A Scoping Review of Policies Related to the Prevention and Control of Overweight and Obesity in Africa


Abstract
:1. Introduction
2. Materials and Methods
2.1. Stage 1: Identifying the Research Questions
2.2. Stage 2: Identification and Collection of Policy Documents
2.3. Stage 3: Screening and Selection of Policy Documents
2.4. Stage 4: Charting the Data
2.5. Stage 5: Collating, Summarising, and Reporting the Results
2.6. Ethics Consideration
3. Results
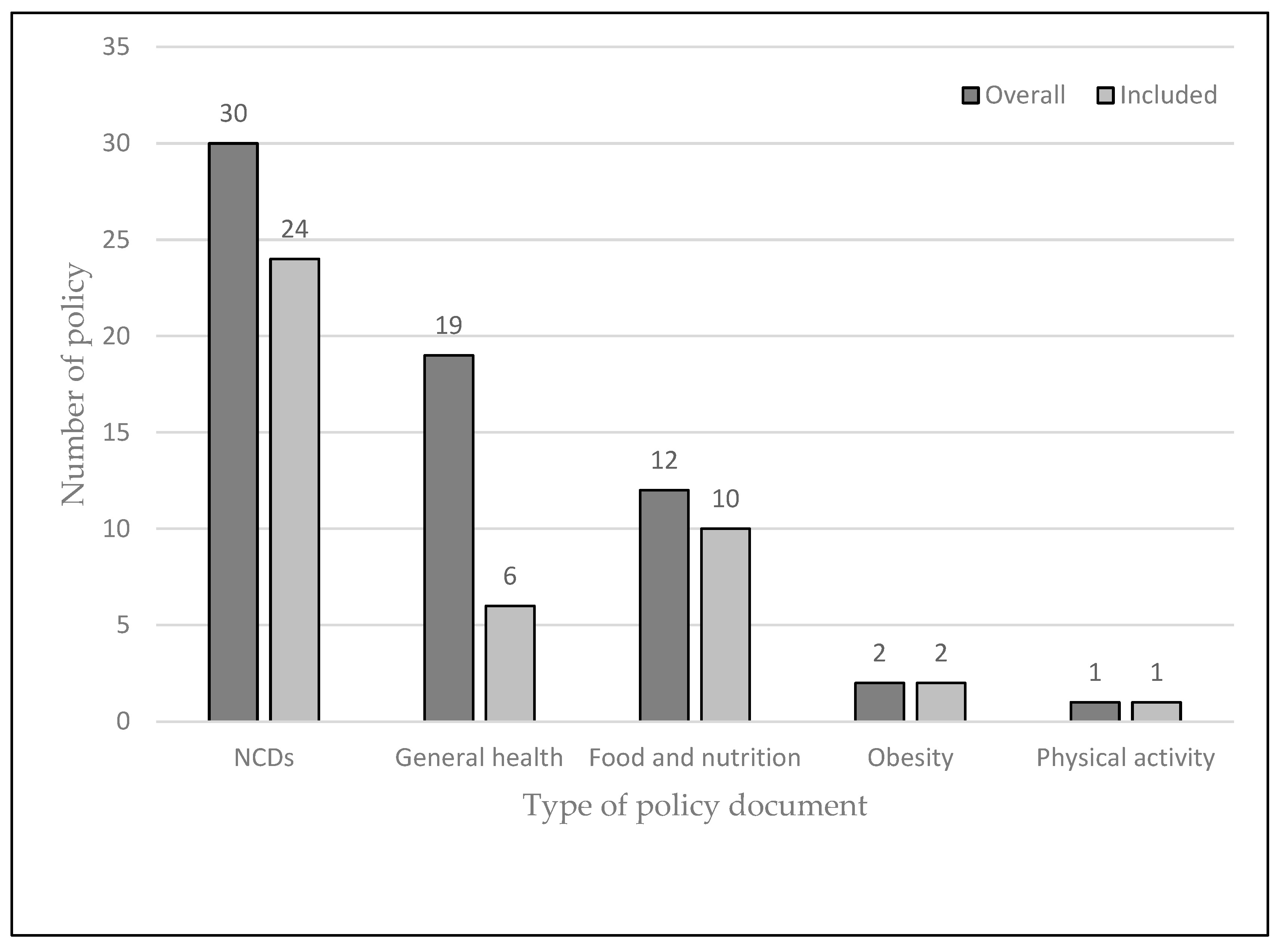
3.1. Description of Policy Documents
3.2. Key Policy Interventions at the Micro Scale (School, Family and Community)
3.2.1. Family
3.2.2. Community
3.3. Key Policy Interventions at the Macro-Scale
3.4. Policy Domains
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- WHO. WHO (2021)–Fact Sheet–Obesity and Overweight; WHO: Geneva, Switzerland, 2021.
