
Circulating Levels of Short-Chain Fatty Acids during Pregnancy and Infant Neurodevelopment

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Procedure
2.2. Instruments and Data Collection
2.2.1. Measurements
2.2.2. Adjustment Measurements
2.3. Statistical Analysis
3. Results
3.1. General Descriptive Data of the Sample
3.2. General Descriptive Data of the Levels of Short Chain Fatty Acids
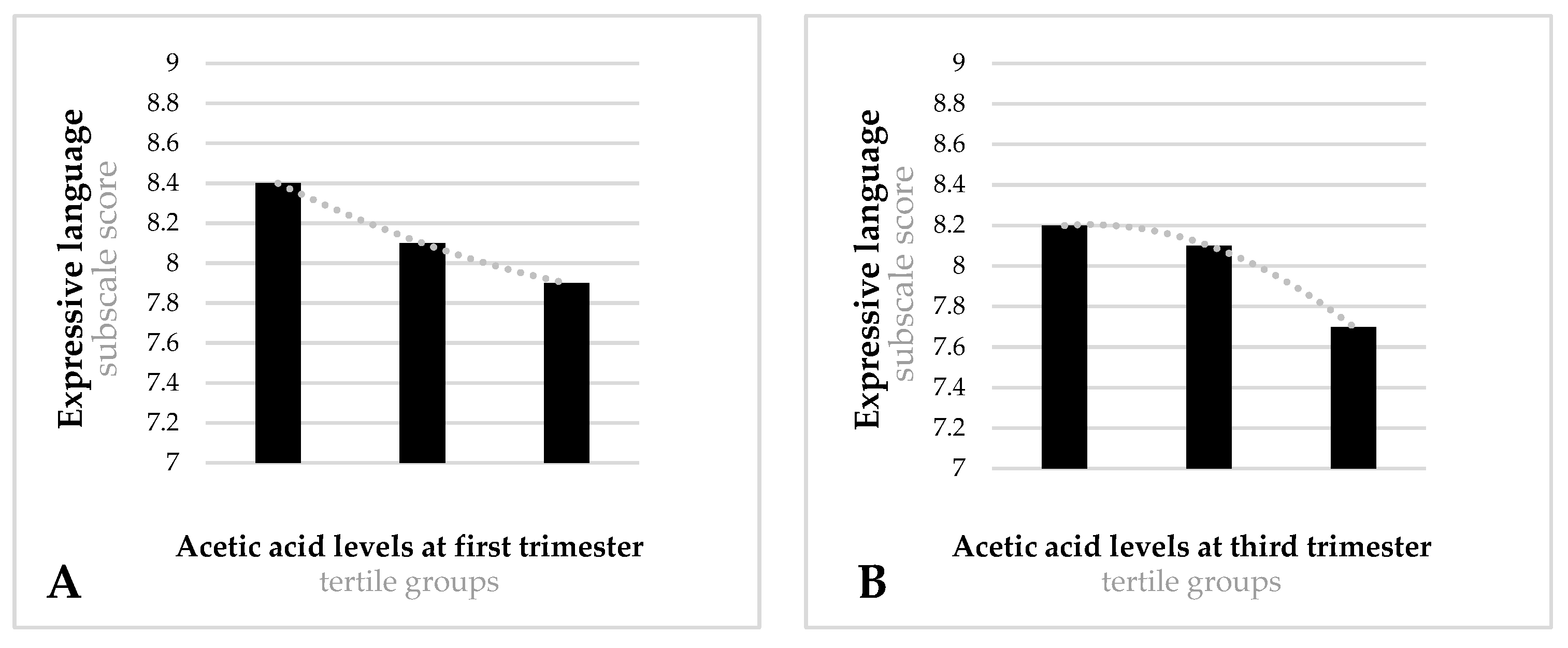
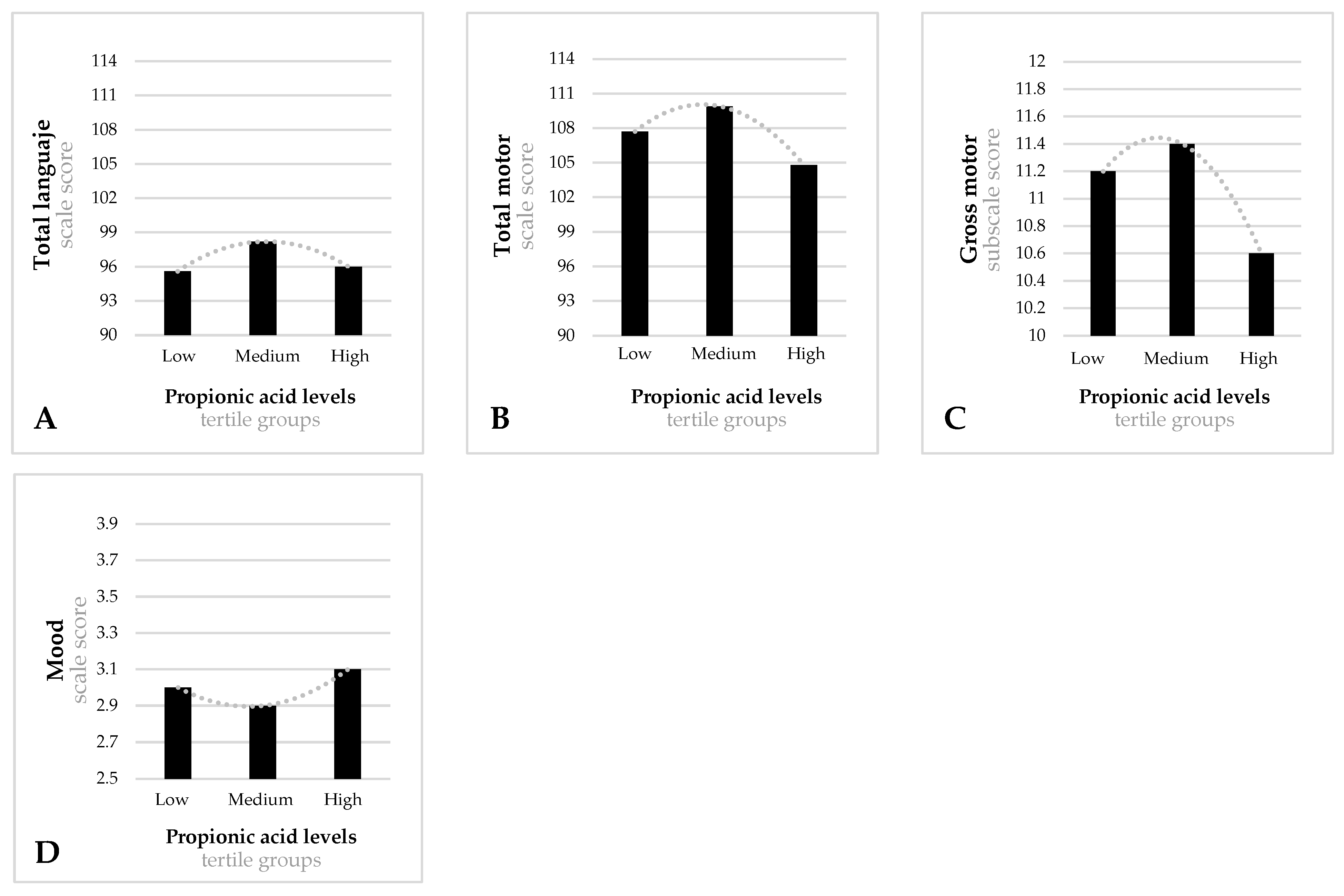
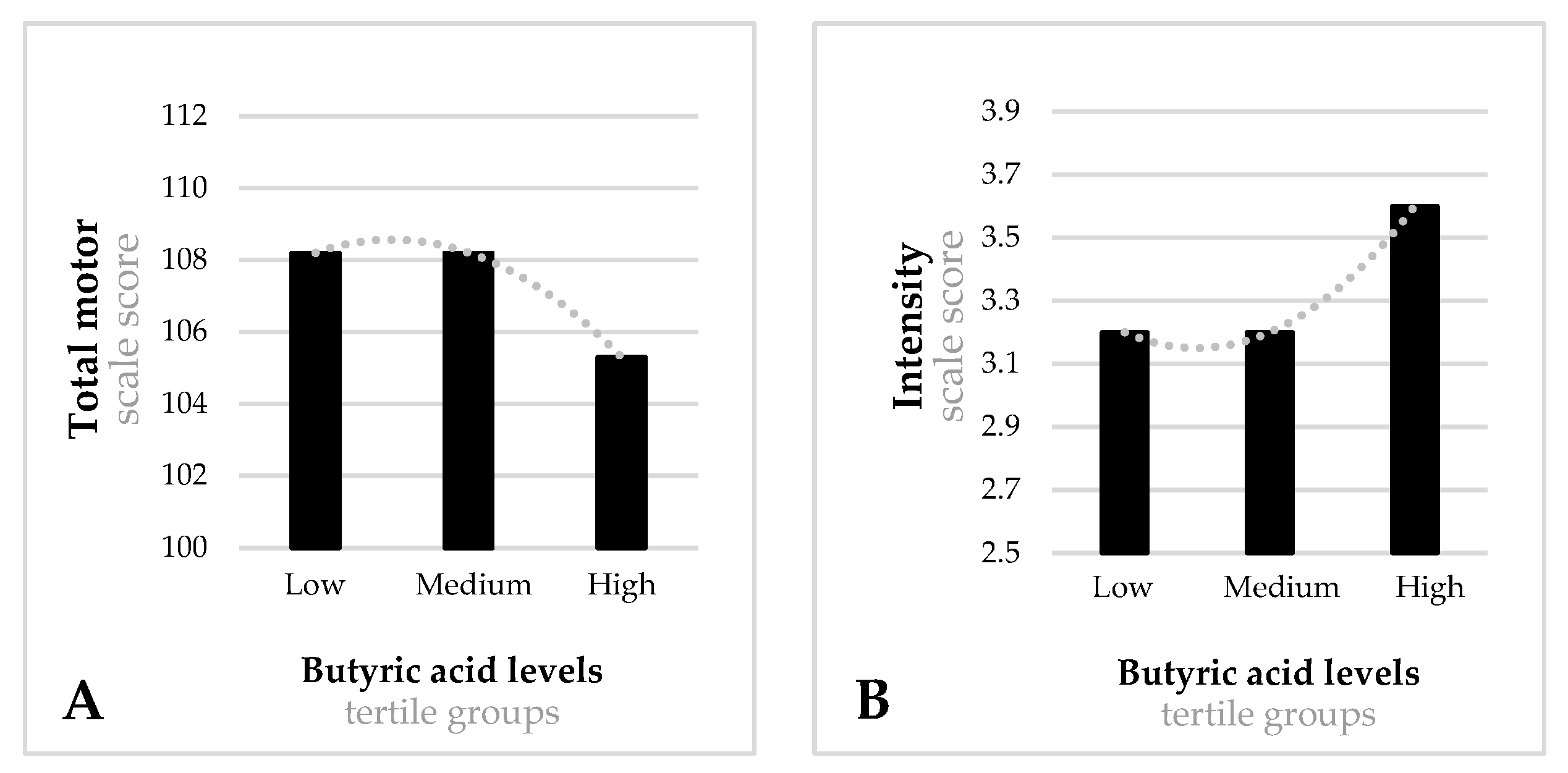
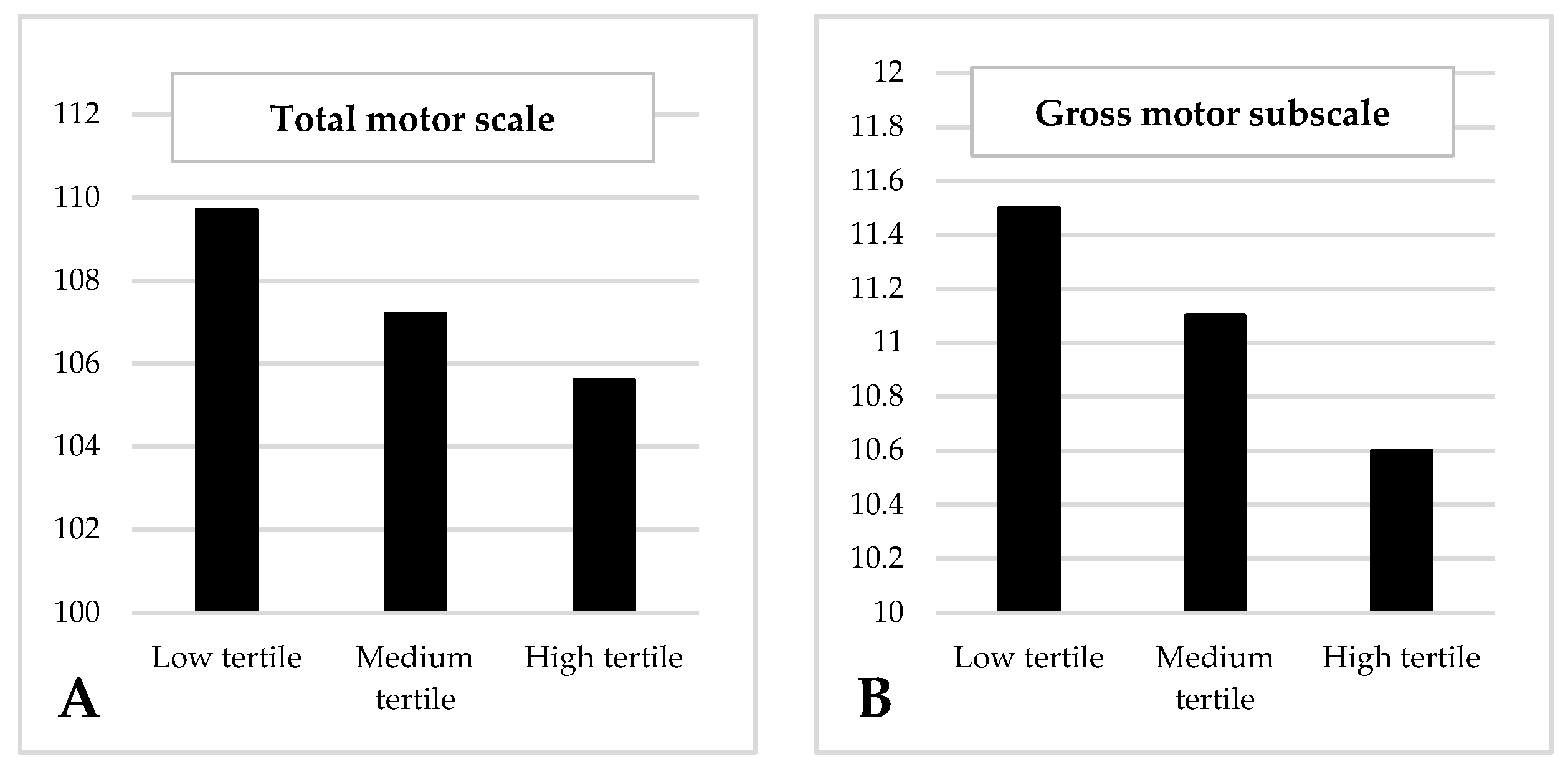
3.3. Cognitive Development and Temperament for Levels of Acetic, Propionic, Butyric and Isobutyric acid during the First and Third Trimester of Pregnancy
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cryan, J.F.; Dinan, T.G. Mind-Altering Microorganisms: The Impact of the Gut Microbiota on Brain and Behaviour. Nat. Rev. Neurosci. 2012, 13, 701–712. [Google Scholar] [CrossRef] [PubMed]
- Carlson, A.L.; Xia, K.; Azcarate-Peril, M.A.; Goldman, B.D.; Ahn, M.; Styner, M.A.; Thompson, A.L.; Geng, X.; Gilmore, J.H.; Knickmeyer, R.C. Infant Gut Microbiome Associated with Cognitive Development. Biol. Psychiatry 2018, 83, 148–159. [Google Scholar] [CrossRef] [PubMed]
- Aatsinki, A.-K.; Lahti, L.; Uusitupa, H.-M.; Munukka, E.; Keskitalo, A.; Nolvi, S.; O’Mahony, S.; Pietilä, S.; Elo, L.L.; Eerola, E.; et al. Gut Microbiota Composition Is Associated with Temperament Traits in Infants. Brain. Behav. Immun. 