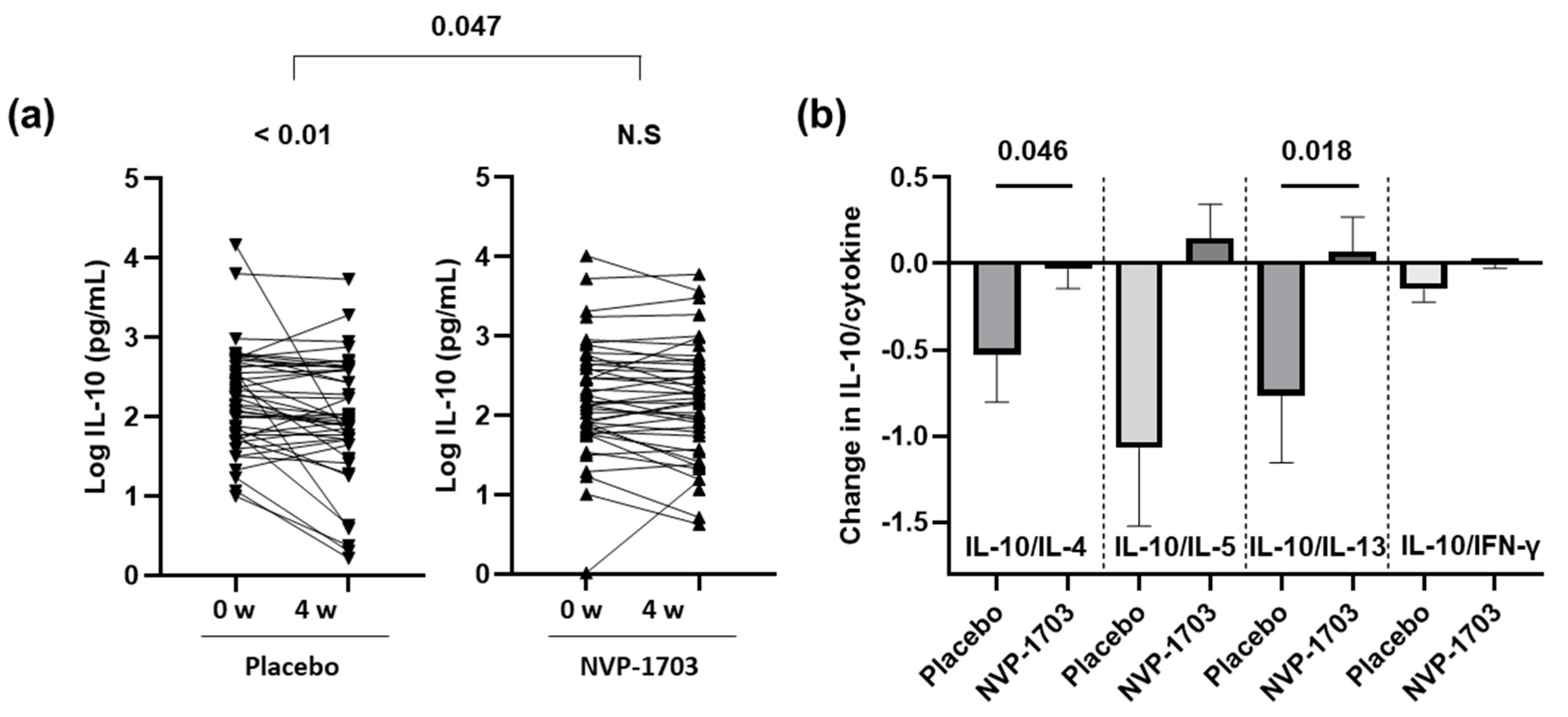
3.5. Effect of NVP-1703 on Serum Cytokines
3.6. Effect of NVP-1703 on Urinary LTE4 and PGF2α
3.7. Safety and Compliance
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bousquet, J.; Khaltaev, N.; Cruz, A.A.; Denburg, J.; Fokkens, W.J.; Togias, A.; Zuberbier, T.; Baena-Cagnani, C.E.; Canonica, G.W.; van Weel, C.; et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy 2008, 63, 8–160. [Google Scholar] [CrossRef]
- Baraniuk, J.N. Pathogenesis of allergic rhinitis. J. Allergy Clin. Immunol. 1997, 99, S763–S772. [Google Scholar] [CrossRef]
- Akdis, M.; Verhagen, J.; Taylor, A.; Karamloo, F.; Karagiannidis, C.; Crameri, R.; Thunberg, S.; Deniz, G.; Valenta, R.; Fiebig, H.; et al. Immune responses in healthy and allergic individuals are characterized by a fine balance between allergen-specific T regulatory 1 and T helper 2 cells. J. Exp. Med. 2004, 199, 1567–1575. [Google Scholar] [CrossRef] [PubMed]
- Coomes, S.M.; Kannan, Y.; Pelly, V.S.; Entwistle, L.J.; Guidi, R.; Perez-Lloret, J.; Nikolov, N.; Muller, W.; Wilson, M.S. CD4(+) Th2 cells are directly regulated by IL-10 during allergic airway inflammation. Mucosal Immunol. 2017, 10, 150–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Głobińska, A.; Boonpiyathad, T.; Satitsuksanoa, P.; Kleuskens, M.; van de Veen, W.; Sokolowska, M.; Akdis, M. Mechanisms of allergen-specific immunotherapy: Diverse mechanisms of immune tolerance to allergens. Ann. Allergy Asthma Immunol. 2018, 121, 306–312. [Google Scholar] [CrossRef]
- Singh, A.; Hacini-Rachinel, F.; Gosoniu, M.L.; Bourdeau, T.; Holvoet, S.; Doucet-Ladeveze, R.; Beaumont, M.; Mercenier, A.; Nutten, S. Immune-modulatory effect of probiotic Bifidobacterium lactis NCC2818 in individuals suffering from seasonal allergic rhinitis to grass pollen: An exploratory, randomized, placebo-controlled clinical trial. Eur. J. Clin. Nutr. 2013, 67, 161–167. [Google Scholar] [CrossRef]
- Ishida, Y.; Nakamura, F.; Kanzato, H.; Sawada, D.; Hirata, H.; Nishimura, A.; Kajimoto, O.; Fujiwara, S. Clinical effects of Lactobacillus acidophilus strain L-92 on perennial allergic rhinitis: A double-blind, placebo-controlled study. J. Dairy Sci. 2005, 88, 527–533. [Google Scholar] [CrossRef] [Green Version]
- Peng, Y.; Li, A.; Peng, Y.; Li, A.; Yu, L.; Qin, G. The role of probiotics in prevention and treatment for patients with allergic rhinitis: A systematic review. Am. J. Rhinol. Allergy 2015, 29, 292–298. [Google Scholar] [CrossRef]