- Kengne, A.P.; Bentham, J.; Zhou, B.; Peer, N.; Matsha, T.E.; Bixby, H.; Di Cesare, M.; Hajifathalian, K.; Lu, Y.; Taddei, C.; et al. Trends in obesity and diabetes across Africa from 1980 to 2014: An analysis of pooled population-based studies. Int. J. Epidemiol. 2017, 46, 1421–1432. [Google Scholar]
- Gona, P.N.; Kimokoti, R.W.; Gona, C.M.; Ballout, S.; Rao, S.R.; Mapoma, C.C.; Lo, J.; Mokdad, A.H. Changes in body mass index, obesity, and overweight in Southern Africa development countries, 1990 to 2019: Findings from the Global Burden of Disease, Injuries, and Risk Factors Study. Obes. Sci. Pract. 2021, 7, 509–524. [Google Scholar] [CrossRef]
- Newby, P.K. Are dietary intakes and eating behaviors related to childhood obesity? A comprehensive review of the evidence. J. Law. Med. Ethics 2007, 35, 35–60. [Google Scholar] [CrossRef]
- Hills, A.P.; Andersen, L.B.; Byrne, N.M. Physical activity and obesity in children. Br. J. Sports Med. 2011, 45, 866–870. [Google Scholar] [CrossRef] [Green Version]
- Kamath, C.C.; Vickers, K.S.; Ehrlich, A.; McGovern, L.; Johnson, J.; Singhal, V.; Paulo, R.; Hettinger, A.; Erwin, P.J.; Montori, V.M. Behavioral interventions to prevent childhood obesity: A systematic review and metaanalyses of randomized trials. J. Clin. Endocrinol. Metab. 2008, 93, 4606–4615. [Google Scholar] [CrossRef] [Green Version]
- Harris, K.C.; Kuramoto, L.K.; Schulzer, M.; Retallack, J.E. Effect of school-based physical activity interventions on body mass index in children: A meta-analysis. CMAJ 2009, 180, 719–726. [Google Scholar] [CrossRef] [Green Version]
- Dobbins, M.; Husson, H.; Decorby, K.; Rl, L. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst. Rev. 2013, CD007651. [Google Scholar] [CrossRef] [PubMed]
- Hooper, L.; Abdelhamid, A.; Moore, H.J.; Douthwaite, W.; Skeaff, C.M.; Summerbell, C.D. Effect of reducing total fat intake on body weight: Systematic review and meta-analysis of randomised controlled trials and cohort studies. BMJ 2012, 345, e7666. [Google Scholar] [CrossRef] [Green Version]
- Ledoux, T.A.; Hingle, M.D.; Baranowski, T. Relationship of fruit and vegetable intake with adiposity: A systematic review. Obes. Rev. 2011, 12, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Friel, S.; Chopra, M.; Satcher, D. Unequal weight: Equity oriented policy responses to the global obesity epidemic. BMJ 2007, 335, 1241–1243. [Google Scholar] [CrossRef] [Green Version]
- Thow, A.M.; Sanders, D.; Drury, E.; Puoane, T.; Chowdhury, S.N.; Tsolekile, L.; Negin, J. Regional trade and the nutrition transition: Opportunities to strengthen NCD prevention policy in the Southern African Development Community. Glob. Heal. Action 2015, 8, 28338. [Google Scholar] [CrossRef] [PubMed]
- Thow, A.M.; Jan, S.; Swinburn, B. The effect of fiscal policy on diet, obesity and chronic disease: A systematic review. Bull. World Health Organ. 2010, 88, 609–614. [Google Scholar] [CrossRef] [PubMed]
- Friel, S.; Hattersley, L.; Snowdon, W.; Thow, A.M.; Lobstein, T.; Sanders, D.; Barquera, S.; Mohan, S.; Hawkes, C.; Kelly, B.; et al. Monitoring the impacts of trade agreements on food environments. Obes. Rev. 2013, 14, 120–134. [Google Scholar] [CrossRef] [Green Version]
- WHO. Report of the Commission on Ending Childhood Obesity; WHO: Geneva, Switzerland, 2016.
- WHO. Global Strategy on Diet, Physical Activity and Health; WHO: Geneva, Switzerland, 2004; Volume 8, pp. 1–21.
- WHO. Action Plan for the Global Strategy for the Prevention and Control of Noncommunicable Diseases 2008–2013; WHO: Geneva, Switzerland, 2008; p. 35.
