
Parent Involvement in Diet or Physical Activity Interventions to Treat or Prevent Childhood Obesity: An Umbrella Review

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategies and Eligibility Criteria
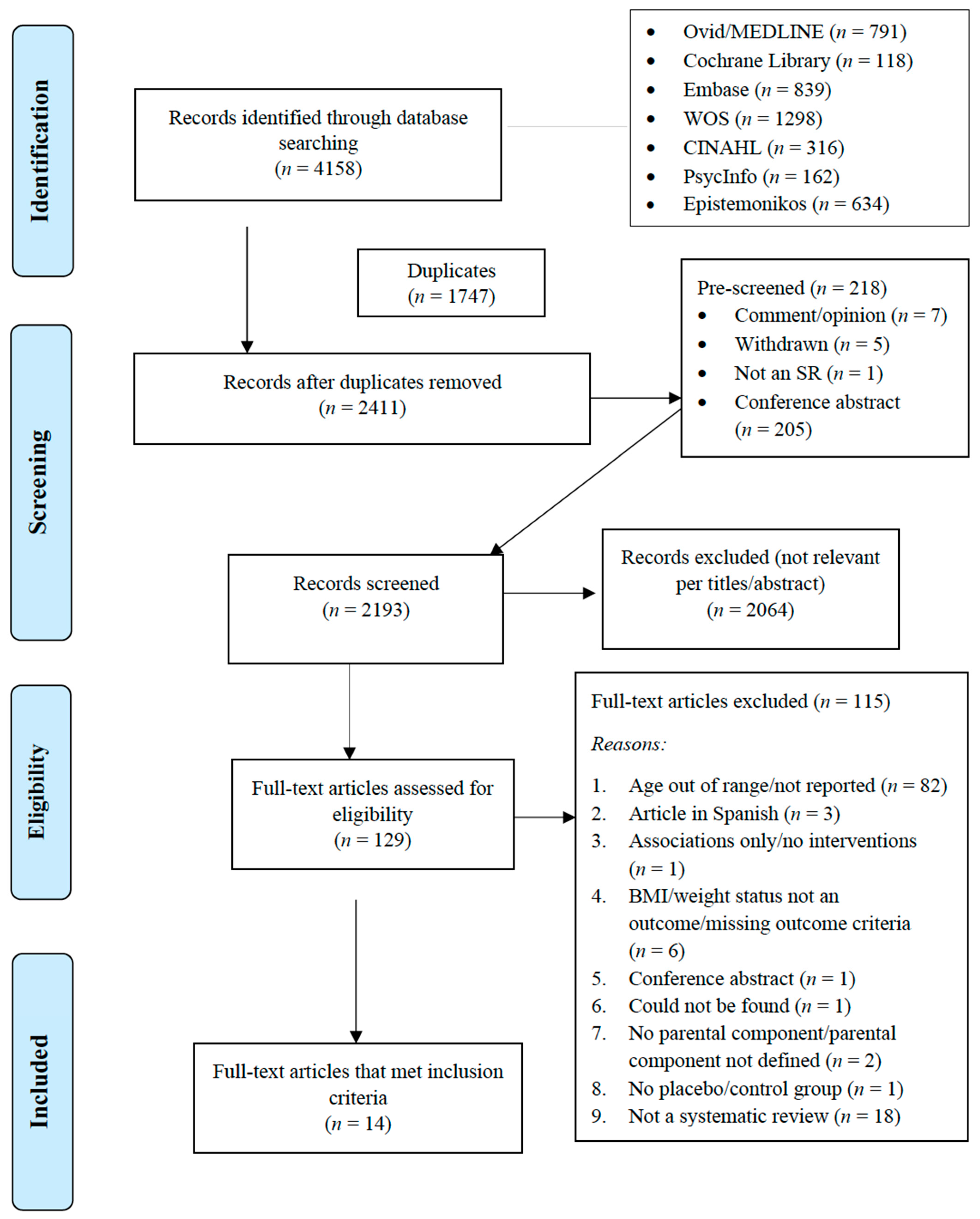
2.2. Study Selection
2.3. Quality Assessment
2.4. Data Extraction
2.5. Data Items and Measures
2.6. Data Synthesis
3. Results
3.1. Study Characteristics
3.2. Quality Assessment
3.3. Interventions and Study Settings
3.4. Treatment-Focused Reviews
3.4.1. Treatment Focus: Parents Involved
3.4.2. Treatment Focus: Parent Only
3.5. Prevention-Focused Reviews
3.5.1. Prevention Focus: Parent Component—Involvement Not Specified
3.5.2. Prevention Focus: Parent Component—Involvement Specified

{kind=link}
| Author (SR, MA, Both) | Research Question/Purpose | Umbrella Review Research Question(s) | Results | Conclusion |
|---|---|---|---|---|
| Gori (both) [49] | To update the Waters et al. (2011) meta-analysis results about the effectiveness of educational and lifestyle interventions aimed at preventing child obesity. | Are interventions that include diet or PA components or the combination of diet and PA effective in family settings or family and school settings combined? | Primary Outcome: BMI-SDS Reduction Intervention: Diet alone delivered in family setting or combined family + school: NS Intervention: PA alone * or PA + diet in family setting: NS Intervention: Combined (diet + physical activity) interventions delivered in combined (family + school) settings −0.15 (CI: −0.22 to −0.07); Z = 4.02, p < 0.0001; I2 = 94%; 5 or 6 studies; 451 participants**. Notes: * Table 1 indicates 0 family studies with PA alone. Text on page 241 does not specify whether NS studies in family setting were PA alone or PA + diet. Table S1 lists 2 PA-alone family studies, but descriptions of interventions do not mention PA. ** One of the 6 studies included in Figure S5 is not listed as combined study in Table S1 but as a school study. Whether the N of studies is 5 or 6 cannot be determined. | Combined diet and PA interventions delivered to children in settings that combined home and school settings resulted in significant reductions in BMI-SDS. |
| Laws (SR) [44] | To systematically review the literature to examine effectiveness of interventions to prevent obesity or improve obesity-related behaviors in children aged 0–5 years from Indigenous families or families experiencing socioeconomic disadvantage. | Are interventions delivered in preschool settings effective in preventing obesity in families who experience socioeconomic disadvantage? | Primary Outcome: BMI or body fat 3/7 studies found significant intervention effects on BMI (2 studies) or body fat (1 study)—1 high quality study; 2 moderate quality studies. 4/7 studies did not find significant intervention effects—3 low quality studies and 1 study with quality not reported in the review. DETAILS
| Some evidence for effectiveness of preschool interventions delivered to families who experience socioeconomic disadvantage as long as studies are of moderate or high quality. |
| Nixon (SR) [46] | To identify the most effective behavioral models and strategies underpinning preschool- and school-based interventions for preventing obesity in 4–6 year olds. | Are interventions for 4 to 6 year olds with parental involvement effective in preventing obesity? | Primary Outcome: Weight Status 3/7 studies with parental involvement found significant impact on weight status; 4/7 with parental involvement did not find significant impact on weight status.
| Some evidence for effectiveness of obesity prevention interventions with parental involvement. |
| Oosterhoff (both) [55] | To systematically review the evidence of the impact of school-based lifestyle RCTS on children’s BMI and blood pressure. | Lifestyle RCTs with parent involvement will reduce child BMI | Primary Outcome: BMI 53/83 unique RCTs included a parental involvement component in addition to the single or multiple lifestyle components; k = 151 effect sizes.
| Parent involvement significantly enhanced the positive impact of school-based lifestyle RCTs in reducing child BMI. |
| Sobol-Goldberg (both) [54] | To evaluate efficacy of school-based obesity prevention programs. To test the hypothesis that studies that were comprehensive and at least one year long with parental support would have the best results. | Do school-based interventions that address nutrition and physical activity and include parent involvement reduce child BMI? |
