
Effects of Vitamin D3 Supplementation and Resistance Training on 25-Hydroxyvitamin D Status and Functional Performance of Older Adults: A Randomized Placebo-Controlled Trial

 , , , , ,
, , , , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Participants
2.3. Interventions
2.3.1. Nutrient Supplementation
2.3.2. Resistance Training
2.4. Outcomes
2.4.1. Vitamin D Status
2.4.2. 30-s Chair Stand Test
2.4.3. 30-s Arm Curl Test
2.4.4. Timed up and Go Test
2.4.5. Gait Speed
2.4.6. Six-Minute Walk Test
2.4.7. Anthropometry
2.4.8. Step Counts
2.5. Statistics
2.5.1. Sample Size Determination
2.5.2. Randomization and Blinding
2.5.3. Statistical Analyses
3. Results
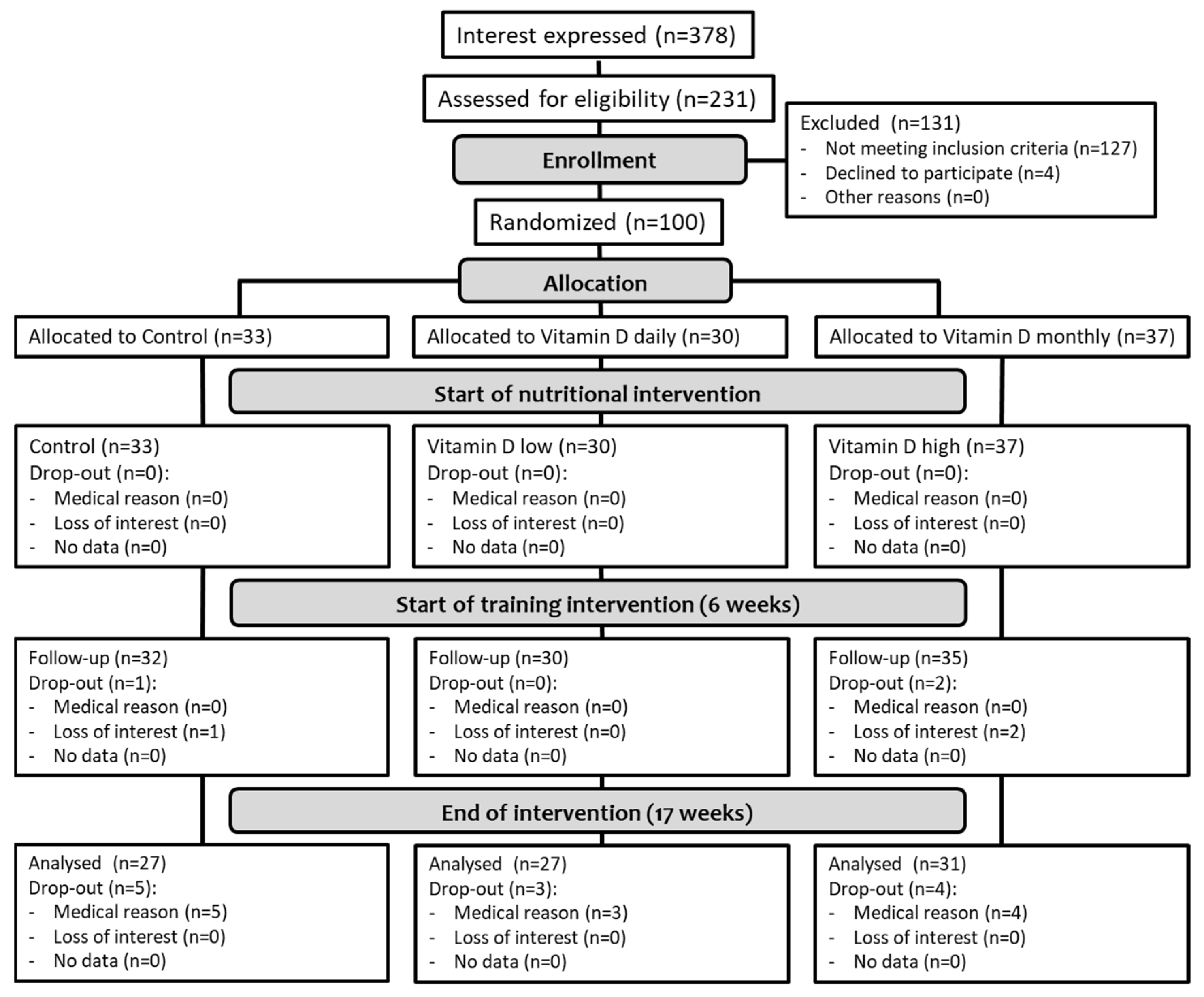
3.1. Participant Flow and Baseline Characteristics
3.2. 25(OH)D Status
3.3. Primary Outcome (30-s Chair Stand Test)
3.4. Secondary Outcomes (Physical Performance)
3.5. Covariates (Body Mass, Physical Activity)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Frontera, W.R.; Hughes, V.A.; Fielding, R.A.; Fiatarone, M.A.; Evans, W.J.; Roubenoff, R. Aging of skeletal muscle: A 12-yr longitudinal study. J. Appl. Physiol. 2000, 88, 1321–1326. [Google Scholar] [CrossRef] [PubMed]
- Maden-Wilkinson, T.M.; McPhee, J.S.; Jones, D.A.; Degens, H. Age-Related Loss of Muscle Mass, Strength, and Power and Their Association With Mobility in Recreationally-Active Older Adults in the United Kingdom. J. Aging Phys. Act. 2015, 23, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, J.; Neyens, J.C.; Van Rossum, E.; Spreeuwenberg, M.D.; De Witte, L.P. Predicting ADL disability in community-dwelling elderly people using physical frailty indicators: A systematic review. BMC Geriatr. 2011, 11, 33. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.Y.; Wei, S.H.; Chen, P.Y.; Tsai, M.W.; Cheng, I.C.; Liu, D.H.; Kao, C.L. Can sit-to-stand lower limb muscle power predict fall status? Gait Posture 2014, 40, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Westbury, L.D.; Syddall, H.E.; Fuggle, N.R.; Dennison, E.M.; Harvey, N.C.; Cauley, J.A.; Shiroma, E.J.; Fielding, R.A.; Newman, A.B.; Cooper, C. Relationships Between Level and Change in Sarcopenia and Other Body Composition Components and Adverse Health Outcomes: Findings from the Health, Aging, and Body Composition Study. Calcif. Tissue Int. 2021, 108, 302–313. [Google Scholar] [CrossRef]
- Guizelini, P.C.; de Aguiar, R.A.; Denadai, B.S.; Caputo, F.; Greco, C.C. Effect of resistance training on muscle strength and rate of force development in healthy older adults: A systematic review and meta-analysis. Exp. Gerontol. 2018, 102, 51–58. [Google Scholar] [CrossRef]
