
Risk of Developing Metabolic Syndrome Is Affected by Length of Daily Siesta: Results from a Prospective Cohort Study

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Ethics
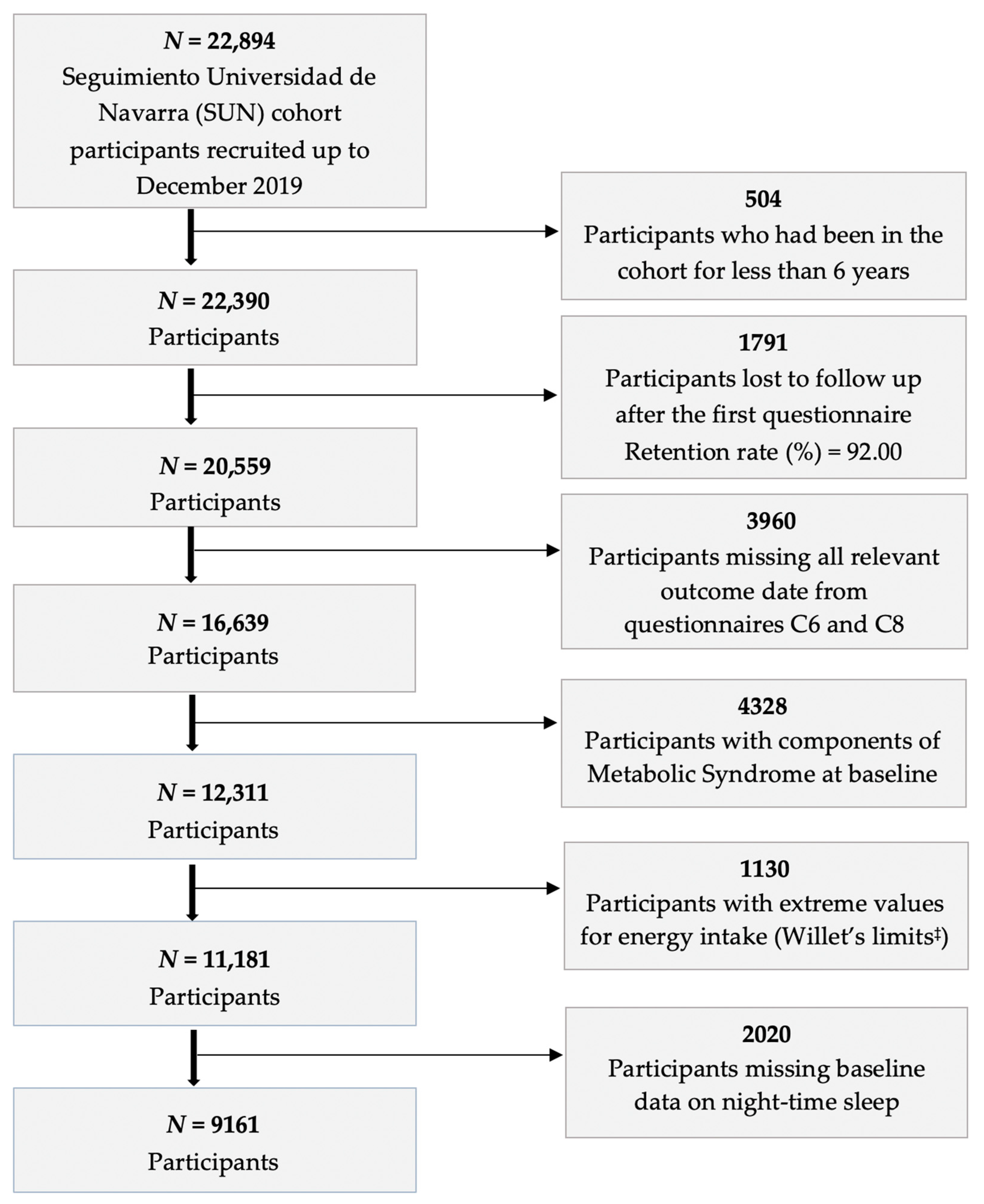
2.3. Study Sample
- -
- They did not have outcome data for any component of metabolic syndrome;
- -
- They met criteria for any component of metabolic syndrome at baseline;
- -
- Their baseline questionnaire responses did not meet minimum quality standards, as assessed by whether their Food Frequency Questionnaire yielded realistic values for energy intake [37];
- -
- They did not have baseline data about how long they slept at night.
