Dietary Patterns as Characterized by Food Processing Levels and Their Association with the Health Outcomes of Rural Women in East Africa


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Areas and Design
2.2. Data Collection
2.3. Extration of Patterns and Food Processing Levels
2.4. Statistical Analysis
3. Results
3.1. Socio-Economic and Demographic Characteristics
3.2. Body Mass Index as a Proxy for Health Outcomes
3.3. Patterns as Characterized by Food Processing Levels
3.4. Correlation between Patterns and Socio-Economic and Demographics Indicators
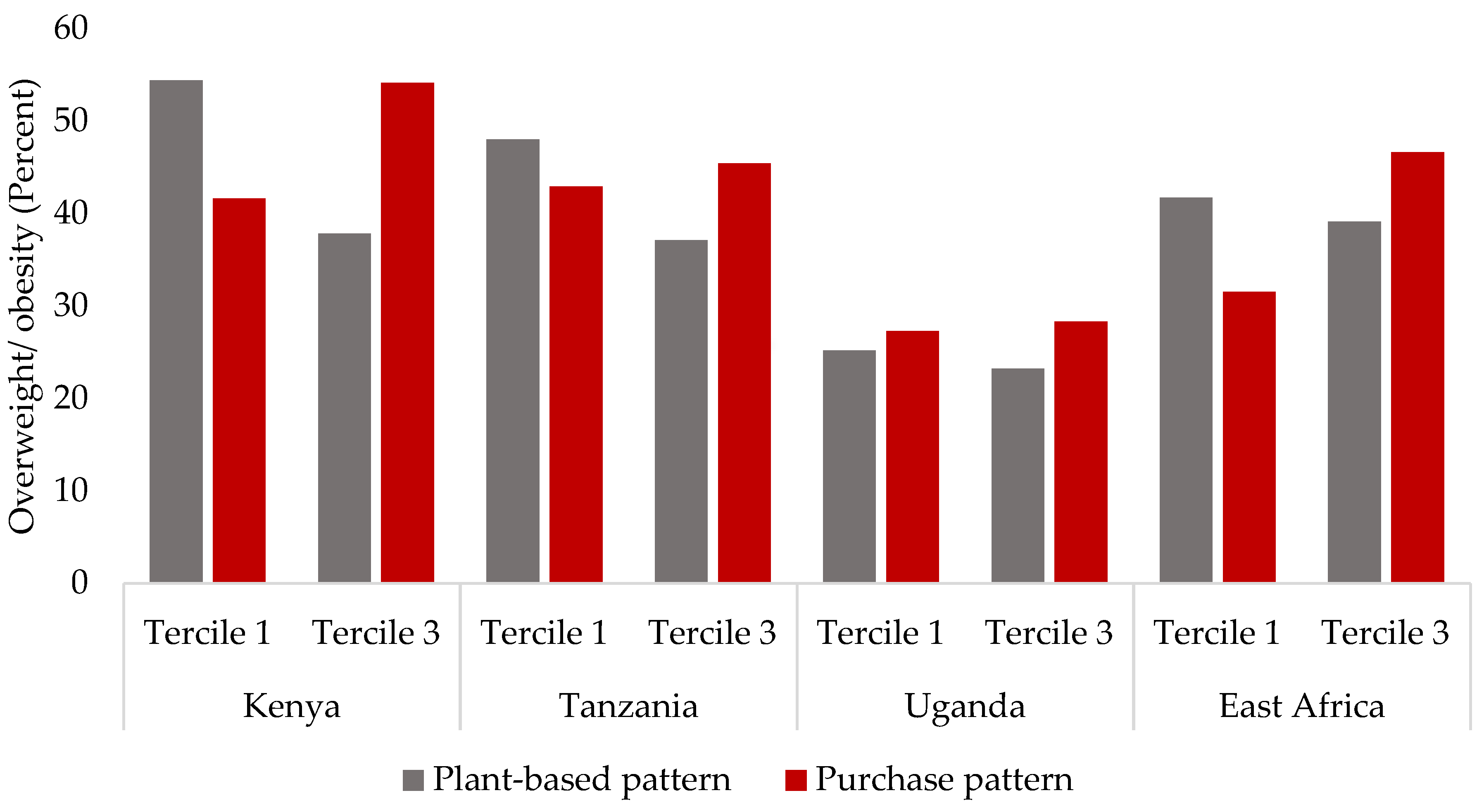
3.5. Association between Patterns and Overweight and Obesity
3.6. Relationship between Patterns and BMI (in Continous Values)
4. Discussion
4.1. Overweight and Obesity in Sub-Saharan Africa
4.2. Patterns and the Nutrition Transition
4.3. Processed Foods, Wealth, and Overweight and Obesity
4.4. Country Comparison
4.5. Study Strengths and Limitations
4.6. Policy Implications and Further Work
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Swinburn, B.A.; Kraak, V.I.; Allender, S.; Atkins, V.J.; Baker, P.I.; Bogard, J.R.; Brinsden, H.; Calvillo, A.; De Schutter, O.; Devarajan, R.; et al. The Global Syndemic of Obesity, Undernutrition, and Climate Change: The Lancet Commission report. Lancet 2019, 393, 791–846. [Google Scholar] [CrossRef]
- Global Nutrition Report. Action on Equity to End Malnutrition: Development Initiatives; Development Initiatives Poverty Research Ltd.: Bristol, UK, 2020. [Google Scholar]
- Shekar, M.; Popkin, B. Obesity: Health and Economic Consequences of an Impending Global Challenge; The World Bank: Washington, DC, USA, 2020; ISBN 978-1-4648-1491-4. [Google Scholar]
- Afshin, A. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef]
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Global Status Report on Noncommunicable Diseases 2010; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Steyn, N.P.; Mchiza, Z.J. Obesity and the nutrition transition in Sub-Saharan Africa. Ann. N. Y. Acad. Sci. 2014, 1311, 88–101. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Frank, L.K.; Kröger, J.; Schulze, M.B.; Bedu-Addo, G.; Mockenhaupt, F.; Danquah, I. Dietary patterns in urban Ghana and risk of type 2 diabetes. Br. J. Nutr. 2014, 112, 89–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Togo, P.; Osler, M.; Sørensen, T.; Heitmann, B.L. Food intake patterns and body mass index in observational studies. Int. J. Obes. 2001, 25, 1741–1751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulze, M.B.; Hoffmann, K. Methodological approaches to study dietary patterns in relation to risk of coronary heart disease and stroke. Br. J. Nutr. 2006, 95, 860–869. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, K.; Schulze, M.B.; Schienkiewitz, A.; Nöthlings, U.; Boeing, H. Application of a New Statistical Method to Derive Dietary Patterns in Nutritional Epidemiology. Am. J. Epidemiol. 2004, 159, 935–944. [Google Scholar] [CrossRef]
