
The Relationships between Sleep and Mental and Physical Health of Chinese Elderly: Exploring the Mediating Roles of Diet and Physical Activity


Abstract
:1. Introduction
1.1. The Mediating Role of Diet Quality in the Relationships between Sleep and Health in Older Adults
1.2. The Mediating Role of Physical Activity in the Relationships between Sleep and Health in Older Adults
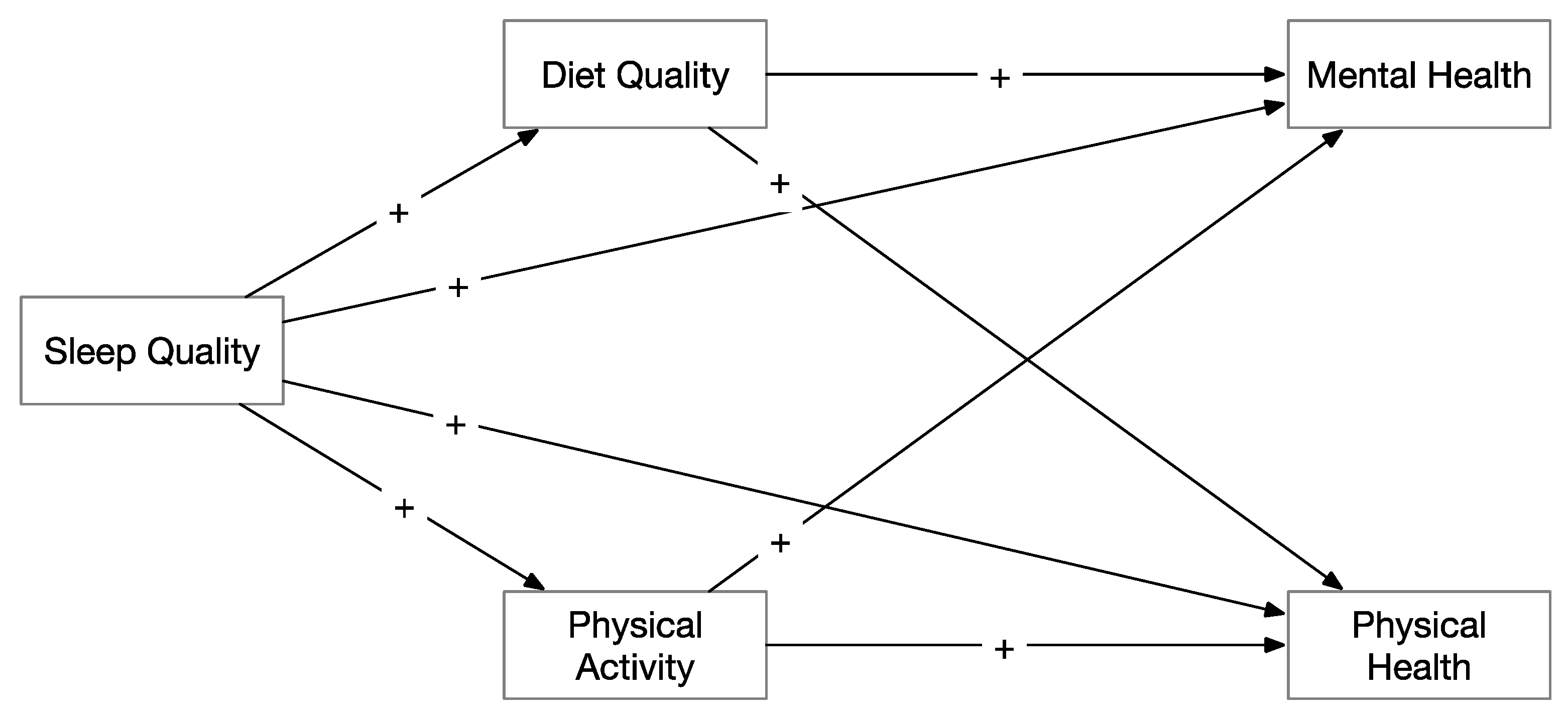
1.3. The Current Study
