
Choice Architecture Cueing to Healthier Dietary Choices and Physical Activity at the Workplace: Implementation and Feasibility Evaluation

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Recruitment of Participating Organisations
2.3. Intervention Development and Content
2.4. Implementation Process
2.5. Data Collection
2.5.1. Interviews
2.5.2. Observation
2.6. Analyses
2.6.1. Fidelity
2.6.2. Facilitators and Barriers of Implementation
2.6.3. Maintenance
3. Results
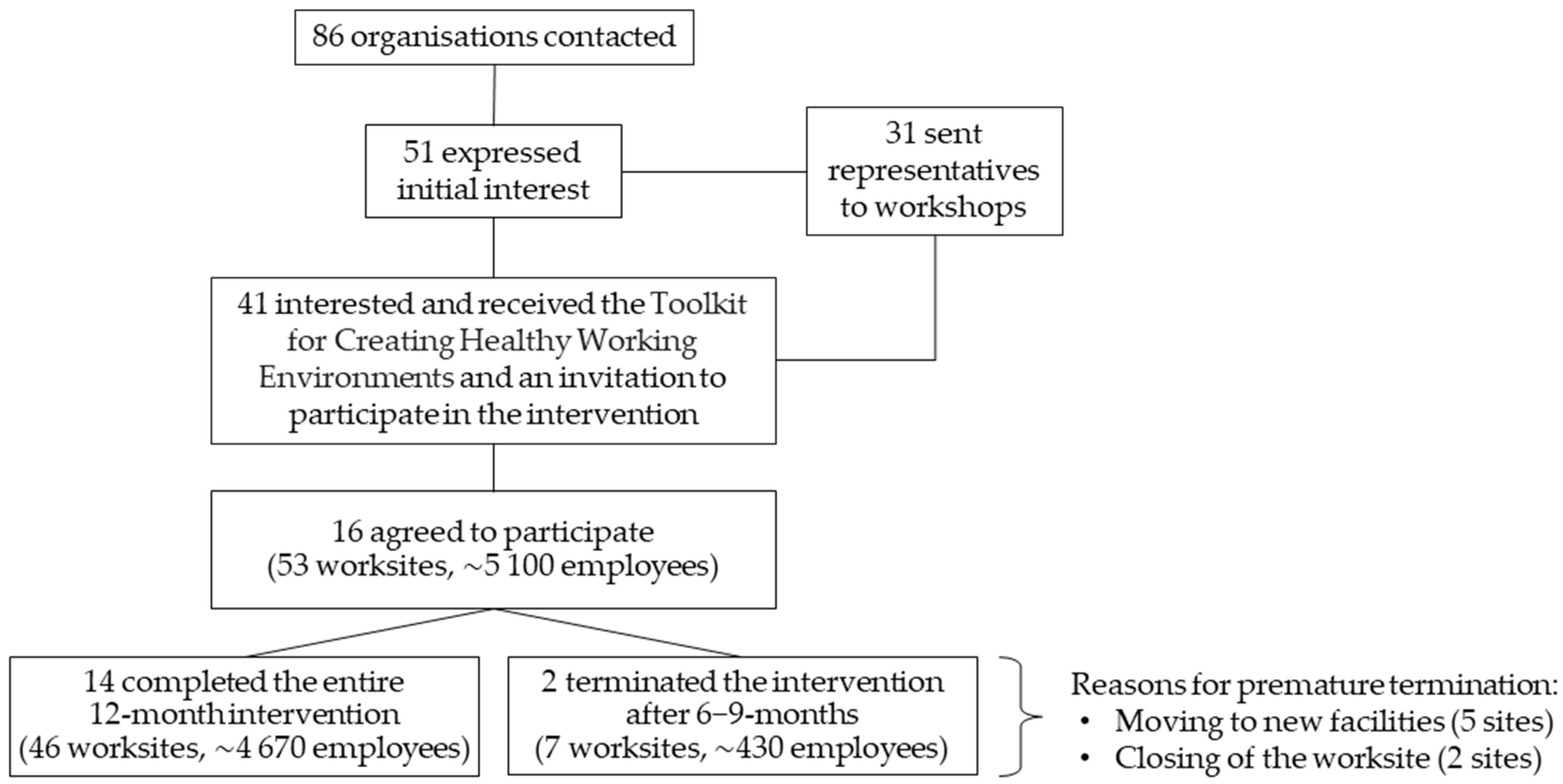
3.1. Participating Organisations
3.2. Characteristics of Implemented Strategies
3.2.1. Descriptions, Mechanisms, and Settings
3.2.2. Ease of Implementation
3.2.3. Required Purchases
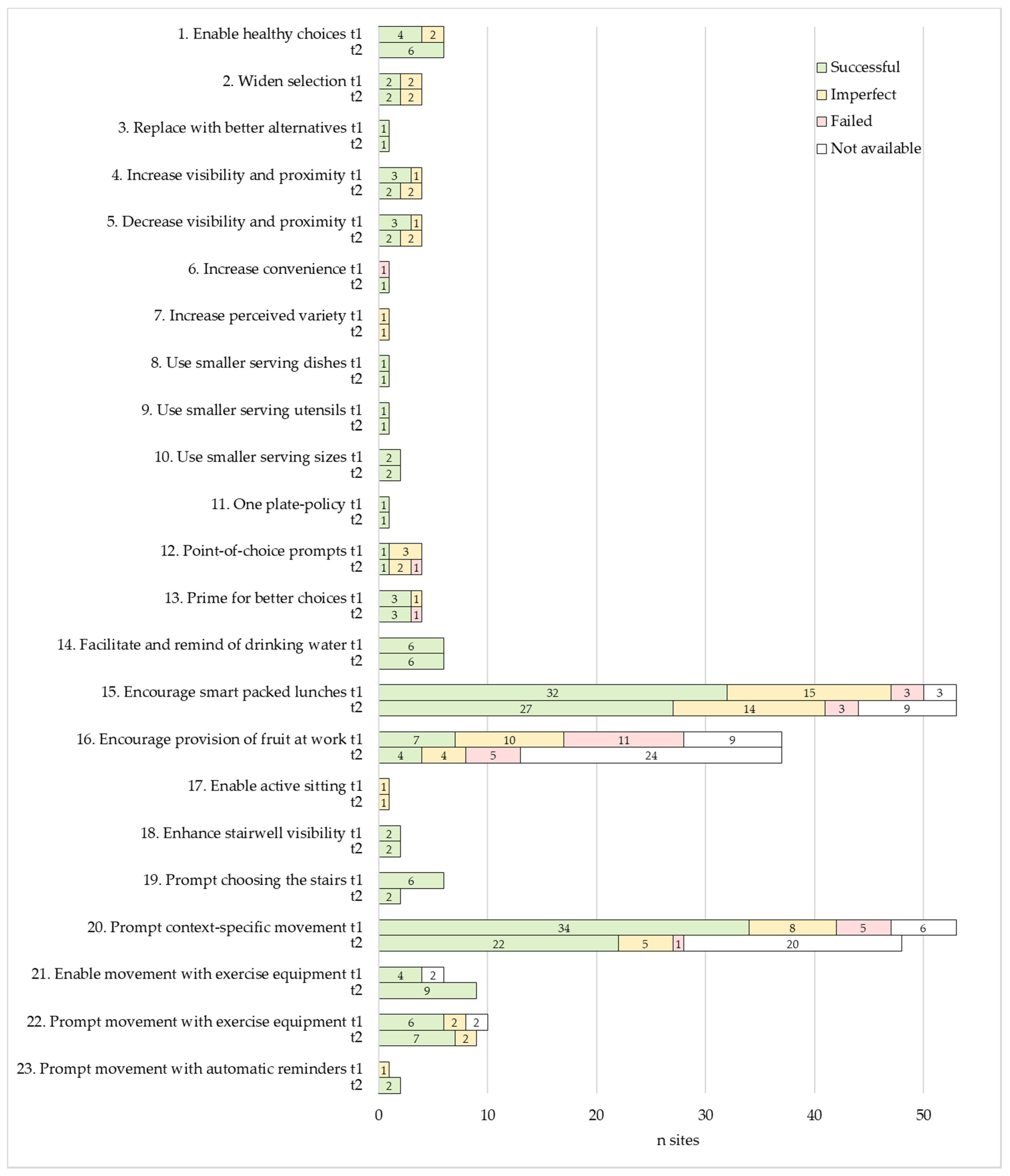
3.3. Fidelity
3.3.1. Dose Delivered
3.3.2. Quality of Implementation
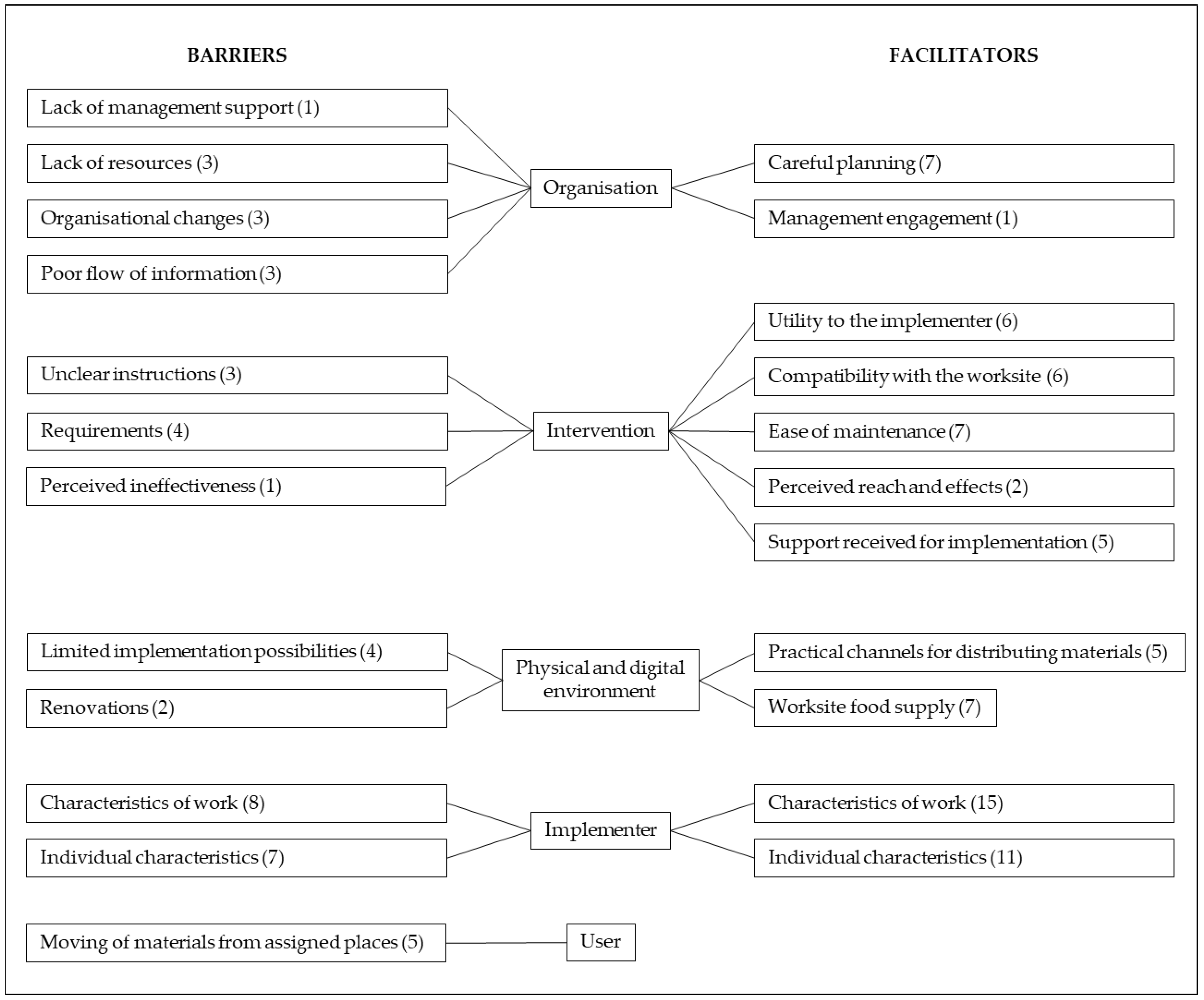
3.4. Facilitators and Barriers of Implementation
3.4.1. Facilitators
Characteristics of the Organisation
Characteristics of the Intervention
Characteristics of the Physical and Digital Environment
Characteristics of the Implementer
3.4.2. Barriers
Characteristics of the Organisation
Characteristics of the Intervention
Characteristics of the Physical and Digital Environment
Characteristics of the Implementer
Characteristics of the User
3.5. Maintenance
4. Discussion
4.1. Implementation and Feasibility Evaluation
4.1.1. Applicability to Worksites, Ease of Implementation, and Required Purchases
4.1.2. Fidelity
4.1.3. Facilitators and Barriers of Implementation
4.2. Strenghts and Limitations
4.3. Implications for Practice and Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marteau, T.M. Changing Minds about Changing Behaviour. Lancet 2018, 391, 116–117. [Google Scholar] [CrossRef]
- WHO; World Economic Forum. Preventing Noncommunicable Diseases in the Workplace through Diet and Physical Activity: WHO/World Economic Forum Report of a Joint Event; WHO: Geneva, Switzerland; World Economic Forum: Geneva, Switzerland, 2008; ISBN 978 92 4 159632 9. [Google Scholar]
- Krekel, C.; Ward, G.; De Neve, J.-E. Employee Wellbeing, Productivity, and Firm Performance. Saïd Bus. School WP 2019-04 2019, 1–44. Available online: https://ssrn.com/abstract=3356581 (accessed on 12 October 2021). [CrossRef] [Green Version]
- Grimani, A.; Aboagye, E.; Kwak, L. The Effectiveness of Workplace Nutrition and Physical Activity Interventions in Improving Productivity, Work Performance and Workability: A Systematic Review. BMC Public Health 2019, 19, 1676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OECD/EU. Health at a Glance: Europe 2016—State of Health in the EU Cycle; OECD Publishings: Paris, France, 2016; ISBN 9789264265585. [Google Scholar]
- Beard, E.; West, R.; Lorencatto, F.; Gardner, B.; Michie, S.; Owens, L.; Shahab, L. What Do Cost-Effective Health Behaviour-Change Interventions Contain? A Comparison of Six Domains. PLoS ONE 2019, 14, e0213983. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.; Mytton, O.; White, M.; Monsivais, P. Why Are Some Population Interventions for Diet and Obesity More Equitable and Effective Than Others? The Role of Individual Agency. PLoS Med. 2016, 13, e1001990. [Google Scholar] [CrossRef] [Green Version]
