
Accuracy of the Simplified Nutritional Appetite Questionnaire for Malnutrition and Sarcopenia Screening among Older Patients Requiring Rehabilitation

 , , ,
, , ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurements
2.3. Appetite Assessment Tools: SNAQ and SNAQ-JE
2.4. Diagnosis of GLIM-Defined Malnutrition
2.5. Diagnosis of Sarcopenia
2.6. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Morley, J.E. Anorexia of aging: A true geriatric syndrome. J. Nutr. Health Aging 2012, 16, 422–425. [Google Scholar] [CrossRef]
- Wysokiński, A.; Sobów, T.; Kłoszewska, I.; Kostka, T. Mechanisms of the anorexia of aging—A review. Age 2015, 37, 9821. [Google Scholar] [CrossRef] [PubMed]
- Tsutsumimoto, K.; Doi, T.; Makizako, H.; Hotta, R.; Nakakubo, S.; Makino, K.; Suzuki, T.; Shimada, H. Aging-related anorexia and its association with disability and frailty. J. Cachexia Sarcopenia Muscle 2018, 9, 834–843. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E. Anorexia of ageing: A key component in the pathogenesis of both sarcopenia and cachexia. J. Cachexia Sarcopenia Muscle 2017, 8, 523–526. [Google Scholar] [CrossRef] [Green Version]
- Cox, N.J.; Ibrahim, K.; Sayer, A.A.; Robinson, S.M.; Roberts, H.C. Assessment and Treatment of the Anorexia of Aging: A Systematic Review. Nutrients 2019, 11, 144. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Jensen, G.L.; Cederholm, T.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; de Baptista, G.A.; Barazzoni, R.; Blaauw, R.; Coats, A.J.S.; et al. GLIM Criteria for the Diagnosis of Malnutrition: A Consensus Report From the Global Clinical Nutrition Community. JPEN J. Parenter. Enteral Nutr. 2019, 43, 32–40. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef]
- Ye, X.-J.; Ji, Y.-B.; Ma, B.-W.; Huang, D.-D.; Chen, W.-Z.; Pan, Z.-Y.; Shen, X.; Zhuang, C.-L.; Yu, Z. Comparison of three common nutritional screening tools with the new European Society for Clinical Nutrition and Metabolism (ESPEN) criteria for malnutrition among patients with geriatric gastrointestinal cancer: A prospective study in China. BMJ Open 2018, 8, e019750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Inoue, T.; Maeda, K.; Shimizu, A.; Nagano, A.; Ueshima, J.; Sato, K.; Murotani, K. Calf circumference value for sarcopenia screening among older adults with stroke. Arch. Gerontol. Geriatr. 2021, 93, 104290. [Google Scholar] [CrossRef]
- Wilson, M.-M.G.; Thomas, D.R.; Rubenstein, L.Z.; Chibnall, J.T.; Anderson, S.; Baxi, A.; Diebold, M.R.; Morley, J.E. Appetite assessment: Simple appetite questionnaire predicts weight loss in community-dwelling adults and nursing home residents. Am. J. Clin. Nutr. 2005, 82, 1074–1081. [Google Scholar] [CrossRef]
