
DASH Diet as a Proposal for Improvement in Cellular Immunity and Its Association with Metabolic Parameters in Persons with Overweight and Obesity

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility Criteria
2.3. Clinical Measurements
2.3.1. Anthropometric
2.3.2. Body Composition
2.3.3. Biochemical Tests and Determination of Metabolic Syndrome
2.3.4. Leukocyte Measurement
2.4. Intervention
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Laboratory Analysis, Anthropometric Parameters, and Body Composition
3.3. Leukocytes Subpopulation
3.4. Implementation of a Dietary Plan for Metabolic and Immunological Improvement
3.5. Leukocyte Subpopulations after Intervention
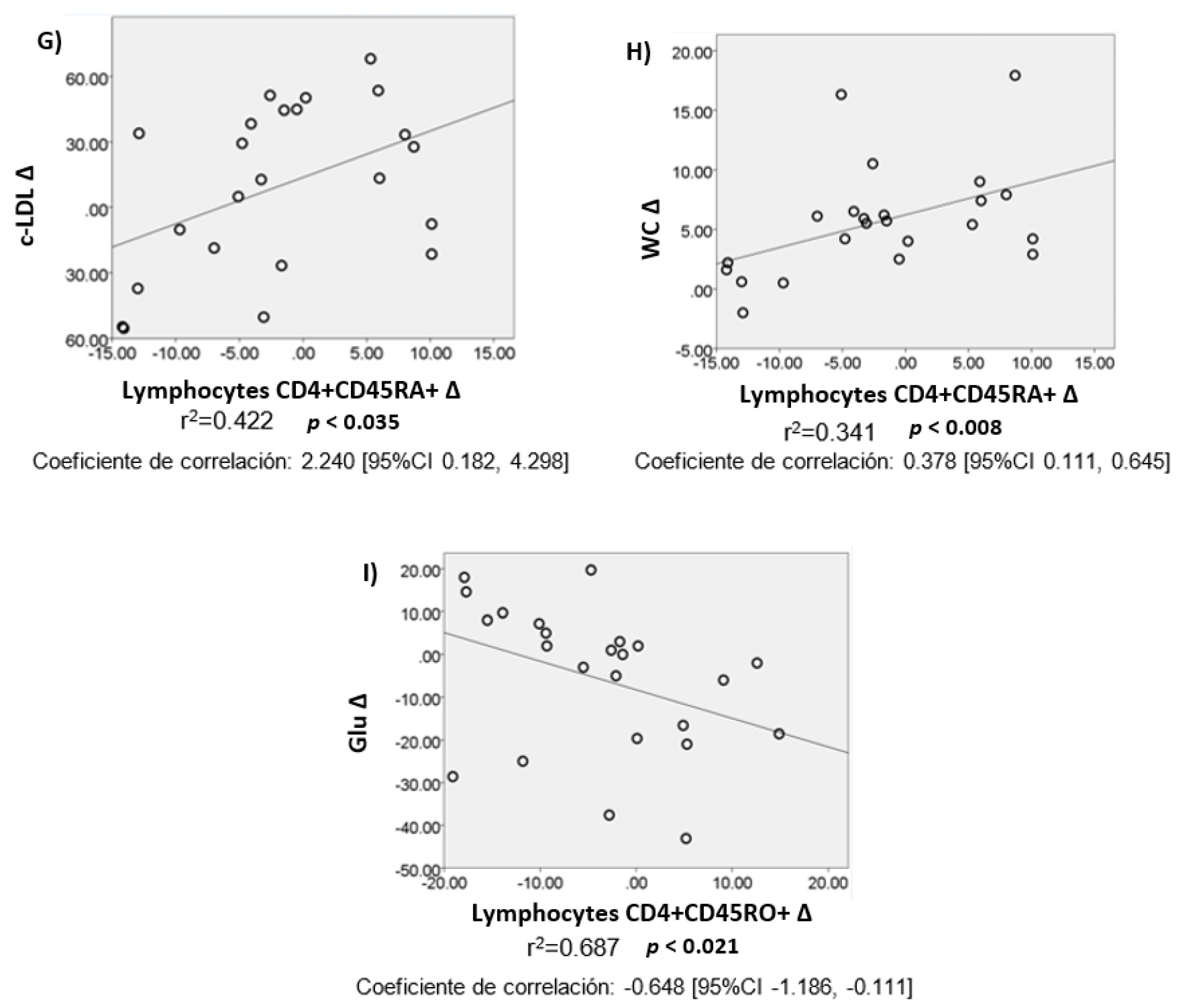
3.6. Partial Correlations and Linear Regressions after Intervention
4. Discussion
5. Conclusions
Author Contributions
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Roumans, N.J.; Vink, R.G.; Fazelzadeh, P.; van Baak, M.A.; Mariman, E.C. A role for leukocyte integrins and extracellular matrix remolding of adipose tissue in the risk or weight regain after weight loss. Am. J. Clin. Nutr. 2017, 105, 1054–1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zatterale, F.; Longo, M.; Naderi, J.; Raciti, G.A.; Desiderio, A.; Miele, C.; Beguinot, F. Chronic adipose tissue inflammation linking obesity to insulin resistance and type 2 diabetes. Front. Physiol. 2020, 10, 1607. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.K.; Gutierrez, D.A.; Kennedy, A.; Hasty, A.H. Weight cycling increases T-cell Accumulation in adipose tissue and impairs systemic glucose tolerance. Diabetes 2013, 62, 3180–3188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esser, N.; Legrand-Poels, S.; Piette, J.; Scheen, A.J.; Paquot, N. Inflammation as a link between obesity, metabolic syndrome and type 2 diabetes. Diabetes Res. Clin. Pr. 2014, 105, 141–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryder, E.; Diez-Ewald, M.; Mosquera, J.; Fernández, E.; Pedreanez, A.; Vargas, R.; Peña, C.; Fernández, N. Association of obesity with leukocyte count in obese individuals without metabolic syndrome. Diabetes Metab. Syndr. Clin. Res. Rev. 2014, 8, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Donninelli, G.; del Cornò, M.; Pierdominici, M.; Scazzocchio, B.; Varì, R.; Varano, B.; Pacella, I.; Piconese, S.; Barnaba, V.; D’Archivio, M.; et al. Distinct blood and visceral adipose tissue regulatory T cell and innate lymphocyte profiles characterize obesity and colorectal cancer. Front. Immunol. 