8 studies of children with parent involvement identified by the authors
Primary Outcome: BMI
There were 0 comprehensive shorter duration studies without parental involvement. There were 9 studies that were “none of the above.” These would appear to be studies that were not comprehensive. The authors did not classify these 9 studies as to parental involvement; therefore, data could not be extracted. | The five studies identified as being comprehensive and with parental involvement resulted in significant reductions in child BMI. |
| Verjans-Janssen (SR) [47] | To study effectiveness of school-based physical activity and nutrition interventions with direct parental involvement on children’s BMI or BMI z-score, physical activity, sedentary behavior and nutrition behavior. | Do school-based physical activity and nutrition interventions with direct parental involvement reduce BMI and/or BMI-z? |
18 studies of children aged 5 to 12 on average, all with direct parental involvement, and BMI or BMI-z scores as primary outcome
| 61% of school-based PA and nutrition interventions with direct parental involvement reduced child BMI or BMI-z. |
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ogden, C.L.; Carroll, M.D.; Lawman, H.G.; Fryar, C.D.; Kruszon-Moran, D.; Kit, B.K.; Flegal, K.M. Trends in Obesity Prevalence Among Children and Adolescents in the United States, 1988–1994 through 2013–2014. JAMA 2016, 315, 2292–2299. [Google Scholar] [CrossRef]
- Reilly, J.J.; Methven, E.; McDowell, Z.C.; Hacking, B.; Alexander, D.; Stewart, L.; Kelnar, C.J.H. Health consequences of obesity. Arch. Dis. Child. 2003, 88, 748–752. [Google Scholar] [CrossRef]
- Ayer, J.; Charakida, M.; Deanfield, J.; Celermajer, D.S. Lifetime risk: Childhood obesity and cardiovascular risk. Eur. Hear. J. 2015, 36, 1371–1376. [Google Scholar] [CrossRef] [Green Version]
- Latzer, Y.; Stein, D. A review of the psychological and familial perspectives of childhood obesity. J. Eat. Disord. 2013, 1, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Tsiros, M.; Olds, T.; Buckley, J.; Grimshaw, P.; Brennan, L.; Walkley, J.; Hills, A.; Howe, P.; Coates, A.M. Health-related quality of life in obese children and adolescents. Int. J. Obes. 2009, 33, 387–400. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, S.A.; Datar, A.; Narayan, K.V.; Kramer, M.R. Entrenched obesity in childhood: Findings from a national cohort study. Ann. Epidemiol. 2017, 27, 435–441. [Google Scholar] [CrossRef]
- Singh, A.S.; Mulder, C.; Twisk, J.W.R.; van Mechelen, W.; Chinapaw, M.J.M. Tracking of childhood overweight into adulthood: A systematic review of the literature. Obes. Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef]
- Simmonds, M.; Llewellyn, A.; Owen, C.; Woolacott, N. Predicting adult obesity from childhood obesity: A systematic review and meta-analysis. Obes. Rev. 2015, 17, 95–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGuire, M. Institute of Medicine. 2012. Accelerating Progress in Obesity Prevention: Solving the Weight of the Nation. Washington, DC: The National Academies Press. Adv. Nutr. 2012, 3, 708–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brug, J.; van Stralen, M.; Velde, S.J.T.; Chinapaw, M.J.M.; De Bourdeaudhuij, I.; Lien, N.; Bere, E.; Maskini, V.; Singh, A.S.; Maes, L.; et al. Differences in Weight Status and Energy-Balance Related Behaviors among Schoolchildren across Europe: The ENERGY-Project. PLoS ONE 2012, 7, e34742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhadoria, A.S.; Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R. Childhood obesity: Causes and consequences. J. Fam. Med. Prim. Care 2015, 4, 187–192. [Google Scholar] [CrossRef]
- Faught, E.; Ploeg, K.V.; Chu, Y.L.; Storey, K.; Veugelers, P. The influence of parental encouragement and caring about healthy eating on children’s diet quality and body weights. Public Health Nutr. 2015, 19, 822–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patrick, H.; Nicklas, T.A. A Review of Family and Social Determinants of Children’s Eating Patterns and Diet Quality. J. Am. Coll. Nutr. 2005, 24, 83–92. [Google Scholar] [CrossRef]
