
Long-Term Evolution of Malnutrition and Loss of Muscle Strength after COVID-19: A Major and Neglected Component of Long COVID-19

 , and
, and
Abstract
:1. Introduction
2. Methods
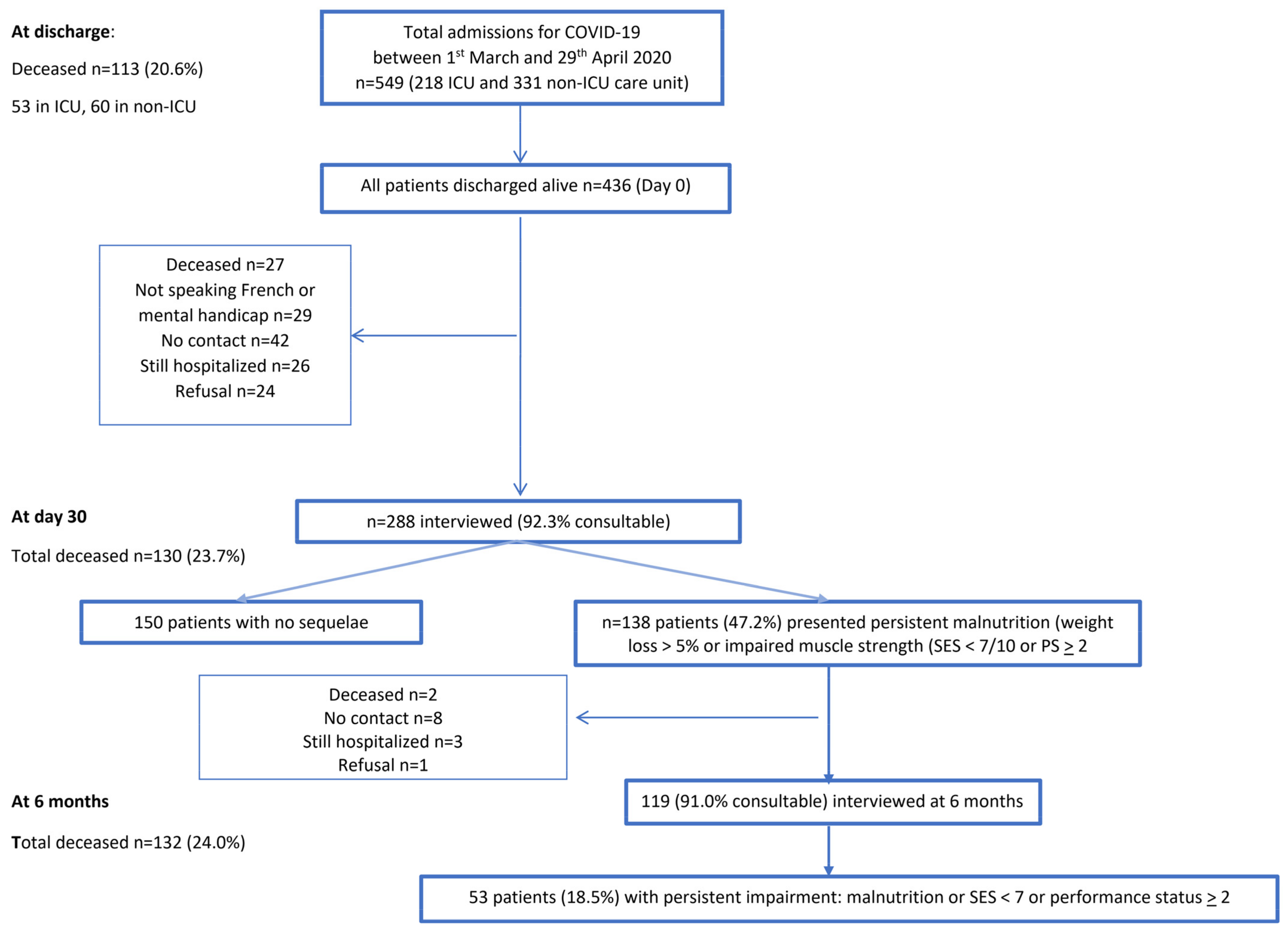
2.1. Study Design and Participants
2.2. Demographics, Comorbidities and Hospitalization Data Collection
2.3. Recorded Symptoms
2.4. Nutritional Assessment
2.5. SEFI and Self-Assessment of Muscle Function (SES) at Discharge, at Day 30 and at 6 Months Post-Discharge
2.6. Malnutrition Diagnosis
2.7. Statistical Analysis
3. Results
3.1. Long COVID Symptoms at 6 Months Post-Discharge
3.2. Characteristics of Patients with Impairment at 6 Months Post-Discharge, Comparison with Recovered Patients
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Venturelli, S.; Benatti, S.V.; Casati, M.; Binda, F.; Zuglian, G.; Imeri, G.; Conti, C.; Biffi, A.M.; Spada, M.S.; Bondi; et al. Surviving COVID-19 in Bergamo province: A post-acute outpatient re-evaluation. Epidemiol. Infect. 2021, 149, e32. [Google Scholar] [CrossRef] [PubMed]
- Abate, S.M.; Chekole, Y.A.; Estifanos, M.B.; Abate, K.H.; Kabthymer, R.H. Prevalence and outcomes of malnutrition among hospitalized COVID-19 patients: A systematic review and meta-analysis. Clin. Nutr. ESPEN 2021, 43, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Anker, M.S.; Landmesser, U.; von Haehling, S.; Butler, J.; Coats, A.J.S.; Anker, S.D. Weight loss, malnutrition, and cachexia in COVID-19: Facts and numbers. J. Cachexia Sarcopenia Muscle 2021, 12, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; Yang, Z.; Liu, J.; Liao, L.; Wang, F. Digestive system manifestations and clinical significance of coronavirus disease 2019: A systematic literature review. J. Gastroenterol. Hepatol. 2021, 36, 1414–1422. [Google Scholar] [CrossRef]
- Liu, R.; Paz, M.; Siraj, L.; Boyd, T.; Salamone, S.; Lite, T.V.; Leung, K.M.; Chirinos, J.D.; Shang, H.H.; Townsend, M.J.; et al. Feeding intolerance in critically ill patients with COVID-19. Clin. Nutr. 2021, 29, S261–S5614. [Google Scholar]
- Tong, J.Y.; Wong, A.; Zhu, D.; Fastenberg, J.H.; Tham, T. The Prevalence of Olfactory and Gustatory Dysfunction in COVID-19 Patients: A Systematic Review and Meta-analysis. Otolaryngol. Head Neck Surg. 2020, 163, 3–11. [Google Scholar] [CrossRef]
- Roos, D.S.; Oranje, O.J.M.; Freriksen, A.F.D.; Berendse, H.W.; Boesveldt, S. Flavor perception and the risk of malnutrition in patients with Parkinson’s disease. J. Neural Transm. 2018, 125, 925–930. [Google Scholar] [CrossRef] [Green Version]
- Li, T.; Zhang, Y.; Gong, C.; Wang, J.; Liu, B.; Shi, L.; Duan, J. Prevalence of malnutrition and analysis of related factors in elderly patients with COVID-19 in Wuhan, China. Eur. J. Clin. Nutr. 2020, 74, 871–875. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Chen, S.; Liu, M.; Nie, H.; Lu, H. Comorbid Chronic Diseases are Strongly Correlated with Disease Severity among COVID-19 Patients: A Systematic Review and Meta-Analysis. Aging Dis. 2020, 11, 668–678. [Google Scholar] [CrossRef]