2017, 8, 643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, R.; Nikolajczyk, B.S. Tissue inmmune cells fuel obesity-associated inflammation in adipose tissue and beyond. Front. Immunol. 2019, 10, 1587. [Google Scholar] [CrossRef] [Green Version]
- Manzur, F.; Alvear, C.; Alayón, A.N. Adipocytes, visceral obesity, inflammation and cardiovascular disease. Rev. Colomb. Cardiol. 2010, 17, 207–213. [Google Scholar]
- Coelho, M.; Oliveira, T.; Fernandes, R. Biochemistry of adipose tissue: An endocrine organ. Arch. Med. Sci. 2013, 9, 191–200. [Google Scholar] [CrossRef] [Green Version]
- Marette, A.; Liu, Y.; Sweeney, G. Skeletal muscle glucose metabolism and inflammation in the development of the metabolic syndrome. Rev. Endocr. Metab. Disord. 2014, 15, 299–305. [Google Scholar] [CrossRef]
- Muhammad, H.F.L.; Vink, R.G.; Roumans, N.J.T.; Arkenbosch, L.A.J.; Mariman, E.C.; Van Baak, M.A. Dietary intake after weight loss and the risk of weight regain: Macronutrient composition and inflammatory properties of the diet. Nutrients 2017, 9, 1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steck, S.; Shivappa, N.; Tabung, F.K.; Harmon, B.E.; Wirth, M.D.; Hurley, T.G.; Hebert, J.R. The dietary inflammatory index: A new tool for assessing diet quality based on inflammatory potential. Digest 2014, 49, 1–9. [Google Scholar]
- Shivappa, N.; Hébert, J.R.; Rietzschel, E.R.; De Buyzere, M.L.; Langlois, M.; Debruyne, E.; Marcos, A.; Huybrechts, I. Associations between dietary inflammatory index and inflammatory markers in the Asklepios study. Br. J. Nutr. 2015, 113, 665–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wirth, M.D.; Hébert, J.R.; Shivappa, N.; Hand, G.A.; Hurley, T.G.; Drenowatz, C.; McMahon, D.; Shook, R.P.; Blair, S.N. Anti-inflammatory dietary inflammatory index scores are associated with healthier scores on other dietary indices. Nutr. Res. 2016, 36, 214–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2013, 17, 1689–1696. [Google Scholar] [CrossRef] [Green Version]
- Sociedad Argentina de Hipertensión Arterial (Arterial Hypertension Argentine Society). (SAHA). Dieta DASH. 2010. Available online: http://www.saha.org.ar/dieta-dash.php (accessed on 5 June 2021).