- Weikert, C.; Schulze, M.B. Evaluating dietary patterns. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 341–346. [Google Scholar] [CrossRef]
- Becquey, E.; Savy, M.; Danel, P.; Dabiré, H.B.; Tapsoba, S.; Martin-Prével, Y. Dietary patterns of adults living in Ouagadougou and their association with overweight. Nutr. J. 2010, 9, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keding, G.B.; Msuya, J.M.; Maass, B.; Krawinkel, M. Dietary Patterns and Nutritional Health of Women: The Nutrition Transition in Rural Tanzania. Food Nutr. Bull. 2011, 32, 218–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisa, P.T.; Pedro, T.M.; Kahn, K.; Tollman, S.M.; Pettifor, J.M.; Norris, S.A. Nutrient Patterns and Their Association with Socio-Demographic, Lifestyle Factors and Obesity Risk in Rural South African Adolescents. Nutrients 2015, 7, 3464–3482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, M.D.; Dalal, S.; Sewram, V.; Diamond, M.B.; Adebamowo, S.N.; Ajayi, I.O.; Adebamowo, C.; Chiwanga, F.S.; Njelekela, M.; Laurence, C.; et al. Consumption of processed food dietary patterns in four African populations. Public Health Nutr. 2018, 21, 1529–1537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auma, C.I.; Pradeilles, R.; Blake, M.K.; Holdsworth, M. What Can Dietary Patterns Tell Us about the Nutrition Transition and Environmental Sustainability of Diets in Uganda? Nutrients 2019, 11, 342. [Google Scholar] [CrossRef] [Green Version]
- Floros, J.D.; Newsome, R.; Fisher, W.; Barbosa-Cánovas, G.V.; Chen, H.; Dunne, C.P.; German, J.B.; Hall, R.L.; Heldman, D.R.; Karwe, M.V.; et al. Feeding the World Today and Tomorrow: The Importance of Food Science and Technology. Compr. Rev. Food Sci. Food Saf. 2010, 9, 572–599. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.-C.; Louzada, M.L.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; et al. Ultra-processed foods: What they are and how to identify them. Public Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef]
- Elizabeth, L.; Machado, P.; Zinöcker, M.; Baker, P.; Lawrence, M. Ultra-Processed Foods and Health Outcomes: A Narrative Review. Nutrients 2020, 12, 1955. [Google Scholar] [CrossRef]
- Reardon, T.; Tschirley, D.; Liverpool-Tasie, L.S.O.; Awokuse, T.; Fanzo, J.; Minten, B.; Vos, R.; Dolislager, M.; Sauer, C.; Dhar, R.; et al. The processed food revolution in African food systems and the double burden of malnutrition. Glob. Food Secur. 2020, 28, 100466. [Google Scholar] [CrossRef]
- Kurz, K.M.; Johnson-Welch, C. Enhancing Women’s Contributions to Improving Family Food Consumption and Nutrition. Food Nutr. Bull. 2001, 22, 443–453. [Google Scholar] [CrossRef]
- McMullin, S.; Wekesa, B. Food Consumption and Nutritional Status of Mothers/Caregivers and Children in Project Sites: Overview; World Agroforestry Centre: Nairobi, Kenya, 19 July 2017. [Google Scholar]
- Taita Taveta County Government the First Taita Taveta County Integrated Development Plan. 2013. Available online: http://www.kpda.or.ke/documents/CIDP/Taita%20Taveta.pdf (accessed on 15 January 2019).
