
Is There a Correlation between Dietary and Blood Cholesterol? Evidence from Epidemiological Data and Clinical Interventions



Abstract
:1. Introduction
2. Epidemiolocal Evidence
3. Meta-Analysis

{kind=link}
| Population/Number of Studies | Association Assessed | Main Result | Reference (Year) |
|---|---|---|---|
| 177,555 adults from PURE, TRASCEND and ONTARGET studies | Egg consumption with blood lipids and CVD | Higher egg intake is not associated with TC, LDL, TG, HDL, total mortality, or CVD. | [23] (2020) |
| 8095 hypertense adults from the China Health and Nutrition Survey | Cholesterol intake from eggs and other sources and mortality | Cholesterol from eggs but not other sources is associated with lower mortality. | [28] (2020) |
| 8358 Chinese adults | Dietary cholesterol and dyslipidemia | Cholesterol intake is associated with lower plasma TG and higher HDL-cholesterol in women, but not men. Cholesterol from eggs is associated with lower risk of dyslipidemia. | [34] (2022) |
| Three large cohort studies: NHS (1980–2012), NHS II (1991–2017) and HPFS (1986–2016). 16 prospective cohort studies (6 American, 8 European, and 2 Asian) | Egg intake and CVD risk | An increase of one egg per day is not associated with any CVD risk. Egg intake is associated with lower CVD risk in Asian populations. | [39] (2017) |
| 39 prospective cohort studies from North America, Europe, and Asia | Egg consumption and the risk of CVD, CHD, and stroke | Consumption of six eggs per week has an inverse association with CVD events (but not stroke), when compared to no intake. No association is found for stroke. | [35] (2021) |
| 40 studies with participants without diagnosed CVD | No association between dietary cholesterol and coronary artery disease (CAD), ischemic stroke, or hemorrhagic stroke. Dietary cholesterol increases total blood cholesterol, without affecting LDL/HDL ratio. | [36] (2015) | |
| NHS (1980–2012), NHS II (1991–2017) and HPFS (1986–2016). 16 prospective cohort studies (6 American, 8 European, and 2 Asian) | Eegg intake and the risk of developing T2DM | Higher egg intake is associated with lower prevalence of hypercholesterolemia. | [42] (2020) |
4. Clinical Interventions. Effects of Dietary Cholesterol on Plasma Lipids and Lipoprotein Subfractions
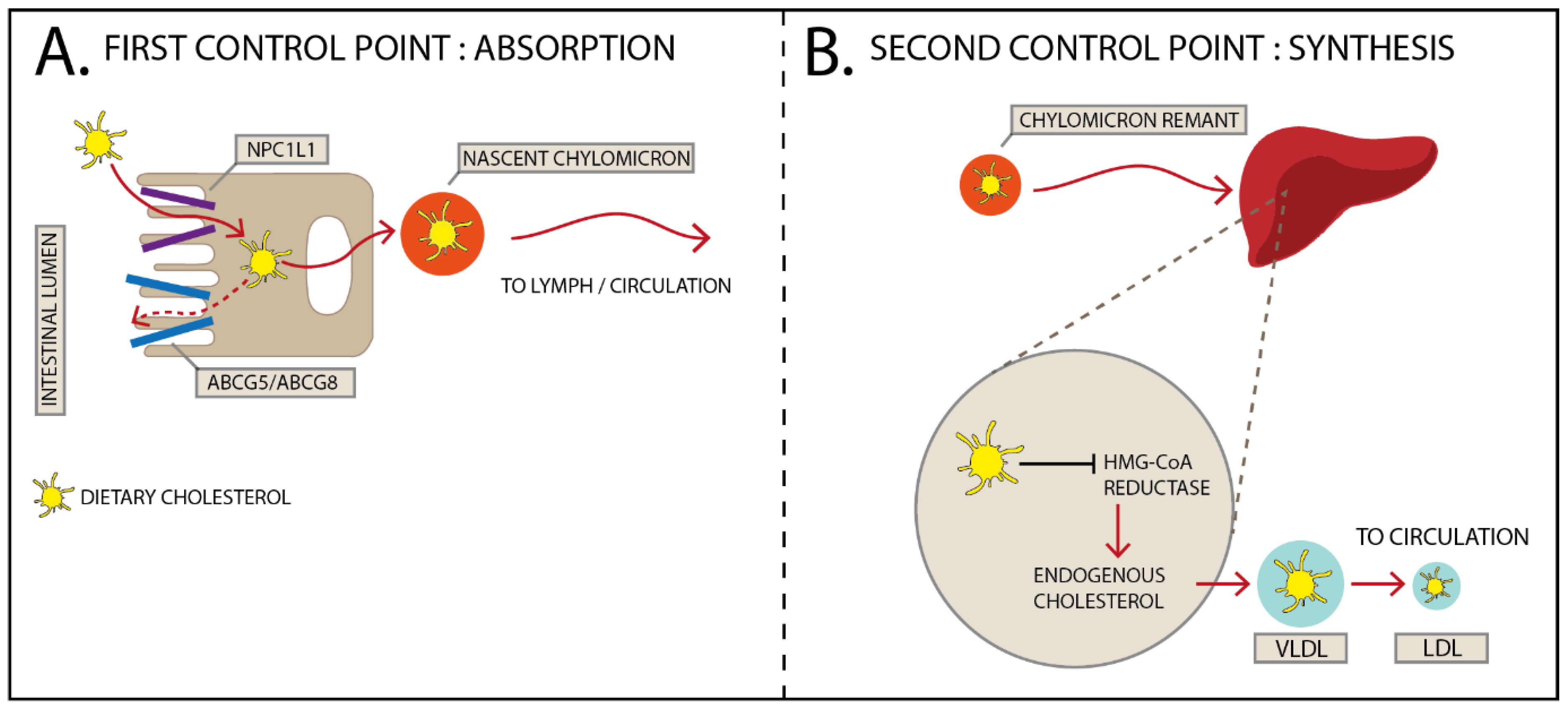
5. Mechanisms to Manage Dietary Cholesterol
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Committee on Nutrition. American Heart Association. Diet and Heart Disease; American Heart Association: Dallas, TX, USA, 1968. [Google Scholar]
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans, 8th ed. 2015. Available online: https://health.gov/our-work/food-nutrition/previous-dietary-guidelines/2015 (accessed on 8 May 2022).
- Vergnes, L.; Phan, J.; Strauss, M.; Tafuri, S.; Reue, K. Cholesterol and cholate components of an atherogenic diet induce distinct stages of hepatic inflammatory gene expression. J. Biol. Chem. 2003, 278, 42774–42784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.T.; Lin, H.Y.; Chan, Y.W.; Li, K.H.; To, O.T.; Yan, B.P.; Liu, T.; Li, G.; Wong, W.T.; Keung, W.; et al. Mouse models of atherosclerosis: A historical perspective and recent advances. Lipids Health Dis. 2017, 16, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishibashi, S.; Goldstein, J.L.; Brown, M.S.; Herz, J.; Burns, D.K. Massive xanthomatosis and atherosclerosis in cholesterol-fed low density lipoprotein receptor-negative mice. J. Clin. Investig. 1994, 93, 1885–1893. [Google Scholar] [CrossRef] [PubMed]