- Piotrowicz, K.; Gasowski, J.; Michel, J.P.; Veronese, N. Post-COVID-19 acute sarcopenia: Physiopathology and management. Aging Clin. Exp. Res. 2021, 33, 2887–2898. [Google Scholar] [CrossRef]
- Wong, D.W.L.; Klinkhammer, B.M.; Djudjaj, S.; Villwock, S.; Timm, M.C.; Buhl, E.M.; Wucherpfennig, S.; Cacchi, C.; Braunschweig, T.; Knuchel-Clarke, R.; et al. Multisystemic Cellular Tropism of SARS-CoV-2 in Autopsies of COVID-19 Patients. Cells 2021, 10, 1900. [Google Scholar] [CrossRef]
- Msigwa, S.S.; Wang, Y.; Li, Y.; Cheng, X. The neurological insights of the emerging coronaviruses. J. Clin. Neurosci. 2020, 78, 1–7. [Google Scholar] [CrossRef]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [Green Version]
- Cereda, E.; Clave, P.; Collins, P.F.; Holdoway, A.; Wischmeyer, P.E. Recovery Focused Nutritional Therapy across the Continuum of Care: Learning from COVID-19. Nutrients 2021, 13, 3293. [Google Scholar] [CrossRef]
- Seessle, J.; Waterboer, T.; Hippchen, T.; Simon, J.; Kirchner, M.; Lim, A.; Muller, B.; Merle, U. Persistent symptoms in adult patients one year after COVID-19: A prospective cohort study. Clin. Infect. Dis. 2021, 5, ciab611. [Google Scholar]
- Adeloye, D.; Elneima, O.; Daines, L.; Poinasamy, K.; Quint, J.K.; Walker, S.; Brightling, C.E.; Siddiqui, S.; Hurst, J.R.; Chalmers, J.D.; et al. The long-term sequelae of COVID-19: An international consensus on research priorities for patients with pre-existing and new-onset airways disease. Lancet Respir. Med. 2021, 17, S2213-2600. [Google Scholar]
- Quilliot, D.; Gerard, M.; Bonsack, O.; Malgras, A.; Vaillant, M.F.; Di Patrizio, P.; Jaussaud, R.; Ziegler, O.; Nguyen-Thi, P.L. Impact of severe SARS-CoV-2 infection on nutritional status and subjective functional loss in a prospective cohort of COVID-19 survivors. BMJ Open 2021, 11, e048948. [Google Scholar] [CrossRef]
- Cheng, M.P.; Papenburg, J.; Desjardins, M.; Kanjilal, S.; Quach, C.; Libman, M.; Dittrich, S.; Yansouni, C.P. Diagnostic Testing for Severe Acute Respiratory Syndrome-Related Coronavirus 2: A Narrative Review. Ann. Intern. Med. 2020, 172, 726–734. [Google Scholar] [CrossRef] [Green Version]
- Hewlett, S.; Hehir, M.; Kirwan, J.R. Measuring fatigue in rheumatoid arthritis: A systematic review of scales in use. Arthritis Rheum. 2007, 57, 429–439. [Google Scholar] [CrossRef] [Green Version]