- Miraglia Del Giudice, M.; Indolfi, C.; Capasso, M.; Maiello, N.; Decimo, F.; Ciprandi, G. Bifidobacterium mixture (B longum BB536, B infantis M-63, B breve M-16V) treatment in children with seasonal allergic rhinitis and intermittent asthma. Ital. J. Pediatr. 2017, 43, 25. [Google Scholar] [CrossRef] [Green Version]
- Zajac, A.E.; Adams, A.S.; Turner, J.H. In a systematic review and meta-analysis of probiotics for the treatment of allergic rhinitis. Int. Forum Allergy Rhinol. 2015, 5, 524–532. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.S.; Jan, R.L.; Lin, Y.L.; Chen, H.H.; Wang, J.Y. Randomized placebo-controlled trial of lactobacillus on asthmatic children with allergic rhinitis. Pediatr. Pulmonol. 2010, 45, 1111–1120. [Google Scholar] [CrossRef]
- Wassenberg, J.; Nutten, S.; Audran, R.; Barbier, N.; Aubert, V.; Moulin, J.; Mercenier, A.; Spertini, F. Effect of Lactobacillus paracasei ST11 on a nasal provocation test with grass pollen in allergic rhinitis. Clin. Exp. Allergy 2011, 41, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Ivory, K.; Chambers, S.J.; Pin, C.; Prieto, E.; Arques, J.L.; Nicoletti, C. Oral delivery of Lactobacillus casei Shirota modifies allergen-induced immune responses in allergic rhinitis. Clin. Exp. Allergy 2008, 38, 1282–1289. [Google Scholar] [CrossRef] [PubMed]
- Lue, K.H.; Sun, H.L.; Lu, K.H.; Ku, M.S.; Sheu, J.N.; Chan, C.H.; Wang, Y.H. A trial of adding Lactobacillus johnsonii EM1 to levocetirizine for treatment of perennial allergic rhinitis in children aged 7–12 years. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 994–1001. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.G.; Kang, G.D.; Kim, H.I.; Han, M.J.; Kim, D.H. Bifidobacterium longum IM55 and Lactobacillus plantarum IM76 alleviate allergic rhinitis in mice by restoring Th2/Treg imbalance and gut microbiota disturbance. Benef. Microbes 2019, 10, 55–67. [Google Scholar] [CrossRef]
- Kim, J.-K.; Kim, J.-Y.; Kim, H.I.; Han, M.J.; Kim, D.H. Bifidobacterium longum and Lactobacillus plantarum alleviate house dust mite allergen-induced allergic rhinitis by regulating IL-4, IL-5, and IL-10 expression. Food Agric. Immunol. 2019, 30, 581–593. [Google Scholar] [CrossRef] [Green Version]
- Lin, T.Y.; Chen, C.J.; Chen, L.K.; Wen, S.H.; Jan, R.H. Effect of probiotics on allergic rhinitis in Df, Dp or dust-sensitive children: A randomized double blind controlled trial. Indian Pediatr. 2013, 50, 209–213. [Google Scholar] [CrossRef]
