
Association of Coffee and Tea Consumption with the Risk of Asthma: A Prospective Cohort Study from the UK Biobank
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Exposure Assessment
2.3. Ascertainment of Asthma
2.4. Covariates
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics
