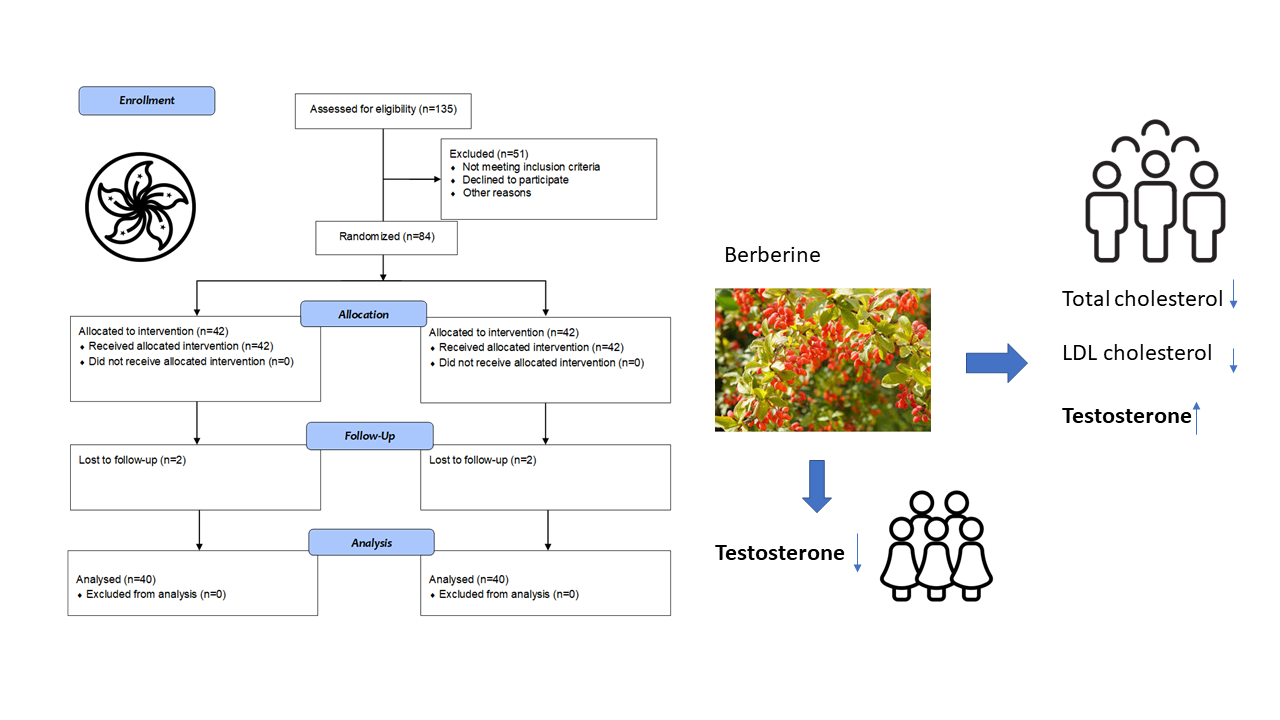
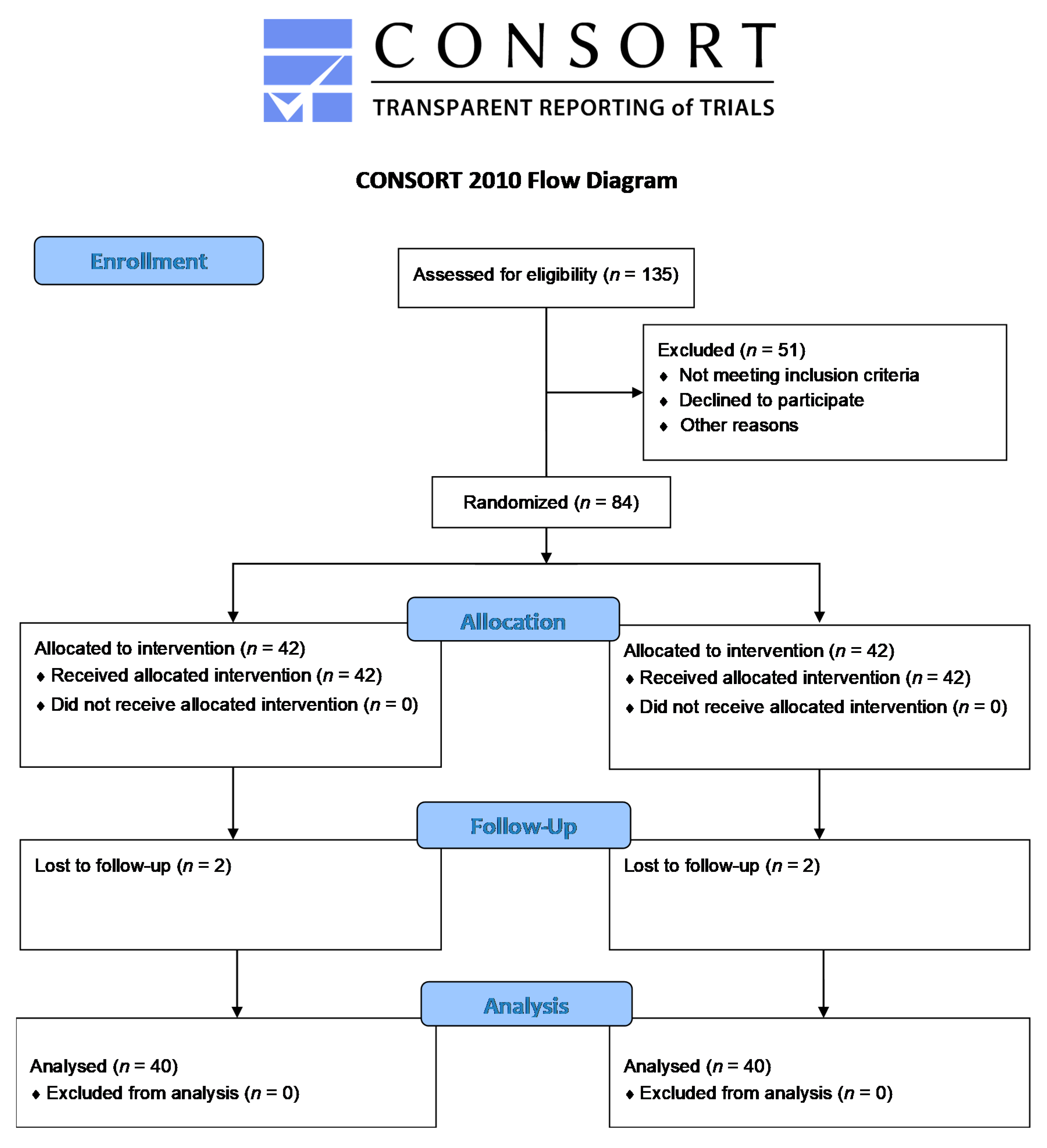
Effect of Berberine on Cardiovascular Disease Risk Factors: A Mechanistic Randomized Controlled Trial



 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Subjects
2.3. Ethical Considerations
2.4. Intervention and Study Outcomes
2.5. Randomization, Allocation Concealment and Blinding
2.6. Data Collection
2.7. Biochemical Assessment
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mauvais-Jarvis, F.; Merz, N.B.; Barnes, P.J.; Brinton, R.D.; Carrero, J.J.; De Meo, D.L.; De Vries, G.J.; Epperson, C.N.; Govindan, R.; Klein, S.L.; et al. Sex and gender: Modifiers of health, disease, and medicine. Lancet 2020, 396, 565–582. [Google Scholar] [CrossRef]
- Nikiforov, S.V.; Mamaev, V.B. The development of sex differences in cardiovascular disease mortality: A historical perspective. Am. J. Public Health 1998, 88, 1348–1353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, N.; Atar, D.; Borentain, M.; Breithardt, G.; van Eickels, M.; Endres, M.; Fraass, U.; Friede, T.; Hannachi, H.; Janmohamed, S.; et al. Improving clinical trials for cardiovascular diseases: A position paper from the Cardiovascular Round Table of the European Society of Cardiology. Eur. Heart J. 2016, 37, 747–754. [Google Scholar] [CrossRef] [Green Version]
- Imanshahidi, M.; Hosseinzadeh, H. Pharmacological and therapeutic effects of Berberis vulgaris and its active constituent, berberine. Phytother. Res. 2008, 22, 999–1012. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Chopra, K.E.; Mukherjee, M.; Pottabathini, R.; Dhull, D.K. Current knowledge and pharmacological profile of berberine: An update. Eur. J. Pharmacol. 2015, 761, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.S.; Zhang, J.H.; Feng, R.; Jin, X.Y.; Yang, F.W.; Ji, Z.C.; Zhao, M.Y.; Zhang, M.Y.; Zhang, B.L.; Li, X.M. Efficacy and Safety of Berberine Alone or Combined with Statins for the Treatment of Hyperlipidemia: A Systematic Review and Meta-Analysis of Randomized Controlled Clinical Trials. Am. J. Chin. Med. 2019, 47, 751–767. [Google Scholar] [CrossRef]