2.4. Exposure Assessment
2.5. Outcome Assessment
2.6. Covariables
2.7. Statistical Analysis
3. Results
4. Discussion
4.1. Interpretation of Findings Related to Metabolic Syndrome
4.2. Interpretation of Findings Related to Metabolic Syndrome Components
4.2.1. Obesity
4.2.2. Triglycerides
4.2.3. Remaining Metabolic Syndrome Criteria
4.3. Limitations
4.4. Strengths
4.5. Biological Explanation
4.6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leng, Y.; Wainwright, N.W.J.; Cappuccio, F.P.; Surtees, P.G.; Hayat, S.; Luben, R.; Brayne, C.; Khaw, K.-T. Daytime Napping and the Risk of All-Cause and Cause-Specific Mortality: A 13-Year Follow-up of a British Population. Am. J. Epidemiol. 2014, 179, 1115–1124. [Google Scholar] [CrossRef] [PubMed]
- Hublin, C.; Lehtovirta, M.; Partinen, M.; Koskenvuo, M.; Kaprio, J. Napping and the risk of type 2 diabetes: A population-based prospective study. Sleep Med. 2016, 17, 144–148. [Google Scholar] [CrossRef][Green Version]
- Van der Pal, K.C.; Koopman, A.D.M.; Lakerveld, J.; van der Heijden, A.A.; Elders, P.J.; Beulens, J.W.; Rutters, F. The association between multiple sleep-related characteristics and the metabolic syndrome in the general population: The New Hoorn study. Sleep Med. 2018, 52, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Häusler, N.; Haba-Rubio, J.; Heinzer, R.; Marques-Vidal, P. Association of napping with incident cardiovascular events in a prospective cohort study. Heart 2019, 105, 1793–1798. [Google Scholar] [CrossRef] [PubMed]
- Langer Research Associates. Sleep in America® Poll 2019: Sleep Health and Scheduling; National Sleep Foundation: Arlington, VA, USA, 2019. [Google Scholar]
- Devine, J.K.; Wolf, J.M. Integrating nap and night-time sleep into sleep patterns reveals differential links to health-relevant outcomes. J. Sleep Res. 2016, 25, 225–233. [Google Scholar] [CrossRef]
- Ficca, G.; Axelsson, J.; Mollicone, D.J.; Muto, V.; Vitiello, M.V. Naps, cognition and performance. Sleep Med. Rev. 2010, 14, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Motoyoshi, N.; Hori, T. Recuperative Power of a Short Daytime Nap With or Without Stage 2 Sleep. Sleep 2005, 28, 829–836. [Google Scholar]
- Watling, C.N.; Smith, S.S.; Horswill, M.S. Stop and revive? The effectiveness of nap and active rest breaks for reducing driver sleepiness: Nap and active rest breaks. Psychophysiol 2014, 51, 1131–1138. [Google Scholar] [CrossRef] [PubMed]
- Philip, P.; Taillard, J.; Moore, N.; Delord, S.; Valtat, C.; Sagaspe, P.; Bioulac, B. The Effects of Coffee and Napping on Nighttime Highway Driving: A Randomized Trial. Ann. Intern. Med. 2006, 144, 785. [Google Scholar] [CrossRef]
- Trichopoulos, D.; Tzonou, A.; Christopoulos, C.; Havatzoglou, S.; Trichopoulou, A. Does a Siesta Protect From Coronary Artery Disease? Lancet 1987, 330, 269–270. [Google Scholar] [CrossRef]
