Diet and Nutraceutical Supplementation in Dyslipidemic Patients: First Results of an Italian Single Center Real-World Retrospective Analysis

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
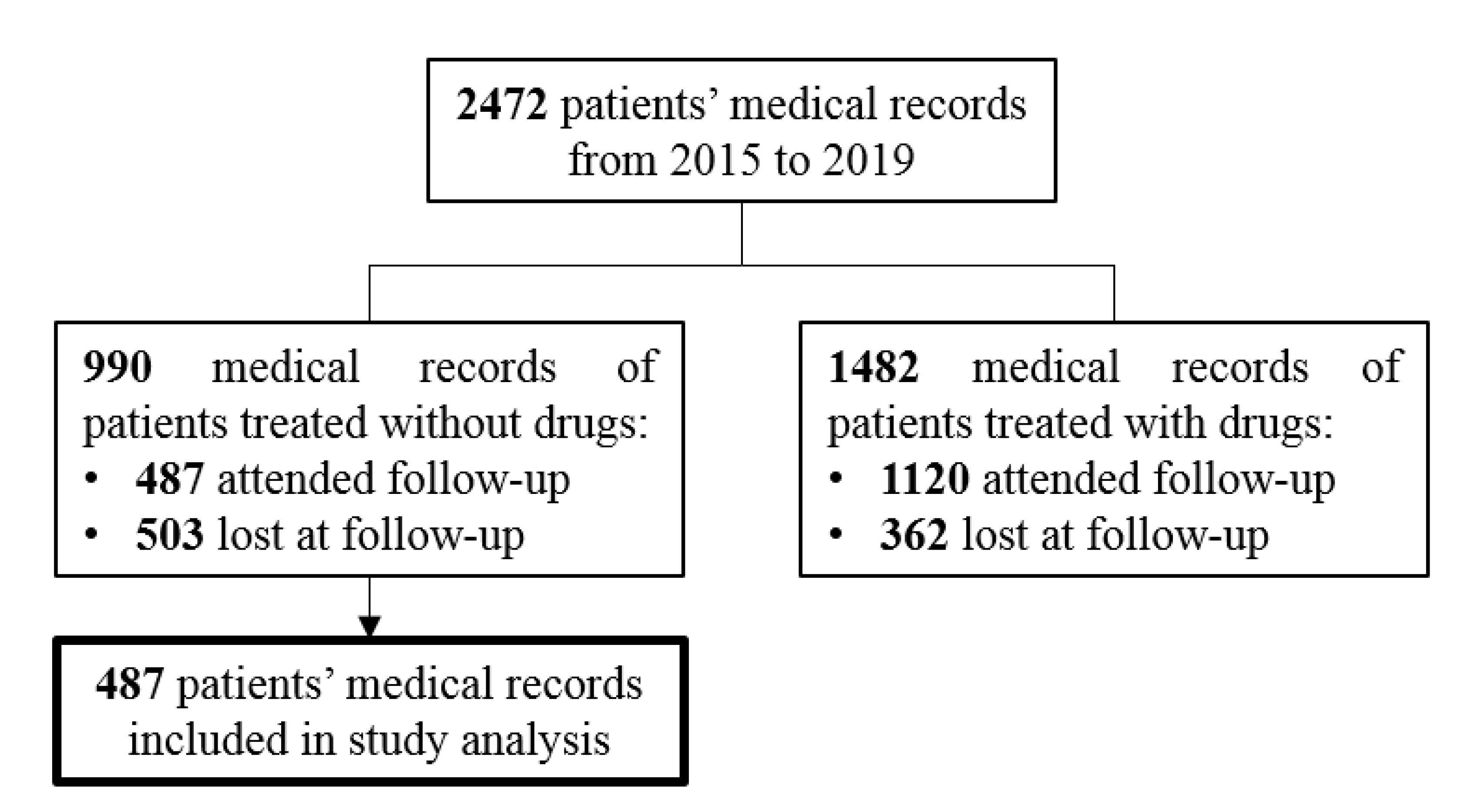
2.1. Subjects
2.2. Data Collection and Ranking Methods
2.3. Lifestyle Intervention
- General advice to reduce the excess of saturated fats and cholesterol intake based on weekly food frequency in normal weight patients with primary hypercholesterolemia
- General advice to reduce the excess of carbohydrates and alcohol based on weekly food frequency in normal weight patients with hypertriglyceridemia or mixed hyperlipemia
- Diet with weekly food frequency and total energy intake of 1700 kcal/day in overweight women
- Diet with weekly food frequency and total energy intake of 2100 kcal/day in overweight men.