- MoALF. Climate Risk Profile for Taita Taveta County. Kenya County Climate Risk Profile Series. 2016. Available online: https://ccafs.cgiar.org/resources/publications/climate-risk-profile-taita-taveta-county-kenya-county-climate-risk (accessed on 15 November 2018).
- United Republic of Tanzania. Morogoro Region Socio-Economic Profile. Available online: http://tzonline.org/pdf/Morogoro.pdf (accessed on 18 November 2018).
- United Republic of Tanzania. Tanzania Demographic and Health Survey and Malaria Indicator Survey 2015–2016; MoHCDGEC, MoH, NBS, OCGS, and ICF: Dar es Salaam, MD, USA, 2016. [Google Scholar]
- Martin, P.; Topper, C.; Bashiru, R.; Boma, F.; De Waal, D.; Harries, H.; Kasuga, L.; Katanila, N.; Kikoka, L.; Lamboll, R.; et al. Cashew nut production in Tanzania: Constraints and progress through integrated crop management. Crop. Prot. 1997, 16, 5–14. [Google Scholar] [CrossRef]
- Republic of Uganda. Jinja District Local Government: Five-Year District Development Plan 2015/16–2019/20. Available online: https://jinja.go.ug/sites/default/files/JINJA%20DISTRICT%20DDP%20II%202015%20to%202020%20%282%29.pdf (accessed on 18 November 2018).
- Uganda Bureau of Statistics. The National Population and Housing Census 2014—Area Specific Profile Series. Kayunga District. Available online: https://www.ubos.org/wp-content/uploads/publications/2014CensusProfiles/KAYUNGA.pdf (accessed on 18 November 2018).
- Cogill, B. Anthropometric Indicators Measurement Guide; Food and Nutrition Technical Assistance, Academy for Educational Development: Washington, DC, USA, 2003. [Google Scholar]
- FAO/Government of Kenya. Kenyan Food Recipes. A Recipe Book of Common Mixed Dishes with Nutrient Value. Available online: http://www.fao.org/3/I8897EN/I8897en.pdf (accessed on 6 October 2019).
- Lukmanji, Z.; Hertzmark, E.; Mlingi, N.; Assey, V.; Ndossi, G.; Fawzi, W. Tanzania Food Composition Tables; MUHAS-TFNC, HSPH: Dar es Salaam, Tanzania, 2008. [Google Scholar]
- McCann, S.E.; Weiner, J.; Graham, S.; Freudenheim, J.L. Is principal components analysis necessary to characterise dietary behaviour in studies of diet and disease? Public Health Nutr. 2001, 4, 903–908. [Google Scholar] [CrossRef] [Green Version]
- WHO. Obesity: Preventing and Managing the Global Epidemic; WHO Technical Report Series No. 894; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Keding, G.B.; Kehlenbeck, K.; Kennedy, G.; McMullin, S. Fruit production and consumption: Practices, preferences and attitudes of women in rural western Kenya. Food Secur. 2017, 9, 453–469. [Google Scholar] [CrossRef]
- Ajayi, I.O.; Adebamowo, C.; Adami, H.-O.; Dalal, S.; Diamond, M.B.; Bajunirwe, F.; Guwatudde, D.; Njelekela, M.; Nankya-Mutyoba, J.; Chiwanga, F.S.; et al. Urban–rural and geographic differences in overweight and obesity in four sub-Saharan African adult populations: A multi-country cross-sectional study. BMC Public Health 2016, 16, 1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keding, G.B.; Msuya, J.M.; Maass, B.L.; Krawinkel, M.B. Obesity as a public health problem among adult women in rural Tanzania. Glob. Health Sci. Pr. 2013, 1, 359–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health, K. Statistical Review of Progress towards the Mid-Term Targets of the Kenya Health Sector Strategic Plan 2014–2018. Available online: https://www.healthdatacollaborative.org/fileadmin/uploads/hdc/Documents/Country_documents/KHSSP_Statistical__Report_2016.pdf (accessed on 1 June 2021).