- Derosa, G.; D’Angelo, A.; Bonaventura, A.; Bianchi, L.; Romano, D.; Maffioli, P. Effects of berberine on lipid profile in subjects with low cardiovascular risk. Expert Opin. Biol. Ther. 2013, 13, 475–482. [Google Scholar] [CrossRef]
- Lan, J.; Zhao, Y.; Dong, F.; Yan, Z.; Zheng, W.; Fan, J.; Sun, G. Meta-analysis of the effect and safety of berberine in the treatment of type 2 diabetes mellitus, hyperlipemia and hypertension. J. Ethnopharmacol. 2015, 161, 69–81. [Google Scholar] [CrossRef]
- Derosa, G.; Maffioli, P.; Cicero, A.F. Berberine on metabolic and cardiovascular risk factors: An analysis from preclinical evidences to clinical trials. Expert Opin. Biol. Ther. 2012, 12, 1113–1124. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.; Li, K.; Guan, F.; Yao, F.; Yu, Y.; Zhang, M.; Hatch, G.M.; Chen, L. Berberine Pretreatment Confers Cardioprotection Against Ischemia-Reperfusion Injury in a Rat Model of Type 2 Diabetes. J. Cardiovasc. Pharmacol. Ther. 2016, 21, 486–494. [Google Scholar] [CrossRef]
- Richter, E.A.; Ruderman, N.B. AMPK and the biochemistry of exercise: Implications for human health and disease. Biochem. J. 2009, 418, 261–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skarydova, L.; Hofman, J.; Chlebek, J.; Havrankova, J.; Kosanova, K.; Skarka, A.; Hostalkova, A.; Plucha, T.; Cahlikova, L.; Wsol, V. Isoquinoline alkaloids as a novel type of AKR1C3 inhibitors. J. Steroid Biochem. Mol. Biol. 2014, 143, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Petitti, D. Commentary: Hormone replacement therapy and coronary heart disease: Four lessons. Int. J. Epidemiol. 2004, 33, 461–463. [Google Scholar] [CrossRef] [Green Version]
- Luo, S.; Yeung, S.L.A.; Zhao, J.V.; Burgess, S.; Schooling, C.M. Association of genetically predicted testosterone with thromboembolism, heart failure, and myocardial infarction: Mendelian randomisation study in UK Biobank. BMJ 2019, 364, l476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemaitre, J.F.; Berger, V.; Bonenfant, C.; Douhard, M.; Gamelon, M.; Plard, F.; Gaillard, J.M. Early-late life trade-offs and the evolution of ageing in the wild. Proc. R. Soc. 2015, 282, 20150209. [Google Scholar] [CrossRef]
