Association between Plant-Based Dietary Patterns and Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Prospective Cohort Studies



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Methods Used to Assess the Adherence to Plant-Based Dietary Patterns
2.5. Data Synthesis and Analysis
2.6. Data Harmonization and Dose–Response Meta-Analyses
3. Results
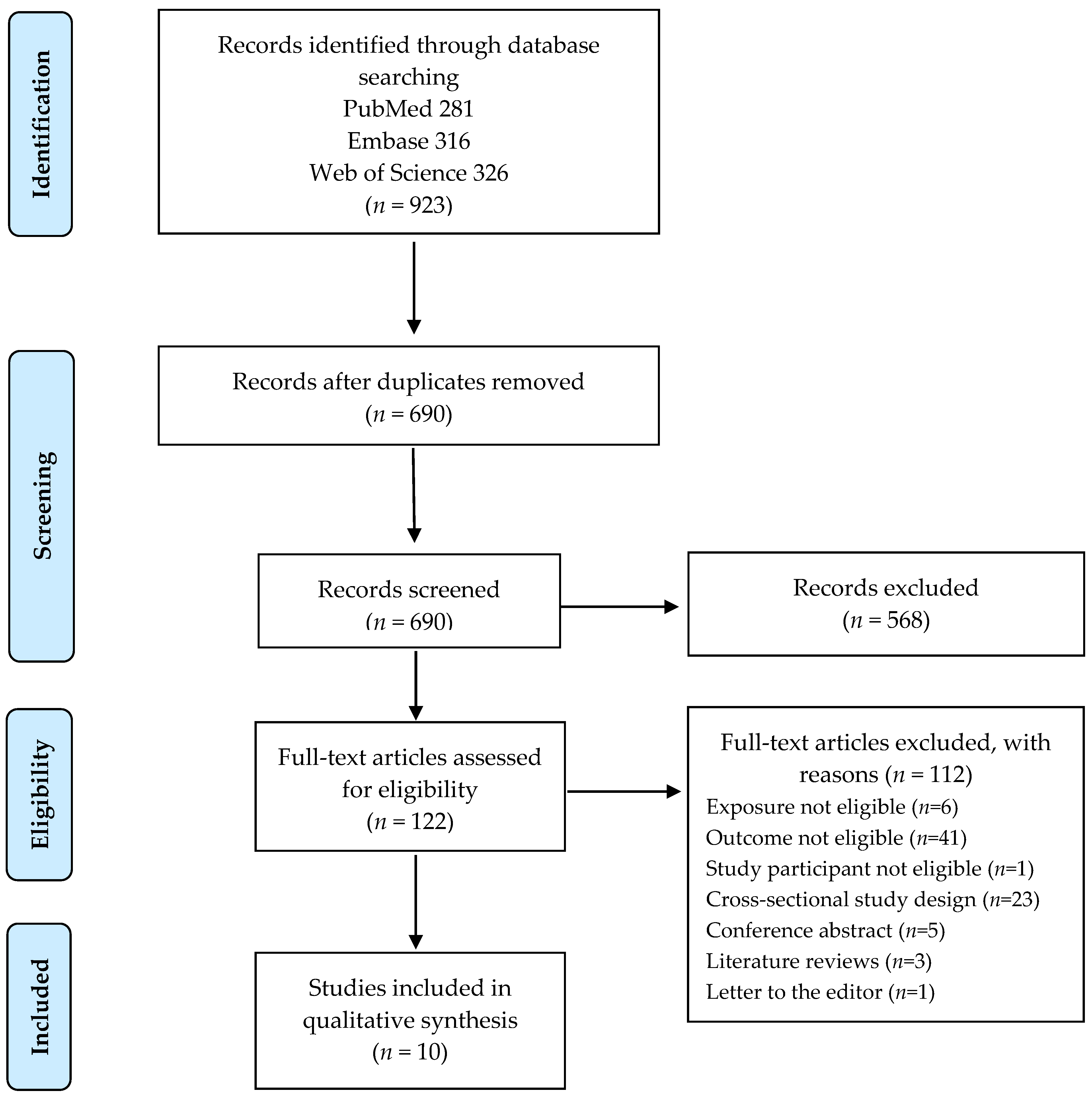
3.1. Literature Search
3.2. Characteristics of the Included Studies
3.3. Plant-Based Dietary Pattern and Risk of Cardiovascular Disease
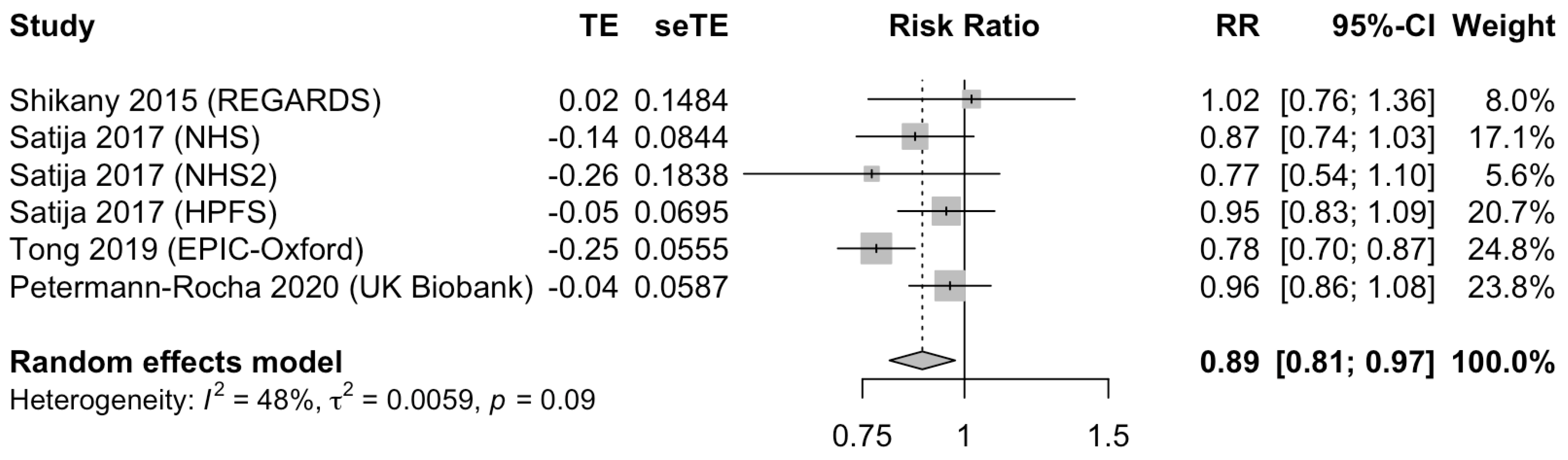
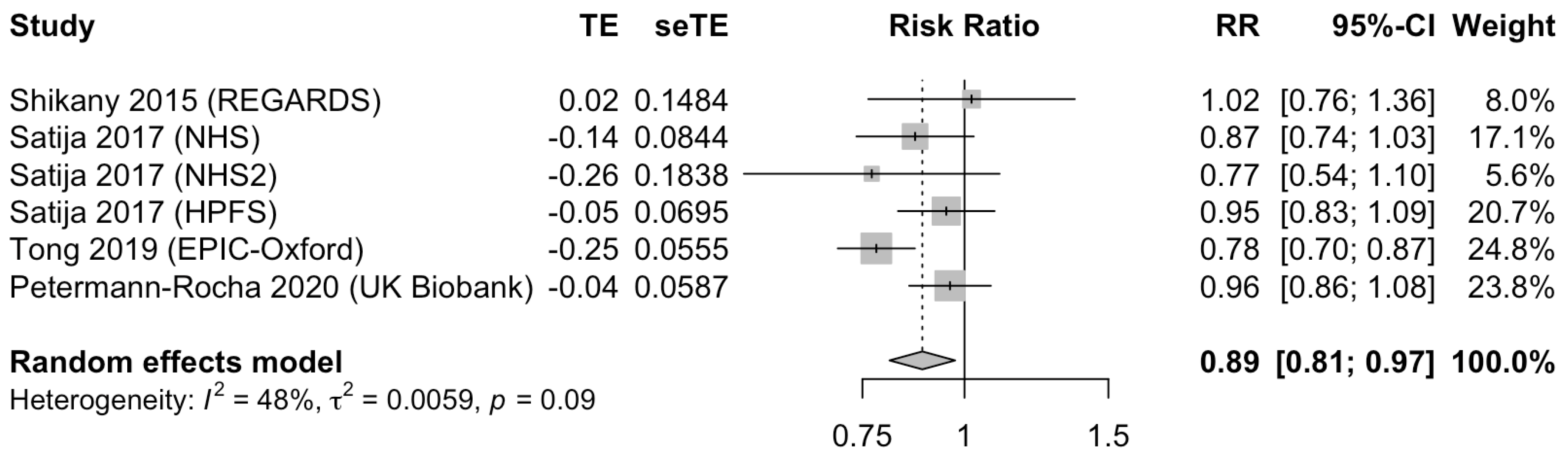
3.4. Plant-Based Dietary Pattern and Risk of Coronary Heart Disease
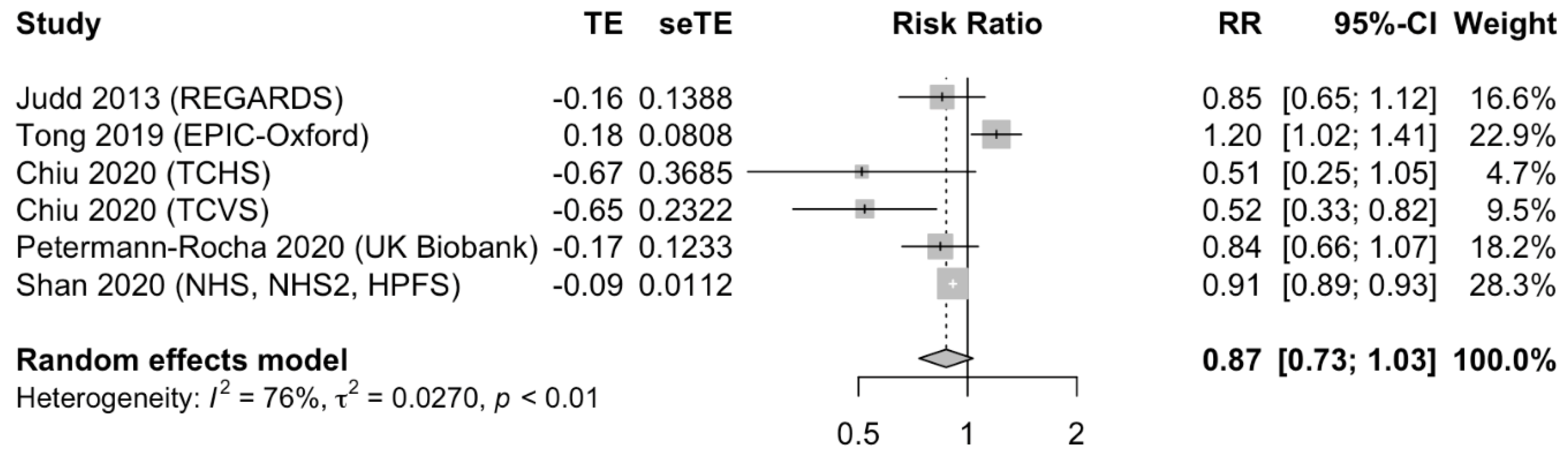
3.5. Plant-Based Dietary Pattern and Risk of Stroke
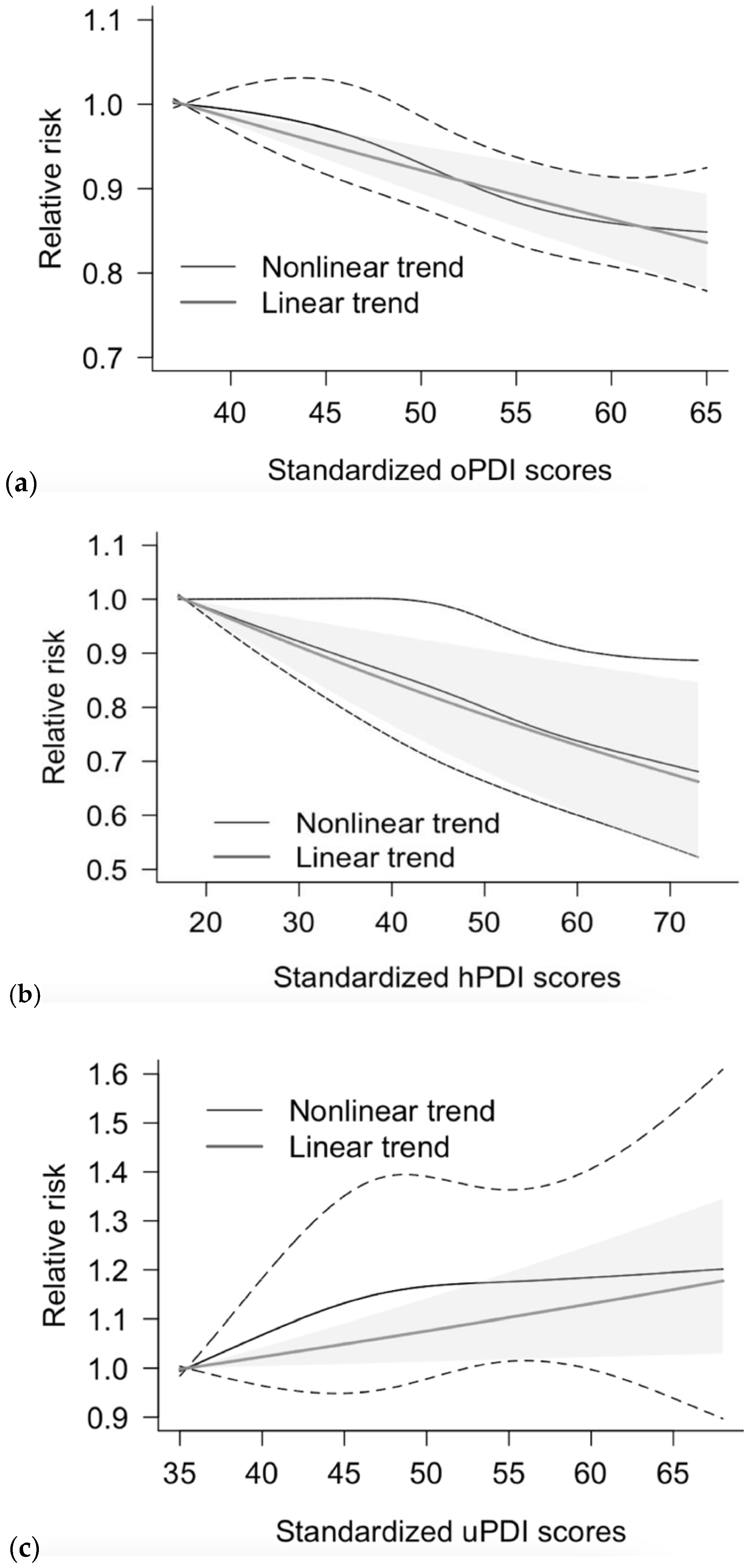
3.6. Dose-Response Meta-Analysis
3.7. Subgroup Analysis, Meta-Regression, and Assessment of Publication Bias