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Adom, T.; Puoane, T.; De Villiers, A.; Kengne, A.P. Protocol for a scoping review of existing policies on the prevention and control of obesity across countries in Africa. BMJ Open 2017, 7, e013541. [Google Scholar] [CrossRef]
- Swinburn, B.; Egger, G.; Raza, F. Dissecting Obesogenic Environments: The Development and Application of a Framework for Identifying and Prioritizing Environmental Interventions for Obesity 1. Prev. Med. (Baltim) 1999, 29, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Algeria. Plan Strategique National Multisectoriel de Lutte Integree Contre les Facteurs de Risque des Maladies Non Transmissibles 2015–2019; Ministere de la Sante, de la Population et de la Reforme Hospitaliere: El Madania, Algeria, 2015. [Google Scholar]
- Botswana. Botswana National Multisectoral Strategy for the Prevention and Control. of Non-Communicable Diseases; Ministry of Health and Wellness: Gaborone, Botswana, 2017.
- Benin. Plan Strategique Integre de Lutte Contre les Maladies Non Transmissibles 2014–2018; Ministère de la Santé: Porto-Novo, Benin, 2014.
- Burkina Faso. Plan Strategique Integre de Lutte Contre les Maladies Non Transmissibles Plan Strategique Integre de Lutte Contre les Maladies Non Transmissibles 2016–2020; Ministère de la Santé: Ouagadougou, Burkina Faso, 2016.
- Central African Republic. Document de Politique Nationale de Prevention et de Lutte Contre les Maladies Non Transmissibles; Ministere de la Sante Publique, des Affaires Sociale, de la Promotion du Genre et de L’action Humanitaire: Bangui, Central African Republic, 2014.
- Tchad. Plan Multisectoriel de Maladies Non Transmissibles 2017–2021; Ministère de la Santé: N’Djamena, Tchad, 2017.
- Des Comores, U. Document de Stratégie Nationale de Prévention et de Lutte Contre les Maladies Non Transmissibles; Ministere de Santé, de la Cohésion Ministère de la Santé, de la Solidarité, de la Cohésion Sociale et de la Promotion du Genre: Moroni, Comoros, 2013.
- Congo. Plan National Integré de Lutte Contre les Maladies Non Transmissibles au Congo 2013–2017; Ministere de la Sante et de la Population: Goma, Congo, 2013.
- Côte d’Ivoire. Plan Stratégique Intégré de Prévention et de Prise en Charge des Maladies Non Transmissibles en Côte d’Ivoire 2015–2019; Ministère de la Santé et de la Lutte contre le Sida: Yamoussoukro, Côte D’ivoire, 2014.
- Egypt; WHO. Egypt Multisectoral Action Plan for Noncommunicable Diseases Prevention and Control 2018–2022; Ministry of Health and Population: Cairo, Egypt, 2018.
- Ethiopia. Ethiopia_National Strategic Action Plan. (NSAP) for Prevention and Control of Non-Communicable Diseases-Final 2014–2016; Ministry of Health: Ababa, Ethiopia, 2014.
- Eritrea. Non-Communicable Diseases Policy; Ministry of Health: Asmara, Eritrea, 2008.
- Ghana. Strategy for the Management, Prevention and Control of Chronic Non-Communicable Diseases in Ghana; Ministry of Health: Accra, Ghana, 2016.
- Guinée. Programme National Intégré de Prévention et de Contrôle des Maladies Non Transmissibles; Ministère de la Santé et de l’hygiène Publique: Conakry, Guinée, 2010.
- Kenya. Kenya National Strategy for the Prevention and Control of Non-Communicable Diseases 2015–2020; Ministry of Health: Nairobi, Kenya, 2015.
- Lesotho. National Multi-Sectoral Integrated Strategic Plan for the Prevention and Control of Non-Communicable Diseases (NCDS): 2014–2020; Ministry of Health: Maseru, Lesotho, 2017.
- Madagascar. Politique Nationale de Prévention et Lutte Intégrées contre les Maladies Chroniques Non Transmissibles; World Health Organization (WHO): Geneva, Switzerland; Ministère de la Santé Publique: Antananarivo, Madagascar, 2013.
- Mali. Politique Nationale de Lutte Contre les Maladies Non Transmissibles; Ministère de la Santé: Bamako, Mali, 2013.
- Moçambique. Plano Estratégico Nacional de Prevenção e Controlo das Doenças não Transmissíveis para Período de 2008–2014; Ministry of Health National Directorate of Public Health Department of Non-Communicable Diseases: Maputo, Mozambique, 2008.
