
Vitamin C in the Treatment of COVID-19


Abstract
:1. Introduction
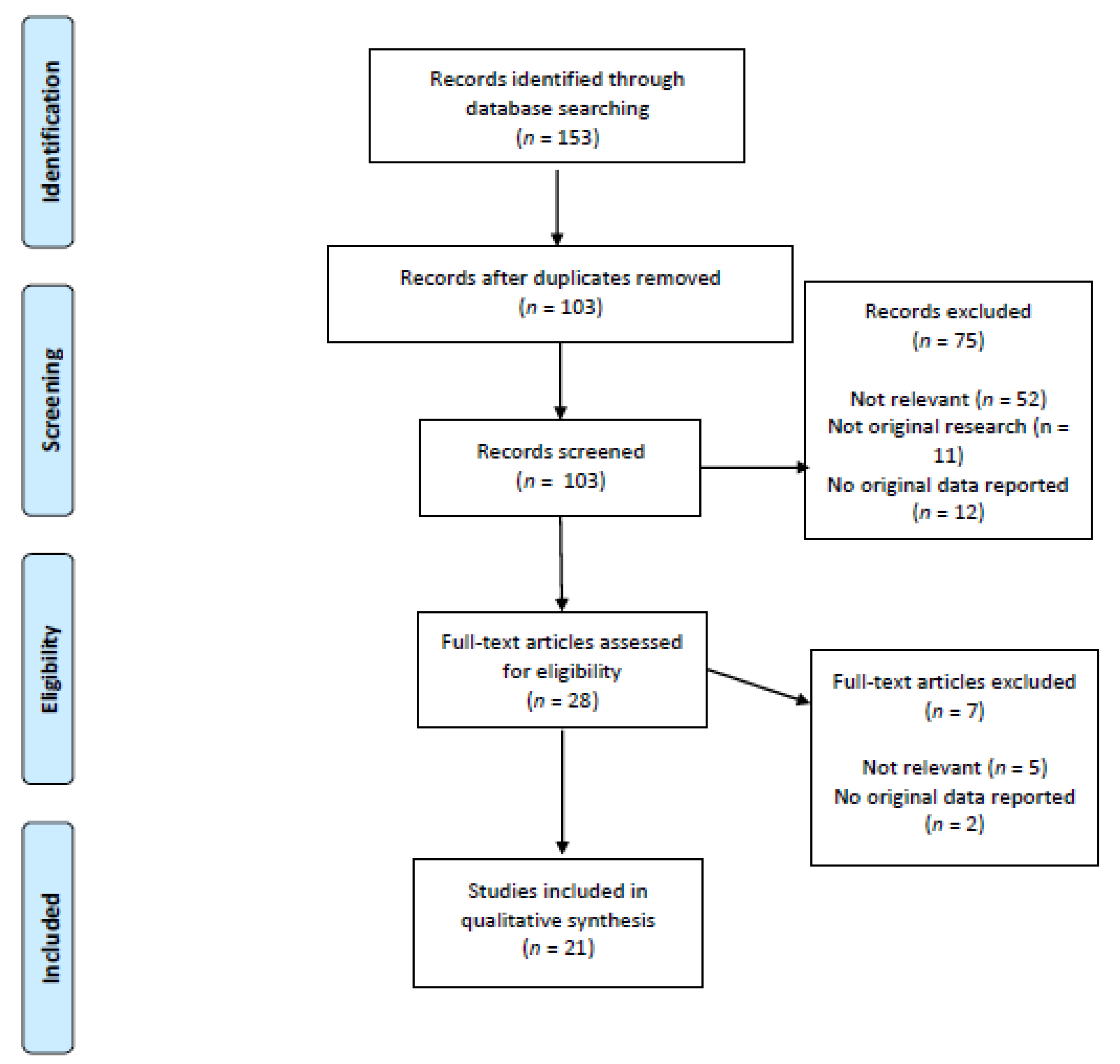
2. Material and Methods
3. Results
3.1. Case Reports and Case Series
3.2. Observational Studies
3.3. Clinical Trials
3.4. Ongoing Trials
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Linster, C.L.; Van Schaftingen, E. Vitamin C. Biosynthesis, recycling and degradation in mammals. FEBS J. 2007, 274, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Cerullo, G.; Negro, M.; Parimbelli, M.; Pecoraro, M.; Perna, S.; Liguori, G.; Rondanelli, M.; Cena, H.; D’Antona, G. The Long History of Vitamin C: From Prevention of the Common Cold to Potential Aid in the Treatment of COVID-19. Front. Immunol. 2020, 11, 2036. [Google Scholar] [CrossRef] [PubMed]
- Vissers, M.C.M.; Wilkie, R.P. Ascorbate deficiency results in impaired neutrophil apoptosis and clearance and is associated with up-regulation of hypoxia-inducible factor 1α. J. Leukoc. Biol. 2007, 81, 1236–1244. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Maggini, S. Vitamina C y función inmune. Nutrients 2017, 9, 1211. [Google Scholar] [CrossRef] [Green Version]
- Hemilä, H. Vitamin C and Infections. Nutrients 2017, 29, 339. [Google Scholar] [CrossRef] [Green Version]
- Bakaev, V.V.; Duntau, A.P. Ascorbic acid in blood serum of patients with pulmonary tuberculosis and pneumonia. Int. J. Tuberc. Lung Dis. 2004, 8, 263–266. [Google Scholar]
- Hemilä, H. Vitamin C and the common cold. Br. J. Nutr. 1992, 67, 3–16. [Google Scholar] [CrossRef] [Green Version]
- Carr, A.C.; Rosengrave, P.C.; Bayer, S.; Chambers, S.; Mehrtens, J.; Shaw, G.M. Hypovitaminosis C and vitamin C deficiency in critically ill patients despite recommended enteral and parenteral intakes. Crit. Care 2017, 21, 300. [Google Scholar] [CrossRef] [Green Version]
- Schorah, C.J.; Downing, C.; Piripitsi, A.; Gallivan, L.; Al-Hazaa, A.H.; Sanderson, M.J.; Bodenham, A. Total vitamin C, ascorbic acid, and dehydroascorbic acid concentrations in plasma of critically ill patients. Am. J. Clin. Nutr. 1996, 63, 760–765. [Google Scholar] [CrossRef]
- Li, R.; Guo, C.; Li, Y.; Qin, Z.; Huang, W. Therapeutic targets and signaling mechanisms of vitamin C activity against sepsis: A bioinformatics study. Brief Bioinf. 2020. [Google Scholar] [CrossRef]
- Pauling, L. The significance of the evidence about ascorbic acid and the common cold. Proc. Natl. Acad. Sci. USA 1971, 68, 2678–2681. [Google Scholar] [CrossRef] [Green Version]
- Dykes, M.H.; Meier, P. Ascorbic acid and the common cold. Evaluation of its efficacy and toxicity. JAMA 1975, 231, 1073–1079. [Google Scholar] [CrossRef] [PubMed]
- Hemilä, H.; Chalker, E. Vitamin C for preventing and treating the common cold. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [Green Version]