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.3. Measures
2.4. Statistical Analysis
3. Results
3.1. Descriptive and Correlation Analysis
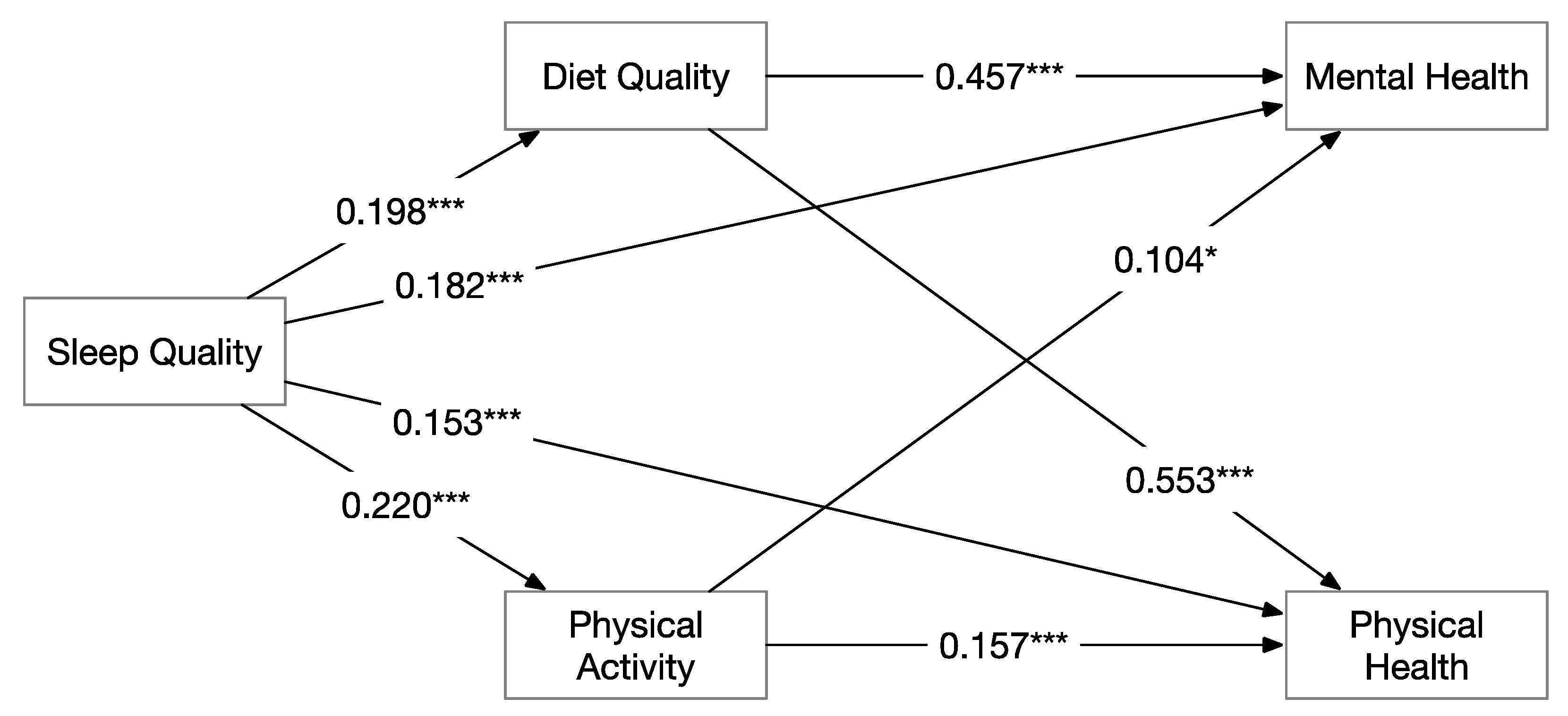
3.2. Mediation Analysis
3.3. Mental Health
3.4. Physical Health
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Textor, C. Aging Population in China—Statistics & Facts. Available online: https://www.statista.com/topics/6000/aging-population-in-china/ (accessed on 1 March 2021).