2019, 80, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Heijtz, R.D.; Wang, S.; Anuar, F.; Qian, Y.; Björkholm, B.; Samuelsson, A.; Hibberd, M.L.; Forssberg, H.; Pettersson, S. Normal Gut Microbiota Modulates Brain Development and Behavior. Proc. Natl. Acad. Sci. USA 2011, 108, 3047–3052. [Google Scholar] [CrossRef] [PubMed]
- Buffington, S.A.; Di Prisco, G.V.; Auchtung, T.A.; Ajami, N.J.; Petrosino, J.F.; Costa-Mattioli, M. Microbial Reconstitution Reverses Maternal Diet-Induced Social and Synaptic Deficits in Offspring. Cell 2016, 165, 1762–1775. [Google Scholar] [CrossRef] [PubMed]
- Dalile, B.; Van Oudenhove, L.; Vervliet, B.; Verbeke, K. The Role of Short-Chain Fatty Acids in Microbiota–Gut–Brain Communication. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 461–478. [Google Scholar] [CrossRef]
- Yoo, D.Y.; Kim, W.; Nam, S.M.; Kim, D.W.; Chung, J.Y.; Choi, S.Y.; Yoon, Y.S.; Won, M.-H.; Hwang, I.K. Synergistic Effects of Sodium Butyrate, a Histone Deacetylase Inhibitor, on Increase of Neurogenesis Induced by Pyridoxine and Increase of Neural Proliferation in the Mouse Dentate Gyrus. Neurochem. Res. 2011, 36, 1850–1857. [Google Scholar] [CrossRef]
- Mirzaei, R.; Bouzari, B.; Hosseini-Fard, S.R.; Mazaheri, M.; Ahmadyousefi, Y.; Abdi, M.; Jalalifar, S.; Karimitabar, Z.; Teimoori, A.; Keyvani, H.; et al. Role of Microbiota-Derived Short-Chain Fatty Acids in Nervous System Disorders. Biomed. Pharmacother. 2021, 139, 111661. [Google Scholar] [CrossRef]
- Tran, S.M.-S.; Hasan Mohajeri, M. The Role of Gut Bacterial Metabolites in Brain Development, Aging and Disease. Nutrients 2021, 13, 732. [Google Scholar] [CrossRef]