- Straight, C.R.; Lindheimer, J.B.; Brady, A.O.; Dishman, R.K.; Evans, E.M. Effects of Resistance Training on Lower-Extremity Muscle Power in Middle-Aged and Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Sports Med. 2016, 46, 353–364. [Google Scholar] [CrossRef]
- Norman, A.W. From vitamin D to hormone D: Fundamentals of the vitamin D endocrine system essential for good health. Am. J. Clin. Nutr. 2008, 88, 491S–499S. [Google Scholar] [CrossRef]
- Olsson, K.; Saini, A.; Strömberg, A.; Alam, S.; Lilja, M.; Rullman, E.; Gustafsson, T. Evidence for Vitamin D Receptor Expression and Direct Effects of 1α,25(OH)2D3 in Human Skeletal Muscle Precursor Cells. Endocrinology 2016, 157, 98–111. [Google Scholar] [CrossRef]
- Girgis, C.M.; Clifton-Bligh, R.J.; Mokbel, N.; Cheng, K.; Gunton, J.E. Vitamin D Signaling Regulates Proliferation, Differentiation, and Myotube Size in C2C12 Skeletal Muscle Cells. Endocrinology 2014, 155, 347–357. [Google Scholar] [CrossRef]
- Bischoff-Ferrari, H.A.; Dietrich, T.; Orav, E.J.; Hu, F.B.; Zhang, Y.; Karlson, E.W.; Dawson-Hughes, B. Higher 25-hydroxyvitamin D concentrations are associated with better lower-extremity function in both active and inactive persons aged ≥60 y. Am. J. Clin. Nutr. 2004, 80, 752–758. [Google Scholar] [CrossRef]
- Iolascon, G.; De Sire, A.; Calafiore, D.; Moretti, A.; Gimigliano, R.; Gimigliano, F. Hypovitaminosis D is associated with a reduction in upper and lower limb muscle strength and physical performance in post-menopausal women: A retrospective study. Aging Clin. Exp. Res. 2015, 27, 23–30. [Google Scholar] [CrossRef]
- Toffanello, E.D.; Perissinotto, E.; Sergi, G.; Zambon, S.; Musacchio, E.; Maggi, S.; Coin, A.; Sartori, L.; Corti, M.-C.; Baggio, G.; et al. Vitamin D and Physical Performance in Elderly Subjects: The Pro.V.A Study. PLoS ONE 2012, 7, e34950. [Google Scholar] [CrossRef] [PubMed]
- Shardell, M.; Semba, R.D.; Kalyani, R.R.; Hicks, G.E.; Bandinelli, S.; Ferrucci, L. Serum 25-Hydroxyvitamin D, Plasma Klotho, and Lower-Extremity Physical Performance Among Older Adults: Findings From the InCHIANTI Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2015, 70, 1156–1162. [Google Scholar] [CrossRef]
- Sohl, E.; De Jongh, R.T.; Heijboer, A.C.; Swart, K.M.; Brouwer-Brolsma, E.M.; Enneman, A.W.; De Groot, C.P.; Van Der Velde, N.; Dhonukshe-Rutten, R.A.; Lips, P.; et al. Vitamin D status is associated with physical performance: The results of three independent cohorts. Osteoporos. Int. 2013, 24, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Wicherts, I.S.; Van Schoor, N.M.; Boeke, A.J.; Visser, M.; Deeg, D.J.; Smit, J.; Knol, D.L.; Lips, P. Vitamin D Status Predicts Physical Performance and Its Decline in Older Persons. J. Clin. Endocrinol. Metab. 2007, 92, 2058–2065. [Google Scholar] [CrossRef] [PubMed]