4. Discussion
4.1. Potential Mechanisms
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: Update from the GBD 2019 study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Storz, M.A. What makes a plant-based diet? A review of current concepts and proposal for a standardized plant-based dietary intervention checklist. Eur. J. Clin. Nutr. 2021, 1–12. [Google Scholar] [CrossRef]
- Libby, P.; Buring, J.E.; Badimon, L.; Hansson, G.K.; Deanfield, J.; Bittencourt, M.S.; Tokgözoğlu, L.; Lewis, E.F. Atherosclerosis. Nat. Rev. Dis. Primers 2019, 5, 1–18. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Nishimura, K.; Barnard, N.D.; Takegami, M.; Watanabe, M.; Sekikawa, A.; Okamura, T.; Miyamoto, Y. Vegetarian diets and blood pressure: A meta-analysis. JAMA Int. Med. 2014, 174, 577–587. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, Y.; Levin, S.M.; Barnard, N.D. Association between plant-based diets and plasma lipids: A systematic review and meta-analysis. Nutr. Rev. 2017, 75, 683–698. [Google Scholar] [CrossRef]
- Qian, F.; Liu, G.; Hu, F.B.; Bhupathiraju, S.N.; Sun, Q. Association between plant-based dietary patterns and risk of type 2 diabetes: A systematic review and meta-analysis. JAMA Int. Med. 2019, 179, 1335–1344. [Google Scholar] [CrossRef] [PubMed]
- Glenn, A.J.; Viguiliouk, E.; Seider, M.; Boucher, B.A.; Khan, T.; Mejia, S.B.; Jenkins, D.J.A.; Kahleová, H.; Rahelić, D.; Salas-Salvadó, J.; et al. Relation of Vegetarian Dietary Patterns with Major Cardiovascular Outcomes: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. Front. Nutr. 2019, 6, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinu, M.; Abbate, R.; Gensini, G.F.; Casini, A.; Sofi, F. Vegetarian, vegan diets and multiple health outcomes: A systematic review with meta-analysis of observational studies. Crit. Rev. Food Sci. Nutr. 2017, 57, 3640–3649. [Google Scholar] [CrossRef]
- A Martínez-González, M.; Sánchez-Tainta, A.; Corella, D.; Salas-Salvadó, J.; Ros, E.; Arós, F.; Gómez-Gracia, E.; Fiol, M.; Lamuela-Raventós, R.M.; Schröder, H.; et al. A provegetarian food pattern and reduction in total mortality in the Prevención con Dieta Mediterránea (PREDIMED) study. Am. J. Clin. Nutr. 2014, 100 (Suppl. S1), 320S–328S. [Google Scholar] [CrossRef] [Green Version]
- Satija, A.; Bhupathiraju, S.N.; Spiegelman, D.; Chiuve, S.; Manson, J.E.; Willett, W.; Rexrode, K.M.; Rimm, E.B.; Hu, F.B. Healthful and unhealthful plant-based diets and the risk of coronary heart disease in US adults. J. Am. Coll. Cardiol. 2017, 70, 411–422. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analysis. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 December 2020).