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, C.A.; Levy, R.B.; Claro, R.; De Castro, I.R.R.; Cannon, G. Increasing consumption of ultra-processed foods and likely impact on human health: Evidence from Brazil. Public Health Nutr. 2010, 14, 5–13. [Google Scholar] [CrossRef]
- Popkin, B.M. Global nutrition dynamics: The world is shifting rapidly toward a diet linked with noncommunicable diseases. Am. J. Clin. Nutr. 2006, 84, 289–298. [Google Scholar] [CrossRef]
- Seferidi, P.; Scrinis, G.; Huybrechts, I.; Woods, J.; Vineis, P.; Millett, C. The neglected environmental impacts of ultra-processed foods. Lancet Planet. Health 2020, 4, e437–e438. [Google Scholar] [CrossRef]
- Boysen, O.; Boysen-Urban, K.; Bradford, H.; Balié, J. Taxing highly processed foods: What could be the impacts on obesity and underweight in sub-Saharan Africa? World Dev. 2019, 119, 55–67. [Google Scholar] [CrossRef]
- Nickanor, N.; Kazembe, L.; Crush, J. Supermarkets and Informal Food Vendors in Windhoek: Hungry Cities Partnership. Available online: https://hungrycities.net/wp-content/uploads/2019/04/DP26.pdf (accessed on 22 June 2021).
- Downs, S.M.; Ahmed, S.; Fanzo, J.; Herforth, A. Food Environment Typology: Advancing an Expanded Definition, Framework, and Methodological Approach for Improved Characterization of Wild, Cultivated, and Built Food Environments toward Sustainable Diets. Foods 2020, 9, 532. [Google Scholar] [CrossRef] [Green Version]
- Khonje, M.G.; Ecker, O.; Qaim, M. Effects of Modern Food Retailers on Adult and Child Diets and Nutrition. Nutrients 2020, 12, 1714. [Google Scholar] [CrossRef]
- Dwyer, J.; Fulgoni, V.L.; Clemens, R.A.; Schmidt, D.B.; Freedman, M.R. Is “Processed” a Four-Letter Word? The Role of Processed Foods in Achieving Dietary Guidelines and Nutrient Recommendations. Adv. Nutr. 2012, 3, 536–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weaver, C.M.; Dwyer, J.; Fulgoni, V.L.; King, J.C.; Leveille, G.A.; Macdonald, R.S.; Ordovas, J.; Schnakenberg, D. Processed foods: Contributions to nutrition. Am. J. Clin. Nutr. 2014, 99, 1525–1542. [Google Scholar] [CrossRef] [PubMed]
- Sarfo, J.; Pawelzik, E.; Keding, G.B. Are processed fruits and vegetables from local food sources able to bridge nutrient gaps and reduce diet cost? Evidence from rural Tanzania, forthcoming.
- Fardet, A.; Rock, E. Ultra-processed foods: A new holistic paradigm? Trends Food Sci. Technol. 2019, 93, 174–184. [Google Scholar] [CrossRef]
- Rutayisire, E.; Wu, X.; Huang, K.; Tao, S.; Chen, Y.; Wang, S.; Tao, F. Dietary patterns are not associated with overweight and obesity in a sample of 8900 Chinese preschool children from four cities. J. Nutr. Sci. 2018, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slagter, S.N.; Corpeleijn, E.; Van Der Klauw, M.M.; Sijtsma, A.; Swart-Busscher, L.G.; Perenboom, C.W.M.; De Vries, J.H.M.; Feskens, E.J.M.; Wolffenbuttel, B.H.R.; Kromhout, D.; et al. Dietary patterns and physical activity in the metabolically (un)healthy obese: The Dutch Lifelines cohort study. Nutr. J. 2018, 17, 18. [Google Scholar] [CrossRef] [Green Version]
- Bedrick, B.S.; Eskew, A.M.; Chavarro, J.E.; Jungheim, E.S. Dietary Patterns, Physical Activity, and Socioeconomic Associations in a Midwestern Cohort of Healthy Reproductive-Age Women. Matern. Child Health J. 2020, 24, 1299–1307. [Google Scholar] [CrossRef]
- Northstone, K.; Ness, A.R.; Emmett, P.M.; Rogers, I.S. Adjusting for energy intake in dietary pattern investigations using principal components analysis. Eur. J. Clin. Nutr. 2007, 62, 931–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- FAO. Food-Based Dietary Guidelines. Available online: http://www.fao.org/nutrition/education/food-dietary-guidelines/regions/africa/en/ (accessed on 16 July 2021).


