1. Introduction
Adolescence constitutes a period of increased nutritional needs, required to support the physical growth that accompanies puberty [
1,
2]. Healthy eating is of vital importance during adolescence [
3,
4], in order to ensure the sufficient macronutrient and micronutrient intake needed for proper physical development [
1], cognitive performance [
5,
6,
7] and good mental health [
8]. Dietary habits during the adolescent years directly influence body weight regulation and play a major role in the healthy development that comes with adolescence [
9]. Adherence to “unhealthy” eating habits during this period increases the risk of obesity development [
10,
11], which has, in turn, been long associated with an increased risk of non-communicable disease manifestation, such as type 2 diabetes, both in adolescence and later on in adult life [
9,
10]. Indeed, the presence of adolescent obesity has been associated with severe obesity in late adulthood [
12,
13] and a greater risk for type 2 diabetes development in early adulthood [
13]. In addition, higher Body Mass Index (BMI) values during adolescence have been associated with higher BMI values during adulthood, as well as a 30 to 40% increased risk in adult mortality [
14].
The causes of overweight, obesity and non-communicable disease development in adolescent populations are related to the consumption of energy-dense foods, reduction of physical activity, as well as socioeconomic factors, such as food availability and food preference, influenced by geographic factors [
9,
11]. Energy-dense foods have been related both directly and indirectly, via their positive association, with overweight and obesity development, in the development of non-communicable diseases [
11]. Indeed, poor eating habits have regularly been associated with a high consumption of foods with high fat and/or sugar contents [
9].
Adolescent dietary habits are also directly linked to the teenagers’ metabolic profile and the interplay between biomarkers of glycemic and lipidemic control [
15]. It has been shown that adherence to an “unhealthy” dietary pattern is associated with a higher risk for metabolic syndrome presence [
15]. Their importance is further highlighted by the increased incidence of type 2 diabetes in young children and teenagers [
16]. Consumption of energy-dense foods in children and teenagers with a family history of type 2 diabetes, plays a central role in the formation of a worse glycemic profile and potentially, subsequent development of type 2 diabetes (T2D) [
16]. T2D in children is associated with a deteriorated lipidemic profile (i.e., dyslipidemia), as a direct effect of the observed insulin resistance [
17]. A different study showed that Greek children with dyslipidemia and unfavourable dietary habits, such as consuming only one meal per day, displayed higher levels of various biomarkers of lipidemic control, namely total cholesterol and low-density lipoprotein cholesterol (LDL-C) [
18].
Another cardiometabolic risk factor receiving more and more attention is the development of hypertension and the elevated levels of arterial pressure in adolescents. Indeed, high blood pressure can be met in teenagers, with boys reporting higher levels of blood pressure than girls [
19].
The present analyses constitute the first step in the context of the 2018 Gutenberg Chair project, aimed at firstly investigating the role of dietary habits in the anthropometric and biochemical profile of two adolescent, European populations and subsequently exploring the potential role of nutrition as a modifier of genetic make-up in adolescence. The latter will take place via an investigation into the relationship between the populations’ dietary habits and their glycemic and lipidemic profile and inflammation markers with genetic risk scores created for anthropometric indices, biomarkers of glycemic and lipidemic control and inflammation markers.
In this context, the aim of the present study is to investigate the dietary habits of the two populations from the Greek TEENAGE Study and the French STANISLAS Family study and their potential associations with blood pressure, biomarkers of glycemic and lipidemic control and levels of C-reactive protein (CRP). Therefore, the objectives of the study are formed as follows: (a) to identify the dietary patterns of adolescents in the Greek and French cohorts; and (b) to investigate potential, respective associations between said patterns and blood pressure, anthropometric indices, biomarkers of glycemic and lipidemic control and CRP levels.