- Nigeria. National Policy and Strategic Plan of Action on Non-Communicable Diseases; Federal Ministry of Health: Abuja, Nigeria, 2013.
- Niger. Politique et Plan Strategique Integre de Lutte Contre les Maladies Non Transmissibles (Psimnt) 2012–2015; Ministère de la Santé Publique: Niamey, Niger, 2012.
- Rwanda. National Food and Nutrition Policy 2013–2018; Social Cluster Ministries: Kigali, Rwanda, 2013.
- Seychelles. Strategy for the Prevention and Control of Non-Communicable Diseases, 2016–2025; Ministry of Health: Victoria, Seychelles, 2016.
- Sierra Leone. National Non-Communicable Diseases Strategic Plan; Ministry of Health and Sanitation: Freetown, Sierra Leone, 2013.
- Swaziland. National Non Communicable Diseases Prevention and Control; Ministry of Health: Geneva, Swaziland; WHO: Geneva, Swaziland, 2016.
- Tanzania. Strategic Action Plan for Prevention and Control of Non communicable Diseases in Tanzania 2016–2020; Ministry of Health, Community Development, Gender, Elderly and Children: Dodoma, Tanzania, 2016.
- Togo. Politique et Plan Strategique Integre de Lutte Contre les Maladies Non Transmissibles (PSIMNT) 2012–2015; Ministere de la Sante: Lome, Togo, 2012.
- Zambia. Zambian Strategic Plan 2013–2016 Non-Communicable Diseases and Their Risk Factors Version 1; Ministry of Health: Lusaka, Zambia, 2016.
- Maroc. Stratégie Multisectorielle de Prévention et de Contrôle des Maladies Non Transmissibles 2016–2025; Ministre de la Santé, l’Organisation Mondiale de la Santé: Rabat, Maroc, 2016.
- Burundi. Plan Strategique Multisectoriel de Securite Alimentaire et Nutritionnelle (PSMSAN) 2014–2017; 2ève Vice-Presidence de la Republique: Gitega, Burundi, 2014.
- Angola. Plano Nacional de Desenvolvimento Sanitário 2012–2025 (PNDS); Ministério da Saúde: Luanda, Angola, 2014; Volume 1.
- Burundi. National Health Development Plan; Ministry of Public Health and Fighting AIDS: Gitega, Burundi, 2015; Volume 151.
- Cameroun. Plan National de Développement Sanitaire, PNDS 2016–2020; Ministere de Santé, de la Cohésion Ministère de la Santé Publique: Yaounde, Cameroun, 2016.
- Cabo Verde. Plano Nacional de Desenvolvimento Sanitário 2012–2016; Ministério da Saúde: Praia, Cabo Verde, 2012.
- Djibouti. Plan National de Developpment 2013–2015; Ministere de la Sante: Djibouti-Ville, Djibouti, 2013.
- Gambia. The Gambia National Health Sector Strategic Plan; Ministry of Health and Social Welfare: Banjul, Gambia, 2014.
- Malawi. Health Sector Strategic Plan. II (2017–2022); Ministry of Health: Lilongwe, Malawi, 2017.
- Mauritanie. Plan National de Developpement Sanitaire 2012–2020; Ministere de Santé: Nouakchott, Mauritanie, 2012.
- East Africa. Mauritius Draft Health Sector Strategy 2017–2021; Ministry of Health and Quality of Life: Port Louis, Mauritius, 2017.
- Namibia. Namibian National Health Policy Framework; Ministry of Health and Social National Services: Windhoek, Namibia, 2010.
- São Tomé et Príncipe. Plano Nacional do Desenvolvimento da Saúde 2017–2021; Ministério da Saúde: São Tomé, São Tomé et Príncipe, 2017.
- Senegal. Plan National de Developpement Sanitaire PNDS 2009–2018; Ministere de la Sante et de la Prevention: Dakar, Senegal, 2009; pp. 1–86.
- Somali. Health Sector Strategic Plan January 2013–December 2016; Ministry of Human Development and Public Services: Hargeysa, Somali, 2013.
- Sudan. 25 Years Strategic Plan for Health Sector; Ministry of Health: Khartoum, Sudan, 2003.
- Uganda. Health Sector Development Plan 2015/16–2019/20; Ministry of Health: Kampala, Uganda, 2015.
- Zimbabwe. The National Health Strategy for Zimbabwe 2016–2020; Ministry of Health and Child Care: Harare, Zimbabwe, 2016.