- Sheeran, P.; Maki, A.; Montanaro, E.; Avishai-Yitshak, A.; Bryan, A.; Klein, W.M.P.; Miles, E.; Rothman, A.J. The Impact of Changing Attitudes, Norms, and Self-Efficacy on Health-Related Intentions and Behavior: A Meta-Analysis. Health Psychol. 2016, 35, 1178–1188. [Google Scholar] [CrossRef]
- Hollands, G.J.; French, D.P.; Griffin, S.J.; Prevost, A.T.; Sutton, S.; King, S.; Marteau, T.M. The Impact of Communicating Genetic Risks of Disease on Risk-Reducing Health Behaviour: Systematic Review with Meta-Analysis. BMJ 2016, 352, i1102. [Google Scholar] [CrossRef] [Green Version]
- Strack, F.; Deutsch, R. Reflective and Impulsive Determinants of Social Behavior. Personal. Soc. Psychol. Rev. 2004, 8, 220–247. [Google Scholar] [CrossRef] [Green Version]
- Bargh, J.A.; Chartrand, T.L. The Unbearable Automaticity of Being. Am. Psychol. 1999, 54, 462–479. [Google Scholar] [CrossRef]
- Webb, T.L.; Sheeran, P. Does Changing Behavioral Intentions Engender Behavior Change? A Meta-Analysis of the Experimental Evidence. Psychol. Bull. 2006, 132, 249–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beauchamp, A.; Backholer, K.; Magliano, D.; Peeters, A. The Effect of Obesity Prevention Interventions According to Socioeconomic Position: A Systematic Review. Obes. Rev. 2014, 15, 541–554. [Google Scholar] [CrossRef]
- Veinot, T.C.; Mitchell, H.; Ancker, J.S. Good Intentions Are Not Enough: How Informatics Interventions Can Worsen Inequality. J. Am. Med. Inform. Assoc. 2018, 25, 1080–1088. [Google Scholar] [CrossRef] [Green Version]
- McGill, R.; Anwar, E.; Orton, L.; Bromley, H.; Lloyd-Williams, F.; O’Flaherty, M.; Taylor-Robinson, D.; Guzman-Castillo, M.; Gillespie, D.; Moreira, P.; et al. Are Interventions to Promote Healthy Eating Equally Effective for All? Systematic Review of Socioeconomic Inequalities in Impact. BMC Public Health 2015, 15, 457. [Google Scholar] [CrossRef] [Green Version]
- Marteau, T.M.; Rutter, H.; Marmot, M. Changing Behaviour: An Essential Component of Tackling Health Inequalities. BMJ 2021, 372, n332. [Google Scholar] [CrossRef]
- Schüz, B.; Meyerhof, H.; Hilz, L.K.; Mata, J. Equity Effects of Dietary Nudging Field Experiments: Systematic Review. Front. Public Health 2021, 9, 668998. [Google Scholar] [CrossRef] [PubMed]
- Hansen, P.G. The Definition of Nudge and Libertarian Paternalism: Does the Hand Fit the Glove? Eur. J. Risk Regul. 2016, 7, 155–174. [Google Scholar] [CrossRef] [Green Version]
- Thaler, R.H.; Sunstein, C.R. Nudge: Improving Decisions about Health, Wealth, and Happiness, Updated ed.; Penguin Books: London, UK, 2009; ISBN 9780300122237. [Google Scholar]
- Ensaff, H. A Nudge in the Right Direction: The Role of Food Choice Architecture in Changing Populations’ Diets. Proc. Nutr. Soc. 2021, 80, 195–206. [Google Scholar] [CrossRef]
- Hummel, D.; Maedche, A. How Effective Is Nudging? A Quantitative Review on the Effect Sizes and Limits of Empirical Nudging Studies. J. Behav. Exp. Econ. 2019, 80, 47–58. [Google Scholar] [CrossRef]