- Society, A.T. Recommended respiratory disease questionnaires for use with adults and children in epidemiologlcal research. Am. Rev. Respir. Dis. 1978, 118, 7–35. [Google Scholar]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- American Psychiatric Association: DSM-V Development. Available online: https://www.psychiatry.org/psychiatrists/practice/dsm/updates-to-dsm-5//updates-to-dsm-5-criteria-text (accessed on 20 July 2021).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; Arlington, V.A.P.A., Ed.; American Psychiatric Association: Washington, DC, USA, 2013; pp. 271–272. [Google Scholar]
- Thibault, R.; Goujon, N.; Le Gallic, E.; Clairand, R.; Sebille, V.; Vibert, J.; Schneider, S.M.; Darmaun, D. Use of 10-point analogue scales to estimate dietary intake: A prospective study in patients nutritionally at-risk. Clin. Nutr. 2009, 28, 134–140. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Cederholm, T.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef] [Green Version]
- HAS. Diagnostic de la Dénutrition de l’Enfant et de l’Adulte. Saint-Denis La Plaine. 2019. Available online: https://www.has-sante.fr/upload/docs/application/pdf/2019-11/reco277_recommandations_rbp_denutrition_cd_2019_11_13_v0.pdf (accessed on 20 July 2021).
- Thibault, R.; Quilliot, D.; Seguin, P.; Tamion, F.; Schneider, S.; Déchelotte, P. Nutritional care at hospital during the Covid-19 viral epidemic: Expert opinion from the French-speaking Society for Clinical Nutrition and Metabolism (SFNCM). Nut. Clin. Métab. 2020, 34, 97–104. [Google Scholar] [CrossRef]
- Fiorindi, C.; Campani, F.; Rasero, L.; Campani, C.; Livi, L.; Giovannoni, L.; Amato, C.; Giudici, F.; Bartoloni, A.; Fattirolli, F.; et al. Prevalence of nutritional risk and malnutrition during and after hospitalization for COVID-19 infection: Preliminary results of a single-centre experience. Clin. Nutr. ESPEN 2021, 45, 351–355. [Google Scholar] [CrossRef]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.M.; et al. Diagnostic criteria for malnutrition—An ESPEN Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef]
- Jeevanandam, M.; Young, D.H.; Schiller, W.R. Obesity and the metabolic response to severe multiple trauma in man. J. Clin. Invest. 1991, 87, 262–269. [Google Scholar] [CrossRef] [Green Version]
- Gualtieri, P.; Falcone, C.; Romano, L.; Macheda, S.; Correale, P.; Arciello, P.; Polimeni, N.; Lorenzo, A. Body Composition Findings by Computed Tomography in SARS-CoV-2 Patients: Increased Risk of Muscle Wasting in Obesity. Int. J. Mol. Sci. 2020, 21, 4670. [Google Scholar] [CrossRef]
- Zhang, X.; Xie, X.; Dou, Q.; Liu, C.; Zhang, W.; Yang, Y.; Deng, R.; Cheng, A.S.K. Association of sarcopenic obesity with the risk of all-cause mortality among adults over a broad range of different settings: A updated meta-analysis. BMC Geriatr. 2019, 19, 183. [Google Scholar] [CrossRef]
- Kurtz, A.; Grant, K.; Marano, R.; Arrieta, A.; Grant, K., Jr.; Feaster, W.; Steele, C.; Ehwerhemuepha, L. Long-term effects of malnutrition on severity of COVID-19. Sci. Rep. 2021, 11, 14974. [Google Scholar] [CrossRef] [PubMed]