- Ahluwalia, N.; Andreeva, V.; Kesse-Guyot, E.; Hercberg, S. Dietary patterns, inflammation and the metabolic syndrome. Diabetes Metab. 2013, 39, 99–110. [Google Scholar] [CrossRef]
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M.; et al. A clinical trial of the effects of dietary patterns on blood pressure. N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef] [Green Version]
- Azadbakht, L.; Surkan, P.J.; Esmaillzadeh, A.; Willett, W.C. The dietary approaches to stop hypertension eating plan affects c-reactive protein, coagulation abnormalities, and hepatic function tests among type 2 diabetic patients. J. Nutr. 2011, 141, 1083–1088. [Google Scholar] [CrossRef]
- Fitzgerald, K.C.; Chiuve, S.; Buring, J.E.; Ridker, P.M.; Glynn, R.J. Comparison of associations of adherence to a dietary approaches to stop hypertension (DASH)-style diet with risks of cardiovascular disease and venous thromboembolism. J. Thromb. Haemost. 2011, 10, 189–198. [Google Scholar] [CrossRef]
- Valentino, G.; Tagle, R.; Acevedo, M. DASH diet and menopause: Beyond the benefits on control of blood pressure. Rev. Chil. Cardiol. 2014, 33, 215–222. [Google Scholar] [CrossRef]
- Medina-Remón, A.; Kirwan, R.; Lamuela-Raventós, R.M.; Estruch, R. Dietary patterns and the risk of obesity, type 2 diabetes mellitus, cardiovascular diseases, asthma, and neurodegenerative diseases. Crit. Rev. Food Sci. Nutr. 2016, 58, 262–296. [Google Scholar] [CrossRef]
- Hill, A.M.; Harris Jackson, K.A.; Roussell, M.A.; West, S.G.; Kris-Etherton, P.M. Type and amount of dietary protein in the treatment of metabolic syndrome: A randomized controlled trial. Am. J. Clin. Nutr. 2015, 102, 757–770. [Google Scholar] [CrossRef] [Green Version]
- Kawamura, A.; Kajiya, K.; Kishi, H.; Inagaki, J.; Mitarai, M.; Oda, H.; Umemoto, S.; Kobayashi, S. Effects of the DASH-JUMP dietary intervention in Japanese participants with high-normal blood pressure and stage 1 hypertension: An open-label single-arm trial. Hypertens. Res. 2016, 39, 777–785. [Google Scholar] [CrossRef] [Green Version]
- Soltani, S.; Shirani, F.; Chitsazi, M.J.; Salehi-Abargouei, A. The effect of dietary approaches to stop hypertension (DASH) diet on weight and body composition in adults: A systematic review and meta-analysis of randomized controlled clinical trials. Obes. Rev. 2016, 17, 442–454. [Google Scholar] [CrossRef]
- Marfell-Jones, M. International Society for the Advancement of Kyneanthropometry I. In International Standards for an-Thropometric Assessment; International Society for the Advancement of Kyneanthropometry: Glasgow, Scotland, 2006; pp. 73–88. [Google Scholar]
- Secretariat of Health of Mexico City. Overweight and Obesity. 2014. Available online: http://www.salud.df.gob.mx/ssdf/index.php?option=com_content&task=view&id=4034 (accessed on 7 April 2014).