- Yang, L.L.; Millischer, V.; Rodin, S.; MacFabe, D.F.; Villaescusa, J.C.; Lavebratt, C. Enteric Short-Chain Fatty Acids Promote Proliferation of Human Neural Progenitor Cells. J. Neurochem. 2020, 154, 635–646. [Google Scholar] [CrossRef]
- Dawson, S.L.; O’Hely, M.; Jacka, F.N.; Ponsonby, A.L.; Symeonides, C.; Loughman, A.; Collier, F.; Moreno-Betancur, M.; Sly, P.; Burgner, D.; et al. Maternal Prenatal Gut Microbiota Composition Predicts Child Behaviour. eBioMedicine 2021, 68, 103400. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Lee-Sarwar, K.; Kelly, R.S.; Lasky-Su, J.A.; Litonjua, A.A.; Weiss, S.T.; Liu, Y.-Y. Identifying the Critical Time Window for the Association of the Early-Life Gut Microbiome and Metabolome with Childhood Neurodevelopment. medRxiv 2022. medRxiv:2021.12.30.21268329. [Google Scholar]
- Cummings, J.H.; Pomare, E.W.; Branch, H.W.J.; Naylor, C.P.E.; MacFarlane, G.T. Short Chain Fatty Acids in Human Large Intestine, Portal, Hepatic and Venous Blood. Gut 1987, 28, 1221–1227. [Google Scholar] [CrossRef] [PubMed]
- Silva, Y.P.; Bernardi, A.; Frozza, R.L. The Role of Short-Chain Fatty Acids from Gut Microbiota in Gut-Brain Communication. Front. Endocrinol. 2020, 11, 25. [Google Scholar] [CrossRef]
- Del Campo-Moreno, R.; Alarcón-Cavero, T.; D’Auria, G.; Delgado-Palacio, S.; Ferrer-Martínez, M. Microbiota En La Salud Humana: Técnicas de Caracterización y Transferencia. Enferm. Infecc. Microbiol. Clin. 2018, 36, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Ziętek, M.; Celewicz, Z.; Szczuko, M. Short-chain Fatty Acids, Maternal Microbiota and Metabolism in Pregnancy. Nutrients 2021, 13, 1244. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Leeds, P.; Chuang, D.-M. The HDAC Inhibitor, Sodium Butyrate, Stimulates Neurogenesis in the Ischemic Brain. J. Neurochem. 2009, 110, 1226–1240. [Google Scholar] [CrossRef]
- Wei, Y.B.; Melas, P.A.; Wegener, G.; Mathe, A.A.; Lavebratt, C. Antidepressant-like Effect of Sodium Butyrate Is Associated with an Increase in Tet1 and in 5-Hydroxymethylation Levels in the BDNF Gene. Int. J. Neuropsychopharmacol. 2015, 18, pyu032. [Google Scholar] [CrossRef]
- Levenson, J.M.; O’Riordan, K.J.; Brown, K.D.; Trinh, M.A.; Molfese, D.L.; Sweatt, J.D. Regulation of Histone Acetylation during Memory Formation in the Hippocampus. J. Biol. Chem. 2004, 279, 40545–40559. [Google Scholar] [CrossRef]
- Hsiao, E.Y.; McBride, S.W.; Hsien, S.; Sharon, G.; Hyde, E.R.; McCue, T.; Codelli, J.A.; Chow, J.; Reisman, S.E.; Petrosino, J.F.; et al. Microbiota Modulate Behavioral and Physiological Abnormalities Associated with Neurodevelopmental Disorders. Cell 2013, 155, 1451–1463. [Google Scholar] [CrossRef]
- Yu, L.; Zhong, X.; He, Y.; Shi, Y. Butyrate, but Not Propionate, Reverses Maternal Diet-Induced Neurocognitive Deficits in Offspring. Pharmacol. Res. 2020, 160, 105082. [Google Scholar] [CrossRef] [PubMed]
- Foley, K.A.; Ossenkopp, K.P.; Kavaliers, M.; MacFabe, D.F. Pre- and Neonatal Exposure to Lipopolysaccharide or the Enteric Metabolite, Propionic Acid, Alters Development and Behavior in Adolescent Rats in a Sexually Dimorphic Manner. PLoS ONE 2014, 9, e87072. [Google Scholar] [CrossRef] [PubMed]