- Dawber, T.R.; Nickerson, R.J.; Brand, F.N.; Pool, J. Eggs, serum cholesterol, and coronary heart disease. Am. J. Clin. Nutr. 1982, 36, 617–625. [Google Scholar] [CrossRef] [Green Version]
- Hu, F.; Stampfer, M.J.; Rimm, E.; Manson, J.E.; Ascherio, A.; Golditz, G.A.; Rosner, B.A.; Spiegelman, D.; Speizer, F.E.; Sacks, F.M.; et al. A prospective study of egg consumption and risk of cardiovascular disease in men and women. JAMA 1999, 281, 1387–1894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, W.O.; Kerver, J.M. Nutritional Contribution of Eggs to American Diets. J. Am. Coll. Nutr. 2000, 19, 556S–562S. [Google Scholar] [CrossRef] [PubMed]
- Magriplis, E.; Mitsopoulou, A.-V.; Karageorgou, D.; Bakogianni, I.; Dimakopoulos, I.; Micha, R.; Michas, G.; Chourdakis, M.; Chrousos, G.; Roma, E.; et al. Frequency and Quantity of Egg Intake Is Not Associated with Dyslipidemia: The Hellenic National Nutrition and Health Survey (HNNHS). Nutrients 2019, 11, 1105. [Google Scholar] [CrossRef] [Green Version]
- Ballesteros, M.N.; Cabrera, R.M.; Saucedo, M.S.; Fernandez, M.L. Dietary cholesterol does not increase biomarkers for chronic disease in a pediatric population at risk from Northern Mexico. Am. J. Clin. Nutr. 2004, 80, 855–861. [Google Scholar] [CrossRef] [Green Version]
- Missimer, A.; DiMarco, D.M.; Andersen, C.J.; Murillo, A.G.; Fernandez, M.L. Consuming 2 eggs per day, as compared to an oatmeal breakfast, decreases plasma ghrelin and maintains the LDL/HDL ratio. Nutrients 2017, 9, 89. [Google Scholar] [CrossRef] [Green Version]
- DiMarco, D.M.; Missimer, A.; Murillo, A.G.; Lemos, B.; Malysheva, O.V.; Caudill, M.A.; Blesso, C.N.; Fernandez, M.L. Intake of up to 3 eggs per day increases HDL cholesterol and plasma choline while plasma trimethylamine-N-Oxide is unchanged in a healthy population. Lipids 2017, 52, 255–263. [Google Scholar] [CrossRef]
- Greene, C.M.; Zern, T.; Wood, R.J.; Aggarwal, D.; Sharman, M.; Volek, J.S.; Fernandez, M.L. Maintenance of the LDL choles-terol: HDL cholesterol ratio in an elderly population given a dietary cholesterol challenge. J. Nutr. 2005, 135, 2793–2798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vshwanathan, R.; Goodrwo-Kotyla, E.F.; Wooten, B.R.; Wilson, T.A.; Nicolosi, R.J. Consumption of 2 and 4 egg yolks/d for 5 wk increases macular pigment concentrations in older adults with low macular pigment taking cholesterol-lowering statins. Am J. Clin. Nutr. 2009, 90, 1272–1279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wal, J.V.; Gupta, A.; Khosla, P.; Dhurandhar, N.V. Egg breakfast enhances weight loss. Int. J. Obes. 2008, 32, 1545–1551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mutungi, G.; Ratliff, J.; Puglisi, M.; Torres-Gonzalez, M.; Vaishnav, U.; Leite, J.; Quann, E.; Volek, J.S.; Fernandez, M.L. Dietary cholesterol from eggs increas-es HDL cholesterol in overweight men consuming a carbohydrate restricted diet. J. Nutr. 2008, 138, 272–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blesso, C.N.; Andersen, C.J.; Barona, J.; Volek, J.; Fernandez, M.L. Whole egg consumption improves lipoprotein profiles and insulin sensitivity in individuals with metabolic syndrome. Metabolism 2013, 62, 400–410. [Google Scholar] [CrossRef]