- World Health Organization (WHO). 10 Datos Sobre la Obesidad (10 Facts about Obesity). 2015. Available online: www.who.int/features/factfiles/obesity/facts/es/ (accessed on 20 July 2015).
- Biospace Co., Ltd. InBody720: The Precision Body Composition Analyzer: User’s Manual; Biospace Co., Ltd.: Seoul, Korea, 1996–2005; pp. 135–784. [Google Scholar]
- NOM-030-SSA2-2009 NOM. Official Mexican Standard. For the Prevention, Detection, Diagnosis, Treatment and Control of Arterial Hypertension. Available online: http://dof.gob.mx/nota_detalle.php?codigo=5144642&fecha=31/05/2010 (accessed on 23 April 2021).
- Albornoz Lopez, R.; Perez Rodrigo, I. Nutrition and metabolic síndrome. Nutr. Clín. Diet. Hosp. 2012, 32, 92–97. [Google Scholar]
- Nájera-Medina, O.; Valencia-Chavarría, F.; Cortés-Bejar, C.; Palacios-Martínez, M.; Rodríguez-López, C.P.; González-Torres, M.C. Infected malnourished children displayed changes in early activation and lymphocyte subpopulations. Acta Paediatr. 2017, 106, 1499–1506. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, C.P.; Gonzalez, M.C.; Aguilar-Salinas, C.A.; Nájera-Medina, O. Peripheral lymphocytes, obesity, and metabolic syndrome in young adults: An immunometabolism study. Metab. Syndr. Relat. Disord. 2018, 16, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Levy, T.; Villalpando, S.; Rivera, J. Nutrition results of the Mexican National Health and Nutrition Survey. 2006. Available online: https://www.scielosp.org/article/spm/2009.v51suppl4/S492-S493/ (accessed on 4 October 2021).
- Hernández-Avila, M.; Romieu, I.; Parra, S.; Hernandez-Avila, J.E.; Madrigal, H.; Willett, W. Validity and reproducibility of a food frequency questionnaire to assess dietary intake of women living in Mexico City. Salud Pública México 1998, 40, 133–140. [Google Scholar] [CrossRef]
- Kathleen, L.; Escott-Stump, S. Krause Dietoterapia, 12th ed.; Elsevier España, S.L.U.: Barcelona, Spain, 2009. [Google Scholar]
- Pérez-Lizaur, A.B.; Palacios González, B.; Castro Becerra, A.L.; Flores-Galicia, I. Sistema Mexicano de Alimentos Equivalentes (Mexican Equivalent Food System); FNS: Monterrey, Mexico, 2014; 160p. [Google Scholar]
- Challa, H.J.; Ameer, M.A.; Uppaluri, K.R. DASH Diet to Stop Hypertension; StatPearls Publishing: Treasure Island, FL, USA, 2014. [Google Scholar]
- Asemi, Z.; Esmaillzadeh, A. DASH diet, insulin resistance, and serum hs-CRP in polycystic ovary syndrome: A randomized controlled clinical trial. Horm. Metab. Res. 2015, 47, 232–238. [Google Scholar] [CrossRef]