- Ford, D.W.; Hartman, T.J.; Still, C.; Wood, C.; Mitchell, D.C.; Erickson, P.; Bailey, R.; Smiciklas-Wright, H.; Coffman, N.L.; Jensen, G.L. Body Mass index, poor diet quality, and health-related quality of life are associated with mortality in rural older adults. J. Nutr. Gerontol. Geriatr. 2014, 33, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Evans, W.J. Nutrition, physical activity, and quality of life in older adults: Summary. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2001, 56, 89–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mamalaki, E.; Anastasiou, C.A.; Ntanasi, E.; Tsapanou, A.; Kosmidis, M.H.; Dardiotis, E.; Hadjigeorgiou, G.M.; Sakka, P.; Scarmeas, N.; Yannakoulia, M. Associations between the mediterranean diet and sleep in older adults: Results from the hellenic longitudinal investigation of aging and diet study. Geriatr. Gerontol. Int. 2018, 18, 1543–1548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsapanou, A.; Gu, Y.; O’Shea, D.; Yannakoulia, M.; Kosmidis, M.; Dardiotis, E.; Hadjigeorgiou, G.; Sakka, P.; Stern, Y.; Scarmeas, N. Sleep quality and duration in relation to memory in the elderly: Initial results from the Hellenic Longitudinal Investigation of Aging and Diet. Neurobiol. Learn. Mem. 2017, 141, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Aminoff, M.J.; Boller, F.; Swaab, D.F. We spend about one-third of our life either sleeping or attempting to do so. Handbook Clin. Neurol. 2011, 98, vii. [Google Scholar]
- Murray, K.; Godbole, S.; Natarajan, L.; Full, K.; Hipp, J.A.; Glanz, K.; Mitchell, J.; Laden, F.; James, P.; Quante, M.; et al. The relations between sleep, time of physical activity, and time outdoors among adult women. PLoS ONE 2017, 12, e0182013. [Google Scholar] [CrossRef]
- Moraes, W.; Piovezan, R.; Poyares, D.; Bittencourt, L.R.; Santos-Silva, R.; Tufik, S. Effects of aging on sleep structure throughout adulthood: A population-based study. Sleep Med. 2014, 15, 401–409. [Google Scholar] [CrossRef]
- Stone, K.L.; Xiao, Q. Impact of poor sleep on physical and mental health in older women. Sleep Med. Clin. 2018, 13, 457–465. [Google Scholar] [CrossRef]
- Ramanathan, L.; Gulyani, S.; Nienhuis, R.; Siegel, J.M. Sleep deprivation decreases superoxide dismutase activity in rat hippocampus and brainstem. Neuro Rep. 2002, 13, 1387–1390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Süer, C.; Dolu, N.; Artis, A.S.; Sahin, L.; Yilmaz, A.; Cetin, A. The effects of long-term sleep deprivation on the long-term potentiation in the dentate gyrus and brain oxidation status in rats. Neurosci. Res. 2011, 70, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Thamaraiselvi, K.; Mathangi, D.; Subhashini, A. Effect of increase in duration of REM sleep deprivation on lipid peroxidation. Int. J. Biol. Med. Res. 2012, 3, 1754–1759. [Google Scholar]
- Lucassen, P.J.; Meerlo, P.; Naylor, A.S.; Van Dam, A.M.; Dayer, A.G.; Fuchs, E.; Oomen, C.A.; Czéh, B. Regulation of adult neurogenesis by stress, sleep disruption, exercise and inflammation: Implications for depression and antidepressant action☆. Eur. Neuropsychopharmacol. 2010, 20, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Meerlo, P.; Mistlberger, R.E.; Jacobs, B.L.; Heller, H.C.; McGinty, D. New neurons in the adult brain: The role of sleep and consequences of sleep loss. Sleep Med. Rev. 2009, 13, 187–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novati, A.; Hulshof, H.; Koolhaas, J.; Lucassen, P.; Meerlo, P. Chronic sleep restriction causes a decrease in hippocampal volume in adolescent rats, which is not explained by changes in glucocorticoid levels or neurogenesis. Neuroscience 2011, 190, 145–155. [Google Scholar] [CrossRef]