{kind=link}
{kind=link}
| Country | Study Area | FruVase Target Crop | Plenty Season | Lean Season | Malnutrition Indicators | References for Malnutrition Indicators | ||
|---|---|---|---|---|---|---|---|---|
| Survey Date | Data Collected | Survey Date | Data Collected | |||||
| Kenya | Kitui | Cowpea leaves | December 2019 | 24-h recall | June 2019 | 24-h recall; anthropometrics; socio-economic and demographics | Stunting (35%) for young children | [24] |
| Taita-Taveta | Guava | April/May 2019 | 24-h recall; anthropometrics; socio-economic and demographics | October 2019 | 24-h recall | 48% food insecure;Stunting (35%) for young children. | [25,26] | |
| Tanzania | Morogoro | African nightshade | June/July 2019 | 24-h recall; anthropometrics; socio-economic and demographics | January 2020 | 24-h recall | Iron deficiency for young children (66%) and women (47%). | [27,28] |
| Mtwara | Cashew apple | October/November 2019 | 24-h recall | April/May 2019 | 24-h recall; anthropometrics; socio-economic and demographics | Iron deficiency for young children (59%) | [28,29] | |
| Uganda | Jinja | Cowpea leaves | February 2020 | 24-h recall | August 2019 | 24-h recall; anthropometrics; socio-economic and demographics | Stunting (31%); wasted (2%); underweight (12%) for young children | [30] |
| Kayunga | Jackfruit | Triple burden of malnutrition among women | [31] | |||||
| Variables | Kenya | Tanzania | Uganda | East Africa (Pooled Data) |
|---|---|---|---|---|
| Age of participants (years) | 33.88 *KT (8.28) | 32.24 (8.55) | 31.25 ***KU (8.46) | 32.52 (8.46) |
| Household size | 5.25 ***KT (2.14) | 4.62 ***TU (1.94) | 6.44 ***KU (2.79) | 5.52 (2.46) |
| Household head (yes = 1, no =0) | 0.24 (0.43) | 0.19 (0.39) | 0.16 *KU (0.37) | 0.20 (0.40) |
| Body mass index (kg/m2) | 25.35 (5.14) | 24.87 ***TU (4.80) | 23.44 ***KU (3.83) | 24.54 (4.69) |
| Nutrition education received during the past 6 months (yes = 1, no = 0) | 0.14 *KT (0.35) | 0.09 (0.28) | 0.10 +KU (0.29) | 0.11 (0.32) |
| Years spent in school | 8.44 ***KT (3.21) | 6.54 **TU (2.49) | 7.21 ***KU (3.65) | 7.52 (3.31) |
| Educational level (%) | ||||
| None | 3.82 | 8.90 | 8.89 | 6.94 |
| Primary | 67.42 | 79.79 | 54.33 | 65.83 |
| Secondary | 22.25 | 10.62 | 34.13 | 23.59 |
| Tertiary | 6.51 | 0.68 | 2.64 | 3.65 |
| Marital status (%) | ||||
| Married | 74.38 | 76.71 | 77.16 | 75.98 |
| Widowed or divorced or single | 25.62 | 23.29 | 22.84 | 24.02 |
| Main occupation (%) | ||||
| None | 15.06 | 7.88 | 17.79 | 14.22 |
| Farmer | 62.92 | 75.00 | 62.26 | 65.74 |
| Trader | 12.58 | 10.27 | 10.34 | 11.19 |
| Other (vocational skills, civil servant, teacher) | 9.44 | 6.85 | 9.61 | 8.84 |
| Wealth status (%) | ||||
| Low | 22.02 | 17.47 | 28.60 | 26.91 |
| Medium | 37.53 | 32.19 | 34.38 | 32.38 |
| High | 40.45 | 50.34 | 37.02 | 40.71 |
| N | 445 | 292 | 415 | 1152 |
| Rotated Component | Extracted Pattern | Food Group with Food Items | Loading Coefficient | Food Processing Level Explaining Pattern(in Nutrition) | Proportion Variance Explained (%) | Cumulative Variance Explained (%) |
|---|---|---|---|---|---|---|
| 1 | Plant-based pattern | Cereals, roots, and tubers: Irish potato, sweet potato, maize, sorghum, millet, taro, plantain | 0.78 | Minimally and highly processed | 17 | 17 |
| Pulses and nuts: Beans, cowpea, green grams, peas | 0.87 | |||||
| Milled cereals, roots, pulses, and nuts: Millet flour, maize flour, sorghum flour, wheat flour | −0.59 | |||||
| Oils and fats: Sunflower cooking oil, margarine, hydrogenated fat | 0.48 | |||||
| 2 | Purchase pattern I | Tea: tea | 0.87 | Minimally and highly processed | 16 | 33 |
| Sugar and sugary drinks: Sugar, soda, sugary drinks (mango sweetened) | 0.64 | |||||
