
Scope of Use and Effectiveness of Dietary Interventions for Improving Health-Related Outcomes in Veterans: A Systematic Review


Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Study Eligibility Criteria
2.3. Screening and Data Extraction
2.4. Risk of Bias Assessment
2.5. Data Synthesis
3. Results
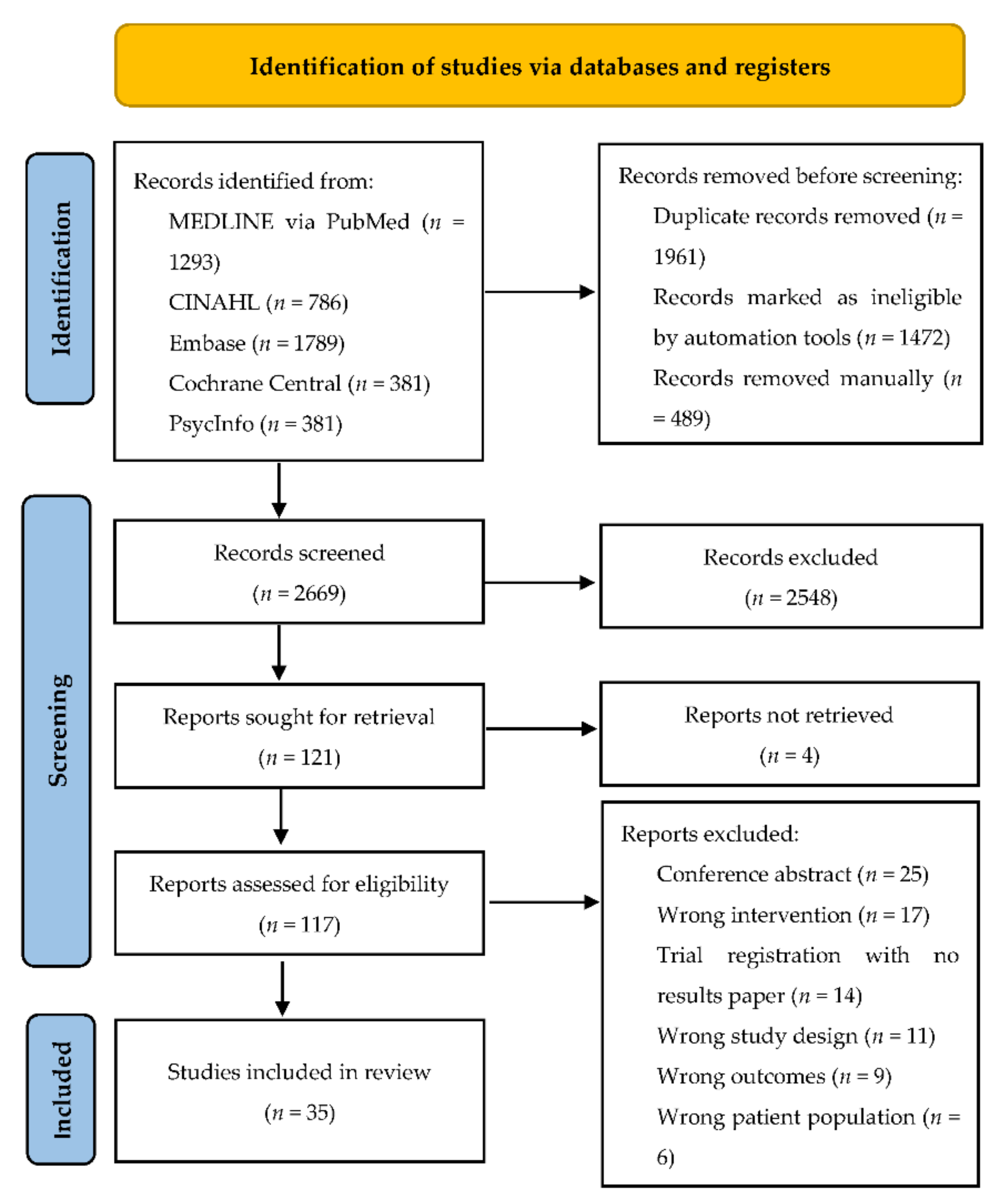
3.1. Study Selection
3.2. Risk of Bias
3.3. Study Characteristics
3.4. Veteran Populations and Dietary Interventions
3.5. Attendance and Attrition
3.6. Health-Related Outcome Measures
3.7. Weight and BMI
3.8. Blood Pressure
3.9. Blood Composition or Metabolic Parameters
3.10. Other Health-Related Outcomes
3.11. The MOVE! Weight Management Program
3.12. Health-Related Study Outcomes
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Boscarino, J.A. Diseases among men 20 years after exposure to severe stress: Implications for clinical research and medical care. Psychosom. Med. 1997, 59, 605–614. [Google Scholar] [CrossRef]
- Yoon, J.; Zulman, D.; Scott, J.Y.; Maciejewski, M.L. Costs associated with multimorbidity among VA patients. Med. Care 2014, 52 (Suppl. S3), S31–S36. [Google Scholar] [CrossRef]
- Kazis, L.E.; Miller, D.R.; Clark, J.; Skinner, K.; Lee, A.; Rogers, W.; Spiro, A., 3rd; Payne, S.; Fincke, G.; Selim, A.; et al. Health-related quality of life in patients served by the Department of Veterans Affairs: Results from the Veterans Health Study. Arch. Intern. Med. 1998, 158, 626–632. [Google Scholar] [CrossRef]
- Hundt, N.E.; Barrera, T.L.; Robinson, A.; Cully, J.A. A systematic review of cognitive behavioral therapy for depression in Veterans. Mil. Med. 2014, 179, 942–949. [Google Scholar] [CrossRef] [Green Version]
- Puetz, T.W.; Youngstedt, S.D.; Herring, M.P. Effects of Pharmacotherapy on Combat-Related PTSD, Anxiety, and Depression: A Systematic Review and Meta-Regression Analysis. PLoS ONE 2015, 10, e0126529. [Google Scholar] [CrossRef] [Green Version]
- Stelmach-Mardas, M.; Walkowiak, J. Dietary Interventions and Changes in Cardio-Metabolic Parameters in Metabolically Healthy Obese Subjects: A Systematic Review with Meta-Analysis. Nutrients 2016, 8, 455. [Google Scholar] [CrossRef] [Green Version]
- Silva, A.R.; Bernardo, A.; Costa, J.; Cardoso, A.; Santos, P.; de Mesquita, M.F.; Vaz Patto, J.; Moreira, P.; Silva, M.L.; Padrao, P. Dietary interventions in fibromyalgia: A systematic review. Ann. Med. 2019, 51, 2–14. [Google Scholar] [CrossRef] [Green Version]
- Philippou, E.; Petersson, S.D.; Rodomar, C.; Nikiphorou, E. Rheumatoid arthritis and dietary interventions: Systematic review of clinical trials. Nutr. Rev. 2021, 79, 410–428. [Google Scholar] [CrossRef]
- Opie, R.S.; O’Neil, A.; Itsiopoulos, C.; Jacka, F.N. The impact of whole-of-diet interventions on depression and anxiety: A systematic review of randomised controlled trials. Public Health Nutr. 2015, 18, 2074–2093. [Google Scholar] [CrossRef]
- Knowles, K.A.; Sripada, R.K.; Defever, M.; Rauch, S.A.M. Comorbid mood and anxiety disorders and severity of posttraumatic stress disorder symptoms in treatment-seeking veterans. Psychol. Trauma 2019, 11, 451–458. [Google Scholar] [CrossRef]
- Ravera, A.; Carubelli, V.; Sciatti, E.; Bonadei, I.; Gorga, E.; Cani, D.; Vizzardi, E.; Metra, M.; Lombardi, C. Nutrition and Cardiovascular Disease: Finding the Perfect Recipe for Cardiovascular Health. Nutrients 2016, 8, 363. [Google Scholar] [CrossRef] [PubMed]
- Evert, A.B.; Dennison, M.; Gardner, C.D.; Garvey, W.T.; Lau, K.H.K.; MacLeod, J.; Mitri, J.; Pereira, R.F.; Rawlings, K.; Robinson, S.; et al. Nutrition Therapy for Adults with Diabetes or Prediabetes: A Consensus Report. Diabetes Care 2019, 42, 731–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, P.H.; Aronson, W.; Freedland, S.J. Nutrition, dietary interventions and prostate cancer: The latest evidence. BMC Med. 2015, 13, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, T.J.W.; Cervenka, M.C. Lessons learned from recent clinical trials of ketogenic diet therapies in adults. Curr. Opin. Clin. Nutr. Metab. Care 2019, 22, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Zazpe, I.; Sanchez-Tainta, A.; Estruch, R.; Lamuela-Raventos, R.M.; Schroder, H.; Salas-Salvado, J.; Corella, D.; Fiol, M.; Gomez-Gracia, E.; Aros, F.; et al. A large randomized individual and group intervention conducted by registered dietitians increased adherence to Mediterranean-type diets: The PREDIMED study. J. Am. Diet. Assoc. 2008, 108, 1134–1144. [Google Scholar] [CrossRef]
- Hoerster, K.D.; Lehavot, K.; Simpson, T.; McFall, M.; Reiber, G.; Nelson, K.M. Health and health behavior differences: U.S. Military, veteran, and civilian men. Am. J. Prev. Med. 2012, 43, 483–489. [Google Scholar] [CrossRef]
- Campbell, S.B.; Gray, K.E.; Hoerster, K.D.; Fortney, J.C.; Simpson, T.L. Differences in functional and structural social support among female and male veterans and civilians. Soc. Psychiatry Psychiatr. Epidemiol. 2020, 56, 375–386. [Google Scholar] [CrossRef]
- Gallant, M.P. The influence of social support on chronic illness self-management: A review and directions for research. Health Educ. Behav. 2003, 30, 170–195. [Google Scholar] [CrossRef]
- Wang, H.X.; Mittleman, M.A.; Orth-Gomer, K. Influence of social support on progression of coronary artery disease in women. Soc. Sci. Med. 2005, 60, 599–607. [Google Scholar] [CrossRef]
- Leavy, R.L. Social support and psychological disorder: A review. J. Community Psychol. 1983, 11, 3–21. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.M.; Sanders, S.; Carter, M.; Honeyman, D.; Cleo, G.; Auld, Y.; Booth, D.; Condron, P.; Dalais, C.; Bateup, S.; et al. Improving the translation of search strategies using the Polyglot Search Translator: A randomized controlled trial. J. Med. Libr. Assoc. 2020, 108, 195–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The EndNote Team. EndNote; Clarivate: Philadelphia, PA, USA, 2013. [Google Scholar]
- Covidence Systematic Review Software; Veritas Health Innovation: Melbourne, Australia. Available online: www.covidence.org (accessed on 23 February 2021).