4. Discussion
The present study sought to investigate the dietary patterns of two adolescent, European populations, based on data from the Greek TEENAGE and the French STANISLAS Family studies, as well as their potential relations with blood pressure, biomarkers of glycemic and lipidemic control and levels of CRP. The study includes healthy teenagers from the two European populations, with a median BMI of 20.88 kg/m
2 (IQR = 5.88 kg/m
2) and 18.44 kg/m
2 (IQR = 3.61 kg/m
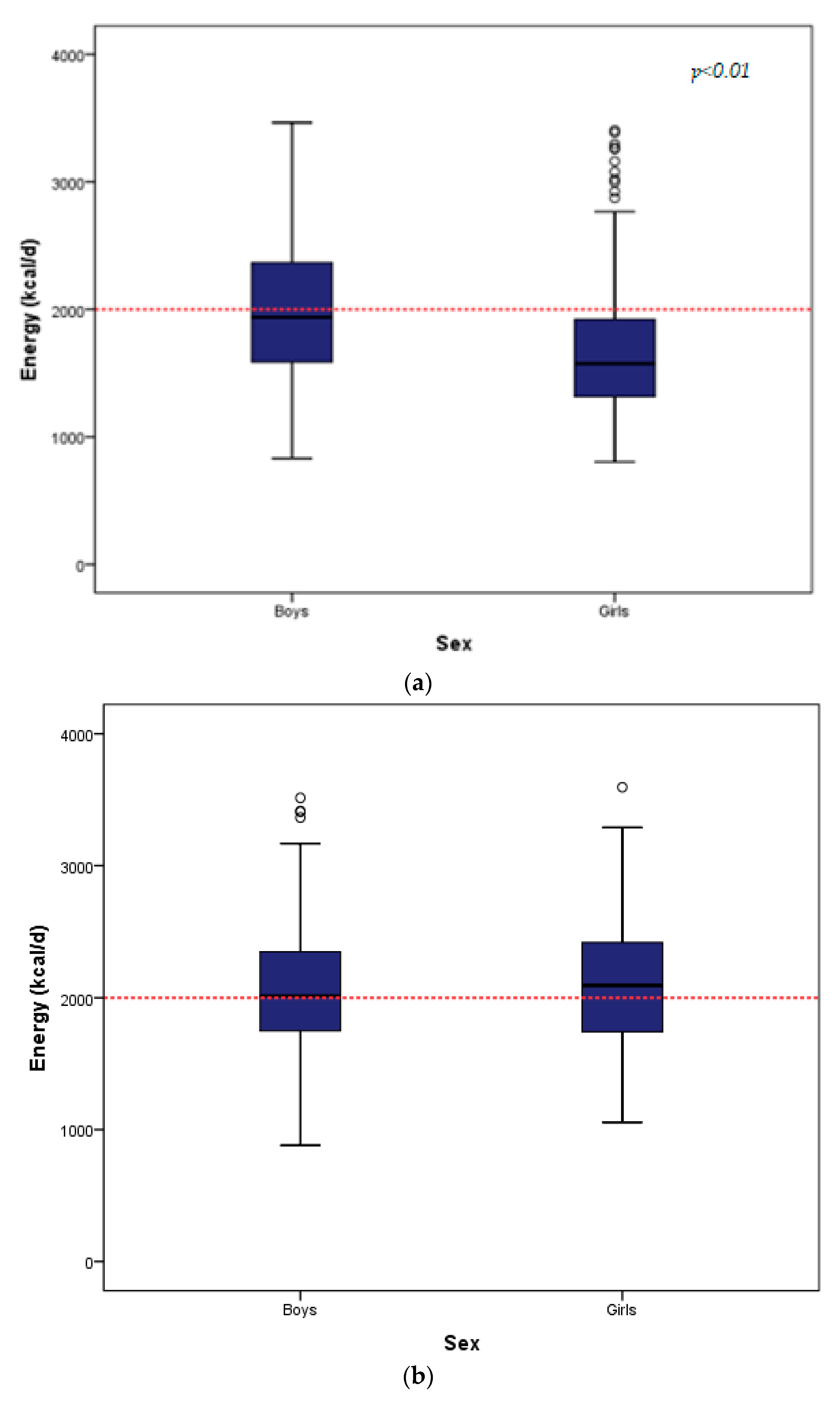
2). For the Greek teenagers, weight, waist-to-hip ratio (WHR), systolic blood pressure (SBP), levels for glucose, HOMA-IR, insulin, HDL-C and CRP significantly differed between boys and girls. Boys presented slightly higher values for weight, WHR, SP and glucose levels, while girls reported slightly higher levels of HOMA-IR, insulin and HDL-C. In the French teenagers group, WHR, SBP, glucose and total cholesterol levels presented statistically significant differences between the two sexes, with boys reporting slightly higher values for WHR, SBP and glucose levels and girls for total cholesterol levels. The teenagers of the study were mostly normal weighted. Both populations reported a mediocre energy intake (TEENAGE: 1741.00 kcal/d and STANISLAS: 2056.03 kcal/d), based on the present dietary guidelines for adolescents [
39]. This could explain the fact that teenagers of both populations mostly reported BMI values within the normal range (18.5–25 kg/m
2).