- Schooling, C.M. Could androgens be relevant to partly explain why men have lower life expectancy than women? J. Epidemiol. Community Health 2016, 70, 324–328. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.; Jiang, C.; Lam, T.H.; Liu, B.; Cheng, K.K.; Xu, L.; Long, M.J.; Zhang, W.; Leung, G.M.; Schooling, C.M. Genetically predicted testosterone and electrocardiographic QT interval duration in Chinese: A Mendelian randomization analysis in the Guangzhou Biobank Cohort Study. Int. J. Epidemiol. 2015, 44, 613–620. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.; Jiang, C.; Lam, T.H.; Liu, B.; Cheng, K.K.; Xu, L.; Yeung, S.L.A.; Zhang, W.; Leung, G.M.; Schooling, C.M. Genetically predicted testosterone and cardiovascular risk factors in men: A Mendelian randomization analysis in the Guangzhou Biobank Cohort Study. Int. J. Epidemiol. 2014, 43, 140–148. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Balsells, M.M.; Murad, M.H.; Lane, M.; Lampropulos, J.F.; Albuquerque, F.; Mullan, R.J.; Agrwal, N.; Elamin, M.B.; Gallegos-Orozco, J.F.; Wang, A.T.; et al. Clinical review 1: Adverse effects of testosterone therapy in adult men: A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2010, 95, 2560–2575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, L.; Schooling, C.M. Differential risks in men and women for first and recurrent venous thrombosis: The role of genes and environment: Comment. J. Thromb. Haemost. 2015, 13, 884–886. [Google Scholar] [CrossRef] [Green Version]
- Ajayi, A.A.; Mathur, R.; Halushka, P.V. Testosterone increases human platelet thromboxane A2 receptor density and aggregation responses. Circulation 1995, 91, 2742–2747. [Google Scholar] [CrossRef]
- Ajayi, A.A.; Halushka, P.V. Castration reduces platelet thromboxane A2 receptor density and aggregability. QJM 2005, 98, 349–356. [Google Scholar] [CrossRef] [Green Version]