- Dibella, M.; Thomas, M.S.; Al-Yousef, H.; Millar, C.; Blesso, C.N.; Malisheva, O. Choline intake as supplement or as a com-ponent of eggs increases plasma choline and reduces interleukin-6 without modifying plasma cholesterol in participants with metabolic syndrome. Nutrients 2020, 12, 3120. [Google Scholar] [CrossRef]
- Ballesteros, M.N.; Valenzuela, F.; Robles, A.E.; Artalejo, E.; Aguilar, D.; Andersen, C.J.; Valdez, H.; Fernandez, M.L. One Egg per Day Improves Inflammation when Compared to an Oatmeal-Based Breakfast without Increasing Other Cardiometabolic Risk Factors in Diabetic Patients. Nutrients 2015, 7, 3449–3463. [Google Scholar] [CrossRef] [PubMed]
- Pearce, K.L.; Clifton, P.M.; Noakes, M. Egg consumption as part of an energy-restricted high-protein diet improves blood lipid and blood glucose profiles in individuals with type 2 diabetes. Brit. J. Nutr. 2011, 105, 584–592. [Google Scholar] [CrossRef] [Green Version]
- Herron, K.L.; Vega-Lopez, S.; Conde, K.; Ramjiganesh, T.; Roy, S.; Shachter, N.S.; Fernandez, M.L. Pre-Menopausal Women, Classified as Hypo-or Hyper-Responders, do not Alter their LDL/HDL Ratio Following a High Dietary Cholesterol Challenge. J. Am. Coll. Nutr. 2002, 21, 250–258. [Google Scholar] [CrossRef]
- Andersen, C.J.; Blesso, C.N.; Lee, J.Y.; Park, Y.K.; Fernandez, M.L. Egg consumption modulates HDL composition and in-creases the cholesterol accepting capacity of serum in metabolic syndrome. Lipids 2013, 48, 557–567. [Google Scholar] [CrossRef] [Green Version]
- Dehghan, M.; Mente, A.; Rangarajan, S.; Mohan, V.; Lear, S.; Swaminathan, S.; Wielgosz, A.; Seron, P.; Avezum, A.; Lopez-Jaramillo, P.; et al. Association of egg intake with blood lipids, cardiovascular disease, and mortality in 177,000 people in 50 countries. Am. J. Clin. Nutr. 2020, 111, 795–803. [Google Scholar] [CrossRef] [PubMed]
- Carson, J.A.S.; Lichtenstein, A.H.; Anderson, C.A.M.; Appel, L.J.; Kris-Etherton, P.M.; Meyer, K.A.; Van Horn, L. Dietary choles-terol and cardiovascular risk: A science advisory from the American heart association. Circulation 2020, 141, E39–E53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhuang, P.; Wu, F.; Mao, L.; Zhu, F.; Zhang, Y.; Chen, X.; Jiao, J.; Zhang, Y. Egg and cholesterol consumption and mortality from cardio-vascular and different causes in the United States: A population-based cohort study. PLoS Med. 2021, 18, e1003508. [Google Scholar] [CrossRef] [PubMed]
- Zhong, V.W.; Van Horn, L.; Cornelis, M.C.; Wilkins, J.T.; Ning, H.; Carnethon, M.; Greenland, P.; Mentz, R.J.; Tucker, K.L.; Zhao, L.; et al. Associations of Dietary Cholesterol or Egg Consumption With Incident Cardiovascular Disease and Mortality. JAMA 2019, 321, 1081–1095. [Google Scholar] [CrossRef]