- Padhani, Z.A.; Moazzam, Z.; Ashraf, A.; Bilal, H.; Salam, R.A.; Das, J.K.; Bhutta, Z.A. Vitamin C supplementation for prevention and treatment of pneumonia. Cochrane Database Syst. Rev. 2020, 27. [Google Scholar] [CrossRef]
- Syed, A.A.; Knowlson, S.; Sculthorpe, R.; Farthing, D.; DeWilde, C.; Farthing, C.A.; Larus, T.L.; Martin, E.; Brophy, D.F.; Gupta, S.; et al. Phase I safety trial of intravenous ascorbic acid in patients with severe sepsis. J. Transl. Med. 2014, 12, 32. [Google Scholar]
- Fowler, A.A., III; Truwit, J.D.; Hite, R.D.; Morris, P.E.; DeWilde, C.; Priday, A.; Fisher, B.; Thacker, L.R., II; Natarajan, R.; Brophy, D.F.; et al. Effect of Vitamin C Infusion on Organ Failure and Biomarkers of Inflammation and Vascular Injury in Patients with Sepsis and Severe Acute Respiratory Failure: The CITRIS-ALI Randomized Clinical Trial. JAMA 2019, 322, 1261–1270. [Google Scholar] [CrossRef]
- Wei, X.-B.; Wang, Z.-H.; Liao, X.-L.; Guo, W.-X.; Wen, J.-Y.; Qin, T.-H.; Wang, S.-H. Efficacy of vitamin C in patients with sepsis: An updated meta-analysis. Eur. J. Pharmacol. 2020, 868, 172889. [Google Scholar] [CrossRef]
- Zhang, M.; Jativa, D.F. Vitamin C supplementation in the critically ill: A systematic review and meta-analysis. SAGE Open Med. 2018, 6. [Google Scholar] [CrossRef] [Green Version]
- Langlois, P.L.; Manzanares, W.; Adhikari, N.A.-O.; Lamontagne, F.; Stoppe, C.A.-O.; Hill, A.; Heyland, D.K. Vitamin C Administration to the Critically Ill: A Systematic Review and Meta-Analysis. JPEN 2019, 43, 335–346. [Google Scholar] [CrossRef]
- Hemilä, H.; Chalker, E. Vitamin C may reduce the duration of mechanical ventilation in critically ill patients: A meta-regression analysis. J. Intensive Care 2020, 8, 15. [Google Scholar] [CrossRef] [Green Version]
- Khan, H.M.W.; Parikh, N.; Megala, S.M.; Predeteanu, G.S.; Waqas Khan, H.M.; Parikh, N.; Megala, S.M.; Predeteanu, G.S. Unusual early recovery of a critical COVID-19 patient after administration of intravenous vitamin C. Am. J. Case Rep. 2020, 21, 1–6. [Google Scholar]
- Hiedra, R.; Lo, K.B.; Elbashabsheh, M.; Gul, F.; Wright, R.M.; Albano, J.; Azmaiprashvili, Z.; Patarroyo Aponte, G. The Use of IV vitamin C for patients with COVID-19: A single center observational study. Expert Rev. Anti-Infect. Ther. 2020, 18, 1259–1261. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Chen, W.; Zhou, J.; Sun, C.; Lei, Y. Large pulmonary cavity in COVID-19 cured patient case report. Ann. Palliat. Med. 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Ding, H.; Deng, W.; Ding, L.; Ye, X.; Yin, S.; Huang, W. Glycyrrhetinic acid and its derivatives as potential alternative medicine to relieve symptoms in nonhospitalized COVID-19 patients. J. Med. Virol. 2020, 92, 2200–2204. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.; Ling, Y.; Li, J.; Peng, Y.; Huang, J.; Wang, Y.; Qu, H.; Gao, Y.; Li, Y.; Hu, B.; et al. Beneficial aspects of high dose intravenous vitamin c on patients with covid-19 pneumonia in severe condition: A retrospective case series study. Ann. Palliat. Med. 2020, 9, 1–11. [Google Scholar] [CrossRef]