- Dzik, K.P.; Kaczor, J.J. Mechanisms of vitamin D on skeletal muscle function: Oxidative stress, energy metabolism and anabolic state. Eur. J. Appl. Physiol. 2019, 119 (Suppl. 1), 825–839. [Google Scholar] [CrossRef] [PubMed]
- Rodman, J.S.; Baker, T. Changes in the kinetics of muscle contraction in vitamin D-depleted rats. Kidney Int. 1978, 13, 189–193. [Google Scholar] [CrossRef]
- Ryan, Z.C.; Craig, T.A.; Folmes, C.D.; Wang, X.; Lanza, I.R.; Schaible, N.S.; Salisbury, J.L.; Nair, K.S.; Terzic, A.; Sieck, G.C.; et al. 1α,25-Dihydroxyvitamin D3 Regulates Mitochondrial Oxygen Consumption and Dynamics in Human Skeletal Muscle Cells. J. Biol. Chem. 2016, 291, 1514–1528. [Google Scholar] [CrossRef]
- Beaudart, C.; Buckinx, F.; Rabenda, V.; Gillain, S.; Cavalier, E.; Slomian, J.; Petermans, J.; Reginster, J.-Y.; Bruyere, O. The Effects of Vitamin D on Skeletal Muscle Strength, Muscle Mass, and Muscle Power: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Endocrinol. Metab. 2014, 99, 4336–4345. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine, S. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Rosen, C.J.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; Kovacs, C.S.; et al. IOM Committee Members Respond to Endocrine Society Vitamin D Guideline. J. Clin. Endocrinol. Metab. 2012, 97, 1146–1152. [Google Scholar] [CrossRef]
- Holwerda, A.M.; Kouw, I.W.; Trommelen, J.; Halson, S.L.; Wodzig, W.K.; Verdijk, L.B.; Van Loon, L.J. Physical Activity Performed in the Evening Increases the Overnight Muscle Protein Synthetic Response to Presleep Protein Ingestion in Older Men. J. Nutr. 2016, 146, 1307–1314. [Google Scholar] [CrossRef] [PubMed]
- Bhasin, S.; Storer, T.W.; Berman, N.; Callegari, C.; Clevenger, B.; Phillips, J.; Bunnell, T.J.; Tricker, R.; Shirazi, A.; Casaburi, R. The Effects of Supraphysiologic Doses of Testosterone on Muscle Size and Strength in Normal Men. N. Engl. J. Med. 1996, 335, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Endo, Y.; Nourmahnad, A.; Sinha, I. Optimizing Skeletal Muscle Anabolic Response to Resistance Training in Aging. Front. Physiol. 2020, 11, 874. [Google Scholar] [CrossRef]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical Activity and Public Health in Older Adults. Med. Sci. Sports Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef]
- Amarante do Nascimento, M.; Januario, R.S.; Gerage, A.M.; Mayhew, J.L.; Cheche Pina, F.L.; Cyrino, E.S. Familiarization and Reliability of One Repetition Maximum Strength Testing in Older Women. J. Strength Cond. Res. 2013, 27, 1636–1642. [Google Scholar] [CrossRef] [PubMed]