- Fuchs, F.D.; Whelton, P.K. High Blood Pressure and Cardiovascular Disease. Hypertension 2020, 75, 285–292. [Google Scholar] [CrossRef]
- Wu, F.; Zhuang, P.; Zhang, Y.; Zhan, C.; Zhang, Y.; Jiao, J. Egg and Dietary Cholesterol Consumption and Mortality Among Hypertensive Patients: Results From a Population-Based Nationwide Study. Front. Nutr. 2021, 8, 1–10. [Google Scholar] [CrossRef]
- Sacks, F.M.; Lichtenstein, A.H.; Wu, J.H.Y.; Appel, L.J.; Creager, M.A.; Kris-Etherton, P.M.; Miller, M.; Rimm, E.B.; Rudel, L.L.; Robinson, J.G.; et al. Dietary fats and cardio-vascular disease: A presidential advisory from the American Heart Association. Circulation 2017, 136, e1–e23. [Google Scholar] [CrossRef]
- Andersen, C.J. Bioactive Egg Components and Inflammation. Nutrients 2015, 7, 7889–7913. [Google Scholar] [CrossRef] [Green Version]
- Hezaveh, Z.S.; Sikaroudi, M.K.; Vafa, M.; Clayton, Z.S.; Soltani, S. Effect of egg consumption on inflammatory markers: A systematic review and meta-analysis of randomized controlled clinical trials. J. Sci. Food. Agric. 2019, 99, 6663–6670. [Google Scholar] [CrossRef]
- Blesso, C.N.; Andersen, C.J.; Bolling, B.W.; Fernandez, M.L. Egg intake improves carotenoid status by increasing plasma HDL cholesterol in adults with metabolic syndrome. Food Funct. 2012, 4, 213–221. [Google Scholar] [CrossRef]
- Nimalaratne, C.; Wu, J. Hen Egg as an Antioxidant Food Commodity: A Review. Nutrients 2015, 7, 8274–8293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, J.; Han, W.; Jiang, Y.; Wu, J.; Zhou, X. Association of dietary cholesterol and dyslipidemia in Chinese health examinees. J. Heal. Popul. Nutr. 2022, 41, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Micek, A.; Brzostek, T.; Toledo, E.; Iacoviello, L.; Astrup, A.; Franco, O.H.; Galvano, F.; Martinez-Gonzalez, M.A.; Grosso, G. Egg consumption and cardiovascular risk: A dose–response meta-analysis of prospective cohort studies. Eur. J. Nutr. 2020, 60, 1833–1862. [Google Scholar] [CrossRef] [PubMed]
- Hansel, B.; Giral, P. Cholestérol alimentaire et morbi/mortalité cardiovasculaire. OCL 2015, 22, D202. [Google Scholar] [CrossRef] [Green Version]
- Millán, J.; Pintó, X.; Muñoz, A.; Zúñiga, M.; Rubiés-Prat, J.; Pallardo, L.F.; Masana, L.; Mangas, A.; Hernández-Mijares, A.; González-Santos, P.; et al. Lipoprotein ratios: Physiological significance and clinical usefulness in cardiovascular prevention. Vasc. Heal. Risk Manag. 2009, 5, 757. [Google Scholar] [CrossRef] [Green Version]
- Torres, N.; Guevara-Cruz, M.; Velázquez-Villegas, L.A.; Tovar, A.R. Nutrition and Atherosclerosis. Arch. Med. Res. 2015, 46, 408–426. [Google Scholar] [CrossRef]
- Drouin-Chartier, J.-P.; Chen, S.; Li, Y.; Schwab, A.L.; Stampfer, M.J.; Sacks, F.M.; Rosner, B.; Willett, W.C.; Hu, F.B.; Bhupathiraju, S.N. Egg consumption and risk of cardiovascular disease: Three large prospective US cohort studies, systematic review, and updated meta-analysis. BMJ 2020, 368, m513. [Google Scholar] [CrossRef] [Green Version]
- Ahmmed, S.; Das Shuvo, S.; Paul, D.K.; Karim, M.R.; Kamruzzaman, M.; Mahmud, N.; Ferdaus, J.; Elahi, T. Prevalence of dyslipidemia and associated risk factors among newly diagnosed Type-2 Diabetes Mellitus (T2DM) patients in Kushtia, Bangladesh. PLOS Glob. Public Heal. 2021, 1, e0000003. [Google Scholar] [CrossRef]