- Bahloul, M.; Ketata, W.; Lahyeni, D.; Mayoufi, H.; Kotti, A.; Smaoui, F.; Kallel, N.; Daoud, E.; Bouaziz, M.; Kammoun, S. Pulmonary capillary leak syndrome following COVID-19 virus infection. J. Med. Virol. 2020. [Google Scholar] [CrossRef]
- Deliwala, S.S.; Ponnapalli, A.; Seedahmed, E.; Berrou, M.; Bachuwa, G.; Chandran, A. A 29-year-old male with a fatal case of covid-19 acute respiratory distress syndrome (Cards) and ventilator-induced lung injury (vili). Am. J. Case Rep. 2020, 21, 1–6. [Google Scholar] [CrossRef]
- Douedi, S.; Miskoff, J. Novel coronavirus 2019 (COVID-19). Medicine 2020, 99, e20207. [Google Scholar] [CrossRef]
- Fontana, F.; Cazzato, S.; Giovanella, S.; Ballestri, M.; Leonelli, M.; Mori, G.; Alfano, G.; Ligabue, G.; Magistroni, R.; Cenacchi, G.; et al. Oxalate Nephropathy Caused by Excessive Vitamin C Administration in 2 Patients with COVID-19. Kidney Int. Rep. 2020, 5, 1815–1822. [Google Scholar] [CrossRef]
- Capone, S.; Abramyan, S.; Ross, B.; Rosenberg, J.; Zeibeq, J.; Vasudevan, V.; Samad, R.; Gerolemou, L.; Pinelis, E.; Gasperino, J.; et al. Characterization of Critically Ill COVID-19 Patients at a Brooklyn Safety-Net Hospital. Cureus 2020, 12. [Google Scholar] [CrossRef]
- Krishnan, S.; Patel, K.; Desai, R.; Sule, A.; Paik, P.; Miller, A.; Barclay, A.; Cassella, A.; Lucaj, J.; Royster, Y.; et al. Clinical comorbidities, characteristics, and outcomes of mechanically ventilated patients in the State of Michigan with SARS-CoV-2 pneumonia. J. Clin. Anesth. 2020, 67, 110005. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Guo, T.; Dong, D.; Zhang, X.; Chen, X.; Feng, Y.; Wei, B.; Zhang, W.; Zhao, M.; Wan, J. Defining heart disease risk for death in COVID-19 infection. QJM 2020. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.-H.; Lu, S.-H.; Chen, J.; Xia, L.; Yang, Z.-G.; Charles, S.; Yang, Y.; Lin, Y.; Lu, H.-Z. Clinical characteristics of foreign-imported COVID-19 cases in Shanghai, China. Emerg. Microbes Infect. 2020, 9, 1230–1232. [Google Scholar] [CrossRef] [PubMed]
- Alamdari, D.H.; Moghaddam, A.B.; Amini, S.; Keramati, M.R.; Zarmehri, A.M.; Alamdari, A.H.; Damsaz, M.; Banpour, H.; Yarahmadi, A.; Koliakos, G. Application of methylene blue -vitamin C–N-acetyl cysteine for treatment of critically ill COVID-19 patients, report of a phase-I clinical trial. Eur. J. Pharmacol. 2020, 885, 173494. [Google Scholar] [CrossRef]
- JamaliMoghadamSiahkali, S.; Zarezade, B.; Koolaji, S.; SeyedAlinaghi, S.; Zendehdel, A.; Tabarestani, M.; Sekhavati Moghadam, E.; Abbasian, L.; Dehghan Manshadi, S.A.; Salehi, M.; et al. Safety and effectiveness of high-dose vitamin C in patients with COVID-19: A randomized open-label clinical trial. Eur. J. Med. Res. 2021, 26, 20. [Google Scholar] [CrossRef]