- Academy of Nutrition and Dietetics (Ed.) Evidence Analysis Manual: Steps in the Academy Evidence Analysis Process; Academy of Nutrition and Dietetics: Chicago, IL, USA, 2012; pp. 90–92. [Google Scholar]
- Bayer-Carter, J.L.; Green, P.S.; Montine, T.J.; VanFossen, B.; Baker, L.D.; Watson, G.S.; Bonner, L.M.; Callaghan, M.; Leverenz, J.B.; Walter, B.K.; et al. Diet intervention and cerebrospinal fluid biomarkers in amnestic mild cognitive impairment. Arch. Neurol. 2011, 68, 743–752. [Google Scholar] [CrossRef] [Green Version]
- Boutelle, K.N.; Dubbert, P.; Vander Weg, M. A pilot study evaluating a minimal contact telephone and mail weight management intervention for primary care patients. Eat. Weight Disord. 2005, 10, e1–e5. [Google Scholar] [CrossRef]
- Conley, M.; Le Fevre, L.; Haywood, C.; Proietto, J. Is two days of intermittent energy restriction per week a feasible weight loss approach in obese males? A randomised pilot study. Nutr. Diet. 2018, 75, 65–72. [Google Scholar] [CrossRef]
- Friedberg, J.P.; Rodriguez, M.A.; Watsula, M.E.; Lin, I.; Wylie-Rosett, J.; Allegrante, J.P.; Lipsitz, S.R.; Natarajan, S. Effectiveness of a tailored behavioral intervention to improve hypertension control: Primary outcomes of a randomized controlled trial. Hypertension 2015, 65, 440–446. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, N.; Vetter, M.L.; Moore, R.H.; Chittams, J.L.; Dalton-Bakes, C.V.; Dowd, M.; Williams-Smith, C.; Cardillo, S.; Wadden, T.A. Effects of a low-intensity intervention that prescribed a low-carbohydrate vs. a low-fat diet in obese, diabetic participants. Obesity 2010, 18, 1733–1738. [Google Scholar] [CrossRef]
- Shahnazari, M.; Ceresa, C.; Foley, S.; Fong, A.; Zidaru, E.; Moody, S. Nutrition-focused wellness coaching promotes a reduction in body weight in overweight US veterans. J. Acad. Nutr. Diet. 2013, 113, 928–935. [Google Scholar] [CrossRef]
- Stern, L.; Iqbal, N.; Seshadri, P.; Chicano, K.L.; Daily, D.A.; McGrory, J.; Williams, M.; Gracely, E.J.; Samaha, F.F. The effects of low-carbohydrate versus conventional weight loss diets in severely obese adults: One-year follow-up of a randomized trial. Ann. Intern. Med. 2004, 140, 778–785. [Google Scholar] [CrossRef] [Green Version]
- Wu, M.K.; Wang, C.K.; Bai, Y.M.; Huang, C.Y.; Lee, S.D. Outcomes of obese, clozapine-treated inpatients with schizophrenia placed on a six-month diet and physical activity program. Psychiatr. Serv. 2007, 58, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Yancy, W.S., Jr.; Westman, E.C.; McDuffie, J.R.; Grambow, S.C.; Jeffreys, A.S.; Bolton, J.; Chalecki, A.; Oddone, E.Z. A randomized trial of a low-carbohydrate diet vs orlistat plus a low-fat diet for weight loss. Arch. Intern. Med. 2010, 170, 136–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dexter, A.S.; Pope, J.F.; Erickson, D.; Fontenot, C.; Ollendike, E.; Walker, E. Cooking Education Improves Cooking Confidence and Dietary Habits in Veterans. Diabetes Educ. 2019, 45, 442–449. [Google Scholar] [CrossRef] [PubMed]
- North, S.L.; Palmer, G.A. Outcome analysis of hemoglobin A1c, weight, and blood pressure in a VA diabetes education program. J. Nutr. Educ. Behav. 2015, 47, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Sikand, G.; Kashyap, M.L.; Yang, I. Medical nutrition therapy lowers serum cholesterol and saves medication costs in men with hypercholesterolemia. J. Am. Diet. Assoc. 1998, 98, 889–894. [Google Scholar] [CrossRef]
- Niv, N.; Cohen, A.N.; Hamilton, A.; Reist, C.; Young, A.S. Implementation and Effectiveness of a Psychosocial Weight Management Program for Individuals with Schizophrenia. J. Behav. Health Serv. Res. 2014, 41, 370–380. [Google Scholar] [CrossRef] [Green Version]
- Serra, M.C.; Addison, O.; Giffuni, J.; Barton-Ort, K.; Parker, E.; Katzel, L. Changes in Self-Reported Fruit and Vegetable Intake following Nutritional Modification in High Risk Older Veterans. J. Nutr. Gerontol. Geriatr. 2021, 40, 1–8. [Google Scholar] [CrossRef]
- Tan-Shalaby, J.L.; Carrick, J.; Edinger, K.; Genovese, D.; Liman, A.D.; Passero, V.A.; Shah, R.B. Modified Atkins diet in advanced malignancies—Final results of a safety and feasibility trial within the Veterans Affairs Pittsburgh Healthcare System. Nutr. Metab. 2016, 13, 52. [Google Scholar] [CrossRef] [Green Version]
- Holton, K.F.; Kirkland, A.E.; Baron, M.; Ramachandra, S.S.; Langan, M.T.; Brandley, E.T.; Baraniuk, J.N. The Low Glutamate Diet Effectively Improves Pain and Other Symptoms of Gulf War Illness. Nutrients 2020, 12, 2593. [Google Scholar] [CrossRef]
- Yancy, W.S., Jr.; McVay, M.A.; Voils, C.I. Effect of allowing choice of diet on weight loss—In response. Ann. Intern. Med. 2015, 163, 805–806. [Google Scholar] [CrossRef]
- Yancy, W.S., Jr.; Mayer, S.B.; Coffman, C.J.; Smith, V.A.; Kolotkin, R.L.; Geiselman, P.J.; McVay, M.A.; Oddone, E.Z.; Voils, C.I. Effect of Allowing Choice of Diet on Weight Loss: A Randomized Trial. Ann. Intern. Med. 2015, 162, 805–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahn, J.R.; Fitzpatrick, S.L.; Llabre, M.M.; Apterbach, G.S.; Helms, R.L.; Cugnetto, M.L.; Klaus, J.; Florez, H.; Lawler, T. Weight management for veterans: Examining change in weight before and after MOVE! Obesity 2011, 19, 977–981. [Google Scholar] [CrossRef]
- Romanova, M.; Liang, L.J.; Deng, M.L.; Li, Z.; Heber, D. Effectiveness of the MOVE! Multidisciplinary weight loss program for veterans in Los Angeles. Prev. Chronic. Dis. 2013, 10, E112. [Google Scholar] [CrossRef] [PubMed]