- Freeman, A.M.; Morris, P.B.; Barnard, N.; Esselstyn, C.B.; Ros, E.; Agatston, A.; Devries, S.; O’Keefe, J.; Miller, M.; Ornish, D.; et al. Trending cardiovascular nutrition controversies. J. Am. Coll. Cardiol. 2017, 69, 1172–1187. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Greenland, S.; Longnecker, M.P. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am. J. Epidemiol. 1992, 135, 1301–1309. [Google Scholar] [CrossRef]
- Crippa, A.; Orsini, N. Multivariate dose-response meta-analysis: The dosresmeta R package. J. Stat. Softw. 2016, 72, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Crowe, F.L.; Appleby, P.N.; Travis, R.C.; Key, T.J. Risk of hospitalization or death from ischemic heart disease among British vegetarians and nonvegetarians: Results from the EPIC-Oxford cohort study. Am. J. Clin. Nutr. 2013, 97, 597–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, T.Y.; Appleby, P.N.; Bradbury, K.E.; Perez-Cornago, A.; Travis, R.C.; Clarke, R.; Key, T.J. Risks of ischaemic heart disease and stroke in meat eaters, fish eaters, and vegetarians over 18 years of follow-up: Results from the prospective EPIC-Oxford study. BMJ 2019, 366, l4897. [Google Scholar] [CrossRef] [Green Version]
- Shan, Z.; Li, Y.; Baden, M.Y.; Bhupathiraju, S.N.; Wang, D.D.; Sun, Q.; Rexrode, K.M.; Rimm, E.B.; Qi, L.; Willett, W.C.; et al. Association between healthy eating patterns and risk of cardiovascular disease. JAMA Int. Med. 2020, 180, 1090–1100. [Google Scholar] [CrossRef]
- Heianza, Y.; Zhou, T.; Sun, D.; Hu, F.B.; Manson, J.E.; Qi, L. Genetic susceptibility, plant-based dietary patterns, and risk of cardiovascular disease. Am. J. Clin. Nutr. 2020, 112, 220–228. [Google Scholar] [CrossRef]
- Petermann-Rocha, F.; Parra-Soto, S.; Gray, S.; Anderson, J.; Welsh, P.; Gill, J.; Sattar, N.; Ho, F.K.; Celis-Morales, C.; Pell, J.P. Vegetarians, fish, poultry and meat-eaters: Who has higher risk of CVD incidence and mortality? A prospective study from UK Biobank. Eur. Heart J. 2020, 42, 1136–1143. [Google Scholar] [CrossRef] [PubMed]
- Judd, S.E.; Gutiérrez, O.M.; Newby, P.K.; Howard, G.; Howard, V.J.; Locher, J.L.; Kissela, B.M.; Shikany, J.M. Dietary patterns are associated with incident stroke and contribute to excess risk of stroke in black Americans. Stroke 2013, 44, 3305–3311. [Google Scholar] [CrossRef] [PubMed]
- Shikany, J.M.; Safford, M.M.; Newby, P.K.; Durant, R.W.; Brown, T.M.; Judd, S.E. Southern dietary pattern is associated with hazard of acute coronary heart disease in the Reasons for Geographic and Racial Differences in Stroke (REGARDS) Study. Circulation 2015, 132, 804–814. [Google Scholar] [CrossRef]
- Kim, H.; Caulfield, L.E.; Garcia-Larsen, V.; Steffen, L.M.; Coresh, J.; Rebholz, C.M. Plant-Based Diets Are Associated with a Lower Risk of Incident Cardiovascular Disease, Cardiovascular Disease Mortality, and All-Cause Mortality in a General Population of Middle-Aged Adults. J. Am. Heart Assoc. 2019, 8, e012865. [Google Scholar] [CrossRef]
- Chiu, T.H.; Chang, H.-R.; Wang, L.-Y.; Chang, C.-C.; Lin, M.-N.; Lin, C.-L. Vegetarian diet and incidence of total, ischemic, and hemorrhagic stroke in 2 cohorts in Taiwan. Neurology 2020, 94, e1112–e1121. [Google Scholar] [CrossRef] [Green Version]
- Rosato, V.; Temple, N.J.; La Vecchia, C.; Castellan, G.; Tavani, A.; Guercio, V. Mediterranean diet and cardiovascular disease: A systematic review and meta-analysis of observational studies. Eur. J. Nutr. 2019, 58, 173–191. [Google Scholar] [CrossRef]
- Chiavaroli, L.; Viguiliouk, E.; Nishi, S.K.; Mejia, S.B.; Rahelić, D.; Kahleova, H.; Salas-Salvadó, J.; Kendall, C.W.C.; Sievenpiper, J.L. DASH dietary pattern and cardiometabolic outcomes: An umbrella review of systematic reviews and meta-analyses. Nutrients 2019, 11, 338. [Google Scholar] [CrossRef] [Green Version]