- Tanabe, N.; Iso, H.; Seki, N.; Suzuki, H.; Yatsuya, H.; Toyoshima, H.; Tamakoshi, A.; JACC Study Group. Daytime napping and mortality, with a special reference to cardiovascular disease: The JACC study. Int. J. Epidemiol. 2010, 39, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Campos, H.; Siles, X. Siesta and the risk of coronary heart disease: Results from a population-based, case-control study in Costa Rica. Int. J. Epidemiol. 2000, 29, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Stang, A.; Dragano, N.; Moebus, S.; Möhlenkamp, S.; Schmermund, A.; Kälsch, H.; Erbel, R.; Jöckel, K.-H.; Heinz Nixdorf Recall Investigative Group. Midday Naps and the Risk of Coronary Artery Disease: Results of the Heinz Nixdorf Recall Study. Sleep 2012, 35, 1705–1712. [Google Scholar] [CrossRef] [PubMed]
- Yan, B.; Li, J.; Li, R.; Gao, Y.; Zhang, J.; Wang, G. Association of daytime napping with incident cardiovascular disease in a community-based population. Sleep Med. 2019, 57, 128–134. [Google Scholar] [CrossRef]
- Bursztyn, M.; Ginsberg, G.; Hammerman-Rozenberg, R.; Stessman, J. The Siesta in the Elderly: Risk Factor for Mortality? Arch. Intern. Med. 1999, 159, 1582. [Google Scholar] [CrossRef] [PubMed]
- Bursztyn, M.; Ginsberg, G.; Stessman, J. The Siesta and Mortality in the Elderly: Effect of Rest Without Sleep and Daytime Sleep Duration. Sleep 2002, 25, 187–191. [Google Scholar] [CrossRef]
- Burazeri, G.; Gofin, J.; Kark, J.D. Siesta and Mortality in a Mediterranean Population: A Community Study in Jerusalem. Sleep 2003, 26, 578–584. [Google Scholar] [CrossRef]
- Bursztyn, M.; Stessman, J. The Siesta and Mortality: Twelve Years of Prospective Observations in 70-Year-Olds. Sleep 2005, 28, 345–347. [Google Scholar] [PubMed]
- Stone, K.L.; Ewing, S.K.; Ancoli-Israel, S.; Ensrud, K.E.; Redline, S.; Bauer, D.C.; Cauley, J.A.; Hillier, T.A.; Cummings, S.R. Self-Reported Sleep and Nap Habits and Risk of Mortality in a Large Cohort of Older Women: Sleep predicts mortality in older women. J. Am. Geriatr. Soc. 2009, 57, 604–611. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, Q.; Shang, X. Meta-Analysis of Self-Reported Daytime Napping and Risk of Cardiovascular or All-Cause Mortality. Med. Sci. Monit. 2015, 21, 1269–1275. [Google Scholar] [PubMed]
- Zhong, G.; Wang, Y.; Tao, T.; Ying, J.; Zhao, Y. Daytime napping and mortality from all causes, cardiovascular disease, and cancer: A meta-analysis of prospective cohort studies. Sleep Med. 2015, 16, 811–819. [Google Scholar] [CrossRef] [PubMed]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The Metabolic Syndrome and Cardiovascular Risk. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S. Risks for All-Cause Mortality, Cardiovascular Disease, and Diabetes Associated With the Metabolic Syndrome: A summary of the evidence. Diabetes Care 2005, 28, 1769–1778. [Google Scholar] [CrossRef]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the Metabolic Syndrome: A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed]
- Sattar, N.; McConnachie, A.; Shaper, A.G.; Blauw, G.J.; Buckley, B.M.; de Craen, A.J.; Ford, I.; Forouhi, N.G.; Freeman, D.J.; Jukema, J.W.; et al. Can metabolic syndrome usefully predict cardiovascular disease and diabetes? Outcome data from two prospective studies. Lancet 2008, 371, 1927–1935. [Google Scholar] [CrossRef]