- Zhang, J.; Rao, X.; Li, Y.; Zhu, Y.; Liu, F.; Guo, G.; Luo, G.; Meng, Z.; De Backer, D.; Xiang, H.; et al. Pilot trial of high-dose vitamin C in critically ill COVID-19 patients. Ann. Intensive Care 2021, 11, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Kumari, P.; Dembra, S.; Dembra, P.; Bhawna, F.; Gul, A.; Ali, B.; Sohail, H.; Kumar, B.; Memon, M.K.; Rizwan, A. The Role of Vitamin C as Adjuvant Therapy in COVID-19. Cureus 2020, 12, 10–13. [Google Scholar] [CrossRef]
- Thomas, S.; Patel, D.; Bittel, B.; Wolski, K.; Wang, Q.; Kumar, A.; Il’Giovine, Z.J.; Mehra, R.; McWilliams, C.; Nissen, S.E.; et al. Effect of High-Dose Zinc and Ascorbic Acid Supplementation vs Usual Care on Symptom Length and Reduction Among Ambulatory Patients With SARS-CoV-2 Infection: The COVID A to Z Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e210369. [Google Scholar] [CrossRef] [PubMed]
- Barnabas, R.V.; Brown, E.; Bershteyn, A.; Miller, R.S.; Wener, M.; Celum, C.; Wald, A.; Chu, H.; Wesche, D.; Baeten, J.M. Efficacy of hydroxychloroquine for post-exposure prophylaxis to prevent severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection among adults exposed to coronavirus disease (COVID-19): A structured summary of a study protocol for a randomis. Trials 2020, 21, 475. [Google Scholar] [CrossRef] [PubMed]
- Beigmohammadi, M.T.; Bitarafan, S.; Hoseindokht, A.; Abdollahi, A.; Amoozadeh, L.; Mahmoodi Ali Abadi, M.; Foroumandi, M. Impact of vitamins A, B, C, D, and E supplementation on improvement and mortality rate in ICU patients with coronavirus-19: A structured summary of a study protocol for a randomized controlled trial. Trials 2020, 21, 614. [Google Scholar] [CrossRef]
- Liu, F.; Zhu, Y.; Zhang, J.; Li, Y.; Peng, Z. Intravenous high-dose vitamin C for the treatment of severe COVID-19: Study protocol for a multicentre randomised controlled trial. BMJ Open 2020, 10. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| First Author, Year and Country | Population | Study Design | Exposure/Intervention with Dosage | Outcomes | Key Findings |
|---|---|---|---|---|---|
| Capone S. et al., USA, 2020 [30] | 102 patients (median age 63 years) affected by SARS-CoV-2 and managed by intensive care team | Observational, retrospective | Supplementation of vitamin C (plus zinc). Posology not specified | Overall survival | 72% received supplementation with vitamin C and zinc. No association between vitamin C and overall survival was observed |
| Krishnana S. et al., USA, 2020 [31] | 152 patients (median age 68 years) affected by SARS-CoV-2, requiring mechanical ventilation | Observational, retrospective | Supplementation of vitamin C. Posology not specified | Overall survival | 52% received supplementation with vitamin C. Survival was higher in patients managed with vitamin C (65%, vs. 43%, p = 0.007) |