- Hoerster, K.D.; Lai, Z.; Goodrich, D.E.; Damschroder, L.J.; Littman, A.J.; Klingaman, E.A.; Nelson, K.M.; Kilbourne, A.M. Weight loss after participation in a national VA weight management program among veterans with or without PTSD. Psychiatr. Serv. 2014, 65, 1385–1388. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, R.W.; Reeves, G.; Tapscott, S.; Medoff, D.; Dickerson, F.; Goldberg, A.P.; Ryan, A.S.; Fang, L.J.; Dixon, L.B. “MOVE!” Outcomes of a weight loss program modified for veterans with serious mental illness. Psychiatr. Serv. 2013, 64, 737–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, A.S.; Cohen, A.N.; Goldberg, R.; Hellemann, G.; Kreyenbuhl, J.; Niv, N.; Nowlin-Finch, N.; Oberman, R.; Whelan, F. Improving Weight in People with Serious Mental Illness: The Effectiveness of Computerized Services with Peer Coaches. J. Gen. Intern. Med. 2017, 32 (Suppl. 1), 48–55. [Google Scholar] [CrossRef] [Green Version]
- Shiroma, P.R.; Velasquez, T.; Usset, T.J.; Wilhelm, J.H.; Thuras, P.; Baltutis, E. Antidepressant Effect of the VA Weight Management Program (MOVE) among Veterans with Severe Obesity. Mil. Med. 2020, 185, e586–e591. [Google Scholar] [CrossRef] [Green Version]
- Ahrendt, A.D.; Kattelmann, K.K.; Rector, T.S.; Maddox, D.A. The effectiveness of telemedicine for weight management in the MOVE! Program. J. Rural Health 2014, 30, 113–119. [Google Scholar] [CrossRef]
- Rutledge, T.; Skoyen, J.A.; Wiese, J.A.; Ober, K.M.; Woods, G.N. A comparison of MOVE! versus TeleMOVE programs for weight loss in Veterans with obesity. Obes. Res. Clin. Pract. 2017, 11, 344–351. [Google Scholar] [CrossRef]
- Skoyen, J.A.; Rutledge, T.; Wiese, J.A.; Woods, G.N. Evaluation of TeleMOVE: A Telehealth Weight Reduction Intervention for Veterans with Obesity. Ann. Behav. Med. 2015, 49, 628–633. [Google Scholar] [CrossRef]
- Spring, B.; Duncan, J.M.; Janke, E.A.; Kozak, A.T.; McFadden, H.G.; DeMott, A.; Pictor, A.; Epstein, L.H.; Siddique, J.; Pellegrini, C.A.; et al. Integrating technology into standard weight loss treatment: A randomized controlled trial. JAMA Intern. Med. 2013, 173, 105–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desouza, C.V.; Padala, P.R.; Haynatzki, G.; Anzures, P.; Demasi, C.; Shivaswamy, V. Role of apathy in the effectiveness of weight management programmes. Diabetes Obes. Metab. 2012, 14, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Frankwich, K.A.; Egnatios, J.; Kenyon, M.L.; Rutledge, T.R.; Liao, P.S.; Gupta, S.; Herbst, K.L.; Zarrinpar, A. Differences in Weight Loss between Persons on Standard Balanced vs Nutrigenetic Diets in a Randomized Controlled Trial. Clin. Gastroenterol. Hepatol. 2015, 13, 1625–1632.e1. [Google Scholar] [CrossRef] [Green Version]
- Allicock, M.; Ko, L.; van der Sterren, E.; Valle, C.G.; Campbell, M.K.; Carr, C. Pilot weight control intervention among US veterans to promote diets high in fruits and vegetables. Prev. Med. 2010, 51, 279–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damschroder, L.J.; Lutes, L.D.; Kirsh, S.; Kim, H.M.; Gillon, L.; Holleman, R.G.; Goodrich, D.E.; Lowery, J.C.; Richardson, C.R. Small-changes obesity treatment among veterans: 12-month outcomes. Am. J. Prev. Med. 2014, 47, 541–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lutes, L.D.; Damschroder, L.J.; Masheb, R.; Kim, H.M.; Gillon, L.; Holleman, R.G.; Goodrich, D.E.; Lowery, J.C.; Janney, C.; Kirsh, S.; et al. Behavioral Treatment for Veterans with Obesity: 24-Month Weight Outcomes from the ASPIRE-VA Small Changes Randomized Trial. J. Gen. Intern. Med. 2017, 32 (Suppl. 1), 40–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moin, T.; Damschroder, L.J.; AuYoung, M.; Maciejewski, M.L.; Datta, S.K.; Weinreb, J.E.; Steinle, N.I.; Billington, C.; Hughes, M.; Makki, F.; et al. Diabetes Prevention Program Translation in the Veterans Health Administration. Am. J. Prev. Med. 2017, 53, 70–77. [Google Scholar] [CrossRef]
- Jackson, S.L.; Safo, S.; Staimez, L.R.; Long, Q.; Rhee, M.K.; Cunningham, S.A.; Olson, D.E.; Tomolo, A.M.; Ramakrishnan, U.; Narayan, K.M.V.; et al. Reduced Cardiovascular Disease Incidence with a National Lifestyle Change Program. Am. J. Prev. Med. 2017, 52, 459–468. [Google Scholar] [CrossRef] [Green Version]
- Das, S.R.; Kinsinger, L.S.; Yancy, W.S., Jr.; Wang, A.; Ciesco, E.; Burdick, M.; Yevich, S.J. Obesity prevalence among veterans at Veterans Affairs medical facilities. Am. J. Prev. Med. 2005, 28, 291–294. [Google Scholar] [CrossRef]
- Bray, G.A. Medical consequences of obesity. J. Clin. Endocrinol. Metab. 2004, 89, 2583–2589. [Google Scholar] [CrossRef] [Green Version]
- Dworkin, E.R.; Bergman, H.E.; Walton, T.O.; Walker, D.D.; Kaysen, D.L. Co-Occurring Post-Traumatic Stress Disorder and Alcohol Use Disorder in U.S. Military and Veteran Populations. Alcohol. Res. 2018, 39, 161–169. [Google Scholar] [PubMed]
- Hoerster, K.D.; Campbell, S.; Dolan, M.; Stappenbeck, C.A.; Yard, S.; Simpson, T.; Nelson, K.M. PTSD is associated with poor health behavior and greater Body Mass Index through depression, increasing cardiovascular disease and diabetes risk among U.S. veterans. Prev. Med. Rep. 2019, 15, 100930. [Google Scholar] [CrossRef] [PubMed]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D. Dietary and Policy Priorities for Cardiovascular Disease, Diabetes, and Obesity: A Comprehensive Review. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef]
- National Heart Foundation of Australia. Dietary Position Statement. Heart Healthy Eating Patterns. Melbourne: National Heart Foundation of Australia. 2019. Available online: https://www.heartfoundation.org.au/health-professional-tools/nutrition-position-statements (accessed on 9 February 2022).
- U.S. Department of Agriculture and U.S. Department of Health and Human Services Dietary Guidelines for Americans, 2020–2025. Updated December. 9th ed. Available online: DietaryGuidelines.gov (accessed on 9 February 2022).