- Esposito, K.; Chiodini, P.; Colao, A.; Lenzi, A.; Giugliano, D. Metabolic Syndrome and Risk of Cancer: A systematic review and meta-analysis. Diabetes Care 2012, 35, 2402–2411. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Chiodini, P.; Capuano, A.; Bellastella, G.; Maiorino, M.I.; Rafaniello, C.; Panagiotakos, D.B.; Giugliano, D. Colorectal cancer association with metabolic syndrome and its components: A systematic review with meta-analysis. Endocrine 2013, 44, 634–647. [Google Scholar] [CrossRef] [PubMed]
- Elsamna, S.; Elkattawy, O.; Merchant, A.M. Association of metabolic syndrome with morbidity and mortality in emergency general surgery. Am. J. Surg. 2020, 220, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Lak, K.L.; Helm, M.C.; Kindel, T.L.; Gould, J.C. Metabolic Syndrome Is a Significant Predictor of Postoperative Morbidity and Mortality Following Bariatric Surgery. J. Gastrointest. Surg. 2019, 23, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Pal, K.; Mukadam, N.; Petersen, I.; Cooper, C. Mild cognitive impairment and progression to dementia in people with diabetes, prediabetes and metabolic syndrome: A systematic review and meta-analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, K.; Kanaya, A.; Lindquist, K.; Simonsick, E.M.; Harris, T.; Shorr, R.I.; Tylavsky, F.A.; Newman, A.B. The Metabolic Syndrome, Inflammation, and Risk of Cognitive Decline. JAMA 2004, 292, 2237–2242. [Google Scholar] [CrossRef]
- Wang, J.; Sarnola, K.; Ruotsalainen, S.; Moilanen, L.; Lepistö, P.; Laakso, M.; Kuusisto, J. The metabolic syndrome predicts incident congestive heart failure: A 20-year follow-up study of elderly finns. Atherosclerosis 2010, 210, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Yamada, T.; Shojima, N.; Yamauchi, T.; Kadowaki, T. J-curve relation between daytime nap duration and type 2 diabetes or metabolic syndrome: A dose-response meta-analysis. Sci. Rep. 2016, 6, 38075. [Google Scholar] [CrossRef] [PubMed]
- Sayón-Orea, C.; Bes-Rastrollo, M.; Carlos, S.; Beunza, J.J.; Basterra-Gortari, F.J.; Martínez-González, M.A. Association between Sleeping Hours and Siesta and the Risk of Obesity: The SUN Mediterranean Cohort. Obes. Facts 2013, 6, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Carlos, S.; De La Fuente-Arrillaga, C.; Bes-Rastrollo, M.; Razquin, C.; Rico-Campà, A.; Martínez-González, M.; Ruiz-Canela, M. Mediterranean Diet and Health Outcomes in the SUN Cohort. Nutrients 2018, 10, 439. [Google Scholar] [CrossRef]
- Willett, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- Fernández-Montero, A.; Beunza, J.J.; Bes-Rastrollo, M.; Barrio, M.T.; de la Fuente-Arrillaga, C.; Moreno-Galarraga, L.; Martínez-González, M.A. Validación de los componentes del síndrome metabólico autodeclarados en un estudio de cohortes. Gac. Sanit. 2011, 25, 303–307. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Consensus Conference Panel; Watson, N.F.; Badr, M.S.; Belenky, G.; Bliwise, D.L.; Buxton, O.M.; Buysse, D.; Dinges, D.F.; Gangwisch, J.; Grandner, M.A.; et al. Recommended Amount of Sleep for a Healthy Adult: A Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society. J. Clin. Sleep Med. 2015, 11, 591–592. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Ouyang, F.; Qiu, D.; Duan, Y.; Luo, D.; Xiao, S. Association of Nap Duration after Lunch with Prevalence of Metabolic Syndrome in a Chinese Government Employee Population. IJERPH 2020, 17, 4268. [Google Scholar] [CrossRef]