- Saltzman, J.A.; Pineros-Leano, M.; Liechty, J.M.; Bost, K.K.; Fiese, B.H. Eating, feeding, and feeling: Emotional responsiveness mediates longitudinal associations between maternal binge eating, feeding practices, and child weight. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, W.H.; Pfeiffer, K.A.; McIver, K.L.; Dowda, M.; Addy, C.L.; Pate, R.R. Social and Environmental Factors Associated with Preschoolers’ Nonsedentary Physical Activity. Child Dev. 2009, 80, 45–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robson, S.M.; Couch, S.C.; Peugh, J.L.; Glanz, K.; Zhou, C.; Sallis, J.F.; Saelens, B.E. Parent Diet Quality and Energy Intake Are Related to Child Diet Quality and Energy Intake. J. Acad. Nutr. Diet. 2016, 116, 984–990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors Influencing Children’s Eating Behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef] [Green Version]
- Yee, A.Z.H.; Lwin, M.O.; Ho, S.S. Promoting Healthier Eating via Parental Communication: Development and Validation of the Active and Restrictive Parental Guidance Questionnaire (PARQ). Health Commun. 2020, 1–13. [Google Scholar] [CrossRef]
- Petersen, T.L.; Møller, L.B.; Brønd, J.C.; Jepsen, R.; Grøntved, A. Association between parent and child physical activity: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Carson, V.; Langlois, K.; Colley, R. Associations between parent and child sedentary behaviour and physical activity in early childhood. Health Rep. 2020, 31, 3–10. [Google Scholar] [CrossRef]
- Langford, R.; Bonnell, C.P.; Jones, H.; Pouliou, T.; Murphy, S.M.; Waters, E.; Komro, K.A.; Gibbs, L.; Magnus, D.; Campbell, R. The WHO Health Promoting School framework for improving the health and well-being of students and their academic achievement. Cochrane Database Syst Rev. 2014. [Google Scholar] [CrossRef]
- Roseman, M.G.; Riddell, M.C.; Haynes, J.N. A Content Analysis of Kindergarten-12th Grade School-based Nutrition Interventions: Taking Advantage of Past Learning. J. Nutr. Educ. Behav. 2011, 43, 2–18. [Google Scholar] [CrossRef]
- Roseman, M.G.; Riddell, M.C.; McGee, J.J. Kindergarten to 12th Grade School-Based Nutrition Interventions: Putting Past Recommendations into Practice. J. Nutr. Educ. Behav. 2020, 52, 808–820. [Google Scholar] [CrossRef]
- Matwiejczyk, L.; Mehta, K.; Scott, J.; Tonkin, E.; Coveney, J. Characteristics of Effective Interventions Promoting Healthy Eating for Pre-Schoolers in Childcare Settings: An Umbrella Review. Nutrients 2018, 10, 293. [Google Scholar] [CrossRef] [Green Version]
- Ayala-Marín, A.M.; Iguacel, I.; De Miguel-Etayo, P.; Moreno, L.A. Consideration of Social Disadvantages for Understanding and Preventing Obesity in Children. Front Public Health 2020, 8, 423. [Google Scholar] [CrossRef]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing systematic reviews. Int. J. Evidence Based Heal. 2015, 13, 132–140. [Google Scholar] [CrossRef] [Green Version]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Ioannidis, J.P. Integration of evidence from multiple meta-analyses: A primer on umbrella reviews, treatment networks and multiple treatments meta-analyses. Can. Med Assoc. J. 2009, 181, 488–493. [Google Scholar] [CrossRef] [Green Version]
- Rajjo, T.; Mohammed, K.; Alsawas, M.; Ahmed, A.T.; Farah, W.; Asi, N.; Almasri, J.; Prokop, L.J.; Murad, M.H. Treatment of Pediatric Obesity: An Umbrella Systematic Review. J. Clin. Endocrinol. Metab. 2017, 102, 763–775. [Google Scholar] [CrossRef] [Green Version]
- Chai, L.K.; Collins, C.; May, C.; Brain, K.; See, D.W.; Burrows, T. Effectiveness of family-based weight management interventions for children with overweight and obesity. JBI Database Syst. Rev. Implement. Rep. 2019, 17, 1341–1427. [Google Scholar] [CrossRef]
- Safron, M.; Cislak, A.; Gaspar, T.; Luszczynska, A. Effects of School-based Interventions Targeting Obesity-Related Behaviors and Body Weight Change: A Systematic Umbrella Review. Behav. Med. 2011, 37, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Goldthorpe, J.; Epton, T.; Keyworth, C.; Calam, R.; Armitage, C.J. Are primary/elementary school-based interventions effective in preventing/ameliorating excess weight gain? A systematic review of systematic reviews. Obes. Rev. 2020, 21. [Google Scholar] [CrossRef]
- Hayba, N.; Rissel, C.; Farinelli, M.A. Effectiveness of lifestyle interventions in preventing harmful weight gain among adolescents: A systematic review of systematic reviews. Obes. Rev. 2020, 22, e13109. [Google Scholar] [CrossRef]
- Psaltopoulou, T.; Tzanninis, S.; Ntanasis-Stathopoulos, I.; Panotopoulos, G.; Kostopoulou, M.; Tzanninis, I.-G.; Tsagianni, A.; Sergentanis, T.N. Prevention and treatment of childhood and adolescent obesity: A systematic review of meta-analyses. World J. Pediatr. 2019, 15, 350–381. [Google Scholar] [CrossRef] [PubMed]