- Yuan, Y.; Li, J.; Jing, Z.; Yu, C.; Zhao, D.; Hao, W.; Zhou, C. The role of mental health and physical activity in the association between sleep quality and quality of life among rural elderly in China: A moderated mediation model. J. Affect. Disord. 2020, 273, 462–467. [Google Scholar] [CrossRef]
- Simopoulos, A.P. Nutrition and Fitness: Mental Health, Aging, and the Implementation of a Healthy Diet and Physical Activity Lifestyle; Karger Medical and Scientific Publishers: Basel, Switzerland, 2005; Volume 2. [Google Scholar]
- Phillips, C. Lifestyle modulators of neuroplasticity: How physical activity, mental engagement, and diet promote cognitive health during aging. Neural Plast. 2017, 2017, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Popovic, S.; Masanovic, B. Effects of Physical Activity and Social Activity on Physical Health and Social Inclusion of Elderly People. Iran. J. Public Health 2020, 48, 1922–1923. [Google Scholar] [CrossRef]
- Hosker, D.K.; Elkins, R.M.; Potter, M.P. Promoting mental health and wellness in youth through physical activity, nutrition, and sleep. Child Adolesc. Psychiatr. Clin. N. Am. 2019, 28, 171–193. [Google Scholar] [CrossRef]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef]
- Shephard, R.J. Aging, physical activity, and health. Int. Encycl. Public Health 2017, 31–37. [Google Scholar] [CrossRef]
- Koolhaas, C.M.; Dhana, K.; van Rooij, F.J.A.; Schoufour, J.D.; Hofman, A.; Franco, O.H. Physical activity types and health-related quality of life among middle-aged and elderly adults: The Rotterdam Study. J. Nutr. Health Aging 2018, 22, 246–253. [Google Scholar] [CrossRef]
- Lok, N.; Lok, S.; Canbaz, M. The effect of physical activity on depressive symptoms and quality of life among elderly nursing home residents: Randomized controlled trial. Arch. Gerontol. Geriatr. 2017, 70, 92–98. [Google Scholar] [CrossRef]
- Wu, I.H.; Nguyen, N.; Balachandran, D.D.; Lu, Q.; McNeill, L.H. Sleep and obesity: The mediating role of health behaviors among African Americans. Sleep Health 2019, 5, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Günther, A.L.; Liese, A.D.; Bell, R.A.; Dabelea, D.; Lawrence, J.M.; Rodriguez, B.L.; Standiford, D.A.; Mayer-Davis, E.J. Association Between the Dietary Approaches to Hypertension Diet and Hypertension in Youth With Diabetes Mellitus. Hypertension 2009, 53, 6–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urpi-Sarda, M.; Casas, R.; Chiva-Blanch, G.; Romero-Mamani, E.S.; Valderas-Martínez, P.; Arranz, S.; Andres-Lacueva, C.; Llorach, R.; Medina-Remón, A.; Lamuela-Raventos, R.M.; et al. Virgin olive oil and nuts as key foods of the Mediterranean diet effects on inflammatory biomarkers related to atherosclerosis. Pharmacol. Res. 2012, 65, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, R.W.; Linde, J.A.; Simon, G.E.; Ludman, E.J.; Rohde, P.; Ichikawa, L.E.; Finch, E.A. Reported food choices in older women in relation to body mass index and depressive symptoms. Appetite 2009, 52, 238–240. [Google Scholar] [CrossRef] [Green Version]
- Jansen, E.C.; Dunietz, G.L.; Tsimpanouli, M.-E.; Guyer, H.M.; Shannon, C.; Hershner, S.D.; O’Brien, L.M.; Baylin, A. Sleep, Diet, and cardiometabolic health investigations: A systematic review of analytic strategies. Curr. Nutr. Rep. 2018, 7, 235–258. [Google Scholar] [CrossRef]