2.4. Statistical Analysis
3. Results
3.1. Baseline Population Characteristics
3.2. Effect of Diet Alone Treatment
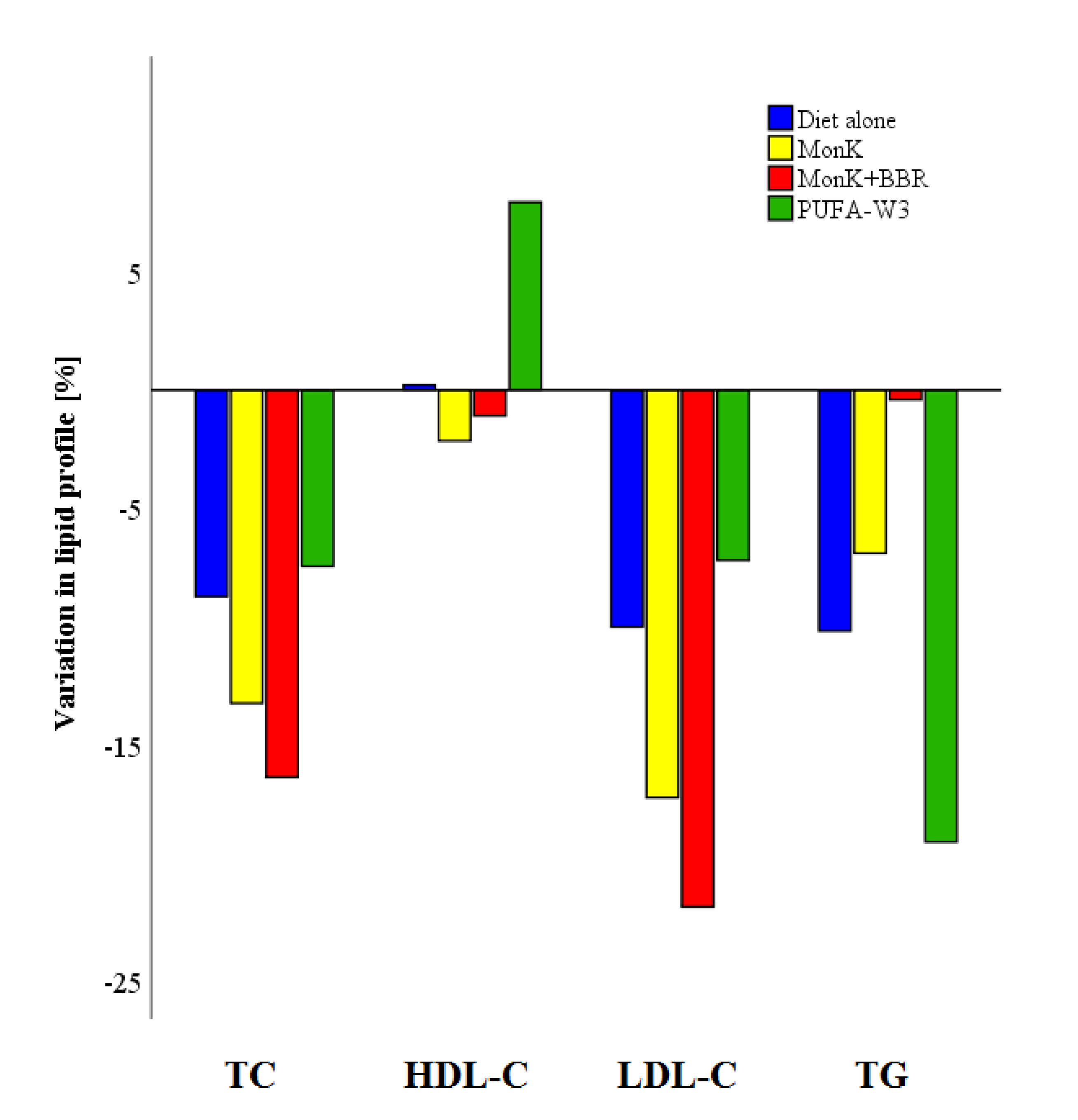
3.3. Effect of Lipid Lowering Nutraceuticals
3.4. Lipid Lowering Intervention and Therapeutic Targets
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ASCVD | atherosclerotic cardiovascular disease |
| LDL-C | low-density lipoprotein cholesterol |
| TC | total cholesterol |
| HDL-C | high-density lipoprotein cholesterol |
| TG | triglycerides |
| PCSK9 | proprotein convertase subtilisin/kexin type 9 |
| BMI | body mass index |
| NUT | lipid lowering nutraceutical |
| MonK | Monacolin K |
| PS | Phytosterols |
| BBR | Berberine |
| PUFA-W3 | Fatty acids - ω3 |
| n | number |
References
- Yu, J.N.; Cunningham, J.A.; Thouin, S.R.; Gurvich, T.; Liu, D. Hyperlipidemia. Prim. Care 2000, 27, 541–587. [Google Scholar] [CrossRef]
- Nelson, R.H. Hyperlipidemia as a Risk Factor for Cardiovascular Disease. Prim. Care 2013, 40, 195–211. [Google Scholar] [CrossRef] [PubMed]
- Roy, S. Atherosclerotic Cardiovascular Disease Risk and Evidence-based Management of Cholesterol. N Am. J. Med. Sci. 2014, 6, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Cabezas, M.C.; Burggraaf, B.; Klop, B. Dyslipidemias in clinical practice. Clin. Chim. Acta 2018, 487, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Scherer, J.; Singh, V.P.; Pitchumoni, C.S.; Yadav, D. Issues in hypertriglyceridemic pancreatitis: An update. J. Clin. Gastroenterol. 2014, 48, 195–203. [Google Scholar] [CrossRef]
- Vega, G.L.; Grundy, S.M. Hypoalphalipoproteinemia (low high density lipoprotein) as a risk factor for coronary heart disease. Curr. Opin. Lipidol. 1996, 7, 209–216. [Google Scholar] [CrossRef]
- Ziaeian, B.; Fonarow, G.C. Statins and the Prevention of Heart Disease. JAMA Cardiol. 2017, 2, 464. [Google Scholar] [CrossRef]
- Sampson, U.K.; Fazio, S.; Linton, M.F. Residual cardiovascular risk despite optimal LDL cholesterol reduction with statins: The evidence, etiology, and therapeutic challenges. Curr. Atheroscler. Rep. 2012, 14, 1–10. [Google Scholar] [CrossRef]
- Toth, P.P.; Catapano, A.; Tomassini, J.E.; Tershakovec, A.M. Update on the efficacy and safety of combination ezetimibe plus statin therapy. Clin. Lipidol. 2010, 5, 655–684. [Google Scholar] [CrossRef]
- Morrone, D.; Weintraub, W.S.; Toth, P.P.; Hanson, M.E.; Lowe, R.S.; Lin, J.; Shah, A.K.; Tershakovec, A.M. Lipid-altering efficacy of ezetimibe plus statin and statin monotherapy and identification of factors associated with treatment response: A pooled analysis of over 21,000 subjects from 27 clinical trials. Atherosclerosis 2012, 223, 251–261. [Google Scholar] [CrossRef]
- Pasta, A.; Cremonini, A.L.; Pisciotta, L.; Buscaglia, A.; Porto, I.; Barra, F.; Ferrero, S.; Brunelli, C.; Rosa, G.M. PCSK9 inhibitors for treating hypercholesterolemia. Expert Opin. Pharm. 2020, 21, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Remick, J.; Weintraub, H.; Setton, R.; Offenbacher, J.; Fisher, E.; Schwartzbard, A. Fibrate therapy: An update. Cardiol. Rev. 2008, 16, 129–141. [Google Scholar] [CrossRef] [PubMed]
- Catapano, A.L.; Graham, I.; De Backer, G.; Wiklund, O.; Chapman, M.J.; Drexel, H.; Hoes, A.W.; Jennings, C.S.; Landmesser, U.; Pedersen, T.R.; et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias. Eur. Heart J. 2016, 37, 2999–3058. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef]