- Yonekura, S.; Okamoto, Y.; Okawa, T.; Hisamitsu, M.; Chazono, H.; Kobayashi, K.; Sakurai, D.; Horiguchi, S.; Hanazawa, T. Effects of daily intake of Lactobacillus paracasei strain KW3110 on Japanese cedar pollinosis. Allergy Asthma Proc. 2009, 30, 397–405. [Google Scholar] [CrossRef]
- Nagata, Y.; Yoshida, M.; Kitazawa, H.; Araki, E.; Gomyo, T. Improvements in seasonal allergic disease with Lactobacillus plantarum No. 14. Biosci. Biotechnol. Biochem. 2010, 74, 1869–1877. [Google Scholar] [CrossRef] [Green Version]
- Jan, R.-H.; Chen, C.-J.; Chen, L.-K.; Wen, S.-H.; Lin, T.-Y. Is the effect of probiotics on allergic rhinitis confined to Dermatophagoides farinae, Dermatophagoides pteronyssinus, or dust-sensitive children? A randomized prospective double-blind controlled trial. Tzu Chi Med. J. 2011, 23, 51–54. [Google Scholar] [CrossRef] [Green Version]
- Kawase, M.; He, F.; Kubota, A.; Hiramatsu, M.; Saito, H.; Ishii, T.; Yasueda, H.; Akiyama, K. Effect of fermented milk prepared with two probiotic strains on Japanese cedar pollinosis in a double-blind placebo-controlled clinical study. Int. J. Food Microbiol. 2009, 128, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Costa, D.J.; Marteau, P.; Amouyal, M.; Poulsen, L.K.; Hamelmann, E.; Cazaubiel, M.; Housez, B.; Leuillet, S.; Stavnsbjerg, M.; Molimard, P.; et al. Efficacy and safety of the probiotic Lactobacillus paracasei LP-33 in allergic rhinitis: A double-blind, randomized, placebo-controlled trial (GA2LEN Study). Eur. J. Clin. Nutr. 2014, 68, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.Y.; Fu, L.S.; Lin, H.K.; Shen, C.Y.; Chen, Y.J. Evaluation of the effect of Lactobacillus paracasei (HF.A00232) in children (6–13 years old) with perennial allergic rhinitis: A 12-week, double-blind, randomized, placebo-controlled study. Pediatr. Neonatol. 2014, 55, 181–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.F.; Lin, H.C.; Wang, Y.Y.; Hsu, C.H. Treatment of perennial allergic rhinitis with lactic acid bacteria. Pediatr. Allergy Immunol. 2004, 15, 152–158. [Google Scholar] [CrossRef]
- Peng, G.C.; Hsu, C.H. The efficacy and safety of heat-killed Lactobacillus paracasei for treatment of perennial allergic rhinitis induced by house-dust mite. Pediatr. Allergy Immunol. 2005, 16, 433–438. [Google Scholar] [CrossRef]
- US Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research. Allergic Rhinitis: Developing Drug Products for Treatment Guidance for Industry. Draft Guidance. 2018. Available online: https://www.fda.gov/downloads/drugs/guidances/ucm071293.pdf (accessed on 4 April 2020).