- Phillips, C.M.; Harrington, J.M.; Perry, I.J. Relationship between dietary quality, determined by DASH score, and cardiometabolic health biomarkers: A cross-sectional analysis in adults. Clin. Nutr. 2019, 38, 1620–1628. [Google Scholar] [CrossRef]
- Chiu, S.; Bergeron, N.; Williams, P.T.; Bray, G.A.; Sutherland, B.; Krauss, R.M. Comparison of the DASH (Dietary Approaches to Stop Hypetension) diet and higher-fat DASH diet on blood pressure and lipids and lipoproteins: A rendomized controlled trial. Am. J. Clin. Nutr. 2016, 103, 341–347. [Google Scholar] [CrossRef] [Green Version]
- Fung, T.T.; Chiuve, S.E.; McCullough, M.L.; Rexrode, K.M.; Logroscino, G.; Hu, F.B. Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch. Intern. Med. 2008, 168, 713–720. [Google Scholar] [CrossRef] [Green Version]
- Farhadnejad, H.; Darand, M.; Teymoori, F.; Asghari, G.; Mirmiran, P.; Azizi, F. The association of Dietary Approach to Stop Hypertension (DASH) diet with metabolic healthy and metabolic unhealthy obesity phenotypes. Sci. Rep. 2019, 9, 1869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azadi-Yazdi, M.; Karimi-Zarchi, M.; Salehi-Abargouei, A.; Fallahzadeh, H.; Nadjarzadeh, A. Effects of dietary approach to stop hypertension diet on androgens, antioxidant status and body composition in overweight and obese women with polycystic ovary syndrome: A randomised controlled trial. J. Hum. Nutr. Diet. 2016, 30, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Kucharska, A.; Gajewska, D.; Kiedrowski, M.; Sińska, B.; Juszczyk, G.P.; Czerw, A.; Augustynowicz, A.; Bobiński, K.; Deptała, A.; Niegowska, J. The impact of individualised nutritional therapy according to DASH diet on blood pressure, body mass, and selected biochemical parameters in overweight/obese patients with primary arterial hypertension: A prospective randomised study. Kardiol. Pol. 2018, 76, 158–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.; Lee, I.S.; Choue, R. Obesity, inflammation and diet. Pediatr. Gastroenterol. Hepatol. Nutr. 2013, 16, 143–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mauro, C.; Smith, J.; Cucchi, D.; Coe, D.; Fu, H.; Bonacina, F.; Baragetti, A.; Cermenati, G.; Caruso, D.; Mitro, N.; et al. Obesity-induced metabolic stress leads to biased effector memory CD4+ T cell differentiation via PI3K p110delta-Akt-mediated signals. Cell Metab. 2017, 25, 593–609. [Google Scholar] [CrossRef] [Green Version]