- American Heart Association Nutrition Committee; Lichtenstein, A.H.; Appel, L.J.; Brands, M.; Carnethon, M.; Daniels, S.; Franch, H.A.; Franklin, B.; Kris-Etherton, P.; Harris, W.S. Diet and lifestyle recommendations revision 2006: A scientific statement from the American Heart Association Nutrition Committee. Circulation 2006, 114, 82–96. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Lagiou, P. Healthy traditional Mediterranean diet: An expression of culture, history, and lifestyle. Nutr. Rev. 1997, 55, 383–389. [Google Scholar] [CrossRef]
- Brinton, E.A. Management of Hypertriglyceridemia for Prevention of Atherosclerotic Cardiovascular Disease. Endocrinol. Metab. Clin. N. Am. 2016, 45, 185–204. [Google Scholar] [CrossRef]
- Obarzanek, E.; Sacks, F.M.; Vollmer, W.M.; Bray, G.A.; Miller, E.R.; Lin, P.H.; Karanja, N.M.; Most-Windhauser, M.M.; Moore, T.J.; Swain, J.F.; et al. Effects on blood lipids of a blood pressure-lowering diet: The Dietary Approaches to Stop Hypertension (DASH) Trial. Am. J. Clin. Nutr. 2001, 74, 80–89. [Google Scholar] [CrossRef]
- Appel, L.J.; Sacks, F.M.; Carey, V.J.; Obarzanek, E.; Swain, J.F.; Miller, E.R.; Conlin, P.R.; Erlinger, T.P.; Rosner, B.A.; Laranjo, N.M.; et al. Effects of protein, monounsaturated fat, and carbohydrate intake on blood pressure and serum lipids: Results of the OmniHeart randomized trial. JAMA 2005, 294, 2455–2464. [Google Scholar] [CrossRef]
- Ginsberg, H.N.; Kris-Etherton, P.; Dennis, B.; Elmer, P.J.; Ershow, A.; Lefevre, M.; Pearson, T.; Roheim, P.; Ramakrishnan, R.; Reed, R.; et al. Effects of reducing dietary saturated fatty acids on plasma lipids and lipoproteins in healthy subjects: The DELTA Study, protocol 1. Arter. Thromb. Vasc. Biol. 1998, 18, 441–449. [Google Scholar] [CrossRef]
- Schaefer, E.J.; Lamon-Fava, S.; Ausman, L.M.; Ordovas, J.M.; Clevidence, B.A.; Judd, J.T.; Goldin, B.R.; Woods, M.; Gorbach, S.; Lichtenstein, A.H. Individual variability in lipoprotein cholesterol response to National Cholesterol Education Program Step 2 diets. Am. J. Clin. Nutr. 1997, 65, 823–830. [Google Scholar] [CrossRef]
- Banach, M.; Patti, A.M.; Giglio, R.V.; Cicero, A.F.G.; Atanasov, A.G.; Bajraktari, G.; Bruckert, E.; Descamps, O.; Djuric, D.M.; Ezhov, M.; et al. The Role of Nutraceuticals in Statin Intolerant Patients. J. Am. Coll. Cardiol. 2018, 72, 96–118. [Google Scholar] [CrossRef]
- Patti, A.M.; Toth, P.P.; Giglio, R.V.; Banach, M.; Noto, M.; Nikolic, D.; Montalto, G.; Rizzo, M. Nutraceuticals as an Important Part of Combination Therapy in Dyslipidaemia. Curr. Pharm. Des. 2017, 23, 2496–2503. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Colletti, A.; Bajraktari, G.; Descamps, O.; Djuric, D.M.; Ezhov, M.; Fras, Z.; Katsiki, N.; Langlois, M.; Latkovskis, G.; et al. Lipid-lowering nutraceuticals in clinical practice: Position paper from an International Lipid Expert Panel. Nutr. Rev. 2017, 75, 731–767. [Google Scholar] [CrossRef]
- Backes, J.; Anzalone, D.; Hilleman, D.; Catini, J. The clinical relevance of omega-3 fatty acids in the management of hypertriglyceridemia. Lipids Health Dis. 2016, 15, 118. [Google Scholar] [CrossRef]
- Arca, M.; Borghi, C.; Pontremoli, R.; De Ferrari, G.M.; Colivicchi, F.; Desideri, G.; Temporelli, P.L. Hypertriglyceridemia and omega-3 fatty acids: Their often overlooked role in cardiovascular disease prevention. Nutr. Metab. Cardiovasc Dis. 2018, 28, 197–205. [Google Scholar] [CrossRef]