- Foley, K.A.; MacFabe, D.F.; Kavaliers, M.; Ossenkopp, K.P. Sexually Dimorphic Effects of Prenatal Exposure to Lipopolysaccharide, and Prenatal and Postnatal Exposure to Propionic Acid, on Acoustic Startle Response and Prepulse Inhibition in Adolescent Rats: Relevance to Autism Spectrum Disorders. Behav. Brain Res. 2015, 278, 244–256. [Google Scholar] [CrossRef] [PubMed]
- Nankova, B.B.; Agarwal, R.; MacFabe, D.F.; La Gamma, E.F. Enteric Bacterial Metabolites Propionic and Butyric Acid Modulate Gene Expression, Including CREB-Dependent Catecholaminergic Neurotransmission, in PC12 Cells—Possible Relevance to Autism Spectrum Disorders. PLoS ONE 2014, 9, e103740. [Google Scholar] [CrossRef]
- Arija, V.; Fargas, F.; March, G.; Abajo, S.; Basora, J.; Canals, J.; Ribot, B.; Aparicio, E.; Serrat, N.; Hernández-Martínez, C.; et al. Adapting Iron Dose Supplementation in Pregnancy for Greater Effectiveness on Mother and Child Health: Protocol of the ECLIPSES Randomized Clinical Trial. BMC Pregnancy Childbirth 2014, 14, 33. [Google Scholar] [CrossRef]
- Iglesias, L.; Arija, V.; Aranda, N.; Aparicio, E.; Serrat, N.; Fargas, F.; Ruiz, F.; Pallejà, M.; Coronel, P.; Gimeno, M.; et al. The Effectiveness of Different Doses of Iron Supplementation and the Prenatal Determinants of Maternal Iron Status in Pregnant Spanish Women: ECLIPSES Study. Nutrients 2019, 11, 2418. [Google Scholar] [CrossRef]