- Hollands, G.J.; Carter, P.; Shemilt, I.; Marteau, T.M.; Jebb, S.A.; Higgins, J.; Ogilvie, D. Altering the Availability or Proximity of Food, Alcohol and Tobacco Products to Change Their Selection and Consumption. Cochrane Database Syst. Rev. 2019, 9, CD012573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bucher, T.; Collins, C.; Rollo, M.E.; McCaffrey, T.A.; de Vlieger, N.; van der Bend, D.; Truby, H.; Perez-Cueto, F.J.A. Nudging Consumers towards Healthier Choices: A Systematic Review of Positional Influences on Food Choice. Br. J. Nutr. 2016, 115, 2252–2263. [Google Scholar] [CrossRef] [PubMed]
- Hollands, G.J.; Shemilt, I.; Marteau, T.M.; Jebb, S.A.; Lewis, H.B.; Wei, Y.; Higgins, J.P.T.; Ogilvie, D. Portion, Package or Tableware Size for Changing Selection and Consumption of Food, Alcohol and Tobacco. Cochrane Database Syst. Rev. 2015, 2015, CD011045. [Google Scholar] [CrossRef] [Green Version]
- Cadario, R.; Chandon, P. Which Healthy Eating Nudges Work Best? A Meta-Analysis of Field Experiments. Mark. Sci. 2019, 39, 459–665. [Google Scholar] [CrossRef]
- Crockett, R.; King, S.; Marteau, T.; Prevost, A.; Bignardi, G.; Roberts, N.; Stubbs, B.; Hollands, G.; Jebb, S. Nutritional Labelling for Promoting Healthier Food Purchasing and Consumption. Cochrane Database Syst. Rev. 2018, 2, CD009315. [Google Scholar] [CrossRef] [Green Version]
- Littlewood, J.A.; Lourenço, S.; Iversen, C.L.; Hansen, G.L. Menu Labelling Is Effective in Reducing Energy Ordered and Consumed: A Systematic Review and Meta-Analysis of Recent Studies. Public Health Nutr. 2016, 19, 2106–2121. [Google Scholar] [CrossRef]
- Jennings, C.A.; Yun, L.; Loitz, C.C.; Lee, E.-Y.; Mummery, W.K. A Systematic Review of Interventions to Increase Stair Use. Am. J. Prev. Med. 2017, 52, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, N.; Kukkonen-Harjula, K.; Verbeek, J.; Ijaz, S.; Hermans, V.; Pedisic, Z. Workplace Interventions for Reducing Sitting at Work. Cochrane Database Syst. Rev. 2018, 6, CD010912. [Google Scholar] [CrossRef]
- Hollands, G.J.; Marteau, T.M.; Fletcher, P.C. Non-Conscious Processes in Changing Health-Related Behaviour: A Conceptual Analysis and Framework. Health Psychol. Rev. 2016, 10, 381–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marteau, T.M.; Fletcher, P.C.; Munafò, M.R.; Hollands, G.J. Beyond Choice Architecture: Advancing the Science of Changing Behaviour at Scale. BMC Public Health 2021, 21, 1531. [Google Scholar] [CrossRef] [PubMed]
- Houghtaling, B.; Serrano, E.; Dobson, L.; Chen, S.; Kraak, V.I.; Harden, S.M.; Davis, G.C.; Misyak, S. Rural Independent and Corporate Supplemental Nutrition Assistance Program (SNAP)-Authorized Store Owners’ and Managers’ Perceived Feasibility to Implement Marketing-Mix and Choice-Architecture Strategies to Encourage Healthy Consumer Purchases. Transl. Behav. Med. 2019, 9, 888–898. [Google Scholar] [CrossRef] [PubMed]
- Frederick, K.D.; Gatwood, J.D.; Atchley, D.R.; Rein, L.J.; Ali, S.G.; Brookhart, A.L.; Crain, J.; Hagemann, T.M.; Ramachandran, S.; Chiu, C.Y.; et al. Exploring the Early Phase of Implementation of a Vaccine-Based Clinical Decision Support System in the Community Pharmacy. J. Am. Pharm. Assoc. 2020, 60, e292–e300. [Google Scholar] [CrossRef] [PubMed]
- Saulais, L.; Massey, C.; Perez-Cueto, F.J.A.; Appleton, K.M.; Dinnella, C.; Monteleone, E.; Depezay, L.; Hartwell, H.; Giboreau, A. When Are “Dish of the Day” Nudges Most Effective to Increase Vegetable Selection? Food Policy 2019, 85, 15–27. [Google Scholar] [CrossRef]