- Ornstein, P.A.; Haden, C.A.; Hedrick, A.M. Learning to remember: Social-communicative exchanges and the development of children’s memory skills. Dev. Rev. 2004, 24, 374–395. [Google Scholar] [CrossRef]
- Smetana, J.G. Toddlers’ social interactions in the context of moral and conventional transgressions in the home. Dev. Psychol. 1989, 25, 499–508. [Google Scholar] [CrossRef]
- Garon, N.M.; Longard, J.; Bryson, S.E.; Moore, C. Making decisions about now and later: Development of future-oriented self-control. Cogn. Dev. 2012, 27, 314–322. [Google Scholar] [CrossRef]
- Kuczmarski, R.J.; Ogden, C.L.; Guo, S.S.; Grummer-Strawn, L.M.; Flegal, K.M.; Mei, Z.; Wei, R.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. 2000 CDC growth charts for the United States: Methods and development. Vital. Health Stat. 2002, 11, 1–190. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- Aromataris, E.; Fernandez, R.; Godfrey, C.; Holly, C.; Khalil, H.; Tungpunkom, P. Methodology for JBI umbrella reviews. In Joanna Briggs Institute Reviewers’ Manual: 2014 Edition; The Joanna Briggs Institute: Adelaide, Australia, 2014; pp. 1–34. [Google Scholar]
- Ewald, H.; Kirby, J.; Rees, K.; Robertson, W. Parent-only interventions in the treatment of childhood obesity: A systematic review of randomized controlled trials. J. Public Health 2013, 36, 476–489. [Google Scholar] [CrossRef] [Green Version]
- Jang, M.; Chao, A.; Whittemore, R. Evaluating Intervention Programs Targeting Parents to Manage Childhood Overweight and Obesity: A Systematic Review Using the RE-AIM Framework. J. Pediatr. Nurs. 2015, 30, 877–887. [Google Scholar] [CrossRef]
- Laws, R.; Campbell, K.J.; Van Der Pligt, P.; Russell, G.; Ball, K.; Lynch, J.; Crawford, D.; Taylor, R.; Askew, D.; Denney-Wilson, E. The impact of interventions to prevent obesity or improve obesity related behaviours in children (0–5 years) from socioeconomically disadvantaged and/or indigenous families: A systematic review. BMC Public Health 2014, 14, 779. [Google Scholar] [CrossRef] [Green Version]
- McLean, N.; Griffin, S.; Toney, K.; Hardeman, W. Family involvement in weight control, weight maintenance and weight-loss interventions: A systematic review of randomised trials. Int. J. Obes. 2003, 27, 987–1005. [Google Scholar] [CrossRef] [Green Version]
- Nixon, C.A.; Moore, H.J.; Douthwaite, W.; Gibson, E.L.; Vogele, C.; Kreichauf, S.; Wildgruber, A.; Manios, Y.; Summerbell, C.D.; ToyBox-Study Group. Identifying effective behavioural models and behaviour change strategies underpinning preschool- and school-based obesity prevention interventions aimed at 4-6-year-olds: A systematic review. Obes. Rev. 2012, 13, 106–117. [Google Scholar] [CrossRef]
- Verjans-Janssen, S.R.B.; Van De Kolk, I.; van Kann, D.H.H.; Kremers, S.P.J.; Gerards, S.M.P.L. Effectiveness of school-based physical activity and nutrition interventions with direct parental involvement on children’s BMI and energy balance-related behaviors—A systematic review. PLoS ONE 2018, 13, e0204560. [Google Scholar] [CrossRef]
- Young, K.M.; Northern, J.J.; Lister, K.M.; Drummond, J.A.; O’Brien, W.H. A meta-analysis of family-behavioral weight-loss treatments for children. Clin. Psychol. Rev. 2007, 27, 240–249. [Google Scholar] [CrossRef]
- Gori, D.; Guaraldi, F.; Cinocca, S.; Moser, G.; Rucci, P.; Fantini, M.P. Effectiveness of educational and lifestyle interventions to prevent paediatric obesity: Systematic review and meta-analyses of randomized and non-randomized controlled trials. Obes. Sci. Pr. 2017, 3, 235–248. [Google Scholar] [CrossRef]
- Loveman, E.; Al-Khudairy, L.; Johnson, R.; Robertson, W.; Colquitt, J.L.; Mead, E.L.; Ells, L.J.; Metzendorf, M.-I.; Rees, K. Parent-only interventions for childhood overweight or obesity in children aged 5 to 11 years. Cochrane Database Syst. Rev. 2015, 21, CD012008. [Google Scholar] [CrossRef] [Green Version]
- Mead, E.; Brown, T.; Rees, K.; Azevedo, L.B.; Whittaker, V.; Jones, D.; Olajide, J.; Mainardi, G.M.; Corpeleijn, E.; O’Malley, C.; et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese children from the age of 6 to 11 years. Cochrane Database Syst. Rev. 2017, 2017, CD012651. [Google Scholar] [CrossRef] [Green Version]
- Luttikhuis, H.O.; Baur, L.; Jansen, H.; Shrewsbury, V.A.; O’Malley, C.; Stolk, R.; Summerbell, C. Interventions for treating obesity in children. Cochrane Database Syst. Rev. 2009, 21, CD001872. [Google Scholar] [CrossRef] [Green Version]