- Lin, A.A.; Freeman, A.F.; Nutman, T.B. IL-10 Indirectly Downregulates IL-4-Induced IgE Production by Human B Cells. Immunohorizons 2018, 2, 398–406. [Google Scholar] [CrossRef]
- Royer, B.; Varadaradjalou, S.; Saas, P.; Guillosson, J.J.; Kantelip, J.P.; Arock, M. Inhibition of IgE-induced activation of human mast cells by IL-10. Clin. Exp. Allergy 2001, 31, 694–704. [Google Scholar] [CrossRef]
- Kennedy Norton, S.; Barnstein, B.; Brenzovich, J.; Bailey, D.P.; Kashyap, M.; Speiran, K.; Ford, J.; Conrad, D.; Watowich, S.; Moralle, M.R.; et al. IL-10 suppresses mast cell IgE receptor expression and signaling in vitro and in vivo. J. Immunol. 2008, 180, 2848–2854. [Google Scholar] [CrossRef] [Green Version]
- Peters-Golden, M.; Gleason, M.M.; Togias, A. Cysteinyl leukotrienes: Multi-functional mediators in allergic rhinitis. Clin. Exp. Allergy 2006, 36, 689–703. [Google Scholar] [CrossRef] [Green Version]
- Okano, M.; Fujiwara, T.; Sugata, Y.; Gotoh, D.; Masaoka, Y.; Sogo, M.; Tanimoto, W.; Yamamoto, M.; Matsumoto, R.; Eguchi, N.; et al. Presence and characterization of prostaglandin D2-related molecules in nasal mucosa of patients with allergic rhinitis. Am. J. Rhinol. 2006, 20, 342–348. [Google Scholar] [CrossRef]
- Kumlin, M. Measurement of leukotrienes in humans. Am. J. Respir. Crit. Care Med. 2000, 161, S102–S106. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.M.; O’Byrne, P.M.; Parameswaran, K. Leukotriene receptor antagonists for allergic rhinitis: A systematic review and meta-analysis. Am. J. Med. 2004, 116, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Güvenç, I.A.; Muluk, N.B.; Mutlu, F.Ş.; Eşki, E.; Altıntoprak, N.; Oktemer, T.; Cingi, C. Do Probiotics have a role in the Treatment of Allergic Rhinitis? A Comprehensive Systematic Review and Meta-analysis. Am. J. Rhinol. Allergy 2016, 30, e157–e175. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | NVP-1703 (n = 41) | Placebo (n = 43) | p-Value |
|---|---|---|---|
| Male [n (%)] | 10 (24.39) | 19 (44.19) | 0.057 |
| Age, years [mean (SEM)] | 33.61 (1.23) | 33.49 (1.33) | 0.947 |
| Duration of allergic rhinitis, months [mean (SEM)] | 175.41 (14.59) | 176.09 (13.46) | 0.923 |
| Family history of allergic diseases [n (%)] | 33 (80.49) | 33 (76.74) | 0.676 |
| Positivity of skin prick test [n (%)] | |||
| D. pteronyssinus | 38 (92.86) | 39 (90.70) | 1.000 |
| D. farinae | 38 (92.68) | 41 (95.35) | 0.672 |
| Mold 1 | 1 (2.44) | 2 (4.65) | 1.000 |
| Mold 2 | 0 | 1 (2.33) | 1.000 |
| Cat | 7 (17.07) | 5 (11.63) | 0.688 |
| Dog | 6 (14.63) | 5 (11.63) | 0.933 |
| Cockroach | 5 (12.20) | 4 (9.30) | 0.735 |
| Tree pollen mixture | 4 (9.76) | 9 (20.93) | 0.265 |
| Birch | 7 (17.07) | 11 (25.58) | 0.494 |