- Hartwell, H.; Bray, J.; Lavrushkina, N.; Rodrigues, V.; Saulais, L.; Giboreau, A.; Perez-Cueto, F.J.A.; Monteleone, E.; Depezay, L.; Appleton, K.M. Increasing Vegetable Consumption Out-of-home: VeggiEAT and Veg+projects. Nutr. Bull. 2020, 45, 424–431. [Google Scholar] [CrossRef]
- Zhou, X.; Perez-Cueto, F.J.A.; dos Santos, Q.; Bredie, W.L.P.; Molla-Bauza, M.B.; Rodrigues, V.M.; Buch-Andersen, T.; Appleton, K.M.; Hemingway, A.; Giboreau, A.; et al. Promotion of Novel Plant-Based Dishes among Older Consumers Using the ‘Dish of the Day’ as a Nudging Strategy in 4 EU Countries. Food Qual. Prefer. 2019, 75, 260–272. [Google Scholar] [CrossRef] [Green Version]
- dos Santos, Q.; Perez-Cueto, F.J.A.; Rodrigues, V.M.; Appleton, K.; Giboreau, A.; Saulais, L.; Monteleone, E.; Dinnella, C.; Brugarolas, M.; Hartwell, H. Impact of a Nudging Intervention and Factors Associated with Vegetable Dish Choice among European Adolescents. Eur. J. Nutr. 2020, 59, 231–247. [Google Scholar] [CrossRef] [Green Version]
- Szaszi, B.; Palinkas, A.; Palfi, B.; Szollosi, A.; Aczel, B. A Systematic Scoping Review of the Choice Architecture Movement: Toward Understanding When and Why Nudges Work. J. Behav. Decis. Mak. 2018, 31, 355–366. [Google Scholar] [CrossRef] [Green Version]
- Wierenga, D.; Engbers, L.H.; van Empelen, P.; Duijts, S.; Hildebrandt, V.H.; van Mechelen, W. What Is Actually Measured in Process Evaluations for Worksite Health Promotion Programs: A Systematic Review. BMC Public Health 2013, 13, 1190. [Google Scholar] [CrossRef] [Green Version]
- Wolfenden, L.; Goldman, S.; Stacey, F.G.; Grady, A.; Kingsland, M.; Williams, C.M.; Wiggers, J.; Milat, A.; Rissel, C.; Bauman, A.; et al. Strategies to Improve the Implementation of Workplace-Based Policies or Practices Targeting Tobacco, Alcohol, Diet, Physical Activity and Obesity. Cochrane Database Syst. Rev. 2018, 11, CD012439. [Google Scholar] [CrossRef] [PubMed]
- Durlak, J.A.; DuPre, E.P. Implementation Matters: A Review of Research on the Influence of Implementation on Program Outcomes and the Factors Affecting Implementation. Am. J. Community Psychol. 2008, 41, 327–350. [Google Scholar] [CrossRef] [PubMed]
- Wierenga, D.; Engbers, L.H.; van Empelen, P.; Hildebrandt, V.H.; van Mechelen, W. The Design of a Real-Time Formative Evaluation of the Implementation Process of Lifestyle Interventions at Two Worksites Using a 7-Step Strategy (BRAVO@Work). BMC Public Health 2012, 12, 619. [Google Scholar] [CrossRef] [Green Version]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O’Cathain, A.; Tinati, T.; Wight, D.; et al. Process Evaluation of Complex Interventions: Medical Research Council Guidance. BMJ 2015, 350, h1258. [Google Scholar] [CrossRef] [Green Version]
- Gearing, R.E.; El-Bassel, N.; Ghesquiere, A.; Baldwin, S.; Gillies, J.; Ngeow, E. Major Ingredients of Fidelity: A Review and Scientific Guide to Improving Quality of Intervention Research Implementation. Clin. Psychol. Rev. 2011, 31, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Dusenbury, L.; Brannigan, R.; Falco, M.; Hansen, W.B. A Review of Research on Fidelity of Implementation: Implications for Drug Abuse Prevention in School Settings. Health Educ. Res. 2003, 18, 237–256. [Google Scholar] [CrossRef] [PubMed]