- An, Y.; Sun, Z.; Zhang, Y.; Liu, B.; Guan, Y.; Lu, M. The use of berberine for women with polycystic ovary syndrome undergoing IVF treatment. Clin. Endocrinol. 2014, 80, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Ju, J.Q.; Li, J.E.; Lin, Q.; Xu, H. Efficacy and safety of berberine for dyslipidaemias: A systematic review and meta-analysis of randomized clinical trials. Phytomedicine 2018, 50, 25–34. [Google Scholar] [CrossRef]
- Xiong, P.; Niu, L.; Talaei, S.; Kord-Varkaneh, H.; Clark, C.C.T.; Gaman, M.A.; Rahmani, J.; Dorosti, M.; Mousavi, S.M.; Zarezadeh, M.; et al. The effect of berberine supplementation on obesity indices: A dose- response meta-analysis and systematic review of randomized controlled trials. Complement. Ther. Clin. Pract. 2020, 39, 101113. [Google Scholar] [CrossRef]
- Mirzaee, F.; Razmjouei, P.; Shahrahmani, H.; Vafisani, F.; Najafi, M.N.; Ghazanfarpour, M. The effect and safety of Berberine on polycystic ovary syndrome: A systematic review. J. Obstet. Gynaecol. 2020, 41, 684–689. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.; Jin, X.; Liang, C.; Bu, F.; Pan, D.; He, Q.; Ming, Y.; Little, P.; Du, H.; Liang, S.; et al. Berberine for diarrhea in children and adults: A systematic review and meta-analysis. Ther. Adv. Gastroenterol. 2020, 13, 1756284820961299. [Google Scholar] [CrossRef]
- Moran, A.E.; Forouzanfar, M.H.; Roth, G.A.; Mensah, G.A.; Ezzati, M.; Flaxman, A.; Murray, C.J.; Naghavi, M. The global burden of ischemic heart disease in 1990 and 2010: The Global Burden of Disease 2010 study. Circulation 2014, 129, 1493–1501. [Google Scholar] [CrossRef] [PubMed]
- Wittes, J. Sample size calculations for randomized controlled trials. Epidemiol. Rev. 2002, 24, 39–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, B. How to calculate sample size in randomized controlled trial? J. Thorac. Dis. 2009, 1, 51–54. [Google Scholar]
- Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, X.; Zou, D.; Liu, W.; Yang, J.; Zhu, N.; Huo, L.; Wang, M.; Hong, J.; Wu, P.; et al. Treatment of type 2 diabetes and dyslipidemia with the natural plant alkaloid berberine. J. Clin. Endocrinol. Metab. 2008, 93, 2559–2565. [Google Scholar] [CrossRef] [Green Version]
- Cochrane Handbook. Available online: https://handbook-5-1.cochrane.org/chapter_16/16_2_1_introduction.htm (accessed on 6 July 2021).