- Lopresti, A.L.; Hood, S.D.; Drummond, P.D. A review of lifestyle factors that contribute to important pathways associated with major depression: Diet, sleep and exercise. J. Affect. Disord. 2013, 148, 12–27. [Google Scholar] [CrossRef] [Green Version]
- St-Onge, M.-P.; Wolfe, S.; Sy, M.; Shechter, A.; Hirsch, J. Sleep restriction increases the neuronal response to unhealthy food in normal-weight individuals. Int. J. Obes. 2014, 38, 411–416. [Google Scholar] [CrossRef] [Green Version]
- Taheri, S.; Lin, L.; Austin, D.; Young, T.; Mignot, E. Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index. PLoS Med. 2004, 1, e62. [Google Scholar] [CrossRef]
- Chaput, J.-P. Sleep patterns, diet quality and energy balance. Physiol. Behav. 2014, 134, 86–91. [Google Scholar] [CrossRef]
- Al-Disi, D.; Al-Daghri, N.; Khanam, L.; Al-Othman, A.; Al-Saif, M.; Sabico, S.; Chrousos, G. Subjective sleep duration and quality influence diet composition and circulating adipocytokines and ghrelin levels in teen-age girls. Endocr. J. 2010, 57, 915–923. [Google Scholar] [CrossRef] [Green Version]
- Chaput, J.-P.; Klingenberg, L.; Rosenkilde, M.; Gilbert, J.-A.; Tremblay, A.; Sjödin, A. Physical activity plays an important role in body weight regulation. J. Obes. 2010, 2011, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhodes, R.E.; Janssen, I.; Bredin, S.S.; Warburton, D.E.; Bauman, A. Physical activity: Health impact, prevalence, correlates and interventions. Psychol. Health 2017, 32, 942–975. [Google Scholar] [CrossRef] [PubMed]
- Vallance, J.K.; Winkler, E.A.; Gardiner, P.A.; Healy, G.N.; Lynch, B.M.; Owen, N. Associations of objectively-assessed physical activity and sedentary time with depression: NHANES (2005–2006). Prev. Med. 2011, 53, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Foti, K.E.; Eaton, D.K.; Lowry, R.; McKnight-Ely, L.R. Sufficient Sleep, Physical Activity, and Sedentary Behaviors. Am. J. Prev. Med. 2011, 41, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Kilani, H.; Al-Hazzaa, H.; Waly, M.I.; Musaiger, A. Lifestyle habits: Diet, physical activity and sleep duration among Omani adolescents = عاداتنمطالحياة: الغذاءوالنشاطالبدنيومدةالنومبينالمراهقينالعمانيين. Sultan Qaboos Univ. Med. J. [SQUMJ] 2013, 13, 510–519. [Google Scholar] [CrossRef] [PubMed]
- Oftedal, S.; Vandelanotte, C.; Duncan, M.J. Patterns of diet, physical activity, sitting and sleep are associated with socio-demographic, behavioural, and health-risk indicators in adults. Int. J. Environ. Res. Public Health 2019, 16, 2375. [Google Scholar] [CrossRef] [Green Version]
- Li, X.-D.; Cao, H.-J.; Xie, S.-Y.; Li, K.-C.; Tao, F.-B.; Yang, L.-S.; Zhang, J.-Q.; Bao, Y.-S. Adhering to a vegetarian diet may create a greater risk of depressive symptoms in the elderly male Chinese population. J. Affect. Disord. 2019, 243, 182–187. [Google Scholar] [CrossRef]
- Li, J.; Yao, Y.-S.; Dong, Q.; Dong, Y.-H.; Liu, J.-J.; Yang, L.-S.; Huang, F. Characterization and factors associated with sleep quality among rural elderly in China. Arch. Gerontol. Geriatr. 2013, 56, 237–243. [Google Scholar] [CrossRef]
- Liu, Y.; Dong, Y.; Li, X.; Mao, X.; Peng, G.; Liu, L. Meta-analysis of the prevalence of sleep disorder among Chinese elderly aged 60 years and over. Modern Prev. Med. 2014, 41, 1442–1445. [Google Scholar]
- Miner, B.; Kryger, M.H. Sleep in the Aging Population. Sleep Med. Clin. 2017, 12, 31–38. [Google Scholar] [CrossRef] [Green Version]