- South Sudan. The Republic of South Sudan Policy Framework 2013–2016; Ministry of Health: Juba, South Sudan, 2013.
- Somaliland. Somaliland National Health Policy; Ministry of Health: Hargeisa, Somaliland, 2011; pp. 1–48.
- Democratic Republic of the Congo. Plan National de Developpement Sanitaire 2016–2020; Ministere de la Sante Publique: Goma, Democratic Republic of the Congo, 2016.
- Mauritius. Plan of Action for Nutrition 2009–2010; Ministry of Health and Quality of Life: Port Louis, Mauritius, 2009.
- Sierra Leone. National Food and Nutrition Security Policy 2012–2016; Ministry of Health and Sanitation: Freetown, Sierra Leone, 2012.
- Namibia. Strategic Plan for Nutrition 2011–2015; Ministry of Health and Social Services: Windhoek, Namibia, 2014.
- Uganda. Nutrition Action Plan 2011–2016; Government of Uganda: Kampala, Uganda, 2011.
- Guinee-Bissau. Politique Nationale de Nutrition 2015–2019; Ministère de la Santé Publique: Bissau, Guinee-Bissau, 2014.
- Gabon. Politique Nationale de Securite Alimentaire et Nutritionnelle (PNSAN) 2017–2025; Ministère de l’Agriculture, de l’elevage, Chargé de la Mise en œuvre du Programme Graine: Libreville, Gabon, 2017.
- Burkina Faso. National Nutrition Policy (Politique Nationale de Nutrition); Ministère de la Santé: Ouagadougou, Burkina Faso, 2016.
- Cameroun. Politique Nationale de Nutrition 2012–2021; Ministère de la Santé Publique: Yaounde, Cameroun, 2006.
- Liberia. National Food Security and Nutrition Strategy Government of Liberia; Ministry of Agriculture: Monrovia, Liberia, 2008.
- Republique de Madagascar. Plan National d’Action Pour la Nutrition (PNAN III 2017–2021); Ministere de Sante: Antananarivo, Madagascar, 2017.
- Malawi. National Multi-Sector Nutrition Policy 2018–2022; Department of Nutrition HIV and AIDS: Lilongwe, Malawi, 2018.
- Tunisia. Stratégie de Prévention et de lutte Contre L’obésité 2013–2017; Ministère de la Santé: Tunis, Tunisia, 2014.
- South Africa. Strategy for the Prevention and Control of Obesity; Department of Health: Pretoria, South Africa, 2015.
- Mauritius. National Action Plan on Physical Activity 2011–2014; Ministry of Health and Quality of Life: Port Louis, Mauritius, 2011.
- Liberia. National Policy and Strategic Plan on Health Promotion; Ministry of Health: Monrovia, Liberia; WHO: Geneva, Switzerland, 2016.
- Lachat, C.; Otchere, S.; Roberfroid, D.; Abdulai, A.; Maria, F.; Seret, A.; Milesevic, J.; Xuereb, G.; Candeias, V.; Kolsteren, P. Diet and Physical Activity for the Prevention of Noncommunicable Diseases in Low- and Middle-Income Countries: A Systematic Policy Review. PLoS Med. 2013, 10, e1001465. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Escamilla, R.; Lutter, C.; Rabadan-Diehl, C.; Rubinstein, A.; Calvillo, A.; Corvalán, C. Prevention of childhood obesity and food policies in Latin America: From research to practice. Obes. Rev. 2017, 18, 28–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Margetts, B. Editorial. Public Health Nutr. 2004, 7, 361–363. [Google Scholar] [CrossRef]
- Thow, A.M.; Downs, S.; Jan, S. A systematic review of the effectiveness of food taxes and subsidies to improve diets: Understanding the recent evidence. Nutr. Rev. 2014, 72, 551–565. [Google Scholar] [CrossRef]
- Escobar, M.A.C.; Veerman, J.L.; Tollman, S.M.; Bertram, M.Y.; Hofman, K.J. Evidence that a tax on sugar sweetened beverages reduces the obesity rate: A meta-analysis. BMC Public Health 2013, 13, 1–10. [Google Scholar]
- Stacey, N.; Mudara, C.; Ng, S.W.; van Walbeek, C.; Hofman, K.; Edoka, I. Sugar-based beverage taxes and beverage prices: Evidence from South Africa’s Health Promotion Levy. Soc. Sci. Med. 2019, 238, 112465. [Google Scholar] [CrossRef]
- Stacey, N.; Edoka, I.; Hofman, K.; Swart, E.C.; Popkin, B.; Ng, S.W. Changes in beverage purchases following the announcement and implementation of South Africa’s Health Promotion Levy: An observational study. Lancet Planet. Health 2021, 5, e200–e208. [Google Scholar] [CrossRef]