- Parisi, M.M.; Grun, L.K.; Lavandoski, P.; Alves, L.B.; Bristot, I.J.; Mattiello, R.; Mottin, C.C.; Klamt, F.; Jones, M.H.; Padoin, A.V.; et al. Immunosenescence induced by plasma from individuals with obesity caused cell signaling dysfunction and inflammation. Obesity 2017, 25, 1523–1531. [Google Scholar] [CrossRef] [Green Version]
- Kanneganti, T.D.; Dixit, V.D. Immunological complications of obesity. Nat. Immunol. 2012, 13, 707–712. [Google Scholar] [CrossRef]
- Mold, J.E.; Réu, P.; Olin, A.; Bernard, S.; Michaëlsson, J.; Rane, S.; Yates, A.; Khosravi, A.; Salehpour, M.; Possnert, G.; et al. Cell generation dynamics underlying naive T-cell homeostasis in adult humans. PLoS Biol. 2019, 17, e3000383. [Google Scholar] [CrossRef]
- Pandolfi, J.B.; Ferraro, A.A.; Sananez, I.; Gancedo, M.C.; Baz, P.; Billordo, L.A.; Fainboim, L.; Arruvito, L. ATP-induced inflammation drives tissue-resident Th17 cells in metabolically unhealthy obesity. J. Immunol. 2016, 196, 3287–3296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magrone, T.; Jirillo, E.; Spagnoletta, A.; Magrone, M.; Russo, M.A.; Fontana, S.; Laforgia, F.; Donvito, I.; Campanella, A.; Silvestris, F.; et al. Immune profile of obese people and in vitro effects of red grape polyphenols on peripheral blood mononuclear cells. Oxidative Med. Cell. Longev. 2017, 2017, 1–11. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria | Values | |
|---|---|---|
| Triglycerides | ≥150 mg/dL | |
| HDL-c | <40 mg/dL | |
| Blood pressure | ≥130/85 mmHg or previous diagnosis | |
| Fasting glucose | ≥100 mg/dL | |
| Waist circumference | Women | Men |
| ≥80 cm | ≥90 cm | |
| Variable (n = 59) | Normal (n = 29) | Overweight (n = 14) | Obesity (n = 16) | p (ANOVA) | |||||
|---|---|---|---|---|---|---|---|---|---|
| B | A | p # | B | A | p # | p | p (post hoc) *,& | ||
| TG (mg/dL) | 90.7 ± 38.1 | 101.5 (69.2–131.5) | 112 (89.4–138.2) | 0.867 | 99 (77.7–126.7) | 115.6 (77.1–145.5) | 0.280 | 0.200 | |
| c-HDL (mg/dL) | 50.1 ± 11.6 | 33.9 ± 7.4 * | 36.9 (34.4–39.5) | 0.327 | 35.9 ± 7.5 * | 35.5 (34–36.8) | 0.824 | 0.000 | 0.000 |
| Glu (mg/dL) | 78.9 ± 8.3 | 73.3 ± 13 | 82.1 ± 10.3 | 0.107 | 85.5 ± 12.3 & | 82.1 ± 7.6 | 0.370 | 0.011 | 0.009 |
| c-LDL (mg/dL) | 70.4 ± 30 | 70 ± 16.1 | 72.4 ± 41.3 | 0.826 | 90.1 ± 33.8 | 75.8 ± 37.7 | 0.154 | 0.070 | |
| TCho (mg/dL) | 138.7 ± 34.4 | 134 (104.4–143.9) | 131.4 ± 41.3 | 0.439 | 143 (124–166.1) | 134.7 ± 40.3 | 0.111 | 0.274 | |
| SBP (mmHg) | 101.7 ± 11 | 105 (100–112.5) | 100 (100–116.2) | 0.919 | 110 (110–120) * | 110 (100–120) | 0.070 | 0.003 | 0.002 |
| DBP (mmHg) | 69.5 ± 7 | 70 (67.5-72.5) | 70 (70–76.2) | 0.328 | 70 (70–80) * | 80 (70-80) | 0.855 | 0.010 | 0.008 |