- Van Horn, L.; Carson, J.A.; Appel, L.J.; Burke, L.E.; Economos, C.; Karmally, W.; Lancaster, K.; Lichtenstein, A.H.; Johnson, R.K.; Thomas, R.J.; et al. Recommended dietary pattern to achieve adherence to the American Heart Association/American College of Cardiology (AHA/ACC) guidelines: A scientific statement from the American Heart Association. Circulation 2016, 134, e505–e529. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.D.; Li, Y.; Chiuve, S.; Stampfer, M.J.; Manson, J.E.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Association of specific dietary fats with total and cause-specific mortality. JAMA Int. Med. 2016, 176, 1134–1145. [Google Scholar] [CrossRef]
- Bechthold, A.; Boeing, H.; Schwedhelm, C.; Hoffmann, G.; Knüppel, S.; Iqbal, K.; De Henauw, S.; Michels, N.; Devleesschauwer, B.; Schlesinger, S.; et al. Food groups and risk of coronary heart disease, stroke and heart failure: A systematic review and dose-response meta-analysis of prospective studies. Crit. Rev. Food Sci. Nutr. 2019, 59, 1071–1090. [Google Scholar] [CrossRef] [Green Version]
- Srour, B.; Fezeu, L.K.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Andrianasolo, R.M.; Chazelas, E.; Deschasaux, M.; Hercberg, S.; Galan, P.; et al. Ultra-processed food intake and risk of cardiovascular disease: Prospective cohort study (NutriNet-Santé). BMJ 2019, 365, l1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baden, M.Y.; Satija, A.; Hu, F.B.; Huang, T. Change in plant-based diet quality is associated with changes in plasma adiposity-associated biomarker concentrations in women. J. Nutr. 2019, 149, 676–686. [Google Scholar] [CrossRef]
- Key, T.J.; Fraser, G.E.; Thorogood, M.; Appleby, P.N.; Beral, V.; Reeves, G.; Burr, M.L.; Chang-Claude, J.; Frentzel-Beyme, R.; Kuzma, J.W.; et al. Mortality in vegetarians and nonvegetarians: Detailed findings from a collaborative analysis of 5 prospective studies. Am. J. Clin. Nutr. 1999, 70 (Suppl. 3), 516s–524s. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.-C.; Lee, C.-C.; Liu, S.-C.; Tseng, P.-J.; Chien, K.-L. Combined healthy lifestyle factors are more beneficial in reducing cardiovascular disease in younger adults: A meta-analysis of prospective cohort studies. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; on behalf of the China Kadoorie Biobank Collaborative Group; Clarke, R.; Bennett, D.; Guo, Y.; Walters, R.G.; Hill, M.; Parish, S.; Millwood, I.Y.; Bian, Z.; et al. Causal associations of blood lipids with risk of ischemic stroke and intracerebral hemorrhage in Chinese adults. Nat. Med. 2019, 25, 569–574. [Google Scholar] [CrossRef]
- O’Donnell, M.J.; Chin, S.L.; Rangarajan, S.; Xavier, D.; Liu, L.; Zhang, H.; Rao-Melacini, P.; Zhang, X.; Pais, P.; Agapay, S.; et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): A case-control study. Lancet 2016, 388, 761–775. [Google Scholar] [CrossRef]
- Barnard, N.D.; Levin, S.M.; Yokoyama, Y. A systematic review and meta-analysis of changes in body weight in clinical trials of vegetarian diets. J. Acad. Nutr. Diet. 2015, 115, 954–969. [Google Scholar] [CrossRef]
- Neuenschwander, M.; Ballon, A.; Weber, K.S.; Norat, T.; Aune, D.; Schwingshackl, L.; Schlesinger, S. Role of diet in type 2 diabetes incidence: Umbrella review of meta-analyses of prospective observational studies. BMJ 2019, 366, l2368. [Google Scholar] [CrossRef] [Green Version]
- Haghighatdoost, F.; Bellissimo, N.; de Zepetnek, J.O.T.; Rouhani, M.H. Association of vegetarian diet with inflammatory biomarkers: A systematic review and meta-analysis of observational studies. Public Health Nutr. 2017, 20, 2713–2721. [Google Scholar] [CrossRef]