- Wood, R.H.; Reyes, R.; Welsch, M.A.; Favaloro-Sabatier, J.; Sabatier, M.; Lee, C.M.; Johnson, L.G.; Hooper, P.F. Concurrent cardiovascular and resistance training in healthy older adults. Med. Sci. Sports Exerc. 2001, 33, 1751–1758. [Google Scholar] [CrossRef]
- Haff, G.G.; Triplett, N.T. Essentials of Strength Training and Conditioning, 4th ed.; Human Kinetics: Champaign, IL, USA, 2016. [Google Scholar]
- Rikli, R.E.; Jones, C.J. Development and Validation of a Functional Fitness Test for Community-Residing Older Adults. J. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Collado-Mateo, D.; Madeira, P.; Dominguez-Muñoz, F.J.; Villafaina, S.; Tomas-Carus, P.; Parraca, J.A. The Automatic Assessment of Strength and Mobility in Older Adults: A Test-Retest Reliability Study. Medicina 2019, 55, 270. [Google Scholar] [CrossRef] [PubMed]
- Mijnarends, D.M.; Meijers, J.M.; Halfens, R.J.; ter Borg, S.; Luiking, Y.C.; Verlaan, S.; Schoberer, D.; Cruz-Jentoft, A.J.; van Loon, L.J.; Schols, J.M. Validity and Reliability of Tools to Measure Muscle Mass, Strength, and Physical Performance in Community-Dwelling Older People: A Systematic Review. J. Am. Med. Dir. Assoc. 2013, 14, 170–178. [Google Scholar] [CrossRef]
- Hansen, B.H.; Kolle, E.; Dyrstad, S.M.; Holme, I.; Anderssen, S.A. Accelerometer-Determined Physical Activity in Adults and Older People. Med. Sci. Sports Exerc. 2012, 44, 266–272. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Oesen, S.; Halper, B.; Hofmann, M.; Jandrasits, W.; Franzke, B.; Strasser, E.-M.; Graf, A.; Tschan, H.; Bachl, N.; Quittan, M.; et al. Effects of elastic band resistance training and nutritional supplementation on physical performance of institutionalised elderly—A randomized controlled trial. Exp. Gerontol. 2015, 72, 99–108. [Google Scholar] [CrossRef]
- Francic, V.; Ursem, S.R.; Dirks, N.F.; Keppel, M.H.; Theiler-Schwetz, V.; Trummer, C.; Pandis, M.; Borzan, V.; Grübler, M.R.; Verheyen, N.D.; et al. The Effect of Vitamin D Supplementation on its Metabolism and the Vitamin D Metabolite Ratio. Nutrients 2019, 11, 2539. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.B.; Kane, L.; Bikle, D. Response of Vitamin D Concentration to Vitamin D3 Administration in Older Adults without Sun Exposure: A Randomized Double-Blind Trial. J. Am. Geriatr. Soc. 2016, 64, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Takacs, I.; Toth, B.E.; Szekeres, L.; Szabo, B.; Bakos, B.; Lakatos, P. Randomized clinical trial to comparing efficacy of daily, weekly and monthly administration of vitamin D3. Endocr. 2016, 55, 60–65. [Google Scholar] [CrossRef]