| Weight (kg) | 55.5 ± 8.3 | 66.8 ± 7.2 * | 64.8 ± 7.2 # | 0.001 | 85.2 ± 10 *,& | 82.4 ±9.4 # | 0.001 | 0.000 | 0.000 |
| BMI (kg/m2) | 21.3 ± 2.1 | 26.8 (26.4–27.3) * | 25.7 (25.1–26.7) # | 0.001 | 31.9 (30.6–35.9) *,& | 31.7 (29.7–34.7) | 0.003 | 0.000 | 0.000 |
| WC (cm) | 78.4 ± 9.3 | 89.5 ± 8 * | 84.1 ± 6.3 # | 0.000 | 102.4 ± 8.7 *,& | 96.8 ± 10.3 # | 0.001 | 0.000 | 0.000 |
| SMM (kg) | 31.5 ± 6.2 | 35.4 ± 7.8 | 35.6 ± 8.1 | 0.874 | 41.1 ± 7 * | 40.3 ± 6.9 | 0.083 | 0.000 | 0.000 |
| ST (%) | 32.3 ± 5.2 | 40.7 ± 5.5 * | 39.6 ± 5.4 # | 0.038 | 46.1 ± 5.1 *,& | 45.1 ± 5.1 # | 0.021 | 0.000 | 0.000 |
| BFM (kg) | 16.4 ± 3.7 | 26.3 ± 3.6 * | 25.2 ± 4.1 # | 0.025 | 38.6 ± 5.8 *,& | 36.3 ± 5.7 # | 0.001 | 0.000 | 0.000 |
| VAT (cm2) | 61 ± 21.4 | 111.3 ± 22.3 * | 106.3 ± 24.6 # | 0.020 | 174 ± 38.6 *,& | 161 ± 34.6 # | 0.000 | 0.000 | 0.000 |
| Variable (n = 59) (%) | Normal (n = 29) | Overweight (n = 14) | Obesity (n = 16) | p (ANOVA) | |||||
|---|---|---|---|---|---|---|---|---|---|
| B | A | p # | B | A | p# | p | p (post hoc) *,& | ||
| Total Lymphocytes | 30.2 ± 9.7 | 29.9 (27.8–40.9) | 26.1 ± 8.2 # | 0.019 | 30.3 (27.4–32.4) | 31.1 ± 8.6 | 0.798 | 0.600 | |
| Monocytes | 8.3 (6.5–9.9) | 7.7 ± 2.3 | 7.3 (6.6–8) | 0.636 | 6.4 ± 2 * | 7.4 (6.9–8.3) | 0.061 | 0.017 | 0.014 |
| Granulocytes | 63.9 (56.5–69.3) | 61.5 (53.1–66.3) | 66.6 ± 7.6 # | 0.016 | 62.7 (61–66.2) | 60.9 ± 8.5 | 0.530 | 0.560 | |
| Lymphocytes B (CD19) | 12.7 (7.1–23.1) | 14.8 (10–23.4) | 15.4 (9.9–19.1) | 0.635 | 13.7 (9.4–23.2) | 9.3 (7.9–16) | 0.052 | 0.384 | |
| Lymphocytes NK (CD16CD56) | 20.4 ± 8.6 | 14.3 ± 5.1 * | 10.9 (7.5–17.6) | 0.253 | 17.2 ± 5.9 | 13.3 (8.9–23.9) | 0.413 | 0.036 | 0.041 |
| Lymphocytes T CD3+ | 63.7 ± 12.7 | 68.2 ± 8.7 | 71.4 ± 8.4 | 0.128 | 65.6 ± 10.3 | 72.1 ± 9.3 # | 0.012 | 0.456 | |
| Lymphocytes T CD4+ | 52.4 ± 11.5 | 51.9 ± 7.5 | 53.5 ± 6.8 | 0.217 | 56.2 ± 10.6 | 54.2 ± 10.9 | 0.455 | 0.506 | |
| CD4+CD62- | 29.1 ± 10 | 46.4 ± 18.3 * | 41.2 ± 13.5 | 0.538 | 36 ± 24.7 | 40.1 ± 15.5 | 0.644 | 0.053 | 0.058 |
| Lymphocytes T CD8+ | 33.4 ± 9 | 39.4 ± 13.7 | 32.6 ± 6.5 | 0.143 | 23.9 ± 6.5 & | 23.5 ± 9.3 | 0.871 | 0.035 | 0.031 |
| CD8+CD28- | 31.7 ± 12.9 | 34.8 ± 20.5 | 32 ± 12.9 | 0.700 | 25.8 ± 16.2 | 22.4 ± 9.6 | 0.476 | 0.587 | |
| CD3+CD45RA+ | 53.8 (43.6–61) | 36.8 ± 12.9 * | 39.4 ± 11.3 | 0.199 | 35.5 ± 12.3 * | 35.5 ± 12.4 | 0.988 | 0.000 | 0.003 |
| CD3+CD54RO+ | 32.5 ± 9.5 | 45.6 ± 10.9 * | 44.2 ± 8.2 | 0.380 | 40.1 ± 13 | 42.7 ± 11.3 | 0.327 | 0.006 | 0.008 |