- Rippe, J.M.; Crossley, S.; Ringer, R. Obesity as a chronic disease: Modern medical and lifestyle management. J. Am. Diet. Assoc. 1998, 98, S9–S15. [Google Scholar] [CrossRef]
- Prochaska, J.O.; DiClemente, C.C. Stages and processes of self-change of smoking: Toward an integrative model of change. J. Consult. Clin. Psychol. 1983, 51, 390–395. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Velicer, W.F. The transtheoretical model of health behavior change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef]
- Allison, D.B.; Newcomer, J.W.; Dunn, A.L.; Blumenthal, J.A.; Fabricatore, A.N.; Daumit, G.L.; Cope, M.B.; Riley, W.T.; Vreeland, B.; Hibbeln, J.R.; et al. Obesity among those with mental disorders: A National Institute of Mental Health meeting report. Am. J. Prev. Med. 2009, 36, 341–350. [Google Scholar] [CrossRef]
- Cabassa, L.J.; Ezell, J.M.; Lewis-Fernandez, R. Lifestyle interventions for adults with serious mental illness: A systematic literature review. Psychiatr. Serv. 2010, 61, 774–782. [Google Scholar] [CrossRef]
- Murimi, M.W.; Kanyi, M.; Mupfudze, T.; Amin, M.R.; Mbogori, T.; Aldubayan, K. Factors Influencing Efficacy of Nutrition Education Interventions: A Systematic Review. J. Nutr. Educ. Behav. 2017, 49, 142–165.e1. [Google Scholar] [CrossRef]
- Douketis, J.D.; Macie, C.; Thabane, L.; Williamson, D.F. Systematic review of long-term weight loss studies in obese adults: Clinical significance and applicability to clinical practice. Int. J. Obes. 2005, 29, 1153–1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamman, R.F.; Wing, R.R.; Edelstein, S.L.; Lachin, J.M.; Bray, G.A.; Delahanty, L.; Hoskin, M.; Kriska, A.M.; Mayer-Davis, E.J.; Pi-Sunyer, X.; et al. Effect of weight loss with lifestyle intervention on risk of diabetes. Diabetes Care 2006, 29, 2102–2107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wing, R.R.; Lang, W.; Wadden, T.A.; Safford, M.; Knowler, W.C.; Bertoni, A.G.; Hill, J.O.; Brancati, F.L.; Peters, A.; Wagenknecht, L.; et al. Benefits of modest weight loss in improving cardiovascular risk factors in overweight and obese individuals with type 2 diabetes. Diabetes Care 2011, 34, 1481–1486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarris, J.; Logan, A.C.; Akbaraly, T.N.; Amminger, G.P.; Balanza-Martinez, V.; Freeman, M.P.; Hibbeln, J.; Matsuoka, Y.; Mischoulon, D.; Mizoue, T.; et al. Nutritional medicine as mainstream in psychiatry. Lancet Psychiatry 2015, 2, 271–274. [Google Scholar] [CrossRef]
- Jacka, F.N.; O’Neil, A.; Opie, R.; Itsiopoulos, C.; Cotton, S.; Mohebbi, M.; Castle, D.; Dash, S.; Mihalopoulos, C.; Chatterton, M.L.; et al. A randomised controlled trial of dietary improvement for adults with major depression (the ‘SMILES’ trial). BMC Med. 2017, 15, 23. [Google Scholar] [CrossRef] [Green Version]
- Henriquez Sanchez, P.; Ruano, C.; de Irala, J.; Ruiz-Canela, M.; Martinez-Gonzalez, M.A.; Sanchez-Villegas, A. Adherence to the Mediterranean diet and quality of life in the SUN Project. Eur. J. Clin. Nutr. 2012, 66, 360–368. [Google Scholar] [CrossRef]
- Tessier, J.M.; Erickson, Z.D.; Meyer, H.B.; Baker, M.R.; Gelberg, H.A.; Arnold, I.Y.; Kwan, C.; Chamberlin, V.; Rosen, J.A.; Shah, C.; et al. Therapeutic Lifestyle Changes: Impact on Weight, Quality of Life, and Psychiatric Symptoms in Veterans with Mental Illness. Mil. Med. 2017, 182, e1738–e1744. [Google Scholar] [CrossRef] [Green Version]
- Peinemann, F.; Tushabe, D.A.; Kleijnen, J. Using multiple types of studies in systematic reviews of health care interventions—A systematic review. PLoS ONE 2013, 8, e85035. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Criteria | Inclusion | Exclusion |
|---|---|---|
| P (Participants or population) |
|
|
| I (Intervention) |
|
|
| C (Control or Comparator) |
| |
| O (Outcomes) |
|
|
| S (Study design) |
|
|
| Bayer-Carter, 2011 | Boutelle, 2005 | Conley, 2018 | Dexter, 2019 | Friedberg, 2015 | Holton, 2020 | Iqbal, 2010 | Niv, 2014 | North, 2015 | Serra, 2021 | Shahnazari, 2013 | Shiroma, 2020 | Sikand, 1998 | Stern, 2004 | Tan-Shalaby, 2016 | Wu, 2007 | Yancy Jr, 2010 | Yancy Jr, 2015 | MOVE! | Ahrendt, 2014 | Allicock, 2010 | Dahn, 2011 | Damschroder, 2010 | Damschroder, 2014 | Desouza, 2012 | Frankwich, 2015 | Goldberg, 2013 | Hoerster, 2014 | Jackson, 2017 | Lutes, 2017 | Moin, 2017 | Romanova, 2013 | Rutledge, 2017 | Skoyen, 2015 | Spring, 2013 | Young, 2017 | |
| Overall Quality Rating | + | + | + | + | + | □ | + | □ | □ | □ | + | + | □ | + | + | □ | + | + | + | □ | □ | + | + | □ | □ | + | + | □ | + | + | + | + | + | + | □ | |
| Relevance Questionsa | ||||||||||||||||||||||||||||||||||||
| All studies received a Yes rating for all Relevance questions. | ||||||||||||||||||||||||||||||||||||
| Validity Questions | ||||||||||||||||||||||||||||||||||||
| 1. Was the research question clearly stated? | ||||||||||||||||||||||||||||||||||||
| 2. Was selection of study subjects free from bias? | ||||||||||||||||||||||||||||||||||||
| 3. Were study groups comparable? | ||||||||||||||||||||||||||||||||||||
| 4. Was method of handling withdrawals described? | ||||||||||||||||||||||||||||||||||||
| 5. Was blinding used to prevent introduction of bias? | ||||||||||||||||||||||||||||||||||||
| 6. Were interventions and any comparison(s) described in detail? | ||||||||||||||||||||||||||||||||||||
| 7. Were outcomes clearly defined and measurements valid and reliable? | ||||||||||||||||||||||||||||||||||||
| 8. Was the statistical analysis appropriate for the study design and type of outcome indicators? | ||||||||||||||||||||||||||||||||||||
| 9. Are conclusions supported by results with biases and limitations taken into consideration? | ||||||||||||||||||||||||||||||||||||
| 10. Is bias due to study’s funding or sponsorship unlikely? | ||||||||||||||||||||||||||||||||||||
| Study, Location and Design | Health Condition | Sample Characteristics a,b | Inclusion Criteria | Intervention c | Control/Comparison c | Intervention Mode | Intervention Description | Intervention Duration and Contact | Attendance/Attrition or Adherence |
|---|---|---|---|---|---|---|---|---|---|
| Stern et al. (2004), USA Randomised trial | Obesity | n = 132 (83% male) Age (y): LC = 53 (9); CD = 54 (9) BMI: LC = 42.9 (6.6); CD = 42.9 (7.7) Weight (kg): LC = 130 (23); CD = 132 (27) | BMI ≥ 35 kg/m2 | Low-carbohydrate diet [LC], n = 64 | Conventional (low-fat/low-calorie) diet [CD], n = 68 | In-person group | Counselling to restrict carbohydrates or calories. LC: ↓ carbohydrate intake to <30 g/day; CD: ↓ caloric intake by 500 calories/day, with <30% calories from fat. | 12 months. Weekly counselling sessions (2-h) for 4 weeks, then monthly sessions (1-h) for 11 months. | 6-month follow-up: n = 79; 1-year: n = 87. 6-month weight data carried forward or obtained from medical records = (89%). 1-year weights obtained from medical records = (final 96%) |