- Lin, D.; Sun, K.; Li, F.; Qi, Y.; Ren, M.; Huang, C.; Tang, J.; Xue, S.; Li, Y.; Yan, L. Association between habitual daytime napping and metabolic syndrome: A population-based study. Metabolism 2014, 63, 1520–1527. [Google Scholar] [CrossRef]
- Yang, L.; Xu, Z.; He, M.; Yang, H.; Li, X.; Min, X.; Zhang, C.; Xu, C.; Angileri, F.; Légaré, S.; et al. Sleep Duration and Midday Napping with 5-Year Incidence and Reversion of Metabolic Syndrome in Middle-Aged and Older Chinese. Sleep 2016, 39, 1911–1918. [Google Scholar] [CrossRef]
- Ghazizadeh, H.; Mobarra, N.; Esmaily, H.; Seyedi, S.M.R.; Amiri, A.; Rezaeitalab, F.; Mokhber, N.; Moohebati, M.; Ebrahimi, M.; Tayebi, M.; et al. The association between daily naps and metabolic syndrome: Evidence from a population-based study in the Middle-East. Sleep Health 2020, 6, 684–689. [Google Scholar] [CrossRef]
- Loredo, J.S.; Weng, J.; Ramos, A.R.; Sotres-Alvarez, D.; Simonelli, G.; Talavera, G.A.; Patel, S.R. Sleep Patterns and Obesity. Chest 2019, 156, 348–356. [Google Scholar] [CrossRef]
- Ramos, A.R.; Weng, J.; Wallace, D.M.; Petrov, M.R.; Wohlgemuth, W.K.; Sotres-Alvarez, D.; Loredo, J.S.; Reid, K.J.; Zee, P.C.; Mossavar-Rahmani, Y.; et al. Sleep Patterns and Hypertension Using Actigraphy in the Hispanic Community Health Study/Study of Latinos. Chest 2018, 153, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Zhang, X.; Liang, Y.; Xue, H.; Gong, Y.; Xiong, J.; He, F.; Yang, Y.; Cheng, G. Associations between nocturnal sleep duration, midday nap duration and body composition among adults in Southwest China. PLoS ONE 2019, 14, e0223665. [Google Scholar] [CrossRef] [PubMed]
- Hubert Lam, K.; Jiang, C.Q.; Thomas, G.N.; Arora, T.; Zhang, W.S.; Taheri, S.; Adab, P.; Lam, T.H.; Cheng, K.K. Napping Is Associated with Increased Risk of Type 2 Diabetes: The Guangzhou Biobank Cohort Study. Sleep 2010, 33, 402–407. [Google Scholar] [CrossRef] [PubMed]
- Guo, V.Y.; Cao, B.; Wong, C.K.H.; Yu, E.Y.T. The association between daytime napping and risk of diabetes: A systematic review and meta-analysis of observational studies. Sleep Med. 2017, 37, 105–112. [Google Scholar] [CrossRef]
- Chen, G.-C.; Liu, M.-M.; Chen, L.-H.; Xu, J.-Y.; Hidayat, K.; Li, F.-R.; Qin, L.-Q. Daytime napping and risk of type 2 diabetes: A meta-analysis of prospective studies. Sleep Breath 2018, 22, 815–824. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Shen, L.; Wu, J.; Yang, H.; Fang, W.; Chen, W.; Yuan, J.; Wang, Y.; Liang, Y.; Wu, T. The effects of midday nap duration on the risk of hypertension in a middle-aged and older Chinese population: A preliminary evidence from the Tongji-Dongfeng Cohort Study, China. J. Hypertens 2014, 32, 1993–1998. [Google Scholar] [CrossRef] [PubMed]
- Barrio-Lopez, M.T.; Bes-Rastrollo, M.; Beunza, J.J.; Fernandez-Montero, A.; Garcia-Lopez, M.; Martinez-Gonzalez, M.A. Validation of metabolic syndrome using medical records in the SUN cohort. BMC Public Health 2011, 11, 867. [Google Scholar] [CrossRef] [PubMed]