| CD3+ CD45RA+CD45RO+ | 13.6 ± 4.1 | 17.7 ± 6.8 | 14.8 (11–18.1) | 0.236 | 18.8 ± 7.7 * | 18.7 (14.4–25.6) | 0.494 | 0.054 | 0.080 |
| CD4+ CD45RA+ | 41.5 ± 10.1 | 24.8 ± 10.6 * | 28.1 ± 13 | 0.183 | 26.2 ± 8.2 * | 26.9 ± 10.2 | 0.791 | 0.000 | 0.000 |
| CD4+ CD45RO+ | 40.7 ± 10.6 | 60.1 ± 11.2 * | 60.3 ± 12.7 | 0.944 | 51.9 ± 12.5 * | 58.9 ± 12.3 # | 0.016 | 0.000 | 0.000 |
| CD4+ CD45RA+CD45RO+ | 14.1 ± 5.2 | 14 ± 3.9 | 11.1 (7.8–14.3) | 0.092 | 17.6 ± 5.8 | 11.8 (8.6–18.5) # | 0.034 | 0.114 | |
| Leukocyte Cells (%) | Variables | p | p |
|---|---|---|---|
| Monocytes Δ | DBP Δ (mmHg) | −0.555 | 0.003 * |
| ST Δ (%) | 0.588 | 0.013 * | |
| Lymphocytes B Δ | c-LDL Δ (md/dL) | 0.370 | 0.069 |
| Lymphocytes NK Δ | TG Δ (md/dL) | 0.431 | 0.032 * |
| Lymphocytes T CD4+ Δ | c-HDL Δ (md/dL) | 0.339 | 0.090 |
| ST Δ (%) | −0.446 | 0.073 | |
| Lymphocytes T CD4+CD62- Δ | WC Δ (cm) | −0.553 | 0.026 * |
| TG Δ (md/dL) | 0.365 | 0.056 | |
| Lymphocytes T CD8+CD28- Δ | ST Δ (%) | 0.721 | 0.028 * |
| T CD4+CD45RA+ Δ | TCho Δ (md/dL) | 0.487 | 0.030 * |
| c-LDL Δ (md/dL) | 0.474 | 0.035 * | |
| WC Δ (cm) | 0.575 | 0.008 * | |
| c-HDL Δ (md/dL) | 0.395 | 0.085 | |
| T CD4+CD45RO+ Δ | Glu Δ (md/dL) | −0.501 | 0.021 * |
| c-HDL Δ (md/dL) | −0.393 | 0.078 | |
| CD4+CD45RO+CD45RA+ Δ | BFM Δ (kg) | −0.516 | 0.071 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-López, C.P.; González-Torres, M.C.; Aguilar-Salinas, C.A.; Nájera-Medina, O. DASH Diet as a Proposal for Improvement in Cellular Immunity and Its Association with Metabolic Parameters in Persons with Overweight and Obesity. Nutrients 2021, 13, 3540. https://doi.org/10.3390/nu13103540
Rodríguez-López CP, González-Torres MC, Aguilar-Salinas CA, Nájera-Medina O. DASH Diet as a Proposal for Improvement in Cellular Immunity and Its Association with Metabolic Parameters in Persons with Overweight and Obesity. Nutrients. 2021; 13(10):3540. https://doi.org/10.3390/nu13103540
Chicago/Turabian StyleRodríguez-López, Carmen Paulina, María Cristina González-Torres, Carlos A. Aguilar-Salinas, and Oralia Nájera-Medina. 2021. "DASH Diet as a Proposal for Improvement in Cellular Immunity and Its Association with Metabolic Parameters in Persons with Overweight and Obesity" Nutrients 13, no. 10: 3540. https://doi.org/10.3390/nu13103540
APA StyleRodríguez-López, C. P., González-Torres, M. C., Aguilar-Salinas, C. A., & Nájera-Medina, O. (2021). DASH Diet as a Proposal for Improvement in Cellular Immunity and Its Association with Metabolic Parameters in Persons with Overweight and Obesity. Nutrients, 13(10), 3540. https://doi.org/10.3390/nu13103540