- Albert, P.S. Longitudinal data analysis (repeated measures) in clinical trials. Stat. Med. 1999, 18, 1707–1732. [Google Scholar] [CrossRef]
- Hanley, J.A.; Negassa, A.; Edwardes, M.D.; Forrester, J.E. Statistical analysis of correlated data using generalized estimating equations: An orientation. Am. J. Epidemiol. 2003, 157, 364–375. [Google Scholar] [CrossRef]
- Richardson, T.G.; Sanderson, E.; Palmer, T.M.; Ala-Korpela, M.; Ference, B.A.; Smith, G.D.; Holmes, M.V. Evaluating the relationship between circulating lipoprotein lipids and apolipoproteins with risk of coronary heart disease: A multivariable Mendelian randomisation analysis. PLoS Med. 2020, 17, e1003062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glavinovic, T.; Sniderman, A.D. Apolipoprotein B: The Rosetta Stone of lipidology. Curr. Opin. Endocrinol. Diabetes Obes. 2021, 28, 90–96. [Google Scholar] [CrossRef]
- Wei, W.; Zhao, H.; Wang, A.; Sui, M.; Liang, K.; Deng, H.; Ma, Y.; Zhang, Y.; Zhang, H.; Guan, Y. A clinical study on the short-term effect of berberine in comparison to metformin on the metabolic characteristics of women with polycystic ovary syndrome. Eur. J. Endocrinol. 2012, 166, 99–105. [Google Scholar] [CrossRef] [Green Version]
- Luo, S. An Investigation of Metformin’s Etiological Role in Major Chronic Diseases Using Mendelian Randomization; HKU: Hong Kong, China, 2020. [Google Scholar]
- Ruth, K.S.; Day, F.R.; Tyrrell, J.; Thompson, D.J.; Wood, A.R.; Mahajan, A.; Beaumont, R.N.; Wittemans, L.; Martin, S.; Busch, A.S.; et al. Using human genetics to understand the disease impacts of testosterone in men and women. Nat. Med. 2020, 26, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Perez-Rubio, K.G.; Gonzalez-Ortiz, M.; Martinez-Abundis, E.; Robles-Cervantes, J.A.; Espinel-Bermudez, M.C. Effect of berberine administration on metabolic syndrome, insulin sensitivity, and insulin secretion. Metab. Syndr. Relat. Disord. 2013, 11, 366–369. [Google Scholar] [CrossRef] [PubMed]
- Bartz, D.; Chitnis, T.; Kaiser, U.B.; Rich-Edwards, J.W.; Rexrode, K.M.; Pennell, P.B.; Goldstein, J.M.; O’Neal, M.A.; LeBoff, M.; Behn, M.; et al. Clinical Advances in Sex- and Gender-Informed Medicine to Improve the Health of All: A Review. JAMA Intern. Med. 2020, 180, 574–583. [Google Scholar] [CrossRef]
- Gu, Y.; Zhang, Y.; Shi, X.; Li, X.; Hong, J.; Chen, J.; Gu, W.; Lu, X.; Xu, G.; Ning, G. Effect of traditional Chinese medicine berberine on type 2 diabetes based on comprehensive metabonomics. Talanta 2010, 81, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Lopez, P.M.; Subramanian, S.V.; Schooling, C.M. Effect measure modification conceptualized using selection diagrams as mediation by mechanisms of varying population-level relevance. J. Clin. Epidemiol. 2019, 113, 123–128. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristics | Number (Percentage) or Mean (SD) * | |