- McKenney, J.M.; Sica, D. Role of prescription omega-3 fatty acids in the treatment of hypertriglyceridemia. Pharmacotherapy 2007, 27, 715–728. [Google Scholar] [CrossRef]
- Nota 13|Agenzia Italiana del Farmaco. Available online: https://aifa.gov.it/nota-13 (accessed on 15 March 2020).
- Conroy, R.M.; Pyörälä, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G.; De Bacquer, D.; Ducimetière, P.; Jousilahti, P.; Keil, U.; et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE project. Eur. Heart J. 2003, 24, 987–1003. [Google Scholar] [CrossRef]
- Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults—The Evidence Report. National Institutes of Health; National Heart, Lung, and Blood Institute: Bethesda, MD, USA, 1998; Volume 6, (Suppl. 2), pp. 51S–209S.
- Population Structure and Ageing—Statistics Explained. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Population_structure_and_ageing#Median_age_is_highest_in_Italy (accessed on 25 April 2020).
- Chung, M.L.; Lennie, T.A.; Mudd-Martin, G.; Moser, D.K. Adherence to the Low Sodium Diet in Patients with Heart Failure is Best When Family Members Also Follow the Diet: A Multicenter Observational Study. J. Cardiovasc Nurs. 2015, 30, 44–50. [Google Scholar] [CrossRef]
- Ayele, A.A.; Emiru, Y.K.; Tiruneh, S.A.; Ayele, B.A.; Gebremariam, A.D.; Tegegn, H.G. Level of adherence to dietary recommendations and barriers among type 2 diabetic patients: A cross-sectional study in an Ethiopian hospital. Clin. Diabetes Endocrinol. 2018, 4, 21. [Google Scholar] [CrossRef] [PubMed]
- Mirahmadizadeh, A.; Khorshidsavar, H.; Seif, M.; Sharifi, M.H. Adherence to Medication, Diet and Physical Activity and the Associated Factors Amongst Patients with Type 2 Diabetes. Diabetes 2020, 11, 479–494. [Google Scholar] [CrossRef]
- Karalis, D.G. A Review of Clinical Practice Guidelines for the Management of Hypertriglyceridemia: A Focus on High Dose Omega-3 Fatty Acids. Adv. Ther. 2017, 34, 300–323. [Google Scholar] [CrossRef] [PubMed]
- Kolovou, G.D.; Anagnostopoulou, K.K.; Damaskos, D.S.; Bilianou, H.I.; Mihas, C.; Milionis, H.J.; Kostakou, P.M.; Cokkinos, D.V. Gender differences in the lipid profile of dyslipidemic subjects. Eur. J. Intern. Med. 2009, 20, 145–151. [Google Scholar] [CrossRef] [PubMed]
- da Silva, P.M.; Aguiar, C.; Morais, J. DISGEN-LIPID study Investigators Suboptimal lipid levels in clinical practice among Portuguese adults with dyslipidemia under lipid-lowering therapy: Data from the DISGEN-LIPID study. Rev. Port. Cardiol. 2019, 38, 559–569. [Google Scholar] [CrossRef]
- Tan, N.C.; Koh, E.Y.L.; Goh, C.C.; Goh, P.S.C.; Koh, K.H. A cross-sectional study of gender differences in lifestyle behavior and usage of medications among community-dwelling Asians towards achieving their LDL-Cholesterol treatment goals. Proc. Singap. Healthc. 2017, 26, 158–165. [Google Scholar] [CrossRef]
- Wang, H.; Peng, D.-Q. New insights into the mechanism of low high-density lipoprotein cholesterol in obesity. Lipids Health Dis 2011, 10, 176. [Google Scholar] [CrossRef]
- Wakabayashi, I.; Daimon, T. Associations between hypo-HDL cholesterolemia and cardiometabolic risk factors in middle-aged men and women: Independence of habitual alcohol drinking, smoking and regular exercise. Obes Res. Clin. Pr. 2017, 11, 324–334. [Google Scholar] [CrossRef]
- Merianos, A.L.; Jandarov, R.A.; Khoury, J.C.; Mahabee-Gittens, E.M. Tobacco Smoke Exposure Association with Lipid Profiles and Adiposity Among U.S. Adolescents. J. Adolesc Health 2018, 62, 463–470. [Google Scholar] [CrossRef]