- Crnko, S.; Du Pré, B.C.; Sluijter, J.P.G.; Van Laake, L.W. Circadian rhythms and the molecular clock in cardiovascular biology and disease. Nat. Rev. Cardiol. 2019, 16, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Maury, E.; Hong, H.K.; Bass, J. Circadian disruption in the pathogenesis of metabolic syndrome. Diabetes Metab. 2014, 40, 338–346. [Google Scholar] [CrossRef] [PubMed]
- Bedrosian, T.A.; Fonken, L.K.; Nelson, R.J. Endocrine Effects of Circadian Disruption. Annu. Rev. Physiol. 2016, 78, 109–131. [Google Scholar] [CrossRef] [PubMed]
- Engin, A.B.; Engin, A. (Eds.) Advances in experimental medicine and biology. In Obesity and Lipotoxicity; Springer International Publishing: Cham, Switzerland, 2017; Volume 960, ISBN 978-3-319-48380-1. [Google Scholar]
- Reutrakul, S.; Van Cauter, E. Sleep influences on obesity, insulin resistance, and risk of type 2 diabetes. Metabolism 2018, 84, 56–66. [Google Scholar] [CrossRef]
- Scheer, F.A.J.L.; Hilton, M.F.; Mantzoros, C.S.; Shea, S.A. Adverse metabolic and cardiovascular consequences of circadian misalignment. Proc. Natl. Acad. Sci. USA 2009, 106, 4453–4458. [Google Scholar] [CrossRef]
- West, A.C.; Smith, L.; Ray, D.W.; Loudon, A.S.I.; Brown, T.M.; Bechtold, D.A. Misalignment with the external light environment drives metabolic and cardiac dysfunction. Nat. Commun. 2017, 8, 417. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Total Sample | No Siesta (0 min/Day) | Short Siesta (≤30 min/Day) | Long Siesta (>30 min/Day) | p |
|---|---|---|---|---|---|
| N | 9161 | 3719 | 3897 | 1545 | |
| Women (%) | 68.92% | 69.86% | 67.33% | 66.93% | 0.03 |
| Age (years) (M ± SD) | 36.1 ± 10.5 | 35.3 ± 10.3 | 36.9 ± 10.1 | 36.1 ± 11.6 | <0.001 |
| Year of entry into cohort (M ± SD) | 2003 ± 2.9 | 2002 ± 2.9 | 2003 ± 3.0 | 2003 ± 2.8 | <0.001 |
| Years of tertiary study (years) (M ± SD) | 5.1 ± 1.5 | 5.1 ± 1.5 | 5.1 ± 1.5 | 4.9 ± 1.4 | <0.001 |
| Employment status: | <0.001 | ||||
| Full-time (%) | 72.76% | 68.73% | 77.34% | 70.94% | |
| Part-time (%) | 9.26% | 10.11% | 8.83% | 8.28% | |
| Other (%) | 17.98% | 21.16% | 13.83% | 20.78% | |
| Working hours (h/wk) (M ± SD) | 36.8 ± 16.7 | 36.2 ± 17.5 | 38.0 ± 15.6 | 35.4 ± 17.2 | <0.001 |
| Lunch at home (days/wk) (M ± SD) | 5.5 ± 2.1 | 5.4 ± 2.1 | 5.4 ± 2.1 | 5.9 ± 1.7 | <0.001 |
| Night-time sleep (h/night) (M ± SD) | 7.4 ± 0.9 | 7.4 ± 0.9 | 7.4 ± 0.8 | 7.3 ± 1.1 | <0.001 |
| Daily television (h/day) (M ± SD) | 1.6 ± 1.3 | 1.5 ± 1.4 | 1.5 ± 1.0 | 2.0 ± 1.5 | <0.001 |
| Smoking pack-years (pack-year) (M ± SD) | 4.6 ± 7.8 | 3.8 ± 7.0 | 4.8 ± 7.8 | 5.7 ± 9.4 | <0.001 |
| Alcohol (g/day) (M ± SD) | 5.8 ± 8.3 | 4.9 ± 7.5 | 6.3 ± 8.3 | 6.7 ± 9.8 | <0.001 |
| Total energy intake (kcal/day) (M ± SD) | 2362.2 ± 594.4 | 2351.6 ± 592.6 | 2362.0 ± 590.4 | 2388.3 ± 608.3 | 0.13 |
| Coffee intake (cups/day) (M ± SD) | 1.2 ± 1.2 | 1.3 ± 1.3 | 1.3 ± 1.2 | 1.1 ± 1.3 | <0.001 |
| Mediterranean Diet Score (score out of 9) (M ± SD) | 4.2 ± 1.8 | 4.0 ± 1.8 | 4.3 ± 1.8 | 4.3 ± 1.8 | <0.001 |