- Sbruzzi, G.; Eibel, B.; Barbiero, S.M.; Petkowicz, R.O.; Ribeiro, R.A.; Cesa, C.C.; Martins, C.C.; Marobin, R.; Schaan, C.W.; Souza, W.B.; et al. Educational interventions in childhood obesity: A systematic review with meta-analysis of randomized clinical trials. Prev. Med. 2013, 56, 254–264. [Google Scholar] [CrossRef]
- Sobol-Goldberg, S.; Rabinowitz, J.; Gross, R. School-based obesity prevention programs: A meta-analysis of randomized controlled trials. Obesity 2013, 21, 2422–2428. [Google Scholar] [CrossRef] [PubMed]
- Oosterhoff, M.; Joore, M.; Ferreira, I. The effects of school-based lifestyle interventions on body mass index and blood pressure: A multivariate multilevel meta-analysis of randomized controlled trials. Obes. Rev. 2016, 17, 1131–1153. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, T.M.; Chen, T.A.; Baranowski, J.; Thompson, D.; Baranowski, T. Physical activity and screen-media-related parenting practices have different associations with children’s objectively measured physical activity. Child Obes. 2013, 9, 446–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, S.A.; Belanger, M.; Donovan, D.; Carrier, N. Systematic review of the relationship between childcare educators’ practices and preschoolers’ physical activity and eating behaviours. Obes. Rev. 2015, 16, 1055–1070. [Google Scholar] [CrossRef] [Green Version]
- Garriguet, D.; Colley, R.; Bushnik, T. Parent-Child association in physical activity and sedentary behaviour. Health Rep. 2017, 28, 3–11. [Google Scholar]
- Mannocci, A.; D’Egidio, V.; Backhaus, I.; Federici, A.; Sinopoli, A.; Varela, A.R.; Villari, P.; La Torre, G. Are There Effective Interventions to Increase Physical Activity in Children and Young People? An Umbrella Review. Int. J. Environ. Res. Public Health 2020, 17, 3528. [Google Scholar] [CrossRef]
- Skelton, K.R.; Lowe, C.; Zaltz, D.A.; Benjamin-Neelon, S.E. Garden-based interventions and early childhood health: An umbrella review. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.N.; Rollo, M.E.; Watson, J.; Burrows, T.L.; Collins, C.E. Relationships between dietary intakes of children and their parents: A cross-sectional, secondary analysis of families participating in the Family Diet Quality Study. J. Hum. Nutr. Diet. 2014, 28, 443–451. [Google Scholar] [CrossRef]
- Collins, C.; Duncanson, K.; Burrows, T. A systematic review investigating associations between parenting style and child feeding behaviours. J. Hum. Nutr. Diet. 2014, 27, 557–568. [Google Scholar] [CrossRef]
- Hubbs-Tait, L.; Kennedy, T.S.; Page, M.C.; Topham, G.L.; Harrist, A.W. Parental Feeding Practices Predict Authoritative, Authoritarian, and Permissive Parenting Styles. J. Am. Diet. Assoc. 2008, 108, 1154–1161. [Google Scholar] [CrossRef] [PubMed]

| Treatment Focused | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Author, Year a | Year Range of Primary Studies | Number of Primary Studies | Participant Number | Participant Characteristics | Study Setting (s) | Country of Origin of Included Studies b | Intervention Targets Included | Target Group (Comparators) | Study Design of Primary Studies | Meta-Analysis Conducted | |
| Nutr | PA | ||||||||||
| Ewald, 2014 | 1998–2011 | 8 studies reported in 10 papers and 2 protocols (12 papers in total) | 466 | Children aged 5–14 years (stated objective to target 5–12 years); children with overweight or obesity at baseline | Family based, university, hospital/outpatient, community | Israel, USA, Switzerland, Australia | ✓ | ✓ | Parent-only (parent-child, child-only) | RCTs | No |
| Jang, 2015 | 2007–2014 | 7 studies reported in 8 papers | 765 c | Children aged 3–13 years (mean age < 10 in 6/7 studies); majority non-Hispanic white (when reported); children with overweight or obesity at baseline | Community, hospital, university, not specified | USA, Australia, Netherlands, Belgium | ✓ | ✓ | Parent-only (usual care, active control, alterative or partial intervention) | RCTs | No |
| Loveman, 2015 | 1975–2015 | 20 studies reported in 20 main papers for qualitative synthesis; of these, 14 studies were included for the meta-analysis | 3057 | Children aged 2–13 years (mean 4.9–11.5 years; stated objective to target 5–11 y); majority non-Hispanic White; children with overweight or obesity at baseline | Outpatient, community, university, primary care, combination | USA, Australia, Netherlands, Israel, Switzerland, Iran, Belgium | ✓ | ✓ | Parent-only (parent-child, waitlist control, minimal contact, other parent-only) | RCTs with at least six months of outcome assessment | Yes |