| Grass pollen mixture | 3 (7.32) | 4 (9.30) | 1.000 |
| Ragweed | 4 (9.76) | 3 (6.98) | 0.710 |
| Mugwort | 7 (17.07) | 5 (11.63) | 0.688 |
| Symptom score [mean (SEM)] | |||
| TNSS | 8.09 (0.29) | 7.55 (0.28) | 0.174 |
| Rhinorrhea | 2.29 (0.07) | 2.03 (0.09) | 0.031 |
| Nasal congestion | 2.12 (0.12) | 1.95 (0.12) | 0.292 |
| Sneezing | 1.88 (0.10) | 1.68 (0.12) | 0.203 |
| Itching | 1.81 (0.14) | 1.89 (0.12) | 0.661 |
| Parameter | Group | Symptom Score | ||||
|---|---|---|---|---|---|---|
| 0 w | 1 w | 2 w | 3 w | 4 w | ||
| TNSS | NVP-1703 | 8.09 (0.29) | 7.62 (0.29) * | 7.16 (0.35) *** | 6.84 (0.37) *** | 6.40 (0.41) *** |
| Placebo | 7.55 (0.28) | 7.65 (0.31) | 7.13 (0.33) * | 7.15 (0.34) | 6.90 (0.36) * | |
| p-Value † | 0.033 | 0.135 | 0.031 | 0.029 | ||
| Rhinorrhea | NVP-1703 | 2.29 (0.07) | 2.09 (0.09) * | 1.99 (0.09) *** | 1.90 (0.09) *** | 1.73 (0.11) *** |
| Placebo | 2.03 (0.09) | 2.10 (0.11) | 1.90 (0.11) | 1.91 (0.11) | 1.87 (0.11) | |
| p-Value † | 0.007 | 0.149 | 0.035 | 0.007 | ||
| Nasal congestion | NVP-1703 | 2.12 (0.12) | 2.02 (0.11) | 1.87 (0.12) * | 1.87 (0.12) * | 1.71 (0.12) ** |
| Placebo | 1.95 (0.12) | 2.03 (0.12) | 1.93 (0.11) | 1.93 (0.11) | 1.85 (0.12) | |
| p-Value † | 0.077 | 0.070 | 0.097 | 0.034 | ||
| Sneezing | NVP-1703 | 1.88 (0.10) | 1.77 (0.09) | 1.69 (0.10) * | 1.57 (0.12) ** | 1.49 (0.13) ** |
| Placebo | 1.68 (0.12) | 1.78 (0.10) | 1.60 (0.11) | 1.62 (0.12) | 1.55 (0.12) | |
| p-Value † | 0.069 | 0.374 | 0.087 | 0.103 | ||
| Itching | NVP-1703 | 1.81 (0.14) | 1.74 (0.11) | 1.61 (0.12) | 1.50 (0.13) ** | 1.47 (0.13) ** |
| Placebo | 1.89 (0.12) | 1.75 (0.11) | 1.69 (0.11) * | 1.69 (0.11) * | 1.63 (0.12) * | |
| p-Value † | 0.597 | 0.955 | 0.394 | 0.641 | ||
| Parameter | Group | Symptom Score | ||
|---|---|---|---|---|
| 0 w | 2 w | 4 w | ||
| Total | NVP-1703 | 15.44 (0.50) | 17.39 (0.62) ** | 19.27 (0.70) *** |
| Placebo | 15.26 (0.44) | 17.26 (0.51) *** | 17.47 (0.56) ** | |
| p-Value † | 0.957 | 0.049 | ||
| Nasal congestion | NVP-1703 | 1.95 (0.14) | 2.20 (0.15) | 2.63 (0.16) *** |
| Placebo | 2.00 (0.11) | 2.33 (0.12) ** | 2.35 (0.13) ** | |
| p-Value † | 0.523 | 0.086 | ||
| Sneezing | NVP-1703 | 2.27 (0.12) | 2.56 (0.12) ** | 2.83 (0.15) ** |
| Placebo | 2.19 (0.13) | 2.63 (0.13) ** | 2.51 (0.14) | |
| p-Value † | 0.483 | 0.143 | ||
| Watery eyes | NVP-1703 | 2.68 (0.15) | 3.05 (0.14) * | 3.49 (0.16) *** |
| Placebo | 2.88 (0.15) | 3.12 (0.16) | 3.05 (0.17) | |
| p-Value † | 0.933 | 0.018 | ||
| Interference of Sleep | NVP-1703 | 3.07 (0.12) | 3.29 (0.16) | 3.73 (0.14) *** |
| Placebo | 3.02 (0.14) | 3.26 (0.12) | 3.35 (0.14) | |
| p-Value † | 0.960 | 0.051 | ||
| Daily activities | NVP-1703 | 3.15 (0.15) | 3.39 (0.15) | 3.59 (0.18) * |