- Becker, D.J.; Gordon, R.Y.; Halbert, S.C.; French, B.; Morris, P.B.; Rader, D.J. Red yeast rice for dyslipidemia in statin-intolerant patients: A randomized trial. Ann. Intern. Med. 2009, 150, 830–839. [Google Scholar] [CrossRef]
- Bogsrud, M.P.; Ose, L.; Langslet, G.; Ottestad, I.; Strøm, E.C.; Hagve, T.-A.; Retterstøl, K. HypoCol (red yeast rice) lowers plasma cholesterol—A randomized placebo controlled study. Scand. Cardiovasc. J. 2010, 44, 197–200. [Google Scholar] [CrossRef]
- Ogier, N.; Amiot, M.-J.; Georgé, S.; Maillot, M.; Mallmann, C.; Maraninchi, M.; Morange, S.; Lescuyer, J.-F.; Peltier, S.L.; Cardinault, N. LDL-cholesterol-lowering effect of a dietary supplement with plant extracts in subjects with moderate hypercholesterolemia. Eur. J. Nutr. 2013, 52, 547–557. [Google Scholar] [CrossRef]
- Barrat, E.; Zaïr, Y.; Ogier, N.; Housez, B.; Vergara, C.; Maudet, C.; Lescuyer, J.-F.; Bard, J.-M.; Carpentier, Y.A.; Cazaubiel, M.; et al. A combined natural supplement lowers LDL cholesterol in subjects with moderate untreated hypercholesterolemia: A randomized placebo-controlled trial. Int J. Food Sci. Nutr. 2013, 64, 882–889. [Google Scholar] [CrossRef]
- Barrat, E.; Zaïr, Y.; Sirvent, P.; Chauveau, P.; Maudet, C.; Housez, B.; Derbord, E.; Lescuyer, J.-F.; Bard, J.-M.; Cazaubiel, M.; et al. Effect on LDL-cholesterol of a large dose of a dietary supplement with plant extracts in subjects with untreated moderate hypercholesterolaemia: A randomised, double-blind, placebo-controlled study. Eur. J. Nutr. 2013, 52, 1843–1852. [Google Scholar] [CrossRef] [PubMed]
- Higashikawa, F.; Noda, M.; Awaya, T.; Ushijima, M.; Sugiyama, M. Reduction of serum lipids by the intake of the extract of garlic fermented with Monascus pilosus: A randomized, double-blind, placebo-controlled clinical trial. Clin. Nutr. 2012, 31, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Barrios, V.; Escobar, C.; Cicero, A.F.G.; Burke, D.; Fasching, P.; Banach, M.; Bruckert, E. A nutraceutical approach (Armolipid Plus) to reduce total and LDL cholesterol in individuals with mild to moderate dyslipidemia: Review of the clinical evidence. Atheroscler. Suppl. 2017, 24, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Formisano, E.; Pasta, A.; Cremonini, A.L.; Favari, E.; Ronca, A.; Carbone, F.; Semino, T.; Di Pierro, F.; Sukkar, S.G.; Pisciotta, L. Efficacy of Nutraceutical Combination of Monacolin K, Berberine, and Silymarin on Lipid Profile and PCSK9 Plasma Level in a Cohort of Hypercholesterolemic Patients. J. Med. Food 2019. [Google Scholar] [CrossRef] [PubMed]
- Adorni, M.P.; Ferri, N.; Marchianò, S.; Trimarco, V.; Rozza, F.; Izzo, R.; Bernini, F.; Zimetti, F. Effect of a novel nutraceutical combination on serum lipoprotein functional profile and circulating PCSK9. Clin. Risk Manag. 2017, 13, 1555–1562. [Google Scholar] [CrossRef] [PubMed]
- Eslick, G.D.; Howe, P.R.C.; Smith, C.; Priest, R.; Bensoussan, A. Benefits of fish oil supplementation in hyperlipidemia: A systematic review and meta-analysis. Int. J. Cardiol. 2009, 136, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Abramson, J. Statins in Persons at Low Risk of Cardiovascular Disease. Am. Fam Physician 2017, 96. [Google Scholar]
- Cholesterol Treatment Trialists’ (CTT) Collaborators; Mihaylova, B.; Emberson, J.; Blackwell, L.; Keech, A.; Simes, J.; Barnes, E.H.; Voysey, M.; Gray, A.; Collins, R. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: Meta-analysis of individual data from 27 randomised trials. Lancet 2012, 380, 581–590. [Google Scholar] [CrossRef]