- Helde Frankling, M.; Norlin, A.C.; Hansen, S.; Wahren Borgstrom, E.; Bergman, P.; Bjorkhem-Bergman, L. Are Vitamin D3 Tablets and Oil Drops Equally Effective in Raising S-25-Hydroxyvitamin D Concentrations? A Post-Hoc Analysis of an Observational Study on Immunodeficient Patients. Nutrients 2020, 12, 1230. [Google Scholar] [CrossRef]
- Vieth, R. Vitamin D supplementation: Cholecalciferol, calcifediol, and calcitriol. Eur. J. Clin. Nutr. 2020, 74, 1493–1497. [Google Scholar] [CrossRef]
- Tripkovic, L.; Lambert, H.; Hart, K.; Smith, C.P.; Bucca, G.; Penson, S.; Chope, G.; Hypponen, E.; Berry, J.; Vieth, R.; et al. Comparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2012, 95, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Stöcklin, E.; Sidelnikov, E.; Willett, W.C.; Edel, J.O.; Stähelin, H.B.; Wolfram, S.; Jetter, A.; Schwager, J.; et al. Oral supplementation with 25(OH)D3versus vitamin D3: Effects on 25(OH)D levels, lower extremity function, blood pressure, and markers of innate immunity. J. Bone Miner. Res. 2012, 27, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Graeff-Armas, L.A.; Bendik, I.; Kunz, I.; Schoop, R.; Hull, S.; Beck, M. Supplemental 25-Hydroxycholecalciferol Is More Effective than Cholecalciferol in Raising Serum 25-Hydroxyvitamin D Concentrations in Older Adults. J. Nutr. 2020, 150, 73–81. [Google Scholar] [CrossRef]
- Houston, D.K.; Cesari, M.; Ferrucci, L.; Cherubini, A.; Maggio, D.; Bartali, B.; Johnson, M.A.; Schwartz, G.G.; Kritchevsky, S. Association Between Vitamin D Status and Physical Performance: The InCHIANTI Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2007, 62, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Aspell, N.; Laird, E.; Healy, M.; Lawlor, B.; O’Sullivan, M. Vitamin D Deficiency Is Associated With Impaired Muscle Strength And Physical Performance In Community-Dwelling Older Adults: Findings From The English Longitudinal Study Of Ageing. Clin. Interv. Aging 2019, 14, 1751–1761. [Google Scholar] [CrossRef]
- Verhaar, H.J.J.; Samson, M.M.; Jansen, P.A.F.; De Vreede, P.L.; Manten, J.W.; Duursma, S.A. Muscle strength, functional mobility and vitamin D in older women. Aging 2000, 12, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Stockton, K.A.; Mengersen, K.; Paratz, J.D.; Kandiah, D.; Bennell, K.L. Effect of vitamin D supplementation on muscle strength: A systematic review and meta-analysis. Osteoporos. Int. 2010, 22, 859–871. [Google Scholar] [CrossRef]
- Uusi-Rasi, K.; Patil, R.; Karinkanta, S.; Kannus, P.; Tokola, K.; Lamberg-Allardt, C.; Sievänen, H. Exercise and Vitamin D in Fall Prevention Among Older Women: A randomized clinical trial. JAMA Intern. Med. 2015, 175, 703–711. [Google Scholar] [CrossRef]