|---|---|---|
| Berberine Group | Placebo Group | |
| Place of birth | ||
| - Hong Kong | 36 (90%) | 33 (82.5%) |
| - Macau | 0 (0%) | 2 (5%) |
| - Mainland China | 4 (10%) | 5 (12.5%) |
| Education level | ||
| - Primary school | 6 (15.0%) | 7 (17.5%) |
| - High school | 25 (62.5%) | 20 (50%) |
| - University and above | 9 (22.5%) | 13 (32.5%) |
| Smoking status | ||
| - Non-smoker | 24 (60%) | 30 (75%) |
| - Ex-smoker | 12 (30%) | 5 (12.5%) |
| - Current smoker | 4 (10%) | 5 (12.5%) |
| Alcohol drinking | ||
| - Never | 6 (15.0%) | 8 (20%) |
| - Ex-drinker | 10 (25.0%) | 8 (20%) |
| - Less than 1 day per week | 15 (37.5%) | 15 (37.5%) |
| - 1–2 days per week | 3 (7.5%) | 7 (17.5%) |
| - 3–7 days per week | 6 (15%) | 2 (5%) |
| Age (year) | 49.5 (11.1) | 44.8 (13.5) |
| Physical activity | ||
| Time of doing vigorous physical activity per day (minutes) | 85.0 (43.7) | 71.0 (60.9) |
| Time of doing moderate physical activity per day (minutes) | 69.6 (51.0) | 76.8 (83.9) |
| Time of doing light physical activity per day (minutes) | 67.3 (61.2) | 60.0 (59.9) |
| Outcomes | Berberine (Mean (SD)) | Placebo (Mean (SD)) | Comparing the Changes in Two Groups (Change (Berberine)–Change (Placebo)) | ||||
|---|---|---|---|---|---|---|---|
| Baseline | 12-Week Treatment | Baseline | 12-Week Treatment | beta | 95% CI | p | |
| Total cholesterol (mmol/L) | 5.4 (0.9) | 4.9 (1.0) | 5.5 (1.1) | 5.4 (1.0) | −0.39 | −0.70, −0.08 | 0.02 |
| LDL-cholesterol (mmol/L) | 3.3 (0.8) | 3.0 (0.8) | 3.5 (1.0) | 3.4 (0.9) | −0.21 | −0.50, 0.08 | 0.15 |
| Triglycerides (mmol/L) | 1.9 (0.8) | 1.6 (0.9) | 1.8 (1.3) | 1.6 (1.0) | −0.08 | −0.37, 0.21 | 0.60 |
| HDL-cholesterol (mmol/L) | 1.17 (0.3) | 1.13 (0.3) | 1.21 (0.4) | 1.24 (0.4) | −0.07 | −0.13, −0.01 | 0.03 |
| SBP (mmHg) | 131 (16.8) | 130 (17.8) | 125 (12.7) | 125 (11.6) | −1.53 | −7.47, 4.41 | 0.62 |
| DBP (mmHg) | 88.3 (13.8) | 86.6 (13.0) | 82.1 (10.8) | 81.0 (9.0) | −0.58 | −4.52, 3.36 | 0.78 |
| BMI | 26.1 (3.8) | 26.0 (4.0) | 26.3 (3.7) | 26.5 (3.7) | −0.27 | −0.74, 0.20 | 0.26 |
| WHR | 0.93 (0.06) | 0.92 (0.06) | 0.91 (0.05) | 0.91 (0.06) | −0.01 | −0.03, 0.01 | 0.26 |
| Thromboxane A2 (pg/mL) | 188 (109) | 255 (162) | 198 (107) | 243 (138) | 21.46 | −21.7, 64.6 | 0.33 |
| Testosterone (nmol/L) | 14.3 (4.5) | 15.0 (4.6) | 15.8 (5.8) | 15.1 (5.4) | 1.43 | −0.10, 2.96 | 0.07 |
| Outcomes | Berberine (Mean (SD)) | Placebo (Mean (SD)) | Comparing the Changes in Two Groups (Change (Berberine)–Change (Placebo)) | ||||
|---|---|---|---|---|---|---|---|
| Baseline | 8-Week Treatment | Baseline | 8-Week Treatment | beta | 95% CI | p | |
| Total cholesterol (mmol/L) | 5.4 (0.9) | 4.6 (0.9) | 5.5 (1.1) | 5.1 (1.2) | −0.39 | −0.72, −0.06 | 0.03 |