- Ridker, P.M.; Pradhan, A.; MacFadyen, J.G.; Libby, P.; Glynn, R.J. Cardiovascular benefits and diabetes risks of statin therapy in primary prevention: An analysis from the JUPITER trial. Lancet 2012, 380, 565–571. [Google Scholar] [CrossRef]
- Ramkumar, S.; Raghunath, A.; Raghunath, S. Statin Therapy: Review of Safety and Potential Side Effects. Acta Cardiol. Sin. 2016, 32, 631–639. [Google Scholar] [CrossRef]
- Pedan, A.; Varasteh, L.; Schneeweiss, S. Analysis of factors associated with statin adherence in a hierarchical model considering physician, pharmacy, patient, and prescription characteristics. J. Manag. Care Pharm. 2007, 13, 487–496. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Diet Alone | Diet + Nut |
|---|---|---|
| Sex [F/M: n; %] | 117 (56.5%)/90 (43.5%) | 169 (60.4%)/111 (39.6%) |
| Age | ||
| [years: mean±SD; median; IQ range] | 50 ± 15; 51 (40, 60) | 52 ± 13; 52 (43, 61) |
| [<45 years/≥45 years: n, %] | 78 (37.7%)/129 (62.3%) | 88 (31.4%)/192 (68.6%) |
| Weight | ||
| [kg: mean±SD; median; IQ range] | 71.0 ± 15.5; 69.0 (60.0, 81.0) | 69.2 ± 14.3; 69.7 (60.0, 77.0) |
| BMI | ||
| [kg/m2: mean±SD; median; IQ range] | 25.2 ± 4.3; 24.7 (22.1, 28.0) | 24.8 ± 3.8; 24.3 (22.5, 26.8) |
| [<25 kg/m2/≥25 kg/m2] | 110 (53.1%)/97 (46.9%) | 166 (59.3%)/114 (40.7%) |
| SBP | ||
| [mm/Hg: mean ± SD; median; IQ range] | 126 ± 2; 126 (125, 128) | 127 ± 2; 127 (125, 128) |
| DBP | ||
| [mm/Hg: mean ± SD; median; IQ range] | 85 ± 3; 85 (83, 87) | 85 ± 3; 85 (83, 87) |
| Risk SCORE | ||
| [%: mean ± SD; median; IQ range] | 2.1 ± 3.0; 0.9 (0.3, 2.9) | 2.0 ± 2.9; 0.9 (0.3, 2.5) |
| Low-Risk: <1% [n; %] | 117 (56.5%) | 145 (51.8%) |
| Moderate-Risk: ≥1% and <5% [n; %] | 64 (30.9%) | 106 (37.9%) |
| High-Risk: ≥5% and <10% [n; %] | 22 (10.6%) | 23 (8.2%) |
| Very-High-Risk: ≥10% [n; %] | 4 (1.9%) | 6 (2.1%) |
| Smoking habits | ||
| [Never + Past/Current: n; %] | 155 (74.9%)/52 (25.1%) | 218 (77.9%)/62 (22.1%) |
| Alcohol intake | ||
| [No + Moderate/Excessive: n; %] | 134 (65.0%)/72 (35.0%) | 208 (74.8%)/70 (25.2%) |
| TC | HDL-C | LDL-C | TG | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline (Median, IQR) | Follow-Up (Median, IQR) | Variation † (Median, IQR, %, p-Value) | Baseline (Median, IQR) | Follow-Up (Median, IQR) | Variation † (Median, IQR, %, p-Value) | Baseline (Median, IQR) | Follow-Up (Median, IQR) | Variation † (Median, IQR, %, p-Value) | Baseline (Median, IQR) | Follow-Up (Median, IQR) | Variation † (Median, IQR, %, p-Value) | |
| All patients (n:207) | 259 (241, 285) | 237 (205, 260) | −19 (−46, −6) −7,7%, p < 0.001 | 54 (42, 66) | 53 (42, 66) | 0 (−6, 5) 0.0%, NS | 176 (154, 194) | 155 (125, 177) | −18 (−40, −1) −10.1%, p < 0.001 | 142 (96, 232) | 120 (82, 173) | −20 (−68, 7) −16,7%, p < 0.001 |
| Sex * | ||||||||||||
| F (n: 117, 56.5%) | 264 (250, 287) | 241 (216, 261) | −22 (−54, −10) −8.4%, p < 0.001 | 61 (50, 73) | 62 (48, 73) | 1 (−6, 5) 0.7%, NS | 178 (159, 192) | 157 (128, 176) | −20 (−45, −7) −11.4%, p < 0.001 | 110 (87, 168) | 100 (76, 163) | −13 (−44, 9) −12.2%, p < 0.001 |
| M (n: 90, 43.5%) | 250 (222, 275) | 224 (203, 256) | −15 (−39, 2) −6.6%, p < 0.001 | 47 (37, 56) | 45 (39, 54) | 0 (−6, 5) 0.0%, NS | 169 (137, 196) | 153 (122, 178) | −8 (−30, 8) −5.6%, p = 0.001 | 197 (130, 315) | 136 (105, 189) | −45 (−150, −2) −27.2%, p < 0.001 |