- Carroll, C.; Patterson, M.; Wood, S.; Booth, A.; Rick, J.; Balain, S. A Conceptual Framework for Implementation Fidelity. Implement. Sci. 2007, 2, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellg, A.J.; Borrelli, B.; Resnick, B.; Hecht, J.; Minicucci, D.S.; Ory, M.; Ogedegbe, G.; Orwig, D.; Ernst, D.; Czajkowski, S. Enhancing Treatment Fidelity in Health Behavior Change Studies: Best Practices and Recommendations From the NIH Behavior Change Consortium. Health Psychol. 2004, 23, 443–451. [Google Scholar] [CrossRef]
- Moncher, F.J.; Prinz, R.J. Treatment Fidelity in Outcome Studies. Clin. Psychol. Rev. 1991, 11, 247–266. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Mitchie, S.; Nazareth, I.; Petticrew, M. Developing and Evaluating Complex Interventions: The New Medical Research Council Guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [Green Version]
- Toomey, E.; Hardeman, W.; Hankonen, N.; Byrne, M.; McSharry, J.; Matvienko-Sikar, K.; Lorencatto, F. Focusing on Fidelity: Narrative Review and Recommendations for Improving Intervention Fidelity within Trials of Health Behaviour Change Interventions. Health Psychol. Behav. Med. 2020, 8, 132–151. [Google Scholar] [CrossRef] [Green Version]
- Pihlajamäki, J.; Männikkö, R.; Tilles-Tirkkonen, T.; Karhunen, L.; Kolehmainen, M.; Schwab, U.; Lintu, N.; Paananen, J.; Järvenpää, R.; Harjumaa, M.; et al. Digitally Supported Program for Type 2 Diabetes Risk Identification and Risk Reduction in Real-World Setting: Protocol for the StopDia Model and Randomized Controlled Trial. BMC Public Health 2019, 19, 255. [Google Scholar] [CrossRef] [Green Version]
- Nordic Council of Ministers. Nordic Nutrition Recommendations 2012: Integrating Nutrition and Physical Activity, 5th ed.; Nordic Council of Ministers: Copenhagen, Denmark, 2014; ISBN 9789289326704. [Google Scholar]
- The National Nutrition Council of Finland. The Finnish Nutrition Recommendations 2014, 4th ed.; The National Nutrition Council of Finland: Helsinki, Finland, 2014; ISBN 978-952-453-801-5. [Google Scholar]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd ed.; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- Hollands, G.J.; Shemilt, I.; Marteau, T.M.; Jebb, S.A.; Kelly, M.P.; Nakamura, R.; Suhrcke, M.; Ogilvie, D. Altering Choice Architecture to Change Population Health Behaviour: A Large-Scale Conceptual and Empirical Scoping Review of Interventions within Micro-Environments; University of Cambridge: Cambridge, UK, 2013. [Google Scholar]
- Hollands, G.J.; Bignardi, G.; Johnston, M.; Kelly, M.P.; Ogilvie, D.; Petticrew, M.; Prestwich, A.; Shemilt, I.; Sutton, S.; Marteau, T.M. The TIPPME Intervention Typology for Changing Environments to Change Behaviour. Nat. Hum. Behav. 2017, 1, 0140. [Google Scholar] [CrossRef]
- Dolan, P.; Hallsworth, M.; Halpern, D.; King, D.; Metcalfe, R.; Vlaev, I. Influencing Behaviour: The Mindspace Way. J. Econ. Psychol. 2012, 33, 264–277. [Google Scholar] [CrossRef]
- Service, O.; Hallsworth, M.; Halpern, D.; Algate, F.; Gallagher, R.; Nguyen, S.; Ruda, S.; Sanders, M.; Pelenur, M.; Gyani, A.; et al. EAST—Four Simple Ways to Apply Behavioural Insights; The Behavioural Insights Team, Cabinet Office: London, UK, 2016.