- Caccialanza, R.; Formisano, E.; Klersy, C.; Ferretti, V.; Ferrari, A.; Demontis, S.; Mascheroni, A.; Masi, S.; Crotti, S.; Lobascio, F.; et al. Nutritional parameters associated with prognosis in non-critically ill hospitalized COVID-19 patients: The NUTRI-COVID19 study. Clin. Nutr. 2021, 25, S261–S5614. [Google Scholar]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Ousseiran, Z.H.; Fares, Y.; Chamoun, W.T. Neurological manifestations of COVID-19: A systematic review and detailed comprehension. Int. J. Neurosci. 2021, 27, 1–16. [Google Scholar] [CrossRef]
- Majolo, F.; Silva, G.L.D.; Vieira, L.; Anli, C.; Timmers, L.; Laufer, S.; Goettert, M.I. Neuropsychiatric Disorders and COVID-19: What We Know So Far. Pharmaceuticals 2021, 14, 933. [Google Scholar] [CrossRef]
- Bouette, G.; Esvan, M.; Apel, K.; Thibault, R. A visual analogue scale for food intake as a screening test for malnutrition in the primary care setting: Prospective non-interventional study. Clin. Nutr. 2020, 40, 174–180. [Google Scholar] [CrossRef]


{kind=link}
| Variables | n and % |
|---|---|
| Age (years) | 59.8 ± 16.6 |
| Sex (F/M) | 132/156 (45.8%/54.2%) |
| Living alone | 54 (18.8%) |
| Couple | 132 (45.8%) |
| Family | 96 (33.3%) |
| Retirement home | 6 (2.1%) |
| BMI Class | |
| 18.5–24.9 | 69 (24.3%) |
| 25–29.9 | 112 (39.4%) |
| >30 | 103 (36.3%) |
| IPAQ (prior to COVID-19) | |
| Low | 162 (56.3%) |
| Moderate | 82 (28.5%) |
| High | 44 (15.3%) |
| ICU | 102 (35.4%) |
| Active smoking | 12 (4.2%) |
| Daily alcohol | 14 (4.9%) |
| Comorbidities | |
| HBP | 113 (39.2%) |
| Coronary heart disease | 41 (14.2%) |
| Dyslipidemia | 64 (22.2%) |
| Diabetes mellitus | 48 (16.7%) |
| Renal failure | 23 (8.0%) |
| Stroke | 9 (3.1%) |
| Asthma | 14 (4.9%) |
| Apnea | 19 (6.6%) |
| Chronic obstructive bronchitis | 13 (4.5%) |
| Respiratory failure | 10 (3.5%) |
| Active cancer | 30 (10.4%) |
| Neurological disease | 13 (4.5%) |
| Admission (n = 119) | At Discharge (n = 119) | D30 Home (n = 119) | At 6 Months (n = 119) | p | |
|---|---|---|---|---|---|
| Weight (kg) | 82.6 ± 19.06 | 76.5 ± 16.1 | 77.6 ± 15.9 | 81.2 ± 17.9 | <10−3 |
| BMI | 28.7 ± 5.9 | 26.7 ± 5.0 | 27.4 ± 5.0 | 28.3 ± 5.5 | <10−3 |
| Weight variation (%) | −3.7 ± 4.9 | −5.1 ± 5.9 | −7.4 ± 5.0 | −3.6 ± 5.9 | <10−3 |
| Malnutrition | <10−3 | ||||
| No | 68/119 (57.1%) | 23/119 (19.3%) | 22/119 (18.5%) | 76/119 (63.9%) | |
| Moderate | 21/119 (17.6%) | 42/119 (35.3%) | 43/119 (36.1%) | 25/119 (21.0%) | |
| Severe | 12/119 (10.1%) | 54/119 (45.4%) | 54/119 (45.4%) | 18/119 (15.1%) | |
| SEFI | 7.2 ± 3.0 | 9.6 ± 1.2 | 9.8 ± 0.9 | <10−3 | |
| SES hands | 4.2 ± 2.4 | 6.9 ± 2.1 | 9.1 ± 1.7 | <10−3 | |