- Asp, M.; Simonsson, B.; Larm, P.; Molarius, A. Physical mobility, physical activity, and obesity among elderly: Findings from a large population-based Swedish survey. Public Health 2017, 147, 84–91. [Google Scholar] [CrossRef]
- Thomas, K.M.; Redd, L.A.; Wright, J.D.; Hartos, J.L. Sleep and mental health in the general population of elderly women. J. Prim. Prev. 2017, 38, 495–503. [Google Scholar] [CrossRef]
- Torres, S.J.; Robinson, S.; Orellana, L.; O’Connell, S.L.; Grimes, C.A.; Mundell, N.L.; Dunstan, D.W.; Nowson, C.A.; Daly, R.M. Effects of progressive resistance training combined with a protein-enriched lean red meat diet on health-related quality of life in elderly women: Secondary analysis of a 4-month cluster randomised controlled trial. Br. J. Nutr. 2017, 117, 1550–1559. [Google Scholar] [CrossRef]
- Strahler, J.; Haddad, C.; Salameh, P.; Sacre, H.; Obeid, S.; Hallit, S. Cross-cultural differences in orthorexic eating behaviors: Associations with personality traits. Nutrition 2020, 77, 110811. [Google Scholar] [CrossRef]
- Zhou, B.F.; Cooperative Meta-Analysis Group of the Working Group on Obesity in, C. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults—Study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomed. Environ. Sci. 2002, 15, 83–96. [Google Scholar]
- Li, Z.; Sun, D.; Cuj, H.; Zhang, L.; Lju, P.; Yang, H.; Baj, J. Refractive error among the elderly in rural southern Harbin, China. Ophthalmic Epidemiol. 2009, 16, 388–394. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Zhao, Y.; Zhang, H.; Lin, Z. Orthorexia nervosa is associated with positive body image and life satisfaction in Chinese elderly: Evidence for a positive psychology perspective. Int. J. Eat. Disord. 2021, 54, 212–221. [Google Scholar] [CrossRef]
- Galesic, M.; Bosnjak, M. Effects of Questionnaire Length on Participation and Indicators of Response Quality in a Web Survey. Public Opin. Q. 2009, 73, 349–360. [Google Scholar] [CrossRef]
- Lee, H.; Baniqued, P.L.; Cosman, J.; Mullen, S.; McAuley, E.; Severson, J.; Kramer, A.F. Examining cognitive function across the lifespan using a mobile application. Comput. Hum. Behav. 2012, 28, 1934–1946. [Google Scholar] [CrossRef]
- McAvinue, L.P.; Habekost, T.; Johnson, K.A.; Kyllingsbæk, S.; Vangkilde, S.; Bundesen, C.; Robertson, I.H. Sustained attention, attentional selectivity, and attentional capacity across the lifespan. Atten. Percept. Psychophys. 2012, 74, 1570–1582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, Y.; Xin, M.; Zhang, C.; Dong, W.; Fang, Y.; Wu, W.; Li, M.; Pang, J.; Zheng, Z.; Wang, Z.; et al. Associations of mental health and personal preventive measure compliance with exposure to Covid-19 information during work resumption following the Covid-19 outbreak in china: Cross-sectional survey study. J. Med. Internet Res. 2020, 22, e22596. [Google Scholar] [CrossRef] [PubMed]
- Snyder, E.; Cai, B.; DeMuro, C.; Morrison, M.F.; Ball, W. A new single-item sleep quality scale: Results of psychometric evaluation in patients with chronic primary insomnia and depression. J. Clin. Sleep Med. 2018, 14, 1849–1857. [Google Scholar] [CrossRef] [Green Version]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Loftfield, E.; Yi, S.; Immerwahr, S.; Eisenhower, D. Construct validity of a single-item, self-rated question of diet quality. J. Nutr. Educ. Behav. 2015, 47, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Carbonneau, E.; Lamarche, B.; Lafrenière, J.; Robitaille, J.; Provencher, V.; Desroches, S.; Corneau, L.; Lemieux, S. Are French Canadians able to accurately self-rate the quality of their diet? Insights from the PREDISE study. Appl. Physiol. Nutr. Metab. 2019, 44, 293–300. [Google Scholar] [CrossRef]