- Miller, S.L.M.; Cassady, D.L.; Applegate, E.A.; Beckett, L.A.; Wilson, M.D.; Gibson, T.N.; Ellwood, K. Relationships among Food Label Use, Motivation, and Dietary Quality. Nutrients 2015, 7, 1068–1080. [Google Scholar] [CrossRef] [Green Version]
- Cecchini, M.; Warin, L. Impact of food labelling systems on food choices and eating behaviours: A systematic review and meta-analysis of randomized studies. Obes. Rev. 2016, 17, 201. [Google Scholar] [CrossRef]
- Sadeghirad, B.; Duhaney, T.; Motaghipisheh, S.; Campbell, N.R.C.; Johnston, B.C. Influence of unhealthy food and beverage marketing on children’s dietary intake and preference: A systematic review and meta-analysis of randomized trials. Obes. Rev. 2016, 17, 945–959. [Google Scholar] [CrossRef]
- Boyland, E.J.; Nolan, S.; Kelly, B.; Tudur-Smith, C.; Jones, A.; Halford, J.C.G.; Robinson, E. Advertising as a cue to consume: A systematic review and meta-analysis of the effects of acute exposure to unhealthy food and nonalcoholic beverage advertising on intake in children and adults. Am. J. Clin. Nutr. 2016, 103, 519–533. [Google Scholar] [CrossRef] [PubMed]
- Mansfield, J.L.; Savaiano, D.A. Effect of school wellness policies and the Healthy, Hunger-Free Kids Act on food-consumption behaviors of students, 2006–2016: A systematic review. Nutr. Rev. 2017, 75, 533–552. [Google Scholar] [CrossRef] [PubMed]
- Micha, R.; Karageorgou, D.; Bakogianni, I.; Trichia, E.; Whitsel, L.P.; Story, M.; Peñalvo, J.L.; Mozaffarian, D. Effectiveness of school food environment policies on children’s dietary behaviors: A systematic review and meta-analysis. PLoS ONE 2018, 13, 1–27. [Google Scholar] [CrossRef]
- Littlewood, J.A.; Lourenço, S.; Iversen, C.L.; Hansen, G.L. Menu labelling is effective in reducing energy ordered and consumed: A systematic review and meta-analysis of recent studies. Public Health Nutr. 2016, 19, 2106–2121. [Google Scholar] [CrossRef] [PubMed]
- Heath, G.W.; Parra, D.C.; Sarmiento, O.L.; Andersen, L.B.; Owen, N.; Goenka, S.; Montes, F.; Brownson, R.C.; Alkandari, J.R.; Bauman, A.E.; et al. Evidence-based intervention in physical activity: Lessons from around the world. Lancet 2012, 380, 272–281. [Google Scholar] [CrossRef] [Green Version]
- Helvaci, N.; Eyupoglu, N.D.; Karabulut, E.; Yildiz, B.O. Prevalence of Obesity and Its Impact on Outcome in Patients With COVID-19: A Systematic Review and Meta-Analysis. Front. Endocrinol. (Lausanne) 2021, 12, 598249. [Google Scholar] [CrossRef] [PubMed]
- Juma, P.A.; Mohamed, S.F.; Mwagomba, B.L.M.; Ndinda, C.; Mapa-tassou, C.; Oluwasanu, M.; Oladepo, O.; Abiona, O.; Nkhata, M.J.; Wisdom, J.P.; et al. Non-communicable disease prevention policy process in five African countries. BMC Public Health 2018, 18, 961. [Google Scholar]
- Nyaaba, G.N.; Stronks, K.; Aikins, A.D.-G.; Kengne, A.P.; Agyemang, C. Tracing Africa’s progress towards implementing the Non-Communicable Diseases Global action plan 2013–2020: A synthesis of WHO country profile reports. BMC Public Health 2017, 17, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Macro-Environment, Diet-Related and Physical Activity-Related (National, Regional, Sectors, Food Industries, Media, etc.) | Micro-Environment, Diet-Related and Physical Activity (Homes, Schools, Community Groups, Food Retailers, etc.) | |
|---|---|---|
| Physical | What is available? Example: facilities, built environment, training opportunities, nutrition and exercise expertise, information. | |
| Economic | What are the monetary cost/factor influences and consequences? Example: taxes and subsidies. | |
| Legislative | What are the statutory provisions, rules and legal guidance, policy messages? | |