- Hornikx, M.; Van Remoortel, H.; Lehouck, A.; Mathieu, C.; Maes, K.; Gayan-Ramirez, G.; Decramer, M.; Troosters, T.; Janssens, W. Vitamin D supplementation during rehabilitation in COPD: A secondary analysis of a randomized trial. Respir. Res. 2012, 13, 84. [Google Scholar] [CrossRef]
- Agergaard, J.; Trostrup, J.; Uth, J.; Iversen, J.V.; Boesen, A.; Andersen, J.L.; Schjerling, P.; Langberg, H. Does vitamin-D intake during resistance training improve the skeletal muscle hypertrophic and strength response in young and elderly men?—a randomized controlled trial. Nutr. Metab. 2015, 12, 32. [Google Scholar] [CrossRef]
- Antoniak, A.E.; Greig, C.A. The effect of combined resistance exercise training and vitamin D 3 supplementation on musculoskeletal health and function in older adults: A systematic review and meta-analysis. BMJ Open 2017, 7, e014619. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.J.; Rikli, R.E.; Beam, W.C. A 30-s Chair-Stand Test as a Measure of Lower Body Strength in Community-Residing Older Adults. Res. Q. Exerc. Sport 1999, 70, 113–119. [Google Scholar] [CrossRef]
- Dunsky, A.; Ayalon, M.; Netz, Y. Arm-Curl Field Test for Older Women: Is it a Measure of Arm Strength? J. Strength Cond. Res. 2011, 25, 193–197. [Google Scholar] [CrossRef]
- Glenn, J.M.; Gray, M.; Binns, A. The effects of loaded and unloaded high-velocity resistance training on functional fitness among community-dwelling older adults. Age Ageing 2015, 44, 926–931. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Barbalho, M.S.M.; Gentil, P.; Izquierdo, M.; Fisher, J.; Steele, J.; Raiol, R.A. There are no no-responders to low or high resistance training volumes among older women. Exp. Gerontol. 2017, 99, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Fahlman, M.M.; McNevin, N.; Boardley, D.; Morgan, A.; Topp, R. Effects of Resistance Training on Functional Ability in Elderly Individuals. Am. J. Health Promot. 2011, 25, 237–243. [Google Scholar] [CrossRef]
- Byrne, C.; Faure, C.; Keene, D.J.; Lamb, S.E. Ageing, Muscle Power and Physical Function: A Systematic Review and Implications for Pragmatic Training Interventions. Sports Med. 2016, 46, 1311–1332. [Google Scholar] [CrossRef] [PubMed]
- da Rosa Orssatto, L.B.; de la Rocha Freitas, C.; Shield, A.J.; Silveira Pinto, R.; Trajano, G.S. Effects of resistance training concentric velocity on older adults’ functional capacity: A systematic review and meta-analysis of randomised trials. Exp. Gerontol. 2019, 127, 110731. [Google Scholar] [CrossRef]
- Braith, R.W.; Graves, J.E.; Pollock, M.L.; Leggett, S.L.; Carpenter, D.M.; Colvin, A.B. Comparison of 2 vs 3 Days/Week of Variable Resistance Training During 10- and 18-Week Programs. Int. J. Sports Med. 1989, 10, 450–454. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and Validation of Criterion-Referenced Clinically Relevant Fitness Standards for Maintaining Physical Independence in Later Years. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| CON | VDD | VDM | p-Value | Partial η2 | |