- Zeng, M.; Cao, H. Fast Quantification of Short Chain Fatty Acids and Ketone Bodies by Liquid Chromatography-Tandem Mass Spectrometry after Facile Derivatization Coupled with Liquid-Liquid Extraction. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2018, 1083, 137–145. [Google Scholar] [CrossRef]
- Martín-Grau, C.; Díaz-López, A.; Aparicio, E.; Arija, V. Short-Chain Fatty Acid Reference Ranges in Pregnant Women from a Mediterranean Region of Northern Spain. ECLIPSES Study. Nutrients 2022, 14, 3798. [Google Scholar] [CrossRef]
- Bayley, N. Bayley Scales for Infant Development—Third Edition; Psychological Corporation: San Antonio, TX, USA, 2006. [Google Scholar]
- Medoff-Cooper, B.; Carey, W.B.; McDevitt, S.C. The Early Infancy Temperament Questionnaire. J. Dev. Behav. Pediatr. 1993, 14, 230–235. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Trinidad, I.; Fernández-Ballart, J.; Cucó, G.; Biarnés, E.; Arija, V. Validación de Un Cuestionario de Frecuencia de Consumo Alimentario Corto: Reproducibilidad y Validez. Nutr. Hosp. 2008, 23, 242–252, ISSN 0212-1611. [Google Scholar]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.E. STAI Cuestionario de Ansiedad Estado Rasgo; TEA Ediciones: Madrid, Spain, 1997. [Google Scholar]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerström, K.O. The Fagerström Test for Nicotine Dependence: A Revision of the Fagerstrom Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Hollingshead, A. Four Factor Index of Social Status. Yale J. Sociol. 2011, 8, 21–52. [Google Scholar]
- Institut Nacional d’Estadística. Classificació Catalana d’Ocupacions (CCO-2011); Generalitat de Catalunya: Barcelona, Brazil, 2011.