| Socio-cultural | What are the attitudes, beliefs, perceptions, and values? | |
| Policy intervention | Environment | Country | |
|---|---|---|---|
| Micro-scale | |||
| School | |||
| Nutrition and diet-related | Provision of healthy school meals (provision of, and access to like fruits and vegetables) | Physical/ Legislative | Algeria, Benin, Botswana, Chad, Egypt, Gabon, Ghana, Guinea-Bissau, Kenya, Liberia, Mauritius, Morocco, Mozambique, Seychelles, South Africa, Tanzania, Tunisia, Zambia |
| Promotion of school vegetable gardens | Legislative | Algeria, Burkina Faso, Gabon, Guinea-Bissau, Rwanda, Tunisia. | |
| Restricting marketing of unhealthy foods and beverages | Legislative | Algeria, Ghana, Mauritius, South Africa, Tunisia | |
| Food supply near schools (limits on refined sugars, fats, and salt | Legislative | Algeria, South Africa | |
| Strengthen nutrition education | Legislative/Sociocultural | Algeria, Angola, Botswana, Burkina Faso, Cameroon, Egypt, Gabon, Gambia, Ghana, Guinea-Bissau, Guinea, Kenya, Liberia, Madagascar, Mauritius, Morocco, Rwanda, Seychelles, Sierra Leone, South Africa, Tanzania, Tunisia | |
| Professional development for teachers and school canteen staff, etc. | Physical/ Sociocultural | Algeria, Burkina Faso, Guinea-Bissau, Tanzania | |
| Monitoring of BMI | Legislative | Algeria, Botswana, Zambia | |
| Physical activity | Mandatory/strengthen physical education and activity in the curriculum | Legislative/Sociocultural | Algeria, Angola, Botswana, Chad, Egypt, Ghana, Guinea-Bissau, Kenya, Lesotho, Liberia, Madagascar, Mauritius, Morocco, Sierra Leone, Seychelles, South Africa, Togo, Tunisia, Zambia |
| After-school physical activity programmes | Physical/ Legislative | Mauritius, Seychelles | |
| Provision of, and access to adequate recreational facilities | Physical | Angola, Algeria, Benin, Botswana, Chad, Egypt, Ethiopia, Mauritius, Nigeria, Seychelles, South Africa, Tanzania, Tunisia | |
| Promote and support active transport | Physical/ Legislative | Algeria, Ethiopia, Mauritius, Seychelles, South Africa | |
| Professional development/trained instructors for school staff including PE teachers and school doctors | Physical/ Sociocultural | Algeria, Liberia, Mauritius | |
| Family | Educational materials/programmes/sensitisation to promote healthy lifestyles | Physical/ Sociocultural | Algeria, Burkina Faso, Ghana, Guinea-Bissau, Liberia, Tunisia |
| Promotion of breastfeeding | Physical/ Legislative/Sociocultural | Algeria, Botswana, Cameroon, Chad, Egypt, Gabon, Gambia, Guinea-Bissau, Kenya, Liberia, Malawi, Mauritania, Mauritius, Morocco, Namibia, Nigeria, Rwanda, Seychelles, South Africa, Togo, Zambia, Zimbabwe | |
| Promotion of vegetable gardens | Physical/ Sociocultural | Lesotho, Mauritius, South Africa | |
| Community | Provision of, and access to adequate recreational facilities | Physical/Legislative | Algeria, Benin, Cameroon, Cote d’Ivoire, Gambia, Ghana, Guinea, Madagascar, Mauritius, Nigeria, Sierra Leone, South Africa, Togo, Tunisia, Zambia |
| Provision of, and access to safe walking paths, cycling lanes, public transport, etc. | Physical/ Legislative | Angola, Algeria, Botswana, Congo, Chad, Egypt, Ghana, Madagascar, Mauritius, Morocco, Nigeria, Seychelles, Sierra Leone, South Africa, Togo, Zambia | |
| Physical activity clubs/organisation of games and sports | Sociocultural | Algeria, Botswana, Egypt, Chad, Ghana, Guinea-Bissau, Mauritius, South Africa, Togo, Tunisia | |
| Health promotion/awareness campaigns of healthy lifestyles (healthy foods/physical activity) | Legislative/ Sociocultural | Angola, Algeria, Benin, Burkina Faso, Cote d’Ivoire, Chad, Central African Republic, Egypt, Ethiopia, Gabon, Gambia, Ghana, Guinea-Bissau, Guinea, Kenya, Lesotho, Liberia, Madagascar, Malawi, Mauritania, Mauritius, Morocco, Namibia, Niger, Nigeria, Seychelles, Sierra Leone, South Africa, Swaziland, Tanzania, Togo, Zambia, Zimbabwe | |