|---|---|---|---|---|---|
| Sex (f/m) | 10/23 (30.3% f) | 10/20 (33.3% f) | 13/24 (35.1% f) | 0.911 | |
| Age (years) | 68.9 (67.0–72.9) | 68.7 (66.9–74.8) | 69.9 (67.0–74.3) | 0.763 | 0.005 |
| Body mass (kg) | 77.4 (65.5–83.4) | 85.8 (73.5–93.1) | 80.3 (72.3–93.8) | 0.123 | 0.042 |
| Height (m) | 1.73 (1.66–1.79) | 1.73 (1.66–1.79) | 1.73 (1.67–1.81) | 0.932 | 0.001 |
| BMI (kg/m²) | 25.7 (23.0–27.5) | 27.2 (25.1–30.7) | 27.6 (24.4–30.0) | 0.059 | 0.057 |
| 25(OH)D (ng/mL) | 22.8 (18.2–26.6) | 23.8 (20.1–28.1) | 23.4 (18.6–26.4) | 0.436 | 0.017 |
| Steps (counts/d) | 7022 (5590–9588) | 7021 (4937–9353) | 6610 (5208–9247) | 0.482 | 0.016 |
| Parameter | Group | t1 | t2 | t3 | Δ (t2 − t1) | Δ (t3 − t2) | Time | Group | Time × Group |
|---|---|---|---|---|---|---|---|---|---|
| 25(OH)D (ng/mL), n = 85 | CON | 21.7 (17.3–27.0) | 22.1 (17.3–21.3) | 23.7 (20.4–28.1) | 0.29 (−1.82–1.83) | 1.32 (−1.69–6.35) | <0.001 | 0.022 | 0.021 |
| VDD | 23.7 (18.9–28.1) | 24.2 (21.3–26.7) | 29.0 (23.8–33.3) **,° | 1.26 (−1.42–3.49) | 3.80 (−0.43–6.90) | ||||
| VDM | 23.4 (18.8–25.9) | 26.0 (21.5–29.7) | 32.7 (28.9–35.7) ***,°°° | 3.11 (−0.04–4.84) | 6.62 (3.60–10.91) ## | ||||
| 30-s chair stand test (reps), n = 84 | CON | 13 (11–14) | 14 (12–15) | 15 (14–18) | 1 (0–2) | 1 (1–3) | <0.001 | 0.316 | 0.859 |
| VDD | 13 (11–15) | 14 (13–16) | 16 (14–18) | 1 (0–3) | 1 (0–3) | ||||
| VDM | 12 (11–14) | 13 (12–15) | 16 (13–17) | 1 (0–2) | 2 (0–3) | ||||
| total | 12 (11–14) | 14 (12–15) *** | 15 (14–17) ***,°°° | 1 (0–2) | 1 (0–3) # | ||||
| 30-s arm curl test (dom) (reps), n = 83 | CON | 18 (16–20) | 20 (17–21) | 22 (20–24) | 1 (0–2) | 3 (2–5) | <0.001 | 0.311 | 0.659 |
| VDD | 19 (15–22) | 20 (19–25) | 23 (20–27) | 1 (0–3) | 3 (1–4) | ||||
| VDM | 19 (17–21) | 19 (17–22) | 22 (20–24) | 1 (−1–2) | 3 (1–6) | ||||
| total | 19 (16–21) | 19 (17–21) *** | 22 (20–24) ***,°°° | 1 (0–2) | 3 (1–5) ### | ||||
| 30-s arm curl test (non–dom) (reps), n = 82 | CON | 17 (16–21) | 18 (16–21) | 21 (19–24) | 0 (−1–2) | 3 (1–5) | <0.001 | 0.213 | 0.327 |
| VDD | 18 (15–21) | 20 (18–24) | 22 (21–25) | 2 (0–3) | 2 (1–5) | ||||
| VDM | 18 (16–20) | 20 (17–21) | 22 (20–24) | 1 (0–3) | 3 (1–5) | ||||
| total | 18 (16–21) | 19 (17–21) *** | 22 (20–24) ***,°°° | 1 (0–3) | 3 (1–5) ### | ||||
| Timed up and go test (s), n = 85 | CON | 4.72 (4.16–5.20) | 4.71 (4.10–5.10) | 4.45 (3.96–5.38) | −0.07 (−0.19–0.13) | −0.15 (−0.36–0.21) | 0.008 | 0.916 | 0.470 |
| VDD | 4.82 (4.24–5.34) | 4.44 (3.99–5.30) | 4.86 (4.03–5.18) | −0.25 (−0.46–0.07) | 0.12 (−0.22–0.44) | ||||