| Age * | ||||||||||||
| <45 years (n: 78, 129%) | 256 (222, 284) | 228 (200, 256) | −20 (−45, −4) −7.7%, p < 0.001 | 53 (41, 63) | 52 (41, 63) | 0 (−7, 5) 0.0%, NS | 170 (152, 192) | 151 (117, 174) | −17 (−41, 3) −9.9%, p < 0.001 | 154 (101, 229) | 124 (80, 172) | −20 (−73, 8) −14.9%, p < 0.001 |
| ≥45 years (n: 129, 62.3%) | 261 (246, 287) | 240 (212, 261) | −19 (−49, −8) −7.7%, p < 0.001 | 54 (43, 67) | 55 (45, 70) | 1 (−6, 5) 1.6%, NS | 177 (158, 196) | 158 (130, 178) | −18 (−40, −4) −10.1%, p < 0.001 | 136 (96, 235) | 120 (82, 174) | −21 (−67, 2) −18.2%, p < 0.001 |
| BMI | ||||||||||||
| <25 kg/m2 (n: 110, 53.1%) | 257 (242, 281) | 236 (205, 256) | −20 (−49, −6) −7.5%, p < 0.001 | 59 (49, 70) | 59 (47, 68) | 0 (−7, 5) 0.0%, NS | 174 (155, 190) | 152 (122, 175) | −19 (−40, −3) −11.1%, p < 0.001 | 117 (82, 180) | 101 (77, 154) | −11 (−47, 11) −11.1%, p < 0.001 |
| ≥25 kg/m2 (n: 97, 46.9%) | 261 (238, 288) | 239 (206, 263) | −17 (−45, −6) −8.1%, p < 0.001 | 48 (40, 60) | 47 (40, 63) | 1 (−5, 6) 2.2%, NS | 179 (154, 198) | 158 (130, 179) | −16 (−40, 1) −9.1%, p < 0.001 | 196 (120, 315) | 137 (99, 209) | −40 (−121, −7) −23.5%, p < 0.001 |
| Smoking habits * | ||||||||||||
| Never/Past (n: 155, 74.9%) | 262 (241, 287) | 240 (205, 261) | −19 (−44, −6) −7.5%, p < 0.001 | 54 (44, 66) | 54 (42, 67) | 0 (−6, 5) 0.0%, NS | 177 (155, 197) | 156 (127, 179) | −17 (−38, −1) −9.9%, p < 0.001 | 138 (94, 228) | 119 (81, 168) | −18 (−63, 8) −14.5%, p < 0.001 |
| Current (n: 52, 25.1%) | 257 (237, 277) | 227 (206, 251) | −19 (−52, −7) −8.2%, p < 0.001 | 53 (40, 65) | 52 (44, 64) | 2 (−6, 10) 4.7%, NS | 171 (152, 187) | 153 (121, 172) | −18 (−45, 1) −11.0%, p < 0.001 | 161 (102, 320) | 123 (88, 185) | −37 (−147, −2) −26.3%, p < 0.001 |
| Alcohol consumption * | ||||||||||||
| Absent/moderate (135, 64.3%) | 262 (237, 288) | 234 (205, 260) | −22 (−53, −6) −8.4%, p < 0.001 | 53 (41, 66) | 54 (42, 67) | 1 (−4, 6) 2.6%, NS | 179 (155, 194) | 154 (121, 176) | −20 (−45, −2) −11.4%, p < 0.001 | 143 (96, 235) | 115 (81, 168) | −20 (−68, 8) −16.2%, p < 0.001 |
| Elevate (72, 35.7%) | 257 (242, 278) | 237 (208, 262) | −16 (−40, −4) −6.0%, p < 0.001 | 54 (46, 65) | 52 (43, 64) | −1 (−7, 4) −2.1%, NS | 170 (152, 194) | 157 (133, 178) | −16 (−29, 8) −8.4%, p = 0.01 | 134 (96, 229) | 132 (82, 177) | −19 (−67, 6) −18.2%, p < 0.001 |
| MonK (n. 29) | MonK + BBR (n. 167) | PUFA-W3 (n. 36) | Bonferoni adj. p-Value † (Unadjusted) | |
|---|---|---|---|---|
| TC (mg/dL) | −30 (−48; −20), | −46 (−66; −23), | −15 (−37; 5), | MonK vs. PUFA-W3: 0.086 (0.014) MonK + BBR vs. Diet: <0.0001 (<0.001) MonK + BBR vs. PUFA-W3: <0.0001 (<0.0001) |
| (median, IQR, %) | −11,3% | −17,4% | −6% | |
| Dif. from diet alone | ||||
| (median, %) | −11, −3,6% | −27, −9,7% | 4, 1,7% | |
| HDL-C (mg/dL) | −1 (−6; 1), | 0 (−7; 5), | 3 (−1; 7), | NS |
| (median, IQR, %) | −2,2% | 0% | 5,3% | |
| Dif. from diet alone | ||||
| (median, %) | −1, −2,2% | 0, 0% | 3, 5,3% | |
| LDL-C (mg/dL) | −23 (−41; −14), | −42 (−62; −20), | −11 (−40; 9), | MonK vs. Diet: 0.294 (0.049) MonK + BBR vs. Diet: <0.0001 (<0.001) MonK + BBR vs. PUFA-W3: <0.0001 (<0.0001) MonK vs. PUFA-W3: 0.253 (0.042) |
| (median, IQR, %) | −14,7% | −23,4% | −7,2% | |
| Dif. from diet alone | ||||
| (median, %) | −5, −4,6% | −24, −13,3% | 7, 2,9% | |
| TG (mg/dL) | −12 (−39; 1), | −11 (−43; 16), | −66 (−148; −18), | PUFA-W3 vs. Diet: 0.049 (0.008) MonK vs. PUFA-W3: 0.058 (0.010) MonK + BBR vs. PUFA-W3: <0.0001 (<0.0001) MonK + BBR vs. Diet: 0.027 (0.004) |