- Tokudome, Y.; Okumura, K.; Kumagai, Y.; Hirano, H.; Kim, H.; Morishita, S.; Watanabe, Y. Development of the Japanese version of the Council on Nutrition Appetite Questionnaire and its simplified versions, and evaluation of their reliability, validity, and reproducibility. J. Epidemiol. 2017, 27, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Rolland, Y.; Perrin, A.; Gardette, V.; Filhol, N.; Vellas, B. Screening older people at risk of malnutrition or malnourished using the Simplified Nutritional Appetite Questionnaire (SNAQ): A comparison with the Mini-Nutritional Assessment (MNA) tool. J. Am. Med. Dir. Assoc. 2012, 13, 31–34. [Google Scholar] [CrossRef]
- Yaxley, A.; Crotty, M.; Miller, M. Identifying Malnutrition in an Elderly Ambulatory Rehabilitation Population: Agreement between Mini Nutritional Assessment and Validated Screening Tools. Healthcare 2015, 3, 822–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.; Shen, J. Usefulness of Simplified Nutritional Appetite Questionnaire (SNAQ) in Appetite Assessment in Elder Patients with Liver Cirrhosis. J. Nutr. Health Aging 2018, 22, 911–915. [Google Scholar] [CrossRef]
- Wleklik, M.; Lisiak, M.; Andreae, C.; Uchmanowicz, I. Psychometric Evaluation of Appetite Questionnaires in Elderly Polish Patients with Heart Failure. Patient Prefer. Adherence 2019, 13, 1751–1759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimizu, A.; Maeda, K.; Honda, T.; Ishida, Y.; Ueshima, J.; Nagami, S.; Nagano, A.; Inoue, T.; Murotani, K.; Kayashita, J.; et al. Comparison between the Global Leadership Initiative on Malnutrition and the European Society for Clinical Nutrition and Metabolism definitions for the prevalence of malnutrition in geriatric rehabilitation care. Geriatr. Gerontol. Int. 2020, 20, 1221–1227. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, A.; Maeda, K.; Koyanagi, Y.; Kayashita, J.; Fujishima, I.; Mori, N. The Global Leadership Initiative on Malnutrition-Defined Malnutrition Predicts Prognosis in Persons with Stroke-Related Dysphagia. J. Am. Med. Dir. Assoc. 2019, 20, 1628–1633. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.B.; Reijnierse, E.M.; Lim, W.K.; Maier, A.B. Prevalence of malnutrition comparing the GLIM criteria, ESPEN definition and MST malnutrition risk in geriatric rehabilitation patients: RESORT. Clin. Nutr. 2020, 39, 3504–3511. [Google Scholar] [CrossRef]
- Shimizu, A.; Maeda, K.; Wakabayashi, H.; Nishioka, S.; Nagano, A.; Kayashita, J.; Fujishima, I.; Momosaki, R. Predictive Validity of Body Mass Index Cutoff Values Used in the Global Leadership Initiative on Malnutrition Criteria for Discriminating Severe and Moderate Malnutrition Based on In-Patients With Pneumonia in Asians. JPEN J. Parenter. Enteral Nutr. 2020. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Wakabayashi, H.; Bise, T.; Nagano, F.; Shimazu, S.; Shiraishi, A.; Yamaga, M.; Koga, H. Sarcopenia is associated with worse recovery of physical function and dysphagia and a lower rate of home discharge in Japanese hospitalized adults undergoing convalescent rehabilitation. Nutrition 2019, 61, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Tsutsumimoto, K.; Doi, T.; Nakakubo, S.; Kim, M.; Kurita, S.; Ishii, H.; Shimada, H. Association between anorexia of ageing and sarcopenia among Japanese older adults. J. Cachexia Sarcopenia Muscle 2020, 11, 1250–1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Kunieda, K.; Ohno, T.; Fujishima, I.; Hojo, K.; Morita, T. Reliability and validity of a tool to measure the severity of dysphagia: The Food Intake LEVEL Scale. J. Pain Symptom Manag. 2013, 46, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Kidd, D.; Stewart, G.; Baldry, J.; Johnson, J.; Rossiter, D.; Petruckevitch, A.; Thompson, A.J. The Functional Independence Measure: A comparative validity and reliability study. Disabil. Rehabil. 1995, 17, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Nakatsu, N.; Sawa, R.; Misu, S.; Ueda, Y.; Ono, R. Reliability and validity of the Japanese version of the simplified nutritional appetite questionnaire in community-dwelling older adults. Geriatr. Gerontol. Int. 2015, 15, 1264–1269. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.B.; Foley, A.L.; Barnard, R.; Isenring, E.A.; Miller, M.D. Nutritional screening in community-dwelling older adults: A systematic literature review. Asia Pac. J. Clin. Nutr. 2010, 19, 440–449. [Google Scholar]
- Yoshimura, Y.; Wakabayashi, H.; Nagano, F.; Bise, T.; Shimazu, S.; Shiraishi, A. Chair-stand exercise improves post-stroke dysphagia. Geriatr. Gerontol. Int. 2020, 20, 885–891. [Google Scholar] [CrossRef]
- Lau, S.; Pek, K.; Chew, J.; Lim, J.P.; Ismail, N.H.; Ding, Y.Y.; Cesari, M.; Lim, W.S. The Simplified Nutritional Appetite Questionnaire (SNAQ) as a Screening Tool for Risk of Malnutrition: Optimal Cutoff, Factor Structure, and Validation in Healthy Community-Dwelling Older Adults. Nutrients 2020, 12, 2885. [Google Scholar] [CrossRef]
- Power, L.; Mullally, D.; Gibney, E.R.; Clarke, M.; Visser, M.; Volkert, D.; Bardon, L.; de van der Schueren, M.A.E.; Corish, C.A. MaNuEL Consortium A review of the validity of malnutrition screening tools used in older adults in community and healthcare settings—A MaNuEL study. Clin. Nutr. ESPEN 2018, 24, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Bellanti, F.; Lo Buglio, A.; Quiete, S.; Pellegrino, G.; Dobrakowski, M.; Kasperczyk, A.; Kasperczyk, S.; Vendemiale, G. Comparison of Three Nutritional Screening Tools with the New Glim Criteria for Malnutrition and Association with Sarcopenia in Hospitalized Older Patients. J. Clin. Med. Res. 2020, 9, 1898. [Google Scholar] [CrossRef]
- Balci, C.; Bolayir, B.; Eşme, M.; Arik, G.; Kuyumcu, M.E.; Yeşil, Y.; Varan, H.D.; Kara, Ö.; Güngör, A.E.; Doğu, B.B.; et al. Comparison of the Efficacy of the Global Leadership Initiative on Malnutrition Criteria, Subjective Global Assessment, and Nutrition Risk Screening 2002 in Diagnosing Malnutrition and Predicting 5-Year Mortality in Patients Hospitalized for Acute Illnesses. JPEN J. Parenter. Enteral Nutr. 2020. [Google Scholar] [CrossRef]