| Special diets (%) | 6.27% | 6.16% | 6.21% | 6.67% | 0.77 |
| Physical activity (METs-h/week) (M ± SD) | 20.9 ± 22.4 | 20.7 ± 22.5 | 21.0 ± 21.8 | 21.2 ± 23.5 | 0.75 |
| Social time (h/day) (M ± SD) | 0.6 ± 0.4 | 0.5 ± 0.4 | 0.5 ± 0.4 | 0.6 ± 0.4 | <0.001 |
| Prevalent cardiovascular disease (%) | 0.67% | 0.59% | 0.69% | 0.78% | 0.73 |
| Prevalent cancer (%) | 2.16% | 2.02% | 2.36% | 2.01% | 0.53 |
| Prevalent depression or use of antidepressant medication (%) | 10.53% | 9.49% | 10.37% | 13.46% | <0.001 |
| Previous history of insomnia (%) | 16.88% | 15.46% | 17.35% | 19.09% | <0.001 |
| Obstructive sleep apnea (%) | 0.75% | 0.67% | 0.80% | 0.84% | 0.75 |
| Snoring (%) | 13.66% | 11.86% | 14.32% | 16.31% | <0.001 |
| Weight gain prior to C0 (kg) (M ± SD) | 0.8 ± 4.0 | 0.7 ± 4.0 | 0.8 ± 3.9 | 1.0 ± 4.1 | 0.01 |
| Tendency to stress (0–10) (M ± SD) | 6.0 ± 2.2 | 6.0 ± 2.2 | 6.0 ± 2.2 | 6.0 ± 2.2 | 0.23 |
| Siesta Length | |||
|---|---|---|---|
| No Siesta | Short Siesta (≤30 min) | Long Siesta (>30 min) | |
| N | 3719 | 3897 | 1545 |
| Cases | 120 | 162 | 93 |
| % Absolute risk (cases/N) | 3.23% | 4.16% | 6.02% |
| Crude OR (95% CI) | 1 Ref. | 1.30 (1.02–1.65) | 1.92 (1.46–2.54) |
| Age and Sex adjusted OR (95% CI) | 1 Ref. | 1.15 (0.89–1.47) | 1.59 (1.19–2.13) |
| Multivariable adjusted OR (95% CI) | 1 Ref. | 1.07 (0.83–1.37) | 1.39 (1.03–1.88) |
| Crude OR (95% CI) | 0.77 (0.60–0.98) | 1 Ref. | 1.48 (1.14–1.92) |
| Age and Sex adjusted OR (95% CI) | 0.87 (0.68–1.12) | 1 Ref. | 1.39 (1.05–1.83) |
| Multivariable adjusted OR (95% CI) | 0.94 (0.73–1.21) | 1 Ref. | 1.30 (0.98–1.73) |
| Siesta Length | |||
|---|---|---|---|
| Metabolic Syndrome Criteria | No Siesta | Short Siesta (≤30 min) | Long Siesta (>30 min) |
| Obesity (Waist Circumference ≥ 80 cm in women or ≥ 94 cm in men or BMI ≥ 30 kg/m2) | |||
| N ** = 9161 | N = 3719 | N = 3897 | N = 1545 |
| Cases = 3662 | 1399 | 1593 | 670 |
| % Absolute risk = 39.97% | 37.62% | 40.88% | 43.37% |
| Multivariable adjusted OR (95% CI) | 1 Ref. | 1.04 (0.94–1.15) | 1.15 (1.01–1.32) |
| High triglycerides (Serum triglycerides ≥ 150 mg/dL or pharmacological treatment for high triglycerides) | |||
| N ** = 5345 | N = 2149 | N = 2294 | N = 902 |
| Cases = 417 | 142 | 185 | 90 |
| % Absolute risk = 7.80% | 6.61% | 8.06% | 9.98% |
| Multivariable adjusted OR (95% CI) | 1 Ref. | 1.10 (0.88–1.39) | 1.33 (1.00–1.76) |
| Low HDL cholesterol (Serum HDL cholesterol < 50 mg/dL in women or <40 mg/dL in men) | |||
| N ** = 4705 | N = 1856 | N = 2054 | N = 795 |
| Cases = 488 | 199 | 193 | 96 |
| % Absolute risk = 10.37% | 10.72% | 9.39% | 12.08% |
| Multivariable adjusted OR (95% CI) | 1 Ref. | 0.90 (0.73–1.10) | 1.13 (0.87–1.47) |
| Hypertension (Systolic blood pressure ≥ 130 mmHg or diastolic blood pressure ≥ 85 mmHg or pharmacological treatment for hypertension) | |||
| N ** = 7724 | N = 3079 | N = 3316 | N = 1329 |
| Cases = 1486 | 550 | 654 | 282 |
| % Absolute risk = 19.24% | 17.86% | 19.72% | 21.22% |
| Multivariable adjusted OR (95% CI) | 1 Ref. | 1.01 (0.88–1.15) | 1.09 (0.92–1.30) |
| Hyperglycaemia (Fasting glucose ≥ 100 mg/dL or pharmacological treatment for hyperglycaemia) | |||