- Heiberger, R.M.; Holland, B. Statistical Analysis and Data Display, 2nd ed.; Springer Texts in Statistics; Springer: New York, NY, USA, 2015; ISBN 978-1-4939-2121-8. [Google Scholar]
- Elo, S.; Kyngäs, H. The Qualitative Content Analysis Process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Sandelowski, M. What’s in a Name? Qualitative Description Revisited. Res. Nurs. Health 2010, 33, 77–84. [Google Scholar] [CrossRef]
- Graneheim, U.H.; Lundman, B. Qualitative Content Analysis in Nursing Research: Concepts, Procedures and Measures to Achieve Trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.; Reddy, M.; Zalta, A.K.; Schueller, S.M. Veterans’ Perspectives on Fitbit Use in Treatment for Post-Traumatic Stress Disorder: An Interview Study. JMIR Ment. Health 2018, 5, e10415. [Google Scholar] [CrossRef] [PubMed]
- Borghouts, J.; Eikey, E.; Mark, G.; de Leon, C.; Schueller, S.M.; Schneider, M.; Stadnick, N.; Zheng, K.; Mukamel, D.; Sorkin, D.H. Barriers to and Facilitators of User Engagement with Digital Mental Health Interventions: Systematic Review. JMIR 2021, 23, e24387. [Google Scholar] [CrossRef] [PubMed]
- Raulio, S.; Roos, E.; Prättälä, R. School and Workplace Meals Promote Healthy Food Habits. Public Health Nutr. 2010, 13, 987–992. [Google Scholar] [CrossRef] [Green Version]
- Raulio, S.; Roos, E.; Ovaskainen, M.-L.; Prättälä, R. Food Use and Nutrient Intake at Worksite Canteen or in Packed Lunches at Work among Finnish Employees. J. Foodserv. 2009, 20, 330–341. [Google Scholar] [CrossRef]
- Roos, E.; Sarlio-Lähteenkorva, S.; Lallukka, T. Having Lunch at a Staff Canteen Is Associated with Recommended Food Habits. Public Health Nutr. 2004, 7, 53–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mozaffarian, D.; Angell, S.Y.; Lang, T.; Rivera, J.A. Role of Government Policy in Nutrition—Barriers to and Opportunities for Healthier Eating. BMJ 2018, 361, k2426. [Google Scholar] [CrossRef] [Green Version]
- Ronto, R.; Rathi, N.; Worsley, A.; Sanders, T.; Lonsdale, C.; Wolfenden, L. Enablers and Barriers to Implementation of and Compliance with School-Based Healthy Food and Beverage Policies: A Systematic Literature Review and Meta-Synthesis. Public Health Nutr. 2020, 23, 2840–2855. [Google Scholar] [CrossRef]
- Niebylski, M.; Lu, T.; Campbell, N.; Arcand, J.; Schermel, A.; Hua, D.; Yeates, K.; Tobe, S.; Twohig, P.; L’Abbé, M.; et al. Healthy Food Procurement Policies and Their Impact. Int. J. Environ. Res. Public Health 2014, 11, 2608–2627. [Google Scholar] [CrossRef] [Green Version]
- Swinburn, B.A.; Kraak, V.I.; Allender, S.; Atkins, V.J.; Baker, P.I.; Bogard, J.R.; Brinsden, H.; Calvillo, A.; de Schutter, O.; Devarajan, R.; et al. The Global Syndemic of Obesity, Undernutrition, and Climate Change: The Lancet Commission Report. Lancet 2019, 393, 791–846. [Google Scholar] [CrossRef]
- Sacks, G.; Kwon, J.; Backholer, K. Do Taxes on Unhealthy Foods and Beverages Influence Food Purchases? Curr. Nutr. Rep. 2021, 10, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, N.N.; Tetens, I.; Løje, H.; Lassen, A.D. The Effectiveness of the Danish Organic Action Plan 2020 to Increase the Level of Organic Public Procurement in Danish Public Kitchens. Public Health Nutr. 2016, 19, 3428–3435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marteau, T.M.; Hollands, G.J.; Fletcher, P.C. Changing Human Behavior to Prevent Disease: The Importance of Targeting Automatic Processes. Science 2012, 337, 1492–1495. [Google Scholar] [CrossRef] [Green Version]
- Rojatz, D.; Merchant, A.; Nitsch, M. Factors Influencing Workplace Health Promotion Intervention: A Qualitative Systematic Review. Health Promot. Int. 2017, 32, 831–839. [Google Scholar] [CrossRef] [Green Version]
- May, C.; Finch, T. Implementing, Embedding, and Integrating Practices: An Outline of Normalization Process Theory. Sociology 2009, 43, 535–554. [Google Scholar] [CrossRef]
- May, C.; Rapley, T.; Mair, F.S.; Treweek, S.; Murray, E.; Ballini, L.; Macfarlane, A.; Girling, M.; Finch, T.L. Normalization Process Theory On-Line Users’ Manual, Toolkit and NoMAD Instrument. Available online: http://www.normalizationprocess.org/ (accessed on 13 June 2021).
- Rogers, E.M. Diffusion of Innovations, 5th ed.; Free Press: New York, NY, USA, 2003; ISBN 0-7432-5823-1. [Google Scholar]
- Wandersman, A.; Duffy, J.; Flaspohler, P.; Noonan, R.; Lubell, K.; Stillman, L.; Blachman, M.; Dunville, R.; Saul, J. Bridging the Gap Between Prevention Research and Practice: The Interactive Systems Framework for Dissemination and Implementation. Am. J. Community Psychol. 2008, 41, 171–181. [Google Scholar] [CrossRef]
- Lally, P.; van Jaarsveld, C.H.M.; Potts, H.W.W.; Wardle, J. How Are Habits Formed: Modelling Habit Formation in the Real World. Eur. J. Soc. Psychol. 2010, 40, 998–1009. [Google Scholar] [CrossRef] [Green Version]
- van der Weiden, A.; Benjamins, J.; Gillebaart, M.; Ybema, J.F.; de Ridder, D. How to Form Good Habits? A Longitudinal Field Study on the Role of Self-Control in Habit Formation. Front. Psychol. 2020, 11, 560. [Google Scholar] [CrossRef]
- Gardner, B.; Rebar, A.L. Habit Formation and Behavior Change. Oxford Research Encyclopedia of Psychology; Oxford University Press: Oxford, UK, 2019. [Google Scholar] [CrossRef]
- Gollwitzer, P.M.; Sheeran, P. Implementation Intentions and Goal Achievement: A Meta-analysis of Effects and Processes. Adv. Exp. Soc. Psychol. 2006, 38, 69–119. [Google Scholar] [CrossRef] [Green Version]
- Lally, P.; Gardner, B. Promoting Habit Formation. Health Psychol. Rev. 2013, 7, S137–S158. [Google Scholar] [CrossRef]
- Gollwitzer, P.M. Implementation Intentions: Strong Effects of Simple Plans. Am. Psychol. 1999, 54, 493–503. [Google Scholar] [CrossRef]