Five dietary patterns were identified in each population. The Greek “eggs and fibers” and the French “prudent snacking” patterns, explaining 7.47% and 10.44% of the respective total variance, included consumption of Mediterranean diet-related food groups, such as non-refined cereals, vegetables and eggs in the Greek teenagers and consumption of eggs and vegetable fats in French adolescents. The Greek teenagers showed a preference for healthy and traditional food combinations, such as consumption of legumes, olives, olive oil and nuts in the “legumes and good fat” pattern and consumption of red meat and potatoes in the “homemade meal” pattern, respectively. The French teenagers opted for consumption of more energy-dense food groups, such as red meat, animal fat and milk and yogurt in the “high protein and animal fat” pattern and soft drinks and sugary snacks in the “sugary snacks” pattern. A number of significant associations were found between the respective dietary patterns and the populations’ glycemic and lipidemic profile. However, after adjusting for the overall adjusted threshold, a smaller number of significant associations remained observed.
The predominant pattern in both populations (the “western breakfast” pattern) appears to relate to food groups whose consumption is primarily found in the basis of a western-type diet [
40], such as cheese, processed meat and food items high in carbohydrates (breads and flours for the French). The “western breakfast” pattern reflects a higher percentage (15.61%) of the variance explained in the Greek population, in comparison to the French one (10.58%). This could be explained by the increasing influences of the westernized world trends in the Greek socio-economic scene during the late 2000s. Moreover, breakfast habits were also highlighted in the first 5-year follow-up in the STANISLAS Cohort, which underlined the importance of the household environment in dietary habits by finding a household variance of 42.5 to 52.9% in the energy intake observed in breakfast [
29]. The importance of breakfast consumption and its contribution to daily energy intake of French children and families, is also supported by another, recent cross-sectional survey [
41].
Although the western diet has been associated with elevated inflammation biomarkers [
42], the cohort of the Greek teenagers reported no comorbidities and we found no associations between adherence to the “western breakfast” pattern and respective CRP levels. Interestingly enough, the “chicken and sugars” pattern identified in the Greek cohort was significantly associated with lower levels of logCRP (Model 1: β = −0.051,
p-value = 0.006, Model 2: β = −0.057,
p-value = 0.004 and Model 3: β = −0.050,
p-value = 0.008). An inverse association between the consumption of poultry and CRP levels in teenagers has previously been reported, in the general context of adherence to the Dietary Approach to Stop Hypertension (DASH) diet regime [
43], although a recent umbrella review showed no association between the DASH diet and CRP levels in adults [
44]. On the contrary, an inverse association between consumption of sweets and CRP levels is not supported by other studies. In fact, consumption of sugars and especially sugar-sweetened beverages has previously been associated with higher CRP levels in adults [
45,
46]. In adolescents, a different review has shown a positive association between sugar consumption and CRP [
47], whereas another review found greater consumption of sugars by normal weight adolescents in comparison with overweight ones, but did not find any association between sugar consumption and CRP [
48]. Α cross-sectional study investigating the relation between food intake and CRP levels in children also found that consumption of milk, citrus, melons and berries displayed associations with lower levels of CRP, potentially due to the general high content of fruits and vegetables in antioxidants and the association of dairy consumption with greater satiety and potential adherence to a generally healthier diet [
49].
Furthermore, our study found that the “high protein and animal fat” pattern displayed significant associations with higher logtriglyceride and logBMI levels (
p < 0.01), for French teenagers. The latter is in accordance with various cross-sectional studies that have researched the dietary habits of adolescents and their potential associations to BMI. A study by Gutiérrez-Pliego et al. unveiled three major dietary patterns in a population of 373 Mexican teenagers including a pattern high in refined “unhealthy” products, such as snacks, sugars and sweets, a pattern with high protein/high fat content and a pattern including high consumption of fruits, vegetables, nuts and whole grains. The study found a strong relationship (
p < 0.01) between higher consumptions of the first two dietary patterns and higher BMI [
50]. In the same context, a different study in Northeastern Brazil investigated data from 1247 adolescents. The study identified two dietary patterns, one referring to high consumption of sugars, sweets and cakes, amongst others, and one correlated with high consumption of fruits and vegetables. Higher adherence to the dietary pattern including “unhealthy” products, was, again, positively correlated with higher values of BMI (
p = 0.018) [
51]. Furthermore, a different study on the dietary habits of female adolescents showed that higher adherence to a “Western” pattern referring to increased consumption of fat and mediocre consumption of protein, among others, was associated with higher levels of BMI, waist circumference, as well as total cholesterol levels [
52].