- Peng, J.; Zhao, F.; Yang, X.; Pan, X.; Xin, J.; Wu, M.; Peng, Y.G. Association between dyslipidemia and risk of type 2 diabetes mellitus in middle-aged and older Chinese adults: A secondary analysis of a nationwide cohort. BMJ Open 2021, 11, e042821. [Google Scholar] [CrossRef]
- Drouin-Chartier, J.-P.; Schwab, A.L.; Chen, S.; Li, Y.; Sacks, F.M.; Rosner, B.; E Manson, J.; Willett, W.C.; Stampfer, M.J.; Hu, F.B.; et al. Egg consumption and risk of type 2 diabetes: Findings from 3 large US cohort studies of men and women and a systematic review and meta-analysis of prospective cohort studies. Am. J. Clin. Nutr. 2020, 112, 619–630. [Google Scholar] [CrossRef]
- Kopp, W. How Western Diet And Lifestyle Drive The Pandemic Of Obesity And Civilization Diseases. Diabetes Metab. Syndr. Obes. 2019, 12, 2221–2236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemos, B.S.; Medina-Vera, I.; Blesso, C.N.; Fernandez, M.L. Intake of 3 Eggs per Day When Compared to a Choline Bitartrate Supplement, Downregulates Cholesterol Synthesis without Changing the LDL/HDL Ratio. Nutrients 2018, 10, 258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maki, K.C.; Palacios, O.M.; Kramer, M.W.; Trivedi, R.; Dicklin, M.R.; Wilcox, M.L.; Maki, C.E. Effects of substituting eggs for high-carbohydrate breakfast foods on the cardiometabolic risk-factor profile in adults at risk for type 2 diabetes mellitus. Eur. J. Clin. Nutr. 2020, 74, 784–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.-E.; Campbell, W.W. Total cholesterol concentration in men and women: Results from 2 randomized controlled crossover studies. Nutrients 2018, 10, 1272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayurasakorn, K.; Srisura, W.; Sitphahul, P.; Hongto, P.-O. High-density lipoprotein cholesterol changes after continuous egg consumption in healthy adults. J. Med. Assoc. Thail. 2008, 91, 400. [Google Scholar]
- Vislocky, L.M.; Pikosky, M.A.; Rubin, K.H.; Vega-López, S.; Gaine, P.C.; Martin, W.F.; Zern, T.L.; Lofgren, I.E.; Fernandez, M.L.; Rodriguez, N.R. Habitual consumption of eggs does not alter the beneficial effects of endurance training on plasma lipids and lipoprotein metabolism in untrained men and women. J. Nutr. Biochem. 2009, 20, 26–34. [Google Scholar] [CrossRef]
- Rueda, J.M.; Khosla, P. Impact of Breakfasts (with or without Eggs) on Body Weight Regulation and blood Lipids in Uni-versity Students over a 14-Week Semester. Nutrients 2013, 5, 5097–5113. [Google Scholar] [CrossRef] [Green Version]
- Khatana, C.; Saini, N.K.; Chakrabarti, S.; Saini, V.; Sharma, A.; Saini, R.V.; Saini, A.K. Mechanistic Insights into the Oxidized Low-Density Lipoprotein-Induced Atherosclerosis. Oxid. Med. Cell. Longev. 2020, 2020, 1–14. [Google Scholar] [CrossRef]
- DiMarco, D.M.; Norris, G.H.; Millar, C.L.; Blesso, C.N.; Fernandez, M.L. Intake of up to 3 Eggs per Day Is Associated with Changes in HDL Function and Increased Plasma Antioxidants in Healthy, Young Adults. J. Nutr. 2017, 147, 323–329. [Google Scholar] [CrossRef]