- Sheeran, P. Intention—Behavior Relations: A Conceptual and Empirical Review. Eur. Rev. Soc. Psychol. 2002, 12, 1–36. [Google Scholar] [CrossRef]
- Sunstein, C.R. Nudges That Fail. Behav. Public Policy 2017, 1, 4–25. [Google Scholar] [CrossRef]
- Weingarten, E.; Chen, Q.; McAdams, M.; Yi, J.; Hepler, J.; Albarracín, D. From Primed Concepts to Action: A Meta-Analysis of the Behavioral Effects of Incidentally Presented Words. Psychol. Bull. 2016, 142, 472–497. [Google Scholar] [CrossRef]
- Papies, E.K. Health Goal Priming as a Situated Intervention Tool: How to Benefit from Nonconscious Motivational Routes to Health Behaviour. Health Psychol. Rev. 2016, 10, 408–424. [Google Scholar] [CrossRef] [Green Version]
- Junghans, A.F.; Cheung, T.T.; de Ridder, D.D. Under Consumers’ Scrutiny—An Investigation into Consumers’ Attitudes and Concerns about Nudging in the Realm of Health Behavior. BMC Public Health 2015, 15, 336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Ridder, D.; Kroese, F.; van Gestel, L. Nudgeability: Mapping Conditions of Susceptibility to Nudge Influence. Perspect. Psychol. Sci. 2021. [Google Scholar] [CrossRef]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the Public Health Impact of Health Promotion Interventions: The RE-AIM Framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Organisation | Sector | Field of Operation | n Sites | n Employees 1 | % Men | Type of Work | Shift Work |
|---|---|---|---|---|---|---|---|
| O1 | Private | Retail | 5 | 360 | 21 | Mixed 2 | Yes |
| O2 | Private | Metal industry | 1 | 600 | 80 | Mixed 2 | Yes |
| O3 | Private | Forest industry | 1 | 950 | 78 | Mixed 2 | Yes |
| O4 | Private | Retail | 3 | 300 | 20 | Mixed 2 | Yes |
| O5 | Private | Higher education | 5 | 370 | 34 | Sedentary | No |
| O6 | Public | Municipality | 1 | 70 | 29 | Sedentary | No |
| O7 | Private | Chemical industry | 1 | 400 | 75 | Mixed 2 | Yes |
| O8 | Private | Farming | 1 | 140 | 35 | Mixed 2 | Yes |
| O9 | Public | Municipality | 1 | 80 | 39 | Sedentary | No |
| O10 | Public | Municipality | 3 | 250 | 32 | Mixed 2 | Yes |
| O11 | Private | Construction industry | 5 | 180 | 91 | Mixed 2 | No |
| O12 | Public | Health care | 20 | 490 | 46 | Mixed 2 | Yes |
| O13 | Private | Food industry | 1 | 250 | 70 | Mixed 2 | Yes |
| O14 | Private | Retail | 3 | 320 | 18 | Mixed 2 | Yes |
| O15 | Public | Municipality | 1 | 300 | 20 | Sedentary | No |
| O16 | Public | Welfare services | 1 | 40 | 5 | Mixed 2 | No |
| Target | Practical Strategy | Description | Behaviour Change Mechanism 3 | Ease of Implementation 4 | Required Purchases 4 | Setting | n |
|---|---|---|---|---|---|---|---|
| Food provision | |||||||
| Nutrition |
| Healthy 1 food and beverage choices, such as fruit and smoothies made available. | Product availability ↑ T | Moderate | Minor | Meetings | 6 |
| Nutrition |
| Greater variety of healthy 1 food and beverage options available. | Product availability ↑ T Attractive (salience ↑) M, E | Moderate | Minor | Cafeteria | 4 |
| Nutrition |
| Energy dense and nutritionally poor options replaced with similar but nutritionally better alternatives. | Product availability ↑ T Easy (substitution, default) E | Moderate | Minor | Meetings | 1 |
| Nutrition |
| Healthy 1 options placed: (a) in visible spots, (b) at the beginning of the buffet, (c) closer to the chooser (e.g., in front row), and/or (d) in the middle of the tray, shelf, or showcase. | Product position T Easy (friction costs ↓) E Attractive (salience ↑) M, E | Demanding | None | Cafeteria | 4 |
| Nutrition |
| Less healthy options placed: (a) in less visible spots, (b) at the end of the buffet, (c) further away from the chooser (e.g., in back row), and/or (d) on the edge of the tray, shelf, or showcase. | Product position T Less easy (friction costs ↑) E Less attractive (salience ↓) M, E | Demanding | None | Cafeteria | 4 |
| Nutrition |
| Fruit and vegetable served ready to eat, i.e., washed, peeled if needed, and cut into pieces. | Product functionality T Easy (friction costs ↓) E | Demanding | None | Meetings | 1 |
| Nutrition |
| Salad components served from separate serving dishes to encourage greater consumption. | Product presentation T Attractive (salience ↑) M, E | Moderate | None | Cafeteria | 1 |
| Nutrition |
| Less healthy foods served from smaller serving dishes. | Product size T Easy (default) M, E | Moderate | None | Cafeteria | 1 |
| Nutrition |
| Less healthy foods served with smaller tongs and spoons. | Product size T Less easy (default) M, E | Moderate | None | Cafeteria | 1 |
| Nutrition |
| Less healthy options served in smaller sizes. | Product size T Easy (default) M, E | Moderate | None | Meetings | 2 |
| Nutrition |
| Separate bread and salad plates moved out of sight to guide employees to choose one large plate; thus facilitating the composition of the meal according to the plate model (i.e., 1/2 vegetable, 1/4 protein, and 1/4 carbohydrates). For the strategy to be effective, salads should be placed first in the buffet line. | Product size T Easy (default) M, E | Easy | None | Cafeteria | 1 |
| Nutrition |
| Healthy 1 options indicated with the Heart Symbol 2 on menus and at the point of choice. | Information on related objects T Attractive (salience ↑) M, E Timely (prompting) E Easy (simplification) E | Demanding | None 5 | Cafeteria | 4 |
| Nutrition |
| Follow the heart posters 2 at restaurant entrance and/or at the beginning of the buffet to guide customers to notice and choose options labelled with the Heart Symbol 2. | Information within the wider environment T Attractive (salience ↑) M, E Timely (priming) M, E | Easy | None 5 | Cafeteria | 4 |