| Boutelle et al. (2005), USA Randomised controlled feasibility trial | Overweight or obese | n = 26 (80% male) Age (y): 53.8 (10.4) BMI: 34.7(4.9) Weight (kg): 111.7 (21.3) | ≥20% above ideal body weight | Educational mailings re weight management d | Usual care d | Weekly individual mailings and phone calls | Both conditions: At initial visit, weight management discussed. IG: weekly educational mailings weeks 2–7 to address weight management issues (self-monitoring, stimulus management, relapse prevention, ↓ fat content, meal planning, exercise). | 8 weeks. | Attendance at 8-week follow-up, IG: 87%; UC: 54.5% (p = 0.095). |
| Yancy Jr et al. (2010), USA Randomised controlled trial | Overweight or obese | n = 146 (72% male) Age (y) (SD): LCKD = 52.9 (10.2) OLFD = 52 (9) BMI (SD): LCKD= 39.9 (6.0) OLFD = 38.8 (7) Weight (kg): LCKD = 123.1 (25.4) OLFD = 117.4 (26.0) WC (cm): LCKD = 127.4 (16.9), OLFD = 124.8 (17.4) | BMI between 27 and 30 kg/m2 and an obesity-related disease; OR, a BMI of ≥30 kg/m2 regardless of comorbidity | Low-carbohydrate, ketogenic diet (LCKD), n = 81 allocated (n = 72 received) | Orlistat therapy combined with low-fat diet (OLFD), n = 79 (n = 74 received) | In-person group | Counselling sessions covered topics parallel between the 2 interventions but specific to diet. Advice re exercise, hydration, ↓ of caffeine/alcohol. Restrict carbohydrate intake to <20 g/day. | 48 weeks. Meetings every 2 weeks for 24 weeks, then every 4 weeks for 24 weeks. (meeting duration = 1 to 2 h) | Post-intervention numbers, LCKD: n = 52; OLFD: n = 61. Completion of measurements at 48 weeks: 57 of LCKD group (79%) and 65 of OLFD group (88%). Attendance at ≥80% of group counselling sessions: LCKD n = 26; OLFD n = 27. |
| Shahnazari et al. (2013), USA Randomised controlled trial | Overweight or obese | n= 50 (84% male) Age (y) [M (95%CI)]: CG = 55 (51, 59), IG = 54 (49, 59) BMI [M (95%CI)]: CG = 30 (28, 32), IG = 31 (29, 33) Weight (kg) [M (95%CI)]: CG = 89 (81, 97), IG = 93 (87, 99) | Veterans responsible for own food selection, preparation, consumption | Individualised wellness coaching, n = 43 | Initial 1-h nutrition education session only, n = 41 | In-person individual or via telephone | Nutrition coaching sessions (healthy eating habits, food choices, label reading, cooking techniques, stages of change model to alter eating behaviours). Nutrition education material. Sessions focused on ↓ intake of sugar, salt, high fat meat, fast foods, etc. and ↑ fruit/vegetables, whole-grain, dairy, lean meat, fish, water. | 6 months. IG (3.75 h contact): 1× 60 min education session; individualized 15 min wellness coaching weekly in 2nd month; 1× monthly for following 4 months; one final 60 min session. | IG n = 28 (65%), CG n = 22 (54%) (p = 0.284) completed. |
| Yancy et al. (2015), USA Doubly randomised preference trial | Obesity | n = 207 (73% men) Age (y): 55 (11) BMI: 36 (6) Weight (kg): 108 (20) WC (cm): 46 (5) | BMI ≥ 30 kg/m2 | Choice of diet, n = 105, (n = 61 low-carb diet [Choice-LCD]; n = 44 low-fat reduced calorie diet [Choice-LFD]) | No choice, n = 102 (n = 53 CG-LCD; n = 49 CG-LFD) | In-person group and individual telephone | Choice arm: advised if food preferences aligned with LCD or LFD based on food preference questionnaire. CG: Randomised to diet. LCD: carbohydrate intake 20 g/day; calories not restricted. LFD: total fat, saturated fat and cholesterol intake restricted to <30%, <10% and <300 mg/day of daily energy intake; calorie intake restricted by ↓ 500 kcal from daily maintenance energy requirement. | 48 weeks. Weeks 1–24: group sessions every 2 weeks. Weeks 25–48: group sessions every 4 weeks, telephone call from dietitian between sessions. 19 visits in total. | Completed intervention: Choice-LCD n = 47/61, Choice-LFD n = 34/44, CG-LCD n = 45/53, CG-LFD n = 35/49. Completed weight measurements at 48 weeks, Choice: 87 (83%); CG: 88 (86%). Attendance, number of group sessions attended (of 19) and calls completed (of 6) [m (SD)]: Choice = 13.5 (5.5) and 2.5 (2.5), respectively; CG = 14.8 (4.7) and 3.0 (2.5). Attendance-at least 15 group sessions, Choice: 55.2%; CG: 67.6%. Dietary adherence similar between arms (p = 0.66). |
| Conley et al. (2018), Australia Parallel group randomised controlled trial | Obesity | n = 24 (100% male) Age (y): SERD = 67.1 (3.9), IER = 68 (2.7) BMI: SERD = 36.2 (4.3), IER = 33.4 (1.8) Weight (kg): SERD = 107.3 (17.1), IER = 99.1 (7.9) WC (cm): SERD = 122.5 (10.4), IER = 114.2 (5.2) | BMI ≥ 30 kg/m2 | Intermittent Energy Restriction (IER) 5:2 diet plan, n = 11 | Standard Energy Restricted Diet (SERD), n = 12 | In-person individual; telephone (if required) | IER diet: ‘fast’ for 2 non-consecutive days/week (daily calorie intake 600 calories) and eat ad libitum on remaining 5 days. SERD: continuous daily energy-restricted diet (500-calorie daily reduction from average requirement). | 6 months. Five individual counselling sessions at weeks 2, 4, 8 and 3 months. Telephone assistance if required from months 4–6. | Post-intervention at 6 months: n = 23 (n = 1 withdrawal, IER group). Adherence at 3 months: 83% SERD and 82% 5:2 following respective diets. Adherence at 6 months: 75% SERD and 73% IER. |
| Wu et al. (2007), Taiwan Randomised controlled trial | Overweight or obese inpatients with schizophrenia | n = 53 (42% male) Age (y): CRD = 42.4 (7.5), UC = 39.0 (6.7) BMI: CRD = 30.43 (4.2), UC = 30.27 (3.31) Weight (kg): CRD= 78.4 (11.6), UC = 77.8 (112.0) WC (cm): CRD = 98.30 (7.33), UC = 97.82 (9.67) HC (cm): CRD = 108 (8.5), UC = 106.1 (6.5) Waist-to-hip ratio: CRD = 0.91 (0.07), UC = 0.92 (0.07) Body fat %: CRD = 36.9 (7.8), UC= 38 (10.6) | Taking ≥300 mg of oral clozapine per day for at least a year, BMI > 27 kg/m2, DSM-IV diagnosis of schizophrenia. | Calorie-restricted diet (CRD) and physical exercise, n = 28 | Usual care (UC), n = 25 | Inpatient program | Caloric intake restricted to 1300 to 1500 kcal/day for women; 1600 to 1800 kcal/day for men. Macronutrient intake complied with expected changes of 20%, 25% and 55% in energy from protein, fat, carbohydrate. | 6 months. | Post-intervention numbers: n = 53 (n = 3 withdrew from UC, as discharged from hospital in second month of study). |
| Niv et al. (2014), USA Pre-post intervention | Obese with schizophrenia or schizoaffective disorder | n = 109 (90.8% male) Age (y): 50.2 (9.7) BMI: 31.5 (5.4) Weight (kg): 97.84 (19.78) | Schizophrenia or schizoaffective disorder as per Structured Clinical Interview for DSM-IV diagnosis | Enhancing Quality-of-care In Psychosis (EQUIP): psychosocial weight management program, n = 55 | Eligible for EQUIP but chose not to enrol, n = 54 | In-person group; in-person individual as needed | EQUIP Program sessions focused on weight management techniques, light physical exercise. Education on nutritional principles and behavioural techniques to adjust unhealthy eating and exercise habits. Handouts, knowledge quizzes, learning principles adapted for schizophrenia. Nurse care coordinators available as needed. | 16 weeks (weekly sessions). | Post-intervention numbers: n = 50 (five attended only one session, and thus were dropped from the weight and BMI analysis). Attendance, group sessions: 100% (n = 55) attended at least one; average of 3.8 (SD = 4.6) sessions. Individual sessions: 75% (n = 41) attended at least one session; average of 3.9 (SD = 3.0) sessions. In total, average of 6.7 (SD = 5.2) in-person sessions (range 1–23). |