- Abidin, R. Parenting Stress Index, 2nd ed.; Psychological Assessment Resources: Odessa, FL, USA, 1995. [Google Scholar]
- Nuriel-Ohayon, M.; Neuman, H.; Koren, O. Microbial Changes during Pregnancy, Birth, and Infancy. Front. Microbiol. 2016, 7, 1031. [Google Scholar] [CrossRef]
- MacFabe, D.F. Enteric Short-Chain Fatty Acids: Microbial Messengers of Metabolism, Mitochondria, and Mind: Implications in Autism Spectrum Disorders. Microb. Ecol. Health Dis. 2015, 26, 28177. [Google Scholar] [CrossRef] [PubMed]
- Serino, M. SCFAs—The Thin Microbial Metabolic Line between Good and Bad. Nat. Rev. Endocrinol. 2019, 15, 318–319. [Google Scholar] [CrossRef]
- Huang, Y.; Gao, S.; Chen, J.; Albrecht, E.; Zhao, R.; Yang, X. Maternal Butyrate Supplementation Induces Insulin Resistance Associated with Enhanced Intramuscular Fat Deposition in the Offspring. Oncotarget 2017, 8, 13073–13084. [Google Scholar] [CrossRef]
- Georgieff, M.K.; Ramel, S.E.; Cusick, S.E. Nutritional Influences on Brain Development. Acta Paediatr. Int. J. Paediatr. 2018, 107, 1310–1321. [Google Scholar] [CrossRef]
- Stinson, L.F.; Boyce, M.C.; Payne, M.S.; Keelan, J.A. The Not-so-Sterile Womb: Evidence That the Human Fetus Is Exposed to Bacteria Prior to Birth. Front. Microbiol. 2019, 10, 1124. [Google Scholar] [CrossRef]
- Orczyk-Pawilowicz, M.; Jawien, E.; Deja, S.; Hirnle, L.; Zabek, A.; Mlynarz, P. Metabolomics of Human Amniotic Fluid and Maternal Plasma during Normal Pregnancy. PLoS ONE 2016, 11, e0152740. [Google Scholar] [CrossRef]
- Cucó, G.; Fernandez-Ballart, J.; Arija, V.; Canals, J. Effect of B1-, B6- and Iron Intake during Pregnancy on Neonatal Behavior. Int. J. Vitam. Nutr. Res. 2005, 75, 320–326. [Google Scholar] [CrossRef]
- Vecchione, R.; Vigna, C.; Whitman, C.; Kauffman, E.M.; Braun, J.M.; Chen, A.; Xu, Y.; Hamra, G.B.; Lanphear, B.P.; Yolton, K.; et al. The Association Between Maternal Prenatal Fish Intake and Child Autism-Related Traits in the EARLI and HOME Studies. J. Autism Dev. Disord. 2021, 51, 487–500. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.; Reichenberg, A.; Kolevzon, A. Prenatal and Perinatal Metabolic Risk Factors for Autism: A Review and Integration of Findings from Population-Based Studies. Curr. Opin. Psychiatry 2021, 34, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Roigé-Castellví, J.; Morales-Hidalgo, P.; Voltas, N.; Hernández-Martínez, C.; van Ginkel, G.; Canals, J. Prenatal and Perinatal Factors Associated with ADHD Risk in Schoolchildren: EPINED Epidemiological Study. Eur. Child Adolesc. Psychiatry 2021, 30, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Davis, A.M. Collateral Damage: Maternal Obesity During Pregnancy Continues to Rise. Obstet. Gynecol. Surv. 2020, 75, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Li, X.; Xia, B.; Jin, X.; Zou, Q.; Zeng, Z.; Zhao, W.; Yan, S.; Li, L.; Yuan, S.; et al. High-Fiber Diet Mitigates Maternal Obesity-Induced Cognitive and Social Dysfunction in the Offspring via Gut-Brain Axis. Cell Metab. 2021, 33, 923–938.e6. [Google Scholar] [CrossRef] [PubMed]
- Priyadarshini, M.; Thomas, A.; Alexandra, A.C.; Scholtens, D.M.; Wolever, T.M.S.; Josefson, J.L.; Layden, B.T. Maternal Short-Chain Fatty Acids Are Associated with Metabolic Parameters in Mothers and Newborns. Transl Res. 2015, 164, 153–157. [Google Scholar] [CrossRef]
- Aubuchon-Endsley, N.; Morales, M.; Giudice, C.; Bublitz, M.H.; Lester, B.M.; Salisbury, A.L.; Stroud, L.R. Maternal Pre-Pregnancy Obesity and Gestational Weight Gain Influence Neonatal Neurobehaviour. Matern. Child Nutr. 2016, 1, e12317. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 12 Weeks of Gestation | 36 Weeks of Gestation | Partum | 40 Days Postpartum | |