- Hooper, L.; Martin, N.; Jimoh, O.F.; Kirk, C.; Foster, E.; Abdelhamid, A.S. Reduction in saturated fat intake for cardiovascular disease. Cochrane Database Syst. Rev. 2020, 8. [Google Scholar] [CrossRef]
- Chen, G.-C.; Lv, D.-B.; Pang, Z.; Liu, Q.-F. Red and processed meat consumption and risk of stroke: A meta-analysis of prospective cohort studies. Eur. J. Clin. Nutr. 2013, 67, 91–95. [Google Scholar] [CrossRef]
- Geiker, N.R.W.; Larsen, M.L.; Dyerberg, J.; Stender, S.; Astrup, A. Egg consumption, cardiovascular diseases and type 2 diabetes. Eur. J. Clin. Nutr. 2018, 72, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; An, P.; Wang, H.; Wang, X.; Shen, X.; Li, X.; Min, J.; Liu, S.; Wang, F. Dietary intake of heme iron and risk of cardiovascular disease: A dose–response meta-analysis of prospective cohort studies. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Klipfell, E.; Bennett, B.J.; Koeth, R.; Levison, B.S.; DuGar, B.; Feldstein, A.E.; Britt, E.B.; Fu, X.; Chung, Y.-M.; et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature 2011, 472, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiattarella, G.G.; Sannino, A.; Toscano, E.; Giugliano, G.; Gargiulo, G.; Franzone, A.; Trimarco, B.; Esposito, G.; Perrino, C. Gut microbe-generated metabolite trimethylamine-N-oxide as cardiovascular risk biomarker: A systematic review and dose-response meta-analysis. Eur. Heart J. 2017, 38, 2948–2956. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Country | Cohort | Sex | Mean Age, Years | Mean F/U, Years | n/N | Exposures | Dietary Assessment | Outcome | Outcome Ascertainment | Adjustments for Confounders |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Crowe 2013 [18] | UK | EPIC-Oxford | M/F | 44 | 11.6 | 1235/44,561 | Vegetarians vs. non-vegetarians | Questionnaire inquiring about meat and fish avoidance | CHD | Medical or death record | Sex, method of recruitment, region of residence, age, smoking, alcohol, physical activity, educational level, Townsend Deprivation Index, use of oral contraceptives or hormone therapy, and BMI |
| Judd 2013 [23] | USA | REGARDS | M/F | 64 | 5.7 | 490/28,151 | Plant-based dietary pattern adherence comparing extreme quartiles | Validated 110-item FFQ, plant-based dietary pattern derived from factor analysis | Stroke | Self-report and medical records confirmation | Age, race, region, sex, age-race, income, education, total energy, smoking, and sedentary behavior |
| Shikany 2015 [24] | USA | REGARDS | M/F | 64 | 5.8 | 536/17,418 | Plant-based dietary pattern adherence comparing extreme quartiles | Validated 110-item FFQ, plant-based dietary pattern derived from factor analysis | CHD | Self-report and medical records confirmation. | Age, sex, race, age–race interaction, education, household income, region, total energy intake, smoking, physical activity, body mass index, waist circumference, and history of hypertension, dyslipidemia, and diabetes mellitus. |
| Satija 2017 [10] | USA | NHS | F | 54 | 36 | 3233/73,710 | oPDI, hPDI, and uPDI, comparing extreme deciles | Validated 131-item FFQ, plant-based dietary indices from 18 food groups | CHD | Self-report and medical or death records confirmation | Age, smoking status, physical activity, alcohol intake, multivitamin use; aspirin use, family history of CHD, margarine intake, energy intake, baseline hypertension, hypercholesterolemia, and diabetes, and updated body mass index. Adjusted also for post-menopausal hormone use in NHS and NHS2, and for oral contraceptive use in NHS2 |
| NHS2 | F | 55 | 24 | 667/93,329 | |||||||
| HPFS | M | 53 | 26 | 4731/43,259 | |||||||