| Li J. et al., China, 2020 [32] | 596 patients (mean age 56 years) affected by SARS-CoV-2, evaluated at the Hospital | Observational, retrospective | Supplementation of vitamin C. Posology not specified | Prognosis of patients with and without cardiovascular diseases | 16% received vitamin C. Patients with cardiovascular diseases received vitamin C more frequently (23% vs. 12%, p < 0.001) than patients without. No data on prognosis related to the supplementation of vitamin C were available |
| Liu XH et al., China, 2020 [33] | 58 patients (median age 29 years) admitted to the hospital with a SARS-CoV-2 infection | Observational, retrospective | Supplementation of vitamin C. Posology not specified | Clinical characteristics | 69% received vitamin C. No data about the association between vitamin C and clinical outcomes were available |
| Alamdari DH et al., Iran, 2020 [34] | 5 patients (mean age 63 years) admitted to ICU for respiratory distress due to SARS-CoV-2 infection | Phase-I clinical trial | Administration of vitamin C (1500 mg/kg) both oral and intravenous | Respiratory symptoms and safety | Four patients showed improvement both in respiratory symptoms and oxygen saturation after vitamin C administration. The patients were discharged in 10 (4–23) days. One patient discontinued the therapy due to limitations of the drug preparation and expired on the second day of admission |
| JamaliMoghadamSiahkali S. et al., Pakistan, 2020 [35] | A total of 60 patients with a severe SARS-CoV-2 infection: 30 patients (mean age 58 years) received lopinavir/rito- navir and hydroxychloroquine plus vitamin C and 30 (mean age 61 years) only lopinavir/rito- navir and hydroxychloroquine | Randomized open-label clinical trial | Administration of intravenous vitamin C (1.5 g every six hours, total 6 g daily) | The main outcomes were: decrease in mortality, length of hospitalization, and number of patients admitted to ICU. Secondary outcomes were: increase in SpO2 and improvements in vital signs and overall wellbeing | Patients managed with and without vitamin C did not differ for any of the outcomes, except for body temperature (36.8 ± 0.5 vs. 37.2 ± 0.7, respectively, p = 0.001) and SpO2 (90.5 [88.0–92.0] vs. 88.0 [80.0–91.0], respectively p = 0.014) on third day of hospitalization. On the contrary, length of hospitalization was higher in patients managed with vitamin C (8.5 days vs. 6.5 days, p = 0.028) |