Although dietary patterns with a higher consumption of fat have generally been positively associated with cardiometabolic risk factors in teenagers [
53,
54], certain diets, including consumption of specific food groups, such as the DASH diet [
55], have been related with a better metabolic profile [
56]. Indeed, higher adherence to the DASH diet has been shown to relate to a reduced prevalence of metabolic syndrome and increased blood pressure during adolescence [
43], as well as lower levels of HbA1c and systolic blood pressure, in young adults with type 1 and type 2 diabetes, respectively [
57]. Better adherence to the components of the DASH diet was even associated with a lower risk of being a metabolic unhealthy obese, in children and adolescents with increased body weight [
58]. Additionally, other high protein diets, such as the ketogenic diet and the Modified Atkins diet, have been associated with better effects on adolescents with epilepsy [
59,
60], with the ketogenic diet to have been related to reduced weight and fasting insulin and HOMA-IR levels in obese teenagers [
61]. However, the aforementioned diets also usually include consumption of vegetables fats and fats derived from nuts, seeds, white meat (such as poultry and fish), as well as food groups like grains, vegetable fats, fruits and vegetables, which are not met when referring to dietary patterns centred on high protein or animal fat consumption. Furthermore, the aforementioned beneficial associations have been primarily observed in adults or obese adolescent populations, who could potentially benefit from the adherence to a structured diet with the above food groups. This could potentially explain why our study demonstrated positive associations between the high consumption of protein and animal fats with BMI and triglyceride levels in adolescents mostly displaying BMI of a normal range. Moreover, the present study evaluates the adherence to each dietary pattern, without comparing them with the respective adherence to the rest of the patterns extracted.
The identification of dietary patterns of adolescents has generally been a subject of interest in recent literature. Gonzalez-Gil et al. investigated the dietary patterns of 5328 European adolescents in the context of the cross-sectional HELENA study [
62]. The latter consisted of adolescent cohorts of 10 different European countries, including Greek teenagers from the cities of Athens and Heraklion, Crete. The study identified four dietary patterns in teenage boys and six dietary patterns in teenage girls. Patterns explaining greater total variance in boys referred to consumption of vegetables, pasta, rice, cheese and sweets among others, at the same time as dominant patterns in girls referred to consumption of Mediterranean-type food items, dairy and consumption of a healthy breakfast [
62].
Additionally, when investigating the dietary habits of adolescents based on data collected in the 1995 Australian National Nutrition Survey, McNaughton et al. showed that a dietary pattern rich in fruit, salads, cereals and fish was found to be negatively associated with levels of diastolic blood pressure in teenagers older than 16 years of age [
63]. Our study found no associations between the patterns containing fruit, vegetable and fish consumption and the levels of diastolic pressure in adolescents younger than 16 years of age.
Furthermore, the I. Family Study investigated the association between the dietary patterns of 2451 pairs of European children and their parents, with regards to the existing food environment conditions. The study showed the role of food availability in the children’s dietary choices, highlighting that the consumption of soft drinks was greatly dependent on their availability in the immediate food environment [
64]. Moreno LA et al. also showed that increased consumption of sweet beverages was also associated with increased risk of adolescent obesity [
65]. In our study, the “sugary snacks” pattern of the French population, which included consumption of sweetened beverages, was not related to logBMI values, but was associated with lower values of logHDL-C. However the effect disappeared when taking into account the adjusted threshold of statistical significance (0.04 > 0.01). A different study of German adolescents demonstrated that higher consumption of dietary patterns containing high-fat and high-carbohydrate, energy-dense foods was associated with lower socioeconomic levels and a lower intake of various vitamins and minerals [
66].
A previous publication on the Greek adolescents of the TEENAGE study investigated a spectrum of factors potentially contributing to the development of overweight, leading to the creation of an Overweight Preventive Score, which included breakfast intake, family meals and consumption of sugar-sweetened beverages, among other factors, and further supports the aforementioned findings. The score was found to be significantly associated with a lower likelihood of overweight presence and better levels of glycemic control [
67].
The limitations of the present study are summarized in the following: (a) data for both populations were collected in a cross-sectional manner, limiting the potential for generalized cause and effect conclusions to be drawn; (b) use of the PCA for the dietary patterns’ extraction, including subjective choices regarding the amount of food groups that are included in the analysis, as well as the number of components to be drawn; (c) comparisons between the two populations’ dietary habits might be affected by the different socio-economic conditions existing in the two countries during the mid-1990s for the STANISLAS and late 2000s for the TEENAGE study. This prolonged gap between the two baseline data collections might manifest itself in the Greek teenagers’ dietary habits, which could have potentially been affected by social changes and changes in food availability and accessibility, mediated by the growing social and technological advancements taking place throughout the 15-year gap.

 ,
, 

{kind=link}