| Iqbal et al. (2010), USA Randomised Controlled Trial | Type II diabetes | n = 144 (90% male) Age (y): 59.4 (9.2) BMI: 37.6 (5.5) | Clinically diagnosed Type II diabetes mellitus BMI ≥ 30 kg/m2 | Low-carb diet (LCD), n = 70; or low-fat diet (LFD), n = 74 | Nil | In-person group | LCD: carbohydrate intake 30 g/day LFD: consume ≤ 30% calories from fat and deficit of 500 kcal/day. To consume <7% total calories from saturated fats; <300 mg of dietary cholesterol daily. | 24 months. Weekly 2-h classes for first month; then every 4 weeks. | Post-intervention: n = 68; Attrition rate: LCD = 60%, LFD = 46% Attendance: mean 9.9 sessions attended. |
| North and Palmer (2015), USA Retrospective chart review | Type II diabetes | n = 359 medical records (100% male) Age (y): Basics = 65.2 (8.87), CG = 66.8 (9.67) | Diagnosis of Type II DM within previous 2 y. | Diabetes group education (Basics), n = 175 | Standard diabetes management follow-up (CG), n = 184 | In-person group sessions | Basics program (3 sessions). Nutrition related topics include: carbohydrate counting, nutrition labels, blood pressure, cholesterol, general healthy eating, weight loss plans. | 4 months. 3 sessions: 2.5, 2, and 1.5 hrs duration. Sessions 1 and 2 held 2 weeks apart, Session 3 held 3 months after session 2. | Attendance: each patient in treatment group completed all three sessions of Basics diabetes education program. |
| Dexter et al. (2019), USA Retrospective chart review | Prediabetes and diabetes | n = 75 (88% male) Age bracket (y) n (%): 41–50: 8 (10.7%) 51–60: 15 (20.0%) 61–70: 46 (61.3%) 71 +: 6 (8.0%) BMI: face-to-face = 36.6 (6.98), telehealth = 36.32 (4.63) | BMI ≥ 25 and either (a) current Dx of Type II DM or (b) Dx of prediabetes | Healthy teaching kitchen (HTK), n = 75 | Nil | In-person group or via Clinical Video Telehealth | Multicomponent intervention. Cooking and nutrition education class topics included carbohydrate counting, meal planning, creating recipes. | 12 weeks. HTK offered once every 12 weeks. | NA |
| Friedberg et al. (2015), USA Randomised controlled trial | Uncontrolled hypertension | n = 533 (99% male) Age (y) [M (SE)]: SMI = 66.4 (0.66), HEI = 66.5 (0.96), UC = 65.4 (0.76) BMI [M(SE)]: SMI = 30.5 (0.38), HEI = 31.2 (0.47), UC = 30.0 (0.34) BP control (%): SMI = 42.6, HEI = 40.6, UC = 44.6 (p = 0.74) SBP (mmHg) [m(SE)]: SMI = 136.0 (0.89), HEI = 137.2 (1.33), UC = 137.0 (0.96) (p = 0.65) | Hypertension, antihypertensive drug therapy for ≥6 months, uncontrolled BP during screening. | Hypertension diet. Stage-matched intervention (SMI), n = 176 | Health Education Intervention (HEI), n = 177; or Usual Care (UC), n = 180 | Individual telephone counselling | SMI: tailored monthly phone counselling for exercise, diet and medications based on current stage of change. HEI: monthly telephone counselling of non-tailored information on HT, diet, medication, exercise guidelines. | 6 months. SMI: monthly phone counselling (approx. 30 min). HEI: monthly telephone counselling (approx. 15 min) | 6 months: n = 481, (6-month missing data rate of <10%). |
| Sikand et al. (1998), USA Retrospective chart review, observational cohort | Primary hypercholesterolaemia | n = 95 (100% male) Age (y): 60.9 (9.9) BMI: 26.9 (0.5) | Primary Dx hypercholesterolemia, previously met NCEP criteria for initiating cholesterol-lowering drug therapy, not on cholesterol-lowering medication, aged 21–75 y. | National Cholesterol Education Program (NCEP) dietary intervention phase of a clinical trial, n = 95 | Nil | In-person individual | Dietitian initiated “medical nutrition therapy” to ↓ elevated cholesterol levels, progressively ↓ saturated fat and cholesterol intake, promote weight loss by eliminating excess total calories. I.e. intake of total fat <30% of calories, saturated fatty acids <10% of calories and cholesterol <300 mg/day. | 8 weeks. 2–4 visits (120–180 min). | Post-intervention: n = 74 (78% complete data). Attendance: mean no. of dietitian visits = 2.8 (0.7) (range = two to four visits); mean total time = 144 (21) minutes over 6.8 (0.7) weeks. Two visits (n = 29); three visits (n = 33); and four visits (n = 12). |
| Tan-Shalaby et al. (2016), USA Observational safety and feasibility trial (pre-post) | Advanced malignant cancers | n = 17 (100% male) Age (y): 65 (11.7) BMI: 29.46 (5) Weight (kg): 92 (2.3) | Advanced solid malignancies measurable on FDG PET/CT imaging; not on chemotherapy. | Modified Atkins Diet (Ketogenic diet) n = 17 | Nil | In-person individual | 20 to 40 g of carbohydrates/day, advised on grocery shopping, menu planning. Restricted consumption of high carbohydrate foods. No restriction on calories, protein, fats. | 16 weeks. | Screen failures in 6/17 (35%). Adherence: 11/17 proceeded with trial. 6 (35%) maintained diet for 8 weeks, 4 (23%) completed 16 wks. Three successfully dieted >16 wks. One died at 80 weeks and one at 116 weeks. One alive without evidence of disease at 131 wks. |
| Holton et al. (2020), USA Cohort study | Gulf War Illness (GWI) | n = 46 (72.5% male) Age (y): 54.35 (6.02) BMI: 32.10 (5.34) | Active deployment during Gulf War; symptoms meeting Kansas criteria and CDC criteria for GWI. | Low Glutamate Diet, n = 20 | Wait-listed control group (started diet 1 month later), n = 20 | Individual via Skype | Whole food diet, restricting free glutamate and aspartate. Provision of materials including list of foods to avoid, food additives to avoid, high antioxidant food list, shopping list, sample recipes. | 1 month. | Post-treatment: n = 40; Adherence: n = 34 at 3 months post-completion, reported 30/34 (88%) were still following the diet at this time point. |
| Bayer-Carter et al. (2011), USA Randomised controlled trial | Amnestic mild cognitive impairment (aMCI) vs. healthy controls (HC) | n = 49 (47% male) Age (y): HC = 69.3 (7.4), aMCI = 67.6 (6.8) BMI [M (SEM)]: HC (LOW) = 26.4 (2.6), HC (HIGH)= 29.5 (4.5), aMCI (LOW) = 27.4 (3.8), aMCI (HIGH) = 27.5 (3.4) | aMCI diagnosed as delayed memory scores deviating ≥1.5 SD from estimated premorbid ability | LOW Diet (low-saturated fat/low glycaemic index diet), n = 25 | HIGH diet (high-saturated fat/high-glycaemic index), n = 24 | Food delivered to participants’ homes twice weekly | The HIGH diet (fat, 45% [saturated fat, >25%]; carbohydrates, 35%–40% [glycaemic index, >70]; and protein, 15%–20%). LOW diet (fat, 25%; [saturated fat, <7%]; carbohydrates, 55%–60% [glycaemic index, <5]; and protein, 15%–20%). | 4 weeks. | Diet adherence: Mean non-adherent incidents per week ranged from 1.23 to 1.80 per group. |