| McLean, 2003 * | 1981–1994 | 7 studies described in 11 papers | 300 | Children aged 6–13 | Not specified | USA, Sweden | ✓ | ✓ | Parent-child (comparators not specified) | Randomized trials | No |
| Mead, 2017 * | 1984–2016 | Analysis included 38 papers that described parental involvement (n = 35) or targeted parents (n = 3) | 4150 | Children aged 6–12 years Children with overweight, obesity, or severe obesity at baseline | Outpatient, primary care, home, community, hospital, school | USA, UK, Germany, Spain, Australia, Israel, Sweden, New Zealand, Italy, Mexico, Canada, Finland, Malaysia | ✓ | ✓ | Parent-child, parent-only (true control, usual/standard care, other parent-child) | RCTs with at least six months of follow-up | Yes |
| Oude Luttikhuis, 2009 * | 2006–2008 | 8 studies | 708 randomized (579 completed) | Children aged 5–12 years; children with overweight or obesity at baseline | Outpatient, school | Australia, Sweden, Israel, UK, Finland, Switzerland, unknown | ✓ | ✓ | Parent-only, parent-child (parent-child, other parent-only, waitlist control, usual/standard care) | RCTs | Yes |
| Sbruzzi, 2013 *,d | 2007–2011 | 8 studies | 849 | Children aged 6–12 years; children with overweight or obesity at baseline | Not specified | USA, UK, Australia, Finland, Sweden, Malaysia | ✓ | ✓ | Parent-only, parent-child, family-based (wait list control, usual/standard care, minimal contact) | RCTs | Yes |
| Young, 2007 | 1982–2004 | 16 studies | 666 | Children aged 5–13 years (stated objective to target 5–12 years); children with overweight or obesity at baseline | Not specified | Not specified | ✓ | ✓ | Parent as “helper” or parent treated Concurrently (other treatment, control) | Not reported | Yes |
| Treatment Participants | 10,961 | ||||||||||
| Prevention Focused | |||||||||||
| Gori, 2017 * | 2003–2014 | Mismatch in number of studies across published text, Table 1 | Not Extractable | Children aged 6–12 years Children with overweight or obesity at baseline | Family or combined family and school based | USA, Australia, Argentina, Italy, Netherlands, Israel, France, Spain, UK | ✓ | ✓ | Family, parent-child, not specified (usual/standard care, minimal contact, true control, not specified) | RCT, non-RCT | Yes |
| Laws, 2014 * | 2005–2013 | 7 studies | 4294 | Children aged 2.5–6 years Studies targeted preschools with high numbers of children with migrant, Black, Latino, or low-income backgrounds | Preschools | USA, France, Switzerland | ✓ | ✓ | Child-parent-teacher (comparators not specified) | Cluster RCT, quasi-experimental | No |
| Nixon, 2012 * | 1998–2010 | 7 studies that included parental involvement | Not Specified | Children aged 4–6.9 years | Preschools and schools | Germany, Greece, Scotland, Switzerland, USA, Australia, China, England, New Zealand, Thailand | ✓ | ✓ | Parent-child, not specified (comparators not specified) | RCTs, non-RCTs | No |
| Oosterhoff, 2016 * | 1985–2013 | 83 studies reported in 89 papers; 53 studies (in 54 papers) for which a parental component was described. All 83 studies were included in multivariable meta-regression model for BMI | 72,934 e | Children aged 4–12 years Range of BMIs at baseline; only 3 studies targeted children with overweight/obesity | Schools | Europe, North America, Oceania, South America, North Africa (individual countries not listed) | ✓ | ✓ | Target group not specified (control groups received no intervention beyond typical school-based activities per inclusion criteria) | RCTs | Yes |
| Sobol-Goldberg, 2013 * | Not Extractable | 8 studies for the target age range for which parental involvement is described | 7710 | Children aged 5–12 years Range of BMIs at baseline | Schools | Not extractable | ✓ | ✓ | Target group not specified (control groups received no intervention per inclusion criteria) | RCTs | Yes |
| Verjans-Janssen, 2018 * | 1999–2018 | 18 studies that included BMI/BMI z-score as an outcome | 34,361 | Children aged 4–12 years | Schools | China, USA, Australia, Greece, Chile, Germany, Italy, Mexico | ✓ | ✓ | Parent-child; all studies had direct parent involvement (comparators not specified) | RCT, quasi-experimental, pre-/post-test | No |
| Prevention Participants | 119,299 | ||||||||||
| Total Reported Participants | 130,260 f | ||||||||||
| AMSTAR-2 Item Number | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Review (Year), Treatment or Prevention Focus | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 |
| Ewald (2014), T | Y | N | N | PY | N | N | N | PY | Y | N | N/A | N/A | N | N | N/A | N |