| Zang J. et al., China, 2021 [36] | 56 patients (mean age 67 years) with a SARS-CoV-2 infection admitted to intensive care | Randomized, controlled, clinical trial | Administration of intravenous vitamin C (12 g every 12 h, total 24 g daily) for 7 days | The main outcome was invasive mechanical ventilation-free days in 28 days. Secondary outcomes were 28-day mortality, organ failure severity, and interleukin-6 levels | Patients managed with and without vitamin C showed no difference in terms of invasive mechanical ventilation-free days in 28 days and 28-day mortality. A rise in the PaO2/FiO2 (229 vs. 151 mmHg, 95% CI 33 to 122) and lower levels of IL-6 on day 7 (19.42 vs. 158.00, 95% CI −301.72 to −29.79), lower ICU mortality (Hazard Ratio = 0.22, 95% CI 0.1–0.9) in patients with severe multiorgan score failure were observed in patients managed with vitamin C. |
| Kumari P. et al., Pakistan, 2020 [37] | A total of 150 patients admitted for a SARS-CoV-2 infection: 75 (mean age 52 years) were managed with vitamin C and 75 (mean age 53 years) without | Randomized controlled trial | Administration of intravenous vitamin C (50 mg/kg/day). Length of the intervention not specified | The endpoints were: number of days before symptoms disappearance, length of hospital stay, need for ventilation and mortality | Patients managed with vitamin C were symptom-free earlier (7.1 ± 1.8 vs. 9.6 ± 2.1 days, p < 0.0001)) and had a shorter duration of hospitalization (8.1 ± 1.8 vs. 10.7 ± 2.2 days, <0.0001) compared to patients managed without vitamin C. No difference was observed in the need for mechanical ventilation and mortality |
| Thomas S. et al., USA, 2021 [38] | A total of 214 outpatients with a SARS-CoV-2 infection: 48 (mean age 46 years) were managed with vitamin C, 50 (mean age 42 years) with the standard care, 58 (mean age 44 years) with zinc and 58 (mean age 49 years) with vitamin C and zinc | Randomized factorial open-label trial | Administration of: (1) vitamin C (8000 mg in 2–3 times per day), (2) 50 mg of zinc gluconate, (3) both vitamin C and zinc | The main outcome was the number of days to obtain a 50% reduction in symptoms. Secondary outcomes were: days required to resolve symptoms, cumulative severity score symptoms at day 5, hospitalizations, adjunctive prescribed medications, mortality and safety | The study was ended for lack of benefits after the interim analysis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milani, G.P.; Macchi, M.; Guz-Mark, A. Vitamin C in the Treatment of COVID-19. Nutrients 2021, 13, 1172. https://doi.org/10.3390/nu13041172
Milani GP, Macchi M, Guz-Mark A. Vitamin C in the Treatment of COVID-19. Nutrients. 2021; 13(4):1172. https://doi.org/10.3390/nu13041172
Chicago/Turabian StyleMilani, Gregorio Paolo, Marina Macchi, and Anat Guz-Mark. 2021. "Vitamin C in the Treatment of COVID-19" Nutrients 13, no. 4: 1172. https://doi.org/10.3390/nu13041172
APA StyleMilani, G. P., Macchi, M., & Guz-Mark, A. (2021). Vitamin C in the Treatment of COVID-19. Nutrients, 13(4), 1172. https://doi.org/10.3390/nu13041172