| (median, IQR, %) | −14,1% | −9,4% | −22,6% | |
| Dif. from diet alone | ||||
| (median, %) | 8, 2,6% | 9, 7,3% | −46, −5,9% |
| ASCVD Risk | Low (<1%) | Moderate (≥1%; <5%) | High (≥5%; <10%) | Very High (≥10%) | |
|---|---|---|---|---|---|
| 2016 ESC/EAS LDL-C targets | <115 mg/dL | <115 mg/dL | <100 mg/dL | <70 mg/dL | |
| Baseline | |||||
| Reaching 2016 ESC/EAS Guidelines | n (%) | 8 (3.1%) | 7 (4.1%) | 0 (0%) | 0 (0%) |
| F/M | 3/5 | 3/4 | NA | NA | |
| Age (years) | 40 (33–45) | 64 (57–68) | NA | NA | |
| Not reaching 2016 ESC/EAS Guidelines | n (%) | 254 (96.9%) | 163 (95.9%) | 45 (100%) | 10 (100%) |
| F/M | 150/104 | 104/59 | 22/23 | 4/6 | |
| Age (years) | 43 (36–50) | 59 (55–65) | 68 (64–74) | 74 (73–77) | |
| Follow-up | |||||
| Reaching 2016 ESC/EAS Guidelines | n (%) | 40 (15.3%) | 23 (13.5%) | 3 (6.7%) | 0 (0%) |
| F/M | 23/17 | 16/7 | 2/1 | NA | |
| Age (years) | 41 (33–49) | 61 (58–65) | 74 (69–77) | NA | |
| Not reaching 2016 ESC/EAS Guidelines | n (%) | 222 (84.7%) | 147 (86.5%) | 42 (93.3%) | 10 (100%) |
| F/M | 130 (58.6%) | 91 (61.9%) | 20 (46.5%) | 4 (40.0%) | |
| Age (years) | 43 (36–50) | 59 (55–65) | 68 (64–73) | 74 (73–77) | |
| 2019 ESC/EAS LDL-C targets | <116 mg/dL | <100 mg/dL | <70 mg/dL | <55 mg/dL | |
| Baseline † | |||||
| Reaching 2019 ESC/EAS Guidelines | n (%) | 8 (3.1%) | 1 (0.6%) | 0 (0%) | 0 (0%) |
| F/M | 3/5 | 1/0 | NA | NA | |
| Age (years) | 40 (33–45) | 70 | NA | NA | |
| Not reaching 2019 ESC/EAS Guidelines | n (%) | 254 (96.9%) | 169 (99.4%) | 45 (100%) | 10 (100%) |
| F/M | 150/104 | 106/63 | 22/23 | 4/6 | |
| Age (years) | 43 (36–50) | 59 (55–65) | 68 (64–74) | 74 (73–77) | |
| Follow-up | |||||
| Reaching 2019 ESC/EAS Guidelines | n (%) | 40 (15.3%) | 11 (6.5%) | 0 (0%) | 0 (0%) |
| F/M | 23/17 | 9/2 | NA | NA | |
| Age (years) | 41 (33–49) | 62 (58–65) | NA | NA | |
| Not reaching 2019 ESC/EAS Guidelines | n (%) | 222 (84.7%) | 159 (93.5%) | 45 (100%) | 10 (100%) |
| F/M | 130/92 | 98/61 | 22/23 | 4/6 | |
| Age (years) | 43 (36–50) | 59 (55–65) | 68 (64–74) | 74 (73–77) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pasta, A.; Formisano, E.; Cremonini, A.L.; Maganza, E.; Parodi, E.; Piras, S.; Pisciotta, L. Diet and Nutraceutical Supplementation in Dyslipidemic Patients: First Results of an Italian Single Center Real-World Retrospective Analysis. Nutrients 2020, 12, 2056. https://doi.org/10.3390/nu12072056
Pasta A, Formisano E, Cremonini AL, Maganza E, Parodi E, Piras S, Pisciotta L. Diet and Nutraceutical Supplementation in Dyslipidemic Patients: First Results of an Italian Single Center Real-World Retrospective Analysis. Nutrients. 2020; 12(7):2056. https://doi.org/10.3390/nu12072056
Chicago/Turabian StylePasta, Andrea, Elena Formisano, Anna Laura Cremonini, Elio Maganza, Erika Parodi, Sabrina Piras, and Livia Pisciotta. 2020. "Diet and Nutraceutical Supplementation in Dyslipidemic Patients: First Results of an Italian Single Center Real-World Retrospective Analysis" Nutrients 12, no. 7: 2056. https://doi.org/10.3390/nu12072056
APA StylePasta, A., Formisano, E., Cremonini, A. L., Maganza, E., Parodi, E., Piras, S., & Pisciotta, L. (2020). Diet and Nutraceutical Supplementation in Dyslipidemic Patients: First Results of an Italian Single Center Real-World Retrospective Analysis. Nutrients, 12(7), 2056. https://doi.org/10.3390/nu12072056