| Gori (2017), P | Y | N | Y | N | N | N | N | Y | N | N | N | Y | Y | Y | N | Y |
| Jang (2015), T | Y | N | N | N | N | Y | N | Y | Y | N | N/A | N/A | Y | N | N/A | N |
| Laws (2014), P | Y | N | Y | N | N | N | N | N | N | N | N/A | N/A | N | N | N/A | Y |
| Loveman (2015), T | Y | PY | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y |
| McLean (2003), T | Y | N | N | N | N | N | N | N | N | N | N/A | N/A | N | N | N/A | N |
| Mead (2017), T | Y | PY | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Nixon (2012), P | N | N | N | N | Y | N | Y | N | N | N | N/A | N/A | N | N | N/A | Y |
| Oosterhoff (2016), P | Y | N | N | N | Y | N | N | N | PY | N | Y | Y | Y | Y | Y | Y |
| Oude Luttikhuis (2009), T | Y | PY | Y | PY | Y | Y | Y | Y | Y | Y | N | N | N | N | Y | Y |
| Sbruzzi (2013), T | Y | N | N | PY | Y | Y | N | PY | PY | N | Y | N | N | Y | N | Y |
| Sobol-Goldberg (2013), P | Y | PY | Y | N | N | Y | N | N | PY | N | N | N | N | N | Y | Y |
| Verjans-Janssen (2018), P | Y | N | Y | N | Y | N | N | N | PY | N | N/A | N/A | Y | Y | N/A | Y |
| Young (2007), T | N | N | N | N | Y | N | N | N | N | N | N | N | N | Y | N | N |
| Author (SR, MA, Both) | Research Question/Purpose | Umbrella Review Research Question (s) | Results | Conclusion |
|---|---|---|---|---|
| Ewald (SR) [42] | Are parent-only interventions effective treatments of obesity in children aged 5–12 years compared with child-only or parent-child interventions? | Are parent-only (PO) interventions better than child-only (CO) interventions? | 1/6 studies offered semi-equivalent PO vs. CO comparison and PO group showed significantly greater weight loss than CO. | PO may be better than CO. |
| Are parent-only (PO) interventions equivalent to parent-child (PC) interventions? | 4/6 studies revealed NS difference in weight status between PO and PC interventions. 1/6 studies revealed greater change in overweight for PO than PC intervention group. | PO and PC appear to be equivalent (4/6 versus 1/6). | ||
| Jang (SR) [43] | To evaluate interventions for child overweight and obesity that target parents. | Are interventions targeting parents and focused on children’s healthy eating (HE) and physical activity (PA) effective? | 5/7 studies that compared intervention group(s) to either a usual care group or a waitlist control group (WLC) revealed significant decreases in BMI or BMI z-scores. 2/7 studies that compared alternative interventions to the focal intervention did not reveal significant between-groups differences in BMI z-scores. | Interventions targeting parents and promoting child HE and PA are more effective than usual care or WLC. |
| Loveman (both) [50] | To assess the efficacy of diet, physical activity, and behavioral interventions delivered only to parents to treat obesity and overweight in children aged 5 to 11 years. | Are parent-only (PO) interventions better than wait list control conditions (WLC) and minimal contact control interventions (MCI)? | MA of PO versus WLC Change in BMI z score
Change in BMI z score
| There is evidence that PO interventions are better than WLC for reducing BMI Z scores. |
| There is no evidence that PO interventions are better than MCI interventions for reducing BMI Z scores, BMI percentile, and BMI. | ||||
| Are parent-only (PO) interventions equivalent to parent-child (PC) interventions? | MA of PO versus PC Change in BMI z score
| There is evidence that PO interventions and PC interventions are equivalent because no MA of PO versus PC revealed significant differences. | ||
| Are parent-only (PO) interventions equivalent to other parent only (OPO) interventions? | MA of PO versus OPO Change in BMI z score (No MA)
| There is evidence that PO interventions are equivalent to OPO interventions because only 1/7 studies revealed a significant difference. | ||
| McLean (SR) [45] | To identify trials evaluating family involvement in weight control, weight maintenance, and weight loss interventions targeting food intake and/or physical activity. | Did trials involving parents lead to weight control or weight loss? | Findings at post-intervention time point (2/7 led to improved outcomes; 5/7 did not) Trials comparing parent-child with child-only or parent-child with control group
| There is some evidence from trials comparing parent-child or family interventions with child-only interventions or controls. |
| There is no evidence that other types of trials led to weight control or weight loss. | ||||