| N ** = 6616 | N = 2615 | N = 2855 | N = 1146 |
| Cases = 759 | 266 | 344 | 149 |
| % Absolute risk = 11.47% | 10.17% | 12.05% | 13.00% |
| Multivariable adjusted OR (95% CI) | 1 Ref. | 1.09 (0.92–1.30) | 1.10 (0.88–1.38) |
| Siesta Length | ||||
|---|---|---|---|---|
| Potential Modifier of Effect of Siesta | No Siesta | Short Siesta (≤30 min) | Long Siesta (>30 min) | p for Interaction |
| N = 3719 | N = 3897 | N = 1545 | ||
| Age | 0.354 | |||
| Age < 50 years (N = 8080) | ||||
| N | 3339 | 3422 | 1319 | |
| Cases | 71 | 104 | 49 | |
| aOR (95% CI) | 1 Ref. | 1.18 (0.86–1.61) | 1.53 (1.04–2.27) | |
| Age ≥ 50 years (N = 1081) | ||||
| N | 380 | 475 | 226 | |
| Cases | 49 | 58 | 44 | |
| aOR (95% CI) | 1 Ref. | 0.87 (0.56–1.33) | 1.31 (0.81–2.12) | |
| Sex | 0.368 | |||
| Men (N = 2905) | ||||
| N | 1121 | 1273 | 511 | |
| Cases | 66 | 87 | 57 | |
| aOR (95% CI) | 1 Ref. | 0.94 (0.66–1.33) | 1.35 (0.90–2.03) | |
| Women (N = 6256) | ||||
| N | 2598 | 2624 | 1034 | |
| Cases | 54 | 75 | 36 | |
| aOR (95% CI) | 1 Ref. | 1.20 (0.83–1.73) | 1.45 (0.92–2.29) | |
| Sleep disorder | 0.879 | |||
| No sleep disorder (N = 7554) | ||||
| N | 3118 | 3199 | 1237 | |
| Cases | 94 | 124 | 68 | |
| aOR (95% CI) | 1 Ref. | 1.10 (0.83–1.47) | 1.42 (1.01–2.01) | |
| Sleep disorder (N = 1607) | ||||
| N | 601 | 698 | 308 | |
| Cases | 26 | 38 | 25 | |
| aOR (95% CI) | 1 Ref. | 1.00 (0.58–1.71) | 1.27 (0.68–2.38) | |
| Night-time sleep duration | 0.104 | |||
| 7–8 h of nightly sleep (N = 6358) | ||||
| N | 2622 | 2837 | 899 | |
| Cases | 85 | 117 | 47 | |
| aOR (95% CI) | 1 Ref. | 1.08 (0.80–1.46) | 1.19 (0.80–1.76) | |
| <7 or >8 h of nightly sleep (N = 2803) | ||||
| N | 1097 | 1060 | 646 | |
| Cases | 35 | 45 | 46 | |
| aOR (95% CI) | 1 Ref. | 1.06 (0.66–1.71) | 1.71 (1.04–2.80) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gribble, A.K.; Sayón-Orea, C.; Bes-Rastrollo, M.; Kales, S.N.; Shirahama, R.; Martínez-González, M.Á.; Fernandez-Montero, A. Risk of Developing Metabolic Syndrome Is Affected by Length of Daily Siesta: Results from a Prospective Cohort Study. Nutrients 2021, 13, 4182. https://doi.org/10.3390/nu13114182
Gribble AK, Sayón-Orea C, Bes-Rastrollo M, Kales SN, Shirahama R, Martínez-González MÁ, Fernandez-Montero A. Risk of Developing Metabolic Syndrome Is Affected by Length of Daily Siesta: Results from a Prospective Cohort Study. Nutrients. 2021; 13(11):4182. https://doi.org/10.3390/nu13114182
Chicago/Turabian StyleGribble, Anne Katherine, Carmen Sayón-Orea, Maira Bes-Rastrollo, Stefanos N. Kales, Ryutaro Shirahama, Miguel Ángel Martínez-González, and Alejandro Fernandez-Montero. 2021. "Risk of Developing Metabolic Syndrome Is Affected by Length of Daily Siesta: Results from a Prospective Cohort Study" Nutrients 13, no. 11: 4182. https://doi.org/10.3390/nu13114182
APA StyleGribble, A. K., Sayón-Orea, C., Bes-Rastrollo, M., Kales, S. N., Shirahama, R., Martínez-González, M. Á., & Fernandez-Montero, A. (2021). Risk of Developing Metabolic Syndrome Is Affected by Length of Daily Siesta: Results from a Prospective Cohort Study. Nutrients, 13(11), 4182. https://doi.org/10.3390/nu13114182