| SES legs | 4.0 ± 2.3 | 6.8 ± 2.1 | 9.1 ± 1.6 | <10−3 | |
| Subjective functional loss (SES < 7)% | 79.8% | 55.5% | 14.3% | <10−3 | |
| Asthenia (VAE)> 5/10 (%) | 3.2 ± 3.0 35/119 (29.4%) | 1.7 ± 2.5 19/119 (16.0%) | <10−3 0.020 | ||
| Performance Status | <10−3 | ||||
| 0 | 22 (18.5%) | 30 (25.2%) | 70/119 (58.8%) | ||
| 1 | 44 (37.0%) | 44 (37.0%) | 27/119 (22.7%) | ||
| 2 | 29 (24.4%) | 29 (24.4%) | 9/119 (7.6%) | ||
| 3–4 | 24 (20.2%) | 16 (13.4%) | 8/119 (6.7%) |
| Recovered Patients | Patients with Impairments at 6 Months | ||
|---|---|---|---|
| Variables | N = 217 (80.4%) | N = 53 (19.6%) | p |
| Symptoms at discharge | |||
| Dyspnea ≥ 2 | 21 (9.6%) | 3 (5.7%) | NS |
| Anosmia at discharge | 95 (43.8%) | 18 (34%) | NS |
| Diarrhea | 10 (4.6%) | 2 (3.8%) | NS |
| cough | 16 (7.4%) | 4 (7.5%) | NS |
| Obesity (BMI ≥ 30) (%) at admission | 31.0% | 52.8% | 0.007 |
| ICU admission | 31.3% | 50.9% | 0.010 |
| SEFI at discharge | 7.4 ± 2.9 | 6.1 ± 3.0 | 0.003 |
| Dietary aversion at discharge | 19 (8.8%) | 8 (15.1%) | NS |
| Weight loss (%) | |||
| Before admission | −2.8% ± 4.1% | −5.5 ± 7.0 | 0.001 |
| Total at discharge | −5.2% ± 4.7% | −10.5 ± 6% | <0.001 |
| Malnutrition at discharge (%) | 102 (49.3%) | 43 (82.6%) | 0.001 |
| Moderate | 62 (30.0%) | 15 (28.8%) | |
| Severe | 40 (19.3%) | 28 (53.8%) | |
| SES at discharge | |||
| Arms | 5.3 ± 2.6 | 4.3 ± 2.4 | 0.013 |
| Legs | 5.2 ± 2.7 | 4.0 ± 2.0 | 0.004 |
| SES < 7 | 138 (71.9%) | 46 (92%) | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gérard, M.; Mahmutovic, M.; Malgras, A.; Michot, N.; Scheyer, N.; Jaussaud, R.; Nguyen-Thi, P.-L.; Quilliot, D. Long-Term Evolution of Malnutrition and Loss of Muscle Strength after COVID-19: A Major and Neglected Component of Long COVID-19. Nutrients 2021, 13, 3964. https://doi.org/10.3390/nu13113964
Gérard M, Mahmutovic M, Malgras A, Michot N, Scheyer N, Jaussaud R, Nguyen-Thi P-L, Quilliot D. Long-Term Evolution of Malnutrition and Loss of Muscle Strength after COVID-19: A Major and Neglected Component of Long COVID-19. Nutrients. 2021; 13(11):3964. https://doi.org/10.3390/nu13113964
Chicago/Turabian StyleGérard, Marine, Meliha Mahmutovic, Aurélie Malgras, Niasha Michot, Nicolas Scheyer, Roland Jaussaud, Phi-Linh Nguyen-Thi, and Didier Quilliot. 2021. "Long-Term Evolution of Malnutrition and Loss of Muscle Strength after COVID-19: A Major and Neglected Component of Long COVID-19" Nutrients 13, no. 11: 3964. https://doi.org/10.3390/nu13113964
APA StyleGérard, M., Mahmutovic, M., Malgras, A., Michot, N., Scheyer, N., Jaussaud, R., Nguyen-Thi, P.-L., & Quilliot, D. (2021). Long-Term Evolution of Malnutrition and Loss of Muscle Strength after COVID-19: A Major and Neglected Component of Long COVID-19. Nutrients, 13(11), 3964. https://doi.org/10.3390/nu13113964