| Mead (both) [51] | How effective are diet, physical activity and behavioral interventions in reducing the weight of children aged 6 to 11 years with overweight or obesity? | Are diet, PA, and behavioral interventions that include parental involvement more effective than no treatment/usual care? | Findings at final follow-up; analyzed studies classified as low-quality evidence Change in BMI—Parental Involvement
| Diet, PA, and behavioral interventions that include parental involvement are more effective than no treatment/usual care for every outcome evaluated:
|
| Oude Luttikhuis (both) [52] | To assess the efficacy of any combination of lifestyle (dietary, physical activity, behavioral therapy), drug or surgical interventions, compared with any other combination of these interventions or no treatment in children and adolescents. | Are behavioral family programs for treatment of childhood obesity better than standard or minimal care? Note: The authors switched the intervention and control groups of an included primary study (Golan 2006) to maintain consistency with other included studies so that parent-child was designated as the intervention group and parent-only as the control. | Behavioral interventions for families/parents and children; no report of cross-study quality Change in BMI Z score Only 8/24 studies met MA criterion for analyses to be based on intention-to-treat principles. MA of family programs versus minimal or standard care at 6 months or first assessment after 6 months 4/8 studies met all criteria for MA which revealed an effect of −0.06 (95% CI: −0.12 to −0.01), Z = 2.18, p = 0.03; 301 participants, I2 = 61%. Other 4 interventions for families/parents and children at 6 months
3/7 studies met all criteria for MA which revealed an effect of −0.04 (95% CI: −0.12 to 0.04), Z = 0.91, p = 0.36; 264 participants, I2 = 0.0%. Other 4 interventions for families/parents and children at 12 or 24 months follow up
| MA provides some evidence that parent/family programs are better than standard or minimal care. |
| Sbruzzi (both) [53] | To systematically review educational interventions, including behavioral modification, nutrition and physical activity, as compared to usual care or no intervention, for prevention or treatment of obesity in school children. 1 | Did treatment trials involving parents lead to decreased obesity compared to usual care or no intervention? | MA of treatment versus usual care or no interventionChange in BMI
| Treatment of obesity with behavior modification, nutrition, and/or physical activity leads to reduction in BMI. |
| Young (MA) [48] | To determine the effectiveness of family-based treatments for weight loss in children. | Are family-behavioral treatments (FBT) more effective than other treatments without parent involvement (OT)?Are FBT more effective than control conditions (CC)? | NOTE: I2 not reported. Quality not reported. Decrease in % overweight at post-test
Due to too few FBT studies for MA, individual treatment effects per study were reported.
| Family-behavioral treatments are more effective than other treatments without parental involvement. Family-behavioral treatments are more effective than control conditions. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomayko, E.J.; Tovar, A.; Fitzgerald, N.; Howe, C.L.; Hingle, M.D.; Murphy, M.P.; Muzaffar, H.; Going, S.B.; Hubbs-Tait, L. Parent Involvement in Diet or Physical Activity Interventions to Treat or Prevent Childhood Obesity: An Umbrella Review. Nutrients 2021, 13, 3227. https://doi.org/10.3390/nu13093227
Tomayko EJ, Tovar A, Fitzgerald N, Howe CL, Hingle MD, Murphy MP, Muzaffar H, Going SB, Hubbs-Tait L. Parent Involvement in Diet or Physical Activity Interventions to Treat or Prevent Childhood Obesity: An Umbrella Review. Nutrients. 2021; 13(9):3227. https://doi.org/10.3390/nu13093227
Chicago/Turabian StyleTomayko, Emily J., Alison Tovar, Nurgul Fitzgerald, Carol L. Howe, Melanie D. Hingle, Michael P. Murphy, Henna Muzaffar, Scott B. Going, and Laura Hubbs-Tait. 2021. "Parent Involvement in Diet or Physical Activity Interventions to Treat or Prevent Childhood Obesity: An Umbrella Review" Nutrients 13, no. 9: 3227. https://doi.org/10.3390/nu13093227
APA StyleTomayko, E. J., Tovar, A., Fitzgerald, N., Howe, C. L., Hingle, M. D., Murphy, M. P., Muzaffar, H., Going, S. B., & Hubbs-Tait, L. (2021). Parent Involvement in Diet or Physical Activity Interventions to Treat or Prevent Childhood Obesity: An Umbrella Review. Nutrients, 13(9), 3227. https://doi.org/10.3390/nu13093227