- Missimer, A.; Fernandez, M.L.; DiMarco, D.M.; Norris, G.H.; Blesso, C.N.; Murillo, A.G.; Vergara-Jimenez, M.; Lemos, B.S.; Medina-Vera, I.; Malysheva, O.V.; et al. Compared to an oatmeal breakfast, two eggs/day increased plasma carotenoids and choline without increasing trimethyl amine N-oxide concentrations. J. Am. Coll Nutr. 2018, 37, 140–148. [Google Scholar] [CrossRef]
- Greene, C.M.; Waters, D.; Clark, R.M.; Contois, J.H.; Fernandez, M.L. Plasma LDL and HDL characteristics and carotenoid content are positively influenced by egg consumption in an elderly population1. Nutr. Metab. 2006, 3, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mutungi, G.; Waters, D.; Ratliff, J.; Puglisi, M.; Clark, R.M.; Volek, J.S.; Fernandez, M.L. Eggs distinctly modulate plasma carotenoid and lipoprotein subclasses in adult men following a carbohydrate-restricted diet. J. Nutr. Biochem. 2010, 21, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Herron, K.L.; Lofgren, I.E.; Sharman, M.; Volek, J.S.; Fernandez, M.L. High intake of cholesterol results in less atherogenic low-density lipoprotein particles in men and women independent of response classification. Metabolism 2004, 53, 823–830. [Google Scholar] [CrossRef] [PubMed]
- Pascot, A.; Lemieux, I.; Prud’homme, D.; Tremblay, A.; Nadeau, A.; Couillard, C.; Després, J.P. Reduced HDL particle size as an additional feature of the atherogenic dyslipidemia of abnormal obesity. J. Lipid Res. 2001, 42, 2007–2014. [Google Scholar] [CrossRef]
- Blesso, C.N.; Andersen, C.J.; Bolling, B.; Fernandez, M.L. Egg intake improves carotenoid status by increasing HDL cholesterol in adults with metabolic syndrome. Food Funct. 2013, 4, 213–221. [Google Scholar]
- Sawrey-Kubicek, L.; Zhu, C.; Bardagjy, A.S.; Rhodes, C.H.; Sacchi, R.; Randolph, J.M.; Steinberg, F.M.; Zivkovic, A.M. Whole egg consumption compared with yolk-free egg increases the cholesterol efflux capacity of high-density lipoproteins in overweight, postmenopausal women. Am. J. Clin. Nutr. 2019, 110, 617–627. [Google Scholar] [CrossRef]
- McNamara, D.J.; Kolb, R.; Parker, T.S.; Batwin, H.; Samues, P.; Brown, C.D.; Ahrens, E.H., Jr. Heterogeneity of cholesterol homeostasis in man. Responses to changes in dietary fat quality and cholesterol quantity. J. Clin. Investig. 1987, 79, 1729–1739. [Google Scholar] [CrossRef]
- Betters, J.L.; Yu, L. NPC1L1 and cholesterol transport. Febs Lett. 2010, 584, 2740–2747. [Google Scholar] [CrossRef] [Green Version]
- Bosner, M.S.; Lange, L.G.; Stenson, W.F.; Ostlund, R.E., Jr. Percent cholesterol absorption in normal women and men quantified with dual stable isotopic tracers and negative ion mass spectrometry. J. Lipid Res. 1999, 40, 302–308. [Google Scholar] [CrossRef]
- Altmann, S.W.; Davis, H.R., Jr.; Zhu, L.-J.; Yao, X.; Hoos, L.M.; Tetzloff, G.; Iyer, S.P.N.; Maguire, M.; Golovko, A.; Zeng, M.; et al. Niemann-Pick C1 Like 1 Protein Is Critical for Intestinal Cholesterol Absorption. Science 2004, 303, 1201–1204. [Google Scholar] [CrossRef] [Green Version]
- Chambers, C.M.; Ness, G.C. Dietary cholesterol regulates hepatic 3-hydroxy-3-methylglutaryl gene expression in rats primarily at the level of translation. Arch. Biochem. Biophys. 1998, 354, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.S.; Goldstein, J.L. The SREBP pathway: Regulation of cholesterol metabolism by proteolysis of a mem-brane-bound transcription factor. Cell 1997, 89, 331–340. [Google Scholar] [CrossRef] [Green Version]