| Serra et al. (2021), USA Single group prospective feasibility trial | Medically stable nursing home residents | n = 50 (92% Male) Age (y) (M ± SEM): 69.7 ± 0.7 BMI (M ± SEM): 31.7 ± 0.9 | Medically stable > 64 y; enrolled in Gerofit clinical demonstration program. | Nutrition education | Nil | In-person group and optional individual counselling | Registered Dietitian (RD) led classes addressing age-related nutrition concerns: nutrition basics, food labels, hydration, meal planning, the DASH diet, protein intake, food shopping on budget. Individualized nutrition counselling sessions available. | 7 months. Class duration: 30 min. | Attended ≥ 1 group class = 39 (78%) Attended ≥ 2 group classes = 24 (62%) (M ± SEM: 2.9 ± 2.0 classes, which was 82% of total available sessions). |
| Study | Dietary Intervention | Health-Related Outcome Measures | Within Group Comparisons a,b | Between Group Comparisons a,b |
|---|---|---|---|---|
| Stern et al., (2004) | Low-carbohydrate diet | Weight; blood lipids (TC, LDL-C, HDL-C, triglycerides); HbA1c; SBP and DBP; insulin level; glucose level | At 1 year Mean change (SD); Mean difference (95% CI) Weight (kg): LCD = −5.1 (8.7), CD = −3.1 (8.4); −2.0 (−4.9, 1.0) (p = 0.195) TC: LCD = 0.16 (1.11), CD = −0.21 (0.91) (p = 0.143) LDL-C: LCD = 0.18 (0.91), CD = −0.10 (0.75) (p = 0.191) HDL-C (mmol/L): LCD = −0.03 (0.18), CD = −0.13 (0.16); 0.08 (0.01, 0.16) (p = 0.028) Triglycerides (mmol/L): LC = −0.65 (1.78), CD = 0.05 (0.96); −0.62 (−1.09, −0.15) (p = 0.044) HbA1C (participants with diabetes, n = 54), %: LCD = −0.7 (1.0), CD = −0.1 (1.6); −0.7 (−1.6, 0.2) (p = 0.102) SBP (mmHg): LC = 1 (19), CD = 2 (15) (p = 0.78) DBP (mmHg): LC = 3 (15), CD = 1 (10) (p = 0.502) Insulin level (participants with diabetes): LC = −35 (236), CD = −28 (139) (p = 0.917) Glucose level (participants with diabetes) mm/L: LC = −1.55 (2.16), CD:−1.17 (3.66) (p = 0.800) | |
| Boutelle et al., (2005) | Educational mailings | Weight; Food habits (FHQ); Health status (MOS SF-36); readiness to change (URICA) | At 8 weeks: Weight (lbs): IG = −3.91 (6.15); CG = −1.62 (3.33), p = 0.138 Weight loss (% participants): IG = 67%, CG = 36% (p = 0.129) FHQ (Fruit and vegetable consumption subscale): Group X Time interaction p = 0.019; IG mean change (SD) = −0.56 (0.58), p = 0.004 (↑consumption). CG = 0.22 (0.69), p = 0.47 (↓consumption). FHQ, other subscales: ns URICA: All subscales ns | |
| Yancy Jr et al., (2010) | Low-carbohydrate, ketogenic diet (LCKD) | Weight; WC; BP; blood lipids (TC, triglycerides, LDL-C, HDL-C); metabolic indices (fasting glucose level, fasting insulin level, HbA1c) | At 48 weeks: Mean change (95%CI) Weight: LCKD = −11.4 kg (−14.8, −7.9), % loss: −9.5% (−12.1, −6.9); OLFD = −9.6 kg (−11.9, −7.3), % loss: −8.5% (−11.0, −6.1); WC: LCKD = −11.07 cm (−13.85, −8.29); OLFD = −11.07 cm (−13.85 to −8.29); SBP: LCKD = −5.94 (−8.80, −3.08); OLFD = ns DBP: LCKD = −4.53 (−6.57, −2.49); OLFD = ns TC: LCKD = ns; OLFD = −8.86 mg/dL (−15.31 to −2.41) Triglycerides: LCKD = −28.83 mg/dL (−48.08, −9.58); OLFD = −21.40 mg/dL (−39.63, −3.17) LDL-C: LCKD = ns; OLFD = −8.29 (−14.06, −2.52) HDL-C: LCKD = ns; OLFD= 3.42 (1.61, 5.25) TC/HDL-C: LCKD = −0.44 (−0.68, −0.20); OLFD = −0.51 (−0.73, −0.28) Triglyceride/HDL-C: LCKD = −1.00 (−1.65, −0.35); OLFD = −0.77 (−1.38, −0.15) Fasting glucose level: LCKD = −9.7 mg/dL (−16.9, −2.6); OLFD = −3.26 mg/dL (−10.05, −3.54) Fasting insulin level (participants without diabetes only): LCKD = −7.3 IU/mL (−13.5, −1.2); OLFD = ns HbA1c: LCKD = −0.3% (−0.5, −0.1); OLFD = ns | At 48 weeks: Mean difference (95% CI) LCKD and OLFD Weight (%): −0.95 (−4.50, 2.61) (p = 0.60) Weight (kg): −1.75 (−5.90, 2.40) (p = 0.41) WC (cm): ns SBP (mm Hg): −7.44 (−11.12, −3.75) (p = 0.001) DBP (mm Hg): −4.97 (−7.64, −2.29) (p = 0.001) Blood lipids and metabolic indices: ns |
| Shahnazari et al., (2013) | Individualised wellness coaching | Weight; BMI; Block 2005 Food Questionnaire; readiness to improve eating behaviour (SOCMII) | Pre (baseline) vs. post (6 months):d Weight (kg): IG = 92.8 (4.1) vs. 88.2 (3.4) (p = 0.006), CG = 88.7 (5.4) vs. 87.4 (4.6) (p = 0.33) BMI e: IG = 30.4 vs. 28.9 (p = 0.02), CG = 29.6 vs. 29.1 (p = 0.37) Nutrients and Intakes: Refer to paper for full details *. SOCMII: IG = 0.32 (0.09) vs. 0.8 (0.15) (p = 0.006); CG = ns | |
| Yancy et al., (2015) | Choice of diet: low-carbohydrate diet, or low-fat reduced calorie diet (Choice) | Weight; WC; dietary adherence (FFQ); QoL (IWQOL-Lite) | At 48 weeks: Weight (kg) [M(95% CI)]: Choice = −5.7 (4.3, 7.0); CG = −6.7 (5.4, 8.0) | At 48 weeks: Estimated mean difference, Choice-CG [95% CI] Weight (kg): 1.1 (−2.9, 0.8); p = 0.26 WC (cm): 0.4 (−0.3, 1.3); p = 0.28 Dietary adherence (FFQ): −0.9 [−4.9,3.1] p = 0.66 IWQOL-Lite: −0.8 (−4.1, 2.6) p = 0.65 |
| Conley et al., (2018) | Intermittent Energy Restriction (IER) diet plan (The 5:2 Diet) | Weight; BMI; WC; BP; FBG; blood lipids (TC, LDL-C, HDL-C, triglycerides); FFQ (energy, protein, fat, CHO, sugars, fibre, calcium, alcohol, sodium); QoL (AQoL-8D) | At 6 months: Weight (kg): IER = −5.3 (3.0) (p < 0.001), SERD = −5.5 (4.3) (p < 0.001) BMI: ↓ in both groups approx. −2.2 (p < 0.001). SERD = 34.4 (5.3), IER = 31.5 (2.2) WC (cm): SERD = -−6.4 (10) (p < 0.001), IER = −8 (10) (p < 0.001) SBP (mmHg): SERD = −10.2, IER = −14 (p < 0.001) DBP (mmHg): p = 0.2 FBG: p = 0.15 TC: p = 0.52 LDL-C: p = 0.6 HDL-C: p = 0.68 Triglycerides: p = 0.22 QoL c: Both groups improved psycho-social dimension score, (p = 0.001); physical dimension score (p = 0.03); and overall AQol-8D score (p = 0.003) FFQ: Significant ↓ in all nutrient intakes (except alcohol, ns) in both groups | At 6 months c: Weight (kg):p = 0.79 BMI: p = 0.85 WC (cm): p = 0.54 SBP (mmHg): p = 0.76 DBP (mmHg): p = 0.83 FBG: p = 0.81 TC: p = 0.69 LDL-C: p = 0.86 HDL-C: p = 0.93 Triglycerides: p = 0.78 QoL c: N/A FFQ: All ns change between groups |
| Wu et al., (2007) | Calorie-restricted diet (CRD) and physical exercise | Weight; BMI; body fat %, waist to hip ratio; blood lipids and metabolic parameters (serum glucose, triglyceride, cholesterol, insulin) | At 6 months: Weight (kg): CRD = –4.2 (4.4) (p < 0.001), CG = 1.0 (3.4) ns BMI: CRD = –1.59 (1.66) (p < 0.001), CG = 0.35 (1.30) ns WC (cm): CRD= 3.32 (4.18) (p < 0.001), CG = 1.02 (4.25) ns HC (cm): CRD = –3.3 (4.5) (p < 0.001), CG = 0.3 (2.7) ns Body fat %: CRD = –1.3 (6.4) ns, CG = 1.3 (4.2) ns Waist to hip ratio: CRD = −0.01 (0.4) ns, CG = 0.01 (0.3) ns At 6 months (p value for baseline to 6mth): Glucose (mg/dL): CRD = 96.4 (16.9) ns, CG = 99.8 (16.9) ns Triglyceride (mg/dL): CRD = 146.8 (90.9) (p < 0.001), CG = 239.3 (188.9) ns Cholesterol (mg/dL): CRD = 159.2 (36.9) ns, CG = 166.8 (35.2) ns Insulin (µIU/mL): CRD = 5.2 (3.1) (p < 0.001), CG = 9.5 (9.2) ns | At 6 months, CRD vs. Control: Weight (kg):p < 0.001 BMI: p < 0.001 WC (cm): p < 0.001 HC (cm): p < 0.05 Body fat %: ns Waist to hip ratio: ns At 6 months: Glucose (mg/dL): ns Triglyceride (mg/dL): p < 0.05 Cholesterol (mg/dL): ns Insulin (µIU/mL): ns |