| Milk: Pasteurized milk, fermented milk | 0.68 | |||||
| 3 | Plant and animal-based pattern | Vegetables: Amaranth leaves, African nightshade, cowpea leaves, cabbage, carrot, eggplant, kales, onion, spinach, tomato, bitter lettuce, pumpkin leaves | 0.86 | Minimally and highly processed | 14 | 47 |
| Meat, poultry, and fish: Beef, poultry, goat meat, offals, small dried fish, fish, egg, pork | 0.46 | |||||
| Oils and fats: Sunflower cooking oil, margarine, hydrogenated fat | 0.72 | |||||
| 4 | Purchase pattern II | Bread and snacks: Bread, chips, noodles, mandazi, halfcake (wheat dough fried in oil), chapati (wheat flatbread) | 0.61 | Minimally and highly processed | 11 | 59 |
| Rice: rice | 0.78 |
| Rotated Component | Extracted Pattern | Food Group with Food Items | Loading Coefficient | Food Processing Level Explaining Pattern (in Nutrition) | Proportion Variance Explained (%) | Cumulative Variance Explained (%) |
|---|---|---|---|---|---|---|
| 1 | Plant and animal-based pattern | Vegetables: Amaranth leaves, African nightshade, cabbage, carrot, cassava leaves, Chinese cabbage, cowpea leaves, cucumber, eggplant, green pepper, jute mallow leaves, kales, okra, onion, potato leaves, pumpkin, pumpkin leaves, spinach, sweet potato leaves, tomato | 0.85 | Minimally and highly processed | 19 | 19 |
| Meat, poultry, and fish: Beef, poultry, fish, goat meat, small dried fish | 0.70 | |||||
| Oils and fats: Cashew nut milk, coconut milk, sunflower cooking oil | 0.84 | |||||
| 2 | Purchase pattern | Tea: tea | 0.90 | Highly processed | 18 | 37 |
| Sugar and sugary drinks: Sugar, soda, sugary drinks (lemon, mango sweetened) | 0.89 | |||||
| Bread and snacks: Bread, noodles, mandazi, vitumbua (dough from rice or maize or wheat flour fried in oil), buns, chapati (wheat flatbread), samosa (fried pastry with vegetables and/or meat filling) | 0.52 | |||||
| 3 | Plant-based pattern | Fruits: Cashew apple, jackfruit, lemon/orange, mango, passion fruit, pawpaw, watermelon, pineapple, sweet banana | 0.63 | Unprocessed and minimally processed | 11 | 49 |
| Milled cereals, roots, pulses, and nuts: Cassava flour, groundnut flour/paste, maize flour, millet flour, rice flour | 0.51 | |||||
| Pulses and nuts: Bambara groundnut, beans, cowpeas, groundnut | 0.60 | |||||
| 4 | Starchy plants | Cereals, roots, and tubers: Cassava, Irish potatoes, maize, plantain, rice, sweet potatoes, taro, millet | 0.87 | Minimally processed | 11 | 60 |
| Bread and snacks: Bread, noodles, mandazi, vitumbua (dough from rice or maize or wheat flour fried in oil), buns, chapati (wheat flatbread), samosa (fried pastry with vegetables and/or meat filling) | −0.59 |
| Rotated Component | Extracted Pattern | Food Group with Food Items | Loading Coefficient | Food Processing Level Explaining Pattern (in Nutrition) | Proportion Variance Explained (%) | Cumulative Variance Explained (%) |
|---|---|---|---|---|---|---|
| 1 | Purchase pattern | Tea: coffee, tea | 0.45 | Highly processed | 14 | 14 |
| Sugar and sugary drinks: Sugar, soda, sugary drinks (orange, passion, pineapple, tamarind sweetened) | 0.74 | |||||
| Bread and snacks: Bread, buns, mandazi, halfcake (dough fried in oil), chapati (wheat flatbread), bagiya (cassava and soybean flour fried in oil), cake, chips, cornflakes, hardcorn, noodles, pancake, popcorn, samosa (fried pastry with vegetables and/or meat filling) | 0.72 | |||||
| 2 | Plant-based pattern I | Milled cereals, roots, pulses, and nuts: Beans flour, groundnut flour/paste, maize flour, millet flour, sesame paste, sorghum flour, soybean flour/paste | 0.80 | Minimally processed | 13 | 27 |
| Pulses and nuts: Beans, groundnut, soybean | 0.81 | |||||