|---|---|---|---|---|
| Participants | 450 | 450 | 450 | 357 |
| Individual assessment |
| |||
| Medical records |
|
|
|
|
| Questionnaires |
|
|
| |
| Blood samples |
|
| ||
| Family Interview |
|
| Mean (SD) * n(%) # | |
| Mother’s age (years) | 30.6 (5.1) * |
| Family’s socioeconomic status | |
| Low | 84 (16.8) # |
| Medium | 323 (64.7) # |
| High | 92 (18.4) # |
| Mother smoking during pregnancy (no) | 428 (85.8) # |
| Quality of diet (total score) | |
| 1st trimester | 9.6 (2.7) |
| 3rd trimester | 9.9 (2.6) |
| Paired T (p) | 1.953 (0.051) |
| State anxiety (total score) | |
| 1st trimester | 17.3 (8.0) |
| 3rd trimester | 19.0 (7.7) |
| Paired T (p) | −5.164 (<0.001) |
| Infant sex (girls)# | 251 (50.5) # |
| Mode of delivery (non-instrumental) | 340 (66.9) # |
| Gestational age (weeks) | 39.70 (1.4) * |
| Birth weight (gr) | 3278.3 (460.9) |
| Infant feeding (breastfeeding) | 407 (81.9) # |
| Mother–infant bonding (total score) | 17.32 (7.9) * |
| Bayley Scales Infant Development | Mean (SD) |
| Cognitive scale (total score) | 101.8 (8.8) * |
| Language scale (total score) | 96.4 (8.4) * |
| Receptive (total score) | 10.6 (2.1) * |
| Expressive (total score) | 8.1 (1.6) * |
| Motor scale (total score) | 107.9 (11.2) * |
| Fine (total score) | 11.5 (1.9) * |
| Gross (total score) | 11.1 (2.3) * |
| Early Infant Temperament Questionnaire | Mean (SD) |
| Activity level (total score) | 3.2 (0.7) * |
| Rhythmicity (total score) | 3.3 (0.8) * |
| Approach (total score) | 2.6 (0.7) * |
| Adaptability (total score) | 2.6 (0.7) * |
| Intensity (total score) | 3.3 (0.9) * |
| Mood (total score) | 3.0 (0.7) * |
| Persistence (total score) | 3.0 (0.8) * |
| Distractibility (total score) | 2.6 (0.8) * |
| Threshold (total score) | 4.1 (0.7) * |
| First Trimester | Third Trimester | Paired T (p) * | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Low-Tertile Mean (SD) | Medium-Tertile Mean (SD) | High-Tertile Mean (SD) | Total Sample * Mean (SD) | Low-Tertile Mean (SD) | Medium-Tertile Mean (SD) | High-Tertile Mean (SD) | Total Sample * Mean (SD) | ||
| Acetic acid | 30.9 (7.7) | 45.7 (3.6) | 70.1 (22.5) | 49.1 (21.4) | 32.5 (5.7) | 45.2 (3.1) | 67.4 (18.1) | 48.5 (18.3) | 0.439 (0.661) |
| Propionic acid | 2.7 (0.3) | 3.5 (0.2) | 4.5 (0.6) | 3.6 (0.9) | 2.6 (0.3) | 3.3 (0.2) | 4.6 (0.9) | 3.5 (1.0) | 0.385 (0.701) |
| Butyric acid | 0.5 (0.1) | 0.7 (0.1) | 1.2 (0.3) | 0.8 (0.3) | 0.5 (0.1) | 0.8 (0.1) | 1.4 (0.4) | 0.9 (0.4) | −5.080 (<0.001) |
| Isobutyric acid | 0.3 (0.1) | 0.5 (0.1) | 0.7 (0.2) | 0.5 (0.2) | 0.3 (0.1) | 0.4 (0.1) | 0.7 (0.3) | 0.4 (0.2) | 1.635 (0.103) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Martínez, C.; Canals, J.; Voltas, N.; Martín-Luján, F.; Arija, V. Circulating Levels of Short-Chain Fatty Acids during Pregnancy and Infant Neurodevelopment. Nutrients 2022, 14, 3946. https://doi.org/10.3390/nu14193946
Hernández-Martínez C, Canals J, Voltas N, Martín-Luján F, Arija V. Circulating Levels of Short-Chain Fatty Acids during Pregnancy and Infant Neurodevelopment. Nutrients. 2022; 14(19):3946. https://doi.org/10.3390/nu14193946
Chicago/Turabian StyleHernández-Martínez, Carmen, Josefa Canals, Núria Voltas, Francisco Martín-Luján, and Victoria Arija. 2022. "Circulating Levels of Short-Chain Fatty Acids during Pregnancy and Infant Neurodevelopment" Nutrients 14, no. 19: 3946. https://doi.org/10.3390/nu14193946