| Placebo | 2.91 (0.12) | 3.28 (0.13) * | 3.42 (0.12) ** | |
| p-Value † | 0.955 | 0.679 | ||
| Degree of rhinitis control | NVP-1703 | 2.32 (0.10) | 2.90 (0.12) *** | 3.00 (0.13) *** |
| Placebo | 2.26 (0.09) | 2.65 (0.12) * | 2.79 (0.12) ** | |
| p-Value † | 0.161 | 0.237 | ||
| Parameter | NVP-1703 | Placebo | |||
|---|---|---|---|---|---|
| 0 w | 4 w | 0 w | 4 w | p-Value † | |
| Blood eosinophil count (/μL) | 175.42 (16.21) | 96.82 (25.24) *** | 178.24 (17.14) | 56.61 (14.35) *** | 0.116 |
| D. pteronyssinus-specific IgE (KU/L) | 7.61 (1.14) | 7.15 (1.04) | 8.92 (1.18) | 8.93 (1.22) | 0.331 |
| D. farinae-specific IgE (KU/L) | 14.75 (2.17) | 12.83 (1.78) ** | 16.86 (2.20) | 17.19 (2.35) | 0.033 |
| IL-4 (log pg/mL) | 2.29 (0.12) | 2.31 (0.12) | 2.28 (0.12) | 2.28 (0.12) | 0.940 |
| IL-5 (log pg/mL) | 1.65 (0.12) | 1.59 (0.14) | 1.36 (0.12) | 1.34 (0.11) | 0.605 |
| IL-10 (log pg/mL) | 2.22 (0.11) | 2.16 (0.11) | 2.23 (0.09) | 1.97 (0.11)** | 0.047 |
| IL-13 (log pg/mL) | 1.49 (0.10) | 1.47 (0.12) | 1.55 (0.10) | 1.51 (0.10) | 0.936 |
| IFN-γ (log pg/mL) | 2.99 (0.08) | 2.98 (0.09) | 2.85 (0.08) | 2.84 (0.08) | 0.488 |
| IL-10/IL-4 | 1.21 (0.15) | 1.17 (0.16) | 1.42 (0.28) | 0.90 (0.09) | 0.046 |
| IL-10/IL-5 | 2.15 (0.24) | 2.27 (0.27) | 3.30 (0.47) | 2.27 (0.22) * | 0.088 |
| IL-10/IL-13 | 2.73 (0.42) | 2.77 (0.44) | 2.71 (0.41) | 1.95 (0.17) | 0.018 |
| IL-10/IFN-γ | 0.53 (0.05) | 0.52 (0.05) | 0.64 (0.08) | 0.49 (0.04) | 0.177 |
| Urinary LTE4 (ng/mmol Cr) | 601.06 (32.53) | 585.78 (31.24) | 546.95 (32.18) | 541.23 (32.31) | 0.701 |
| Urinary PGF2α (ng/mmol Cr) | 77.23 (7.66) | 69.90 (7.90) | 74.19 (6.82) | 72.13 (6.27) | 0.809 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, M.-G.; Han, S.-W.; Kang, H.-R.; Hong, S.-J.; Kim, D.-H.; Choi, J.-H. Probiotic NVP-1703 Alleviates Allergic Rhinitis by Inducing IL-10 Expression: A Four-week Clinical Trial. Nutrients 2020, 12, 1427. https://doi.org/10.3390/nu12051427
Kang M-G, Han S-W, Kang H-R, Hong S-J, Kim D-H, Choi J-H. Probiotic NVP-1703 Alleviates Allergic Rhinitis by Inducing IL-10 Expression: A Four-week Clinical Trial. Nutrients. 2020; 12(5):1427. https://doi.org/10.3390/nu12051427
Chicago/Turabian StyleKang, Min-Gyu, Seung-Won Han, Hye-Ryun Kang, Seok-Jin Hong, Dong-Hyun Kim, and Jeong-Hee Choi. 2020. "Probiotic NVP-1703 Alleviates Allergic Rhinitis by Inducing IL-10 Expression: A Four-week Clinical Trial" Nutrients 12, no. 5: 1427. https://doi.org/10.3390/nu12051427
APA StyleKang, M. -G., Han, S. -W., Kang, H. -R., Hong, S. -J., Kim, D. -H., & Choi, J. -H. (2020). Probiotic NVP-1703 Alleviates Allergic Rhinitis by Inducing IL-10 Expression: A Four-week Clinical Trial. Nutrients, 12(5), 1427. https://doi.org/10.3390/nu12051427