| 3 | Animal based pattern | Milk: Pasteurized milk | 0.45 | Minimally and highly processed | 12 | 39 |
| Meat, poultry, and fish: Beef, poultry, smoked fish, egg, fish, goat meat, offals, small dried fish | 0.80 | |||||
| Oils and fats: Sunflower cooking oil, ghee, palm oil | 0.59 | |||||
| 4 | Plant-based pattern II | Cereals, roots, and tubers: Taro, cassava, cassava flour, cocoyam, Irish potatoes, maize, millet, plantain, rice, sorghum, sweet potatoes | 0.73 | Unprocessed and minimally processed | 11 | 51 |
| Fruits: Apple, avocado, guava, jackfruit, lemon/orange, mango, passion fruit, pawpaw, pineapple, sweet banana, watermelon | 0.77 | |||||
| 5 | Vegetarian pattern | Vegetables: African nightshade, amaranth leaves, bitter berries, bitter tomatoes, cowpea leaves, cucumber, cabbage, carrot, mushroom, eggplant, garden eggs, green pepper, kales, onion, pumpkin, pumpkin leaves, spinach, tomato | 0.76 | Minimally and highly processed | 10 | 61 |
| Oils and fats: Sunflower cooking oil, ghee, palm oil | 0.53 |
| Rotated Component | Extracted Pattern | Food Group with Food Items | Loading Coefficient | Food Processing Level Explaining Pattern (in Nutrition) | Proportion Variance Explained (%) | Cumulative Variance Explained (%) |
|---|---|---|---|---|---|---|
| 1 | Mixed pattern | Cereals, roots, and tubers: Cassava, cocoyam, maize, millet, plantain, Irish potatoes, rice, sorghum, sweet potatoes, taro | 0.75 | Unprocessed, minimally, and highly processed | 17 | 17 |
| Fruits: Apple, avocado, cashew apple, guava, jackfruit, lemon/orange, mango, passion fruit, pawpaw, pineapple, sweet banana, tamarind, watermelon | 0.48 | |||||
| Milk: Pasteurized milk, fermented milk | 0.47 | |||||
| Sugar and sugary drinks: Sugar, soda, sugary drinks (lemon, mango, orange, passion, pineapple, tamarind sweetened) | 0.76 | |||||
| 2 | Plant-based pattern | Pulses and nuts: Bambara groundnut, beans, cowpeas, green grams, groundnut, peas, soybean | 0.73 | Minimally processed | 13 | 30 |
| Milled cereals, roots, pulses, and nuts: Beans flour, cassava flour, groundnut flour/paste, maize flour, millet flour, rice flour, sesame paste, sorghum flour, soybean flour/paste, wheat flour | −0.49 | |||||
| Meat, poultry, and fish: Smoked fish, egg, fish, goat meat, offals, beef, poultry, pork, small-dried fish | −0.54 | |||||
| 3 | Purchase pattern | Tea: tea, coffee | 0.64 | Highly processed | 13 | 44 |
| Bread and snacks: Bread, buns, mandazi, halfcake, vitumbua (dough from rice or maize or wheat flour fried in oil), chapati (unleavened flatbread), bagiya (cassava and soybean flour fried in oil), chips, cornflakes, hardcorn, noodles, pancake, popcorn, samosa (fried pastry with vegetables and/or meat filling) | 0.68 | |||||
| 4 | Vegetarian pattern | Vegetables: African nightshade, amaranth leaves, bitter berries, bitter lettuce, bitter tomatoes, cabbage, carrot, cassava leaves, Chinese cabbage, cowpea leaves, cucumber, eggplant, garden eggs, green pepper, jute mallow leaves, kales, mushroom, onion, okra, sweet potato leaves, pumpkin, pumpkin leaves, spinach, tomato | 0.81 | Minimally processed | 10 | 53 |
| Patterns | Kenya | Tanzania | Uganda | East Africa | ||||
|---|---|---|---|---|---|---|---|---|
| N | OR (90% CI) | N | OR (90% CI) | N | OR (90% CI) | N | OR (90% CI) | |
| Plant-based pattern a | ||||||||
| Tercile 1 | 149 | 1.00 (Ref.) | 98 | 1.00 (Ref.) | 139 | 1.00 (Ref.) | 384 | 1.00 (Ref.) |
| Tercile 2 | 148 | 1.02 (0.66, 1.57) | 97 | 0.79 (0.47, 1.31) | 138 | 1.34 (0.84, 2.13) | 384 | 0.71 (0.51, 0.99) |
| Tercile 3 | 148 | 0.72 (0.46, 1.12) | 97 | 0.59 * (0.35, 0.98) | 138 | 0.91 (0.56, 1.49) | 384 | 0.59 ** (0.41, 0.85) |