| Niv et al., (2014) | Enhancing Quality-of-care In Psychosis (EQUIP)-psychosocial weight management program | Weight; BMI | At week 16, EQUIP: Weight (lbs):−2.4 (10.6), (t = 1.6, p = 0.12) BMI: −0.3 (1.5), (t = 1.5, p = 0.13) At 12 months: Weight: significant ↓in weight in both groups over time [F(1, 94) = 5.2, p < 0.05] BMI: significant ↓ in BMI in both groups over time [F(1, 94) = 5.7, p < 0.05] | At 12 months: Weight (lbs): EQUIP = −2.3 (18.0), CG = −2.2 (11.9); time x treatment group [F(1, 94) = 1.2, p > 0.05] BMI: EQUIP = −0.3 (2.6); CG = −0.3 (1.7); time x treatment group [F(1, 94) = 1.3, p > 0.05] |
| Iqbal et al., (2010) | Low-carbohydrate diet (LCD) or low-fat diet (LFD) | Weight; glucose; HbA1c; serum lipids; BP; dietary intake (24 hr recall) | At 24 months: (ITT analysis) Weight (kg): LC = −1.5, LF = −0.2; Glucose (mg/dL): ns HbA1c: ns All Serum lipids: ns SBP and DBP (mmHg): ns Dietary intake: ns | |
| North and Palmer, (2015) | Diabetes education | HbA1c; weight; SBP | Post Hoc (4-months): HbA1c c: IG = 7.18 (1.19), 6.61 (0.80); CG = 6.68 (0.61), 6.69 (0.74) (p < 0.001) Weight (lbs): IG = 228.95 (43.63), 224.33 (42.66); CG = 231.39 (45.27), 229.72 (45.27) (p < 0.001) SBP c: IG = 131.83 (17.43), 126.01 (15.84); CG = 131.33 (15.04), 128.01 (13.07) ns | |
| Dexter et al., (2019) | Healthy teaching kitchen | Weight; BMI; metabolic parameters (HbA1c, TC, LDL-C, HDL-C, Triglycerides); Questionnaires: cooking frequency (0–3), cooking confidence (0–5), fruit and vegetable incorporation (0–5), confidence in healthy cooking (0–5); Healthy Habits Questionnaire (HHQ, 0–75) | At 12 weeks: Mean change (SD) BMI: −0.35 (0.76) (p < 0.05) Weight (lbs): −2.91 (5.75) (p < 0.05) Metabolic parameters: ns HbA1c: −0.13 (0.94) ns TC: 0.63 (25.75) ns LDL-C: 0.57 (19.22) ns HDL-C: 0.93 (5.62) ns Triglycerides: −18.56 (113.11) ns Cooking confidence: 0.55 (1.07) (p< 0.001) Confidence in incorporating fruits and vegetables: 0.83 (0.89) (p < 0.001) Confidence in preparing healthy meals: 0.62 (1.01) (p < 0.001) Cooking frequency: 0.16 (0.70) ns HHQ (% change): Improvement in 9/10 questionnaire responses (p < 0.05) | |
| Friedberg et al., (2015) | Hypertension diet. Stage-matched intervention (SMI) or health education intervention (HEI) | BP; Diet adherence (DASH) | At 6 months: Improvement in proportion of participants with controlled BP: SMI = 19.7% (p < 0.001), HEI = 11.9% (p = 0.012), UC = 1.3% (p = 0.76) | At 6 months: Participants with controlled BP (%): SMI = 64.6, HEI = 54.3, UC = 45.8; (SMI vs. UC p = 0.001; HEI vs. UC p = 0.108) SBP [M(95% CI)] (mmHg): SMI = 131.2 (129.1, 133.3), HEI = 131.8 (129.9, 133.7), UC = 134.7 (132.7, 136.7); (SMI vs. UC p = 0.009; HEI vs. UC p = 0.047) (ns when adjusting for multiple comparisons) At 6 months: Change in SBP [M (95% CI)]: SMI = −4.7 (−6.9, −2.5), HEI = −5.4 (−8.5, −2.3), UC = −2.7 (−5, −4); (SMI vs. UC p = 0.007; HEI vs. UC p = 0.009) Change in DASH score [M (95% CI)]: SMI = 0.69 (−0.1, 1.5), HEI = −0.16 (−1.1, 0.8), UC = −0.76 (−1.5, 0) (SMI vs. UC p = 0.01; HEI vs. UC p = 0.32) |
| Sikand et al., (1998) | National Cholesterol Education Program (NCEP) Step 1 dietary intervention phase | Metabolic parameters (TC, LDL, HDL, triglycerides); BMI | At 8 weeks: % change, mean actual change value (SE) TC(mmol/L): −13.4%; −0.94 (0.09) (p < 0.0001) LDL (mmol/L): −14.2%; −0.76 (0.08) (p < 0.0001) HDL (mmol/L): −4.4%; −0.05 (0.02) (p < 0.05) Triglyceride: −10.8%; −0.22 (0.87) (p < 0.05) TC/HDL: −9.4%; −0.59 (0.14) (p < 0.001) LDL/HDL: −12.1%; −0.54 (0.11) (p < 0.001) BMI: 0.4%; −0.1 (0.52) ns | |
| Tan-Shalaby et al., (2016) | Modified Atkins Diet (Ketogenic diet) | Safety and feasibility: QoL (EORTC QLQ-c30); Weight; BMI; BP; blood lipids (TC, HDL-C, LDL-C, triglycerides); fasting glucose | Baseline to last visit: Weight (kg): baseline = 95 (18.7), last visit = 87.7 (37.82); change = −7.5 (5.8) (p < 0.0001) BMI: −2.669 (1.99) (p < 0.001) Other biochemical parameters: ns DBP: baseline = 70 (11.27), last visit = 77 (5.57) (p = 0.043) QoL, pts on diet for 4+ weeks (n = 6): ns | |
| Holton et al., (2020) | Low Glutamate Diet | Total symptom score (TSS, 0–33); Improvement (≥30% symptom remission); Patient Global Impression of Change Scale (PGIC); Chalder Fatigue Scale | At 1 month: TSS: pre-diet = 21 (5), post-diet = 12 (5) (p < 0.0001) Improvement: IG = 65% participants PGIC: IG = 73% improved Chalder Fatigue Scale: pre-diet = 29 (8), post-diet = 16 (9) (p < 0.0001) | At 1 month: TSS: IG = 11.7 (5.3), CG = 18.1 (5.7) (p = 0.0009); effect size d = 1.16 |
| Bayer-Carter et al., (2011) | HIGH (high-saturated fat/high-glycaemic index diet) or LOW (low-saturated/low-glycaemic index diet) | Insulin and glucose levels; Homeostasis Model Assessment of Insulin Resistance (HOMA-IR); blood lipids (TC, LDL-C, HDL-C); weight | At week 4 c: Insulin AUC: For both diagnoses, HIGH diet ↑ and LOW diet ↓ insulin AUC (time x diet p = 0.01) Glucose AUC: ns HOMA-IR: ns (time x diet p = 0.06) Weight: ns TC: differed between groups (time × diet × diagnosis p = 0.04)-due to HIGH diet ↑ TC and LOW diet ↓ TC for both diagnoses (time × diet, p < 0.001). 2-fold greater changes in aMCI compared to healthy participants. Change scores for both diagnostic groups in either diet condition = ns LDL: time × diet × diagnosis p = 0.048; time × diet p < 0.001; no differences between CG vs. aMCI diagnoses change scores. HDL: ↑ with HIGH diet and ↓ with LOW diet (time × diet p < 0.001) LDL/HDL: ↑ by HIGH diet and ↓ by LOW diet for both diagnoses (time × diet p = 0.04) | |
| Serra et al., (2021) | Nutrition education | Behavioural Risk Factor Surveillance System (BRFSS); F&V intake Questionnaire, self-rated diet quality (VAS) | Baseline to last class: In those attending ≥ 2 group classes (n = 24): Daily F&V intake [M(SEM)]: baseline = 3.4 (1.9), post-intervention = 4.1 (2.0) servings/day (p = 0.07) Consumption of ≥5 F&V servings/day: baseline = 21%, post-intervention = 33% (p < 0.01) Self-rated diet quality [M(SEM)]: baseline = 4.7 (0.5), post-intervention = 5.9 (0.4) (p = 0.03) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mellor, R.; Saunders-Dow, E.; Mayr, H.L. Scope of Use and Effectiveness of Dietary Interventions for Improving Health-Related Outcomes in Veterans: A Systematic Review. Nutrients 2022, 14, 2094. https://doi.org/10.3390/nu14102094
Mellor R, Saunders-Dow E, Mayr HL. Scope of Use and Effectiveness of Dietary Interventions for Improving Health-Related Outcomes in Veterans: A Systematic Review. Nutrients. 2022; 14(10):2094. https://doi.org/10.3390/nu14102094
Chicago/Turabian StyleMellor, Rebecca, Elise Saunders-Dow, and Hannah L. Mayr. 2022. "Scope of Use and Effectiveness of Dietary Interventions for Improving Health-Related Outcomes in Veterans: A Systematic Review" Nutrients 14, no. 10: 2094. https://doi.org/10.3390/nu14102094
APA StyleMellor, R., Saunders-Dow, E., & Mayr, H. L. (2022). Scope of Use and Effectiveness of Dietary Interventions for Improving Health-Related Outcomes in Veterans: A Systematic Review. Nutrients, 14(10), 2094. https://doi.org/10.3390/nu14102094