| Financial incentives for healthy lifestyle (rewards for active transport) | Economic | Botswana, Ghana, Tunisia, | |
| Production, provision of, and access to healthy foods like fruits and vegetables | Physical/ Sociocultural/ Legislative | Benin, Chad, Congo, Cote d’Ivoire, Ethiopia, Guinea-Bissau, Guinea, Liberia, Madagascar, Mauritius, Seychelles, South Africa, Togo | |
| Role models for physical activity | Sociocultural | Ghana, Mauritius, South Africa, Tunisia | |
| Macro-scale | |||
| Health promotion/awareness campaigns of healthy lifestyles (healthy foods/physical activity) | Legislative/ Sociocultural | Angola, Algeria, Benin, Burkina Faso, Cote d’Ivoire, Chad, Central African Republic, Egypt, Ethiopia, Gabon, Gambia, Ghana, Guinea-Bissau, Guinea, Kenya, Lesotho, Liberia, Madagascar, Malawi, Mauritania, Mauritius, Morocco, Namibia, Niger, Nigeria, Seychelles, Sierra Leone, South Africa, Swaziland, Tanzania, Togo, Zambia, Zimbabwe | |
| Educational material/training relevant stakeholders for healthy lifestyles e.g., consumers, food manufacturers, NGO, etc. | Physical/ Sociocultural | Algeria, Cameroon, Chad, Egypt, Gabon, Ghana, Mauritius, Morocco, Seychelles, South Africa, Tunisia | |
| Financial incentives for healthy lifestyle (e.g., subsidies on sports equipment and bicycles | Economic | Botswana, Ghana, Tunisia | |
| National physical activity guidelines/plans | Legislative | Cote d’Ivoire, Egypt, Ethiopia, Ghana, Mauritius, Nigeria, Seychelles, South Africa, Zambia | |
| Provision of, and access to adequate recreational facilities | Physical/Legislative | Benin, Chad, Congo, Cote d’Ivoire, Ethiopia, Guinea-Bissau, Guinea, Liberia, Madagascar, Mauritius, Seychelles, South Africa, Togo | |
| Food taxes and subsidies to promote healthier diets | Economic | Botswana, Chad, Egypt, Ethiopia, Ghana, Guinea, Kenya, Lesotho, Liberia, Mauritius, Morocco, Seychelles, South Africa | |
| Marketing of unhealthy foods and beverages especially to children | Legislative | Algeria, Botswana, Egypt, Ghana, Guinea-Bissau, Kenya, Mauritius, Morocco, Nigeria, Seychelles, South Africa | |
| Food and nutrition labelling | Sociocultural/ Legislative | Algeria, Egypt, Ethiopia, Ghana, Kenya, Mauritius, Morocco, Namibia, Nigeria, Seychelles, South Africa, Tunisia, Zambia | |
| Production, provision of, and access to healthy foods like fruits and vegetables | Physical/ Sociocultural/ Legislative | Benin, Chad, Congo, Cote d’Ivoire, Ethiopia, Guinea-Bissau, Guinea, Liberia, Madagascar, Mauritius, Seychelles, South Africa, Togo | |
| Regulation of sugars, fats, and salt in processed foods | Legislative/ Sociocultural | Benin, Botswana, Congo, Cote d’Ivoire, Chad, Egypt, Ghana, Kenya, Madagascar, Morocco, Nigeria, Seychelles, South Africa, Zambia |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adom, T.; De Villiers, A.; Puoane, T.; Kengne, A.P. A Scoping Review of Policies Related to the Prevention and Control of Overweight and Obesity in Africa. Nutrients 2021, 13, 4028. https://doi.org/10.3390/nu13114028
Adom T, De Villiers A, Puoane T, Kengne AP. A Scoping Review of Policies Related to the Prevention and Control of Overweight and Obesity in Africa. Nutrients. 2021; 13(11):4028. https://doi.org/10.3390/nu13114028
Chicago/Turabian StyleAdom, Theodosia, Anniza De Villiers, Thandi Puoane, and André Pascal Kengne. 2021. "A Scoping Review of Policies Related to the Prevention and Control of Overweight and Obesity in Africa" Nutrients 13, no. 11: 4028. https://doi.org/10.3390/nu13114028
APA StyleAdom, T., De Villiers, A., Puoane, T., & Kengne, A. P. (2021). A Scoping Review of Policies Related to the Prevention and Control of Overweight and Obesity in Africa. Nutrients, 13(11), 4028. https://doi.org/10.3390/nu13114028