| Drinking water | |||||||
| Nutrition |
| Personal, reusable water bottles provided for employees. | Related object availability ↑ T Easy (friction costs ↓) E | Easy | Minor | Personal workstation | 6 |
| Packed lunches and snacks | |||||||
| Nutrition |
| Temptingly named, visually attractive, and seasonal StopDia packed lunch of the week recipes 2 promoted and provided at workplace coffee rooms and/or via electronic channels, such as info-screens, company intranet, and newsletters. The campaign comprises one recipe for each week of the year, and all recipes meet the nutritional criteria of the Heart Symbol 1. | Easy (friction costs ↓, chunking) E Attractive (salience ↑) M, E Social (descriptive norm) M, E Timely (priming) M, E Affect M | Moderate | None 5 | Coffee rooms | 48 |
| Nutrition |
| The promotion and provision of the fruit crew starting kit 2 that facilitates colleagues to found a fruit circle and consequently have fresh fruit available at the workplace. | Social (network nudge, commitment contracts, descriptive norm, reciprocity) M, E Attractive (gamification, salience ↑) M, E Timely (implementation intentions) E | Easy | None 5 | Coffee rooms | 17 |
| Time spent sitting | |||||||
| Physical activity |
| Introduction of alternative seats, such as wobble chairs or balance cushions. | Product availability T Easy (friction costs ↓) E | Easy | Substantial | Common environments | 1 |
| Stair use | |||||||
| Physical activity |
| Footprints attached on the floor to lead to stairs from the point of choice between the stairs and the elevator. | Atmospheric properties of the wider environment T Attractive (salience ↑) M, E Timely (prompting) E | Easy | None 5 | Elevator, stairs | 2 |
| Physical activity |
| StopDia logo (a stop hand sign with a heart on the palm) 2 placed on elevator doors, next to elevator call buttons, or in their immediacy. | Timely (prompting) E | Easy | None 5 | Elevator | 6 |
| Movement breaks | |||||||
| Physical activity |
| StopDia Flex! movement posters 2 placed on salient spots where employees typically pause for a moment and have the opportunity to perform movements. Such spots can be, for example, by copy machines, microwaves, kettles, coffee makers, and bathrooms. | Timely (prompting) E Attractive (salience ↑) M, E Easy (chunking) E | Easy | None 5 | Common environments | 43 |
| Physical activity |
| Light exercise equipment made available, for example, gym sticks, balance boards, or hanging bars. | Product availability T Easy (friction costs ↓) E | Easy | Minor | Common environments | 9 |
| Physical activity |
| Available exercise equipment placed on salient spots where employees typically pause for a moment, and an opportunity for a short exercise break occurs, for example, by copy machines, micros, kettles, or coffee makers. | Timely (prompting) E Attractive (salience ↑) M, E | Moderate | None | Common environments | 13 |
| Physical activity |
| An application that prompts to take short exercise breaks at pre-set intervals provided for employees. | Timely (prompting) E | Easy | Minor | Personal workstation | 2 |
| Independent Variable | t1 | t2 | ||||||
|---|---|---|---|---|---|---|---|---|
| n Cases | Mean | 95% CI for Mean | p1 | n Cases | Mean | 95% CI for Mean | p1 | |
| Ease of implementation | ||||||||
| Easy | 100 | 1.47 | 1.32–1.62 | 0.535 2 | 68 | 1.65 | 1.49–1.81 | 0.187 2 |
| Moderate | 74 | 1.62 | 1.49–1.75 | 69 | 1.64 | 1.50–1.77 | ||
| Demanding | 13 | 1.46 | 1.06–1.86 | 13 | 1.38 | 0.99–1.78 | ||
| Researcher assisted intervention launch | ||||||||
| Yes | 63 | 1.71 | 1.59–1.84 | 0.021 3 | 54 | 1.59 | 1.42–1.76 | 0.625 3 |
| No | 124 | 1.44 | 1.30–1.57 | 96 | 1.64 | 1.51–1.76 | ||
| Direct contact to intervention site | ||||||||
| Yes | 127 | 1.68 | 1.59–1.77 | 0.000 3 | 117 | 1.64 | 1.54–1.74 | 0.980 3 |
| No | 60 | 1.22 | 0.99–1.44 | 33 | 1.55 | 1.26–1.83 | ||
| SMS reminders for strategy 15 | ||||||||
| Yes | 12 | 1.83 | 1.59–2.08 | 0.100 3 | 12 | 1.75 | 1.46–2.04 | 0.290 3 |
| No | 38 | 1.50 | 1.29–1.71 | 32 | 1.47 | 1.23–1.71 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rantala, E.; Vanhatalo, S.; Tilles-Tirkkonen, T.; Kanerva, M.; Hansen, P.G.; Kolehmainen, M.; Männikkö, R.; Lindström, J.; Pihlajamäki, J.; Poutanen, K.; et al. Choice Architecture Cueing to Healthier Dietary Choices and Physical Activity at the Workplace: Implementation and Feasibility Evaluation. Nutrients 2021, 13, 3592. https://doi.org/10.3390/nu13103592
Rantala E, Vanhatalo S, Tilles-Tirkkonen T, Kanerva M, Hansen PG, Kolehmainen M, Männikkö R, Lindström J, Pihlajamäki J, Poutanen K, et al. Choice Architecture Cueing to Healthier Dietary Choices and Physical Activity at the Workplace: Implementation and Feasibility Evaluation. Nutrients. 2021; 13(10):3592. https://doi.org/10.3390/nu13103592
Chicago/Turabian StyleRantala, Eeva, Saara Vanhatalo, Tanja Tilles-Tirkkonen, Markus Kanerva, Pelle Guldborg Hansen, Marjukka Kolehmainen, Reija Männikkö, Jaana Lindström, Jussi Pihlajamäki, Kaisa Poutanen, and et al. 2021. "Choice Architecture Cueing to Healthier Dietary Choices and Physical Activity at the Workplace: Implementation and Feasibility Evaluation" Nutrients 13, no. 10: 3592. https://doi.org/10.3390/nu13103592
APA StyleRantala, E., Vanhatalo, S., Tilles-Tirkkonen, T., Kanerva, M., Hansen, P. G., Kolehmainen, M., Männikkö, R., Lindström, J., Pihlajamäki, J., Poutanen, K., Karhunen, L., & Absetz, P. (2021). Choice Architecture Cueing to Healthier Dietary Choices and Physical Activity at the Workplace: Implementation and Feasibility Evaluation. Nutrients, 13(10), 3592. https://doi.org/10.3390/nu13103592