| LDL-cholesterol (mmol/L) | 3.3 (0.8) | 2.9 (0.8) | 3.5 (1.0) | 3.3 (0.9) | −0.25 | −0.54, 0.04 | 0.11 |
| Triglycerides (mmol/L) | 1.9 (0.8) | 1.5 (0.8) | 1.8 (1.3) | 1.9 (2.2) | −0.53 | −1.22, 0.16 | 0.13 |
| HDL-cholesterol (mmol/L) | 1.17 (0.3) | 1.07 (0.3) | 1.21 (0.4) | 1.10 (0.5) | 0.01 | −0.09, 0.11 | 0.86 |
| SBP (mmHg) | 131 (16.8) | 129 (21.8) | 125 (12.7) | 124 (10.6) | −0.30 | −5.32, 4.72 | 0.91 |
| DBP (mmHg) | 88.3 (13.8) | 86.7 (16.7) | 82.1 (10.8) | 80.5 (12.3) | −0.05 | −4.83, 4.73 | 0.98 |
| BMI | 26.1 (3.8) | 25.5 (5.3) | 26.3 (3.7) | 26.2 (3.6) | −0.51 | −1.63, 0.61 | 0.38 |
| WHR | 0.93 (0.06) | 0.93 (0.06) | 0.91 (0.05) | 0.91 (0.05) | −0.001 | −0.02, 0.02 | 0.95 |
| Thromboxane A2 (pg/mL) | 188 (109) | 214 (104) | 198 (107) | 228 (145) | −4.5 | −51.1, 42.1 | 0.85 |
| Testosterone (nmol/L) | 14.3 (4.5) | 14.7 (4.7) | 15.8 (5.8) | 15.0 (5.2) | 1.19 | −0.18, 2.56 | 0.09 |
| Outcomes | Beta | 95% CI | p |
|---|---|---|---|
| Total cholesterol (mmol/L) | −0.39 | −0.62, −0.16 | 0.001 |
| LDL-cholesterol (mmol/L) | −0.23 | −0.43, −0.02 | 0.03 |
| Triglycerides (mmol/L) | −0.31 | −0.67, 0.06 | 0.10 |
| HDL-cholesterol (mmol/L) | −0.03 | −0.09, 0.02 | 0.26 |
| SBP (mmHg) | −0.91 | −4.75, 2.93 | 0.64 |
| DBP (mmHg) | −0.31 | −3.42, 2.80 | 0.84 |
| BMI | −0.39 | −0.99, 0.21 | 0.20 |
| WHR | −0.006 | −0.02, 0.01 | 0.36 |
| Thromboxane A2 (pg/mL) | 8.46 | −23.0, 39.9 | 0.60 |
| Testosterone (nmol/L) | 1.31 | 0.30, 2.33 | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, J.V.; Yeung, W.-F.; Chan, Y.-H.; Vackova, D.; Leung, J.Y.Y.; Ip, D.K.M.; Zhao, J.; Ho, W.-K.; Tse, H.-F.; Schooling, C.M. Effect of Berberine on Cardiovascular Disease Risk Factors: A Mechanistic Randomized Controlled Trial. Nutrients 2021, 13, 2550. https://doi.org/10.3390/nu13082550
Zhao JV, Yeung W-F, Chan Y-H, Vackova D, Leung JYY, Ip DKM, Zhao J, Ho W-K, Tse H-F, Schooling CM. Effect of Berberine on Cardiovascular Disease Risk Factors: A Mechanistic Randomized Controlled Trial. Nutrients. 2021; 13(8):2550. https://doi.org/10.3390/nu13082550
Chicago/Turabian StyleZhao, Jie V., Wai-Fung Yeung, Yap-Hang Chan, Dana Vackova, June Y. Y. Leung, Dennis K. M. Ip, Jiaxi Zhao, Wai-Kwan Ho, Hung-Fat Tse, and Catherine Mary Schooling. 2021. "Effect of Berberine on Cardiovascular Disease Risk Factors: A Mechanistic Randomized Controlled Trial" Nutrients 13, no. 8: 2550. https://doi.org/10.3390/nu13082550
APA StyleZhao, J. V., Yeung, W.-F., Chan, Y.-H., Vackova, D., Leung, J. Y. Y., Ip, D. K. M., Zhao, J., Ho, W.-K., Tse, H.-F., & Schooling, C. M. (2021). Effect of Berberine on Cardiovascular Disease Risk Factors: A Mechanistic Randomized Controlled Trial. Nutrients, 13(8), 2550. https://doi.org/10.3390/nu13082550