- Brislin, R.W. Back-translation for cross-cultural research. J. Cross-Cult. Psychol. 1970, 1, 185–216. [Google Scholar] [CrossRef]
- Milton, K.; Bull, F.C.; Bauman, A. Reliability and validity testing of a single-item physical activity measure. Br. J. Sports Med. 2010, 45, 203–208. [Google Scholar] [CrossRef]
- Hays, R.D.; Schalet, B.D.; Spritzer, K.L.; Cella, D. Two-item PROMIS® global physical and mental health scales. J. Patient Rep. Outcomes 2017, 1, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Rosseel, Y. Lavaan: An R package for structural equation modeling and more. Version 0.5–12 (BETA). J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Gerino, E.; Rollè, L.; Sechi, C.; Brustia, P. Loneliness, resilience, mental health, and quality of life in old age: A structural equation model. Front. Psychol. 2017, 8, 2003. [Google Scholar] [CrossRef]
- Baldwin, C.M.; Griffith, K.A.; Nieto, F.J.; O’Connor, G.T.; Walsleben, J.A.; Redline, S. The association of sleep-disordered breathing and sleep symptoms with quality of life in the Sleep Heart Health Study. Sleep 2001, 24, 96–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, K.; Clarke, D. Longitudinal trends in late-life insomnia: Implications for prescribing. Age Ageing 1997, 26, 179–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cespedes, E.M.; Hu, F.B.; Redline, S.; Rosner, B.; Alcantara, C.; Cai, J.; Hall, M.H.; Loredo, J.S.; Mossavar-Rahmani, Y.; Ramos, A.R.; et al. Comparison of self-reported sleep duration with actigraphy: Results from the hispanic community health study/study of Latinos Sueño ancillary study. Am. J. Epidemiol. 2016, 183, 561–573. [Google Scholar] [CrossRef]
- Yeh, S.-S.S.; Brown, R.F. Disordered eating partly mediates the relationship between poor sleep quality and high body mass index. Eat. Behav. 2014, 15, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Kanagasabai, T.; Ardern, C.I. Contribution of inflammation, oxidative stress, and antioxidants to the relationship between sleep duration and cardiometabolic health. Sleep 2015, 38, 1905–1912. [Google Scholar] [CrossRef]
- Harman, D. Aging: Overview. Ann. N. Y. Acad. Sci. 2006, 928, 1–21. [Google Scholar] [CrossRef]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Mâsse, L.C.; Tilert, T.; Mcdowell, M. Physical activity in the United States measured by accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y. Monitoring Sleep Quality Using Smartwatches; Pennsylvania State University: University Park, PA, USA, 2020. [Google Scholar]
- Patterson, R.E.; Haines, P.S.; Popkin, B.M. Diet quality index: Capturing a multidimensional behavior. J. Am. Diet. Assoc. 1994, 94, 57–64. [Google Scholar] [CrossRef]
- Gardner, D.G.; Cummings, L.L.; Dunham, R.B.; Pierce, J.L. Single-item versus multiple-item measurement scales: An empirical comparison. Educ. Psychol. Meas. 1998, 58, 898–915. [Google Scholar] [CrossRef]
- Bergkvist, L. Appropriate use of single-item measures is here to stay. Mark. Lett. 2015, 26, 245–255. [Google Scholar] [CrossRef]
- Fuchs, C.; Diamantopoulos, A. Using single-item measures for construct measurement in management research: Conceptual issues and application guidelines. Die Betr. 2009, 69, 195. [Google Scholar]



{kind=link}
{kind=link}