| VDM | 4.45 (4.19–4.81) | 4.57 (4.08–5.11) | 4.41 (4.07–4.99) | −0.09 (−0.37–0.30) | −0.09 (−0.39–0.13) | ||||
| total | 4.66 (4.19–5.24) | 4.57 (4.06–5.11) | 4.50 (4.04–5.08) * | −0.09 (−0.38–0.14) | −0.08 (−0.35–0.25) | ||||
| Gait speed (m/s), n = 85 | CON | 1.54 (1.47–1.76) | 1.69 (1.36–1.89) | 1.67 (1.44–1.83) | 0.04 (−0.02–0.16) | 0.06 (−0.13–0.12) | 0.016 | 0.823 | 0.320 |
| VDD | 1.59 (1.37–1.83) | 1.75 (1.45–1.87) | 1.61 (1.36–1.88) | 0.04 (−0.05–0.14) | −0.04 (−0.14–0.09) | ||||
| VDM | 1.66 (1.41–1.84) | 1.63 (1.50–1.86) | 1.65 (1.48–1.87) | 0.02 (−0.08–0.12) | 0.06 (−0.03–0.15) | ||||
| total | 1.61 (1.42–1.83) | 1.68 (1.48–1.86) | 1.65 (1.47–1.85) * | 0.04 (−0.06–0.14) | 0.03 (−0.12–0.13) | ||||
| 6-min walk test (m), n = 84 | CON | 636 (549–674) | 643 (570–692) | 628 (581–687) | 18.8 (−4.9–34.7) | 6.7 (−19.8–15.3) | 0.013 | 0.593 | 0.848 |
| VDD | 610 (570–691) | 618 (571–724) | 623 (554–723) | 1.3 (−17.8–30.4) | −1.9 (−23.8–24.6) | ||||
| VDM | 654 (605–697) | 660 (627–716) | 638 (604–713) | 10.0 (−14.4–28.4) | −0.9 (−21.7–28.6) | ||||
| total | 641 (573–689) | 648 (574–707) * | 628 (584–718) * | 9.9 (−10.6–29.29 | −0.05 (−22.5–20.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aschauer, R.; Unterberger, S.; Zöhrer, P.A.; Draxler, A.; Franzke, B.; Strasser, E.-M.; Wagner, K.-H.; Wessner, B. Effects of Vitamin D3 Supplementation and Resistance Training on 25-Hydroxyvitamin D Status and Functional Performance of Older Adults: A Randomized Placebo-Controlled Trial. Nutrients 2022, 14, 86. https://doi.org/10.3390/nu14010086
Aschauer R, Unterberger S, Zöhrer PA, Draxler A, Franzke B, Strasser E-M, Wagner K-H, Wessner B. Effects of Vitamin D3 Supplementation and Resistance Training on 25-Hydroxyvitamin D Status and Functional Performance of Older Adults: A Randomized Placebo-Controlled Trial. Nutrients. 2022; 14(1):86. https://doi.org/10.3390/nu14010086
Chicago/Turabian StyleAschauer, Rudolf, Sandra Unterberger, Patrick A. Zöhrer, Agnes Draxler, Bernhard Franzke, Eva-Maria Strasser, Karl-Heinz Wagner, and Barbara Wessner. 2022. "Effects of Vitamin D3 Supplementation and Resistance Training on 25-Hydroxyvitamin D Status and Functional Performance of Older Adults: A Randomized Placebo-Controlled Trial" Nutrients 14, no. 1: 86. https://doi.org/10.3390/nu14010086
APA StyleAschauer, R., Unterberger, S., Zöhrer, P. A., Draxler, A., Franzke, B., Strasser, E.-M., Wagner, K.-H., & Wessner, B. (2022). Effects of Vitamin D3 Supplementation and Resistance Training on 25-Hydroxyvitamin D Status and Functional Performance of Older Adults: A Randomized Placebo-Controlled Trial. Nutrients, 14(1), 86. https://doi.org/10.3390/nu14010086