- Kern, F. Normal Plasma Cholesterol in an 88-Year-Old Man Who Eats 25 Eggs a Day. N. Engl. J. Med. 1991, 324, 896–899. [Google Scholar] [CrossRef] [PubMed]
| Lipoprotein | Dietary Cholesterol Intake and Population | Changes | Reference (Year) |
|---|---|---|---|
| LDL Diameter Compared to added 0 mg/d cholesterol | 510 mg/day for 4 weeks in children | LDL diameter was larger | [10] (2005) |
| Large LDL compared to 0 added mg/cholesterol | 640 mg/day for 4 weeks in elderly people | Higher concentrations of large LDL | [53] (2006) |
| Large LDL compared to 0 mg of added dietary cholesterol | 210, 425, and 640 mg/day in young individuals for 4 weeks each | Higher concentrations of large LDL | [51] (2017) |
| Large LDL Compared to an oatmeal breakfast | 640 mg/day for 4 weeks in young population | Higher concentrations of large LDL | [52] (2018) |
| Large LDL: Compared to 0 mg of added dietary cholesterol | 640 mg/day for 4 weeks in an overweight/obese population | Higher concentrations of large LDL | [54] (2010) |
| Small LDL: Compared to 0 mg of added dietary cholesterol | 210, 425, and 640 mg/day in young individuals for 4 weeks each | Lower concentrations of small LDL | [51] (2017) |
| Small LDL: Compared to 0 mg of dietary cholesterol | 640 mg/day for 4 weeks in an overweight/obese population | Lower concentrations of small LDL | [54] (2010) |
| HDL Diameter: Compared to 0 mg of added dietary cholesterol | 640 mg/day for 4 weeks in elderly people | Larger HDL diameter | [53] (2006) |
| Large HDL: Compared to 0 mg of added dietary cholesterol | 210, 425, and 640 mg/day in young individuals for 4 weeks each | Higher concentrations of large HDL | [51] (2005) |
| Large HDL: Compared to an oatmeal breakfast | 640 mg/day for 4 weeks in young population | Higher concentrations of large HDL | [52] (2018) |
| Large HDL: Compared to 0 mg of added dietary cholesterol | 640 mg/day for 4 weeks in an overweight/obese population | Higher concentrations of large HDL | [54] (2010) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernandez, M.L.; Murillo, A.G. Is There a Correlation between Dietary and Blood Cholesterol? Evidence from Epidemiological Data and Clinical Interventions. Nutrients 2022, 14, 2168. https://doi.org/10.3390/nu14102168
Fernandez ML, Murillo AG. Is There a Correlation between Dietary and Blood Cholesterol? Evidence from Epidemiological Data and Clinical Interventions. Nutrients. 2022; 14(10):2168. https://doi.org/10.3390/nu14102168
Chicago/Turabian StyleFernandez, Maria Luz, and Ana Gabriela Murillo. 2022. "Is There a Correlation between Dietary and Blood Cholesterol? Evidence from Epidemiological Data and Clinical Interventions" Nutrients 14, no. 10: 2168. https://doi.org/10.3390/nu14102168
APA StyleFernandez, M. L., & Murillo, A. G. (2022). Is There a Correlation between Dietary and Blood Cholesterol? Evidence from Epidemiological Data and Clinical Interventions. Nutrients, 14(10), 2168. https://doi.org/10.3390/nu14102168