| Males (N = 151) | Females (N = 162) | Overall Percent (%) | |
|---|---|---|---|
| Education | |||
| Primary school or less | 15 | 23 | 12.4 |
| Junior high | 29 | 44 | 23.8 |
| Senior high | 81 | 67 | 48.2 |
| Undergraduate | 22 | 22 | 14.3 |
| Postgraduate or above | 4 | 1.3 | |
| Marriage | |||
| Married | 132 | 113 | 78.5 |
| Other | 19 | 48 | 21.5 |
| Residence | |||
| City | 120 | 114 | 75.0 |
| Rural | 31 | 47 | 25.0 |
| Ethnicity | |||
| Han | 129 | 111 | 76.7 |
| Minorities | 22 | 51 | 23.3 |
| Hypertension | |||
| Yes | 71 | 65 | 43.6 |
| No | 79 | 97 | 56.4 |
| Diabetes | |||
| Yes | 39 | 45 | 26.9 |
| No | 111 | 117 | 73.1 |
| M/n% | SD | |
|---|---|---|
| Sex (1 = male; 2 = female) | 48.2 (males) | - |
| Age | 67.9 | 7.95 |
| BMI | 22.70 | 3.36 |
| Sleep quality Diet quality Physical activity Mental health Physical health | 7.06 | 2.58 |
| 3.23 | 1.02 | |
| 5.08 | 2.39 | |
| 48.29 | 9.77 | |
| 45.72 | 9.21 |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| 1. Sex | 1 | |||||||
| 2. Age | −0.058 | 1 | ||||||
| 3. BMI | −0.126 * | 0.005 | 1 | |||||
| 4. Sleep quality | −0.073 | 0.068 | −0.086 | 1 | ||||
| 5. Diet quality | 0.010 | −0.032 | −0.074 | 0.216 *** | 1 | |||
| 6. Physical activity | −0.014 | −0.004 | −0.217 *** | 0.226 *** | 0.240 *** | 1 | ||
| 7. Mental health | −0.072 | 0.032 | −0.202 *** | 0.319 *** | 0.637 *** | 0.332 *** | 1 | |
| 8. Physical health | −0.058 | 0.068 | −0.224 *** | 0.317 *** | 0.545 *** | 0.265 *** | 0.729 *** | 1 |
| Point Estimates | SE | Bootstrapping 95%CI | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Direct effect | 0.182 *** | 0.053 | 0.079 | 0.291 |
| Path 1 | ||||
| Sleep quality | 0.091 ** | 0.03 | 0.038 | 0.154 |
| Diet quality | ||||
| Mental health | ||||
| Path 2 | ||||
| Sleep quality | 0.023 | 0.012 | 0.004 | 0.053 |
| Physical activity | ||||
| Mental health | ||||
| Total effect | 0.296 *** | 0.056 | 0.184 | 0.405 |
| Point Estimates | SE | Bootstrapping 95%CI | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Direct effect | 0.153 *** | 0.048 | 0.056 | 0.246 |
| Path 1 | ||||
| Sleep quality | 0.110 *** | 0.033 | 0.047 | 0.177 |
| Diet quality | ||||
| Mental health | ||||
| Path 2 | ||||
| Sleep quality | 0.035 ** | 0.013 | 0.014 | 0.068 |
| Physical activity | ||||
| Mental health | ||||
| Total effect | 0.297 *** | 0.056 | 0.190 | 0.408 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Y.; Song, J.; Brytek-Matera, A.; Zhang, H.; He, J. The Relationships between Sleep and Mental and Physical Health of Chinese Elderly: Exploring the Mediating Roles of Diet and Physical Activity. Nutrients 2021, 13, 1316. https://doi.org/10.3390/nu13041316
Zhao Y, Song J, Brytek-Matera A, Zhang H, He J. The Relationships between Sleep and Mental and Physical Health of Chinese Elderly: Exploring the Mediating Roles of Diet and Physical Activity. Nutrients. 2021; 13(4):1316. https://doi.org/10.3390/nu13041316
Chicago/Turabian StyleZhao, Yiqing, Jianwen Song, Anna Brytek-Matera, Hengyue Zhang, and Jinbo He. 2021. "The Relationships between Sleep and Mental and Physical Health of Chinese Elderly: Exploring the Mediating Roles of Diet and Physical Activity" Nutrients 13, no. 4: 1316. https://doi.org/10.3390/nu13041316
APA StyleZhao, Y., Song, J., Brytek-Matera, A., Zhang, H., & He, J. (2021). The Relationships between Sleep and Mental and Physical Health of Chinese Elderly: Exploring the Mediating Roles of Diet and Physical Activity. Nutrients, 13(4), 1316. https://doi.org/10.3390/nu13041316