- Schuetz, P.; Fehr, R.; Baechli, V.; Geiser, M.; Deiss, M.; Gomes, F.; Kutz, A.; Tribolet, P.; Bregenzer, T.; Braun, N.; et al. Individualised nutritional support in medical inpatients at nutritional risk: A randomised clinical trial. Lancet 2019, 393, 2312–2321. [Google Scholar] [CrossRef]
- Malmstrom, T.K.; Morley, J.E. SARC-F: A simple questionnaire to rapidly diagnose sarcopenia. J. Am. Med. Dir. Assoc. 2013, 14, 531–532. [Google Scholar] [CrossRef]
- Ida, S.; Kaneko, R.; Murata, K. SARC-F for Screening of Sarcopenia among Older Adults: A Meta-analysis of Screening Test Accuracy. J. Am. Med. Dir. Assoc. 2018, 19, 685–689. [Google Scholar] [CrossRef] [PubMed]
- İlhan, B.; Bahat, G.; Oren, M.M.; BKılıç, C.; Durmazoglu, S.; Karan, M.A. Reliability and validity of Turkish version of the Simplified Nutritional Appetite Questionnaire (SNAQ). J. Nutr. Health Aging 2018, 22, 1039–1044. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| SNAQ < 14 | SNAQ ≥ 14 | p-Value | SNAQ-JE ≤ 14 | SNAQ-JE > 14 | p-Value | |
|---|---|---|---|---|---|---|
| Number of patients, n (%) | 94 (24.7) | 286 (75.3) | 234 (61.6) | 146 (38.4) | ||
| Age, years 1 | 80.1 ± 8.1 | 79.1 ± 7.8 | 0.265 | 79.9 ± 8.0 | 78.5 ± 7.7 | 0.105 |
| Sex (female), n (%) 2 | 64 (68.1) | 164 (57.3) | 0.070 | 143 (61.1) | 85 (58.2) | 0.592 |
| Primary disease, n (%) 2 | ||||||
| - Stroke | 36 (38.3) | 136 (47.6) | 0.011 | 106 (45.3) | 66 (45.2) | 0.365 |
| - Musculoskeletal disease | 47 (50.0) | 140 (49.0) | 112 (47.9) | 75 (51.4) | ||
| - Hospital-associated deconditioning | 11 (11.7) | 10 (3.5) | 16 (6.8) | 5 (3.4) | ||
| Days from onset to rehabilitation 3 | 23 (15–34) | 24 (17–34) | 0.321 | 24 (17–34) | 24 (17–33) | 0.929 |
| Charlson comorbidity index, points 3 | 1 (0–2) | 1 (0–2) | 0.662 | 1 (0–2) | 1 (0–2) | 0.473 |
| Body mass index, kg/m2 1 | 20.6 ± 3.6 | 21.5 ± 4.3 | 0.065 | 20.9 ± 3.8 | 21.9 ± 4.52 | 0.012 |
| SNAQ, points 3 | 12 (11–13) | 15 (15–16) | <0.001 | 14 (13–15) | 16 (16–17) | <0.001 |
| SNAQ-JE, points 3 | 11 (10–12) | 15 (14– 15) | <0.001 | 13 (11–14) | 15 (15–16) | <0.001 |
| SNAQ < 14 | SNAQ ≥ 14 | p-Value | SNAQ-JE ≤ 14 | SNAQ-JE > 14 | p-Value | |
|---|---|---|---|---|---|---|
| Skeletal muscle mass index, kg/m2 1 | ||||||
| - Male | 6.10 ± 1.09 | 6.61 ± 0.89 | 0.009 | 6.36 ± 0.95 | 6.72 ± 0.91 | 0.021 |
| - Female | 4.84 ± 1.04 | 5.13 ± 1.05 | 0.058 | 4.88 ± 1.05 | 5.33 ± 1.00 | 0.002 |
| Handgrip strength, kg 1 | ||||||
| - Male | 24.2 ± 7.8 | 26.8 ± 8.1 | 0.106 | 24.9 ± 7.7 | 28.4 ± 8.1 | 0.007 |
| - Female | 13.4 ± 5.7 | 15.3 ± 5.8 | 0.025 | 13.8 ± 5.4 | 16.3 ± 6.2 | 0.001 |