| Purchase pattern b | ||||||||
| Tercile 1 | 149 | 1.00 (Ref.) | 98 | 1.00 (Ref.) | 139 | 1.00 (Ref.) | 384 | 1.00 (Ref.) |
| Tercile 2 | 148 | 1.13 (0.74, 1.72) | 97 | 0.73 (0.44, 1.23) | 138 | 0.78 (0.48, 1.26) | 384 | 0.99 (0.74, 1.31) |
| Tercile 3 | 148 | 1.52 + (0.99, 2.32) | 97 | 0.85 (0.51, 1.43) | 138 | 0.95 (0.58, 1.53) | 384 | 1.22 * (0.89, 1.66) |
| Plant and animal-based pattern | ||||||||
| Tercile 1 | 149 | 1.00 (Ref.) | 98 | 1.00 (Ref.) | -- | -- | -- | -- |
| Tercile 2 | 148 | 0.96 (0.63, 1.44) | 97 | 0.88 (0.54, 1.47) | -- | -- | -- | -- |
| Tercile 3 | 148 | 1.05 (0.68, 1.60) | 97 | 0.87 (0.52, 1.47) | -- | -- | -- | -- |
| Purchase pattern I | ||||||||
| Tercile 1 | 149 | 1.00 (Ref.) | -- | -- | -- | -- | -- | -- |
| Tercile 2 | 148 | 0.88 (0.58, 1.34) | -- | -- | -- | -- | -- | -- |
| Tercile 3 | 148 | 0.98 (0.64, 1.49) | -- | -- | -- | -- | -- | -- |
| Starchy plants | ||||||||
| Tercile 1 | -- | -- | 98 | 1.00 (Ref.) | -- | -- | -- | -- |
| Tercile 2 | -- | -- | 97 | 1.23 (0.74, 2.05) | -- | -- | -- | -- |
| Tercile 3 | -- | -- | 97 | 0.76 (0.44, 1.28) | -- | -- | -- | -- |
| Vegetarian pattern | ||||||||
| Tercile 1 | -- | -- | -- | -- | 139 | 1.00 (Ref.) | 384 | 1.00 (Ref.) |
| Tercile 2 | -- | -- | -- | -- | 138 | 0.96 (0.60, 1.54) | 384 | 0.86 (0.66, 1.12) |
| Tercile 3 | -- | -- | -- | -- | 138 | 1.04 (0.64, 1.67) | 384 | 0.76 (0.58, 1.00) |
| Plant-based pattern I | ||||||||
| Tercile 1 | -- | -- | -- | -- | 139 | 1.00 (Ref.) | -- | -- |
| Tercile 2 | -- | -- | -- | -- | 138 | 1.24 (0.77, 2.00) | -- | -- |
| Tercile 3 | -- | -- | -- | -- | 138 | 0.91 (0.56, 1.47) | -- | -- |
| Animal-based pattern | ||||||||
| Tercile 1 | -- | -- | -- | -- | 139 | 1.00 (Ref.) | -- | -- |
| Tercile 2 | -- | -- | -- | -- | 138 | 1.31 (0.82, 2.09) | -- | -- |
| Tercile 3 | -- | -- | -- | -- | 138 | 0.81 (0.50, 1.32) | -- | -- |
| Mixed pattern | ||||||||
| Tercile 1 | -- | -- | -- | -- | -- | -- | 384 | 1.00 (Ref.) |
| Tercile 2 | -- | -- | -- | -- | -- | -- | 384 | 0.69 (0.53, 0.90) |
| Tercile 3 | -- | -- | -- | -- | -- | -- | 384 | 0.96 (0.60, 1.57) |
| Independent Variables | Body Mass Index (BMI) | |||
|---|---|---|---|---|
| Kenya | Tanzania | Uganda | East Africa | |
| Plant-based pattern a | −0.568 * (0.258) | −0.693 ** (0.257) | 0.169 (0.166) | −0.696 *** (0.160) |
| Purchase pattern b | 0.422 + (0.256) | −0.243 (0.283) | −0.090 (0.180) | 0.454 *** (0.137) |
| Plant- and animal-based pattern | −0.062 (0.282) | −0.131 (0.267) | -- | -- |
| Purchase pattern I | 0.480 * (0.228) | -- | -- | -- |
| Starchy plants | -- | −0.200 (0.281) | -- | -- |
| Vegetarian pattern | -- | -- | −0.193 (0.118) | −0.117 (0.084) |
| Plant-based pattern I | -- | -- | −0.184 (0.157) | -- |
| Animal-based pattern | -- | -- | −0.072 (0.153) | -- |
| Mixed pattern | -- | -- | -- | −0.180 (0.167) |
| Control Variables | Yes | Yes | Yes | Yes |
| N | 445 | 292 | 415 | 1152 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarfo, J.; Pawelzik, E.; Keding, G.B. Dietary Patterns as Characterized by Food Processing Levels and Their Association with the Health Outcomes of Rural Women in East Africa. Nutrients 2021, 13, 2866. https://doi.org/10.3390/nu13082866
Sarfo J, Pawelzik E, Keding GB. Dietary Patterns as Characterized by Food Processing Levels and Their Association with the Health Outcomes of Rural Women in East Africa. Nutrients. 2021; 13(8):2866. https://doi.org/10.3390/nu13082866
Chicago/Turabian StyleSarfo, Jacob, Elke Pawelzik, and Gudrun B. Keding. 2021. "Dietary Patterns as Characterized by Food Processing Levels and Their Association with the Health Outcomes of Rural Women in East Africa" Nutrients 13, no. 8: 2866. https://doi.org/10.3390/nu13082866