| Kim 2019 [25] | USA | ARIC | M/F | 54 | 25 | 4381/12,168 | oPDI, hPDI and uPDI, comparing extreme deciles | Validated 66-item FFQ, plant-based dietary indices from 17 food groups | CVD | Self-report and medical or death records confirmation. | Age, sex, race–center, total energy intake, education, smoking status, physical activity, alcohol consumption, and margarine consumption |
| Tong 2019 [19] | UK | EPIC-Oxford | M/F | 45 | 18.1 | 2820/48,188 | Vegetarians vs. meat eaters | Questionnaire inquiring about consumption of meat, fish, dairy products, and eggs | CHD Stroke | ICD-9 and ICD-10 codes by record linkage | Age, sex, method of recruitment, region, year of recruitment, education, Townsend deprivation index, smoking, alcohol consumption, physical activity, dietary supplement use, oral contraceptive, and hormone replacement therapy use in women |
| 1072/48,188 | |||||||||||
| Chiu 2020 [26] | Taiwan | TCHS | M/F | 52 | 10 | 54/5050 | Vegetarians vs. non-vegetarians | Questionnaire inquiring about meat and fish avoidance | Stroke | ICD-9 codes by record linkage | Sex, smoking, alcohol drinking, betel nut, leisure time, physical activities, education, hypertension, diabetes mellitus, dyslipidemia, ischemic heart disease, and body mass index |
| TCVS | M/F | 49 | 10 | 121/8302 | |||||||
| Heianza 2020 [21] | UK | UK Biobank | M/F | 56 | 5 | 1812/156,148 | hPDI comparing extreme quintiles | Web-based 24 h dietary assessment, plant-based dietary indices from 17 food groups | CVD CHD Stroke | ICD-9 and ICD-10 codes by record linkage | Age, sex, ethnicity, education, parental history of heart disease, smoking habit, physical activity, multivitamin use, total energy intake, alcohol consumption, Townsend Deprivation Index, BMI, hypertension, dyslipidemia, and type 2 diabetes |
| 1162/156,148 | |||||||||||
| 697/156,148 | |||||||||||
| Petermann-Rocha 2020 [22] | UK | UK Biobank | M/F | 56.48 | 8.5 | 106,690/398,448 | Vegetarians vs. meat-eaters | Questionnaire inquiring about consumption of dairy, fish, meat, and poultry | CVD CHD Stroke | ICD-10 codes by record linkage | Age, sex, deprivation, ethnicity, comorbidities, smoking, alcohol intake, total sedentary time, physical activity, and body mass index |
| 24,794/418,287 | |||||||||||
| 5946/422,102 | |||||||||||
| Shan 2020 [20] | USA | NHS, NHS2, HPFS | M/F | 53.2 | 32 | 23,366/209,133 | hPDI comparing extreme quintiles | Validated 131-item FFQ, plant-based dietary indices from 18 food groups | CVD CHD Stroke | Self-report and medical or death records confirmation | Age, race/ethnicity, body mass index, physical activity, smoking, status, alcohol intake, menopausal status, oral contraceptive use, marital status, alone or with others, family history of myocardial infarction, total energy intake, multivitamin use, and aspirin use |
| 18,092/209,133 | |||||||||||
| 5687/209,133 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gan, Z.H.; Cheong, H.C.; Tu, Y.-K.; Kuo, P.-H. Association between Plant-Based Dietary Patterns and Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. Nutrients 2021, 13, 3952. https://doi.org/10.3390/nu13113952
Gan ZH, Cheong HC, Tu Y-K, Kuo P-H. Association between Plant-Based Dietary Patterns and Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. Nutrients. 2021; 13(11):3952. https://doi.org/10.3390/nu13113952
Chicago/Turabian StyleGan, Zuo Hua, Huey Chiat Cheong, Yu-Kang Tu, and Po-Hsiu Kuo. 2021. "Association between Plant-Based Dietary Patterns and Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Prospective Cohort Studies" Nutrients 13, no. 11: 3952. https://doi.org/10.3390/nu13113952
APA StyleGan, Z. H., Cheong, H. C., Tu, Y.-K., & Kuo, P.-H. (2021). Association between Plant-Based Dietary Patterns and Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. Nutrients, 13(11), 3952. https://doi.org/10.3390/nu13113952