| Mini-Mental Examination State, points 2 | 25 (21–28) | 26 (21–29) | 0.202 | 25 (20–28) | 27 (22–29) | 0.021 |
| Food Intake Level Scale, points 2 | 8 (8–9) | 8 (8–9) | 0.414 | 8 (7–99) | 8 (8– 9) | 0.003 |
| Functional Independence Measure, points 2 | 79 (65–94) | 84 (66–99) | 0.189 | 79 (61–95) | 87 (72–102) | 0.001 |
| Malnourished (MNA-SF ≤ 7), n (%) 3 | 71 (75.5) | 144 (50.3) | <0.001 | 150 (64.1) | 65 (44.5) | <0.001 |
| GLIM-defined malnutrition, n (%) 3 | 71 (75.5) | 145 (50.7) | <0.001 | 158 (67.5) | 58 (39.7) | <0.001 |
| Sarcopenia, n (%) 3 | 67 (71.3) | 158 (55.2) | 0.008 | 158 (67.5) | 67 (45.9) | <0.001 |
| Model 1: GLIM-Defined Malnutrition | |||
| Odds ratio | 95% confidence interval | p-value | |
| Poor appetite in SNAQ | 3.004 | 1.651–5.464 | <0.001 |
| Poor appetite in SNAQ-JE | 2.754 | 1.669–4.545 | <0.001 |
| Model 2: Sarcopenia | |||
| Odds ratio | 95% confidence interval | p-value | |
| Poor appetite in SNAQ | 1.627 | 0.894–2.963 | 0.111 |
| Poor appetite in SNAQ-JE | 1.940 | 1.176–3.198 | 0.009 |
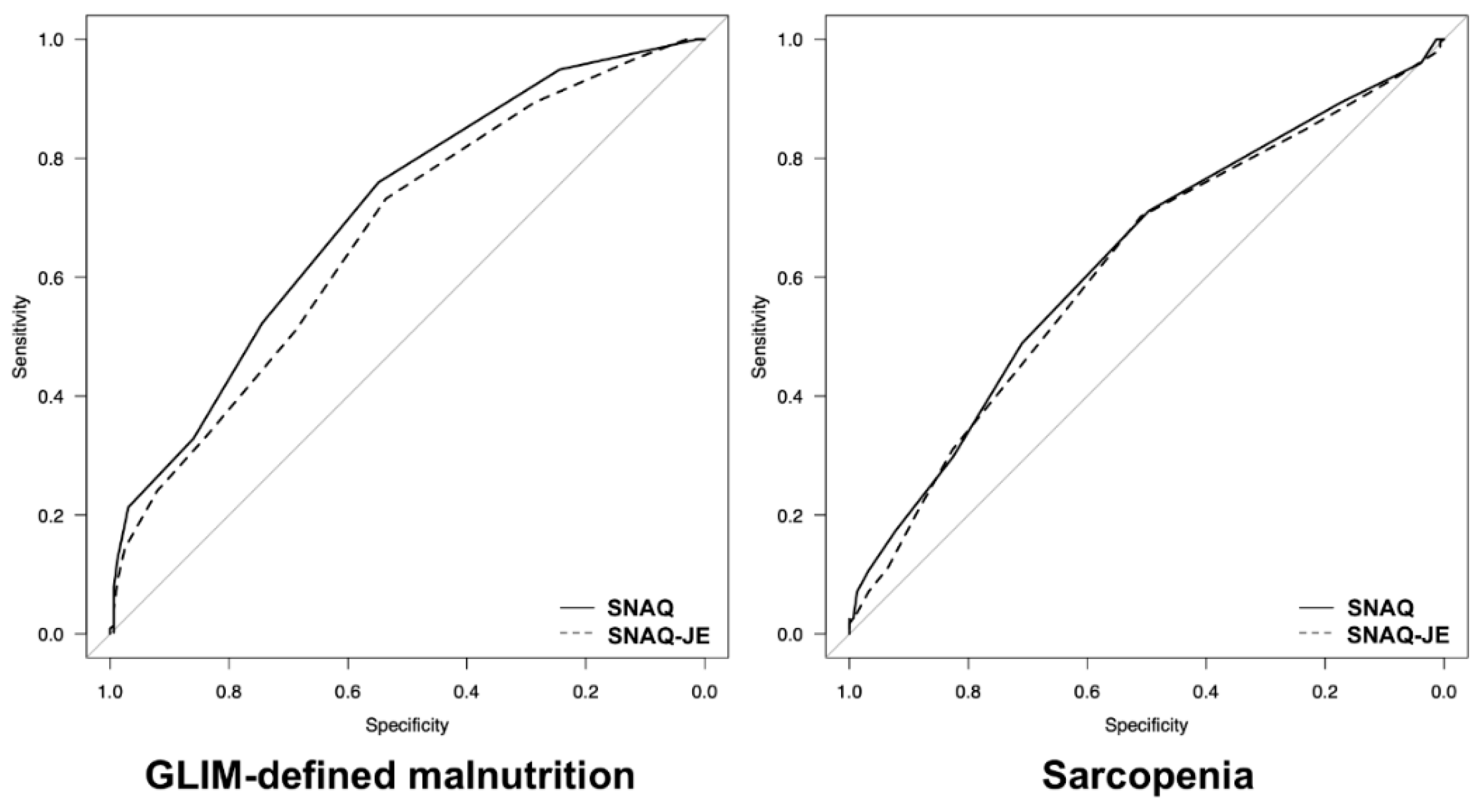
| Poor Appetite in SNAQ | ||||||
| Sensitivity | Specificity | Accuracy | PPV | NPV | AUC | |
| GLIM-defined malnutrition | 0.329 | 0.860 | 0.558 | 0.755 | 0.493 | 0.706 |
| Sarcopenia | 0.298 | 0.826 | 0.513 | 0.713 | 0.513 | 0.627 |
| Poor Appetite in SNAQ-JE | ||||||
| Sensitivity | Specificity | Accuracy | PPV | NPV | AUC | |
| GLIM-defined malnutrition | 0.731 | 0.537 | 0.647 | 0.675 | 0.603 | 0.670 |
| Sarcopenia | 0.702 | 0.510 | 0.624 | 0.675 | 0.541 | 0.616 |
| Undernutrition in MNA-SF ≤ 7 | ||||||
| Sensitivity | Specificity | Accuracy | PPV | NPV | AUC | |
| GLIM-defined malnutrition | 0.778 | 0.713 | 0.750 | 0.781 | 0.709 | 0.815 |
| Sarcopenia | 0.680 | 0.600 | 0.647 | 0.712 | 0.564 | 0.708 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimizu, A.; Fujishima, I.; Maeda, K.; Murotani, K.; Inoue, T.; Ohno, T.; Nomoto, A.; Ueshima, J.; Ishida, Y.; Nagano, A.; et al. Accuracy of the Simplified Nutritional Appetite Questionnaire for Malnutrition and Sarcopenia Screening among Older Patients Requiring Rehabilitation. Nutrients 2021, 13, 2738. https://doi.org/10.3390/nu13082738
Shimizu A, Fujishima I, Maeda K, Murotani K, Inoue T, Ohno T, Nomoto A, Ueshima J, Ishida Y, Nagano A, et al. Accuracy of the Simplified Nutritional Appetite Questionnaire for Malnutrition and Sarcopenia Screening among Older Patients Requiring Rehabilitation. Nutrients. 2021; 13(8):2738. https://doi.org/10.3390/nu13082738
Chicago/Turabian StyleShimizu, Akio, Ichiro Fujishima, Keisuke Maeda, Kenta Murotani, Tatsuro Inoue, Tomohisa Ohno, Akiko Nomoto, Junko Ueshima, Yuria Ishida, Ayano Nagano, and et al. 2021. "Accuracy of the Simplified Nutritional Appetite Questionnaire for Malnutrition and Sarcopenia Screening among Older Patients Requiring Rehabilitation" Nutrients 13, no. 8: 2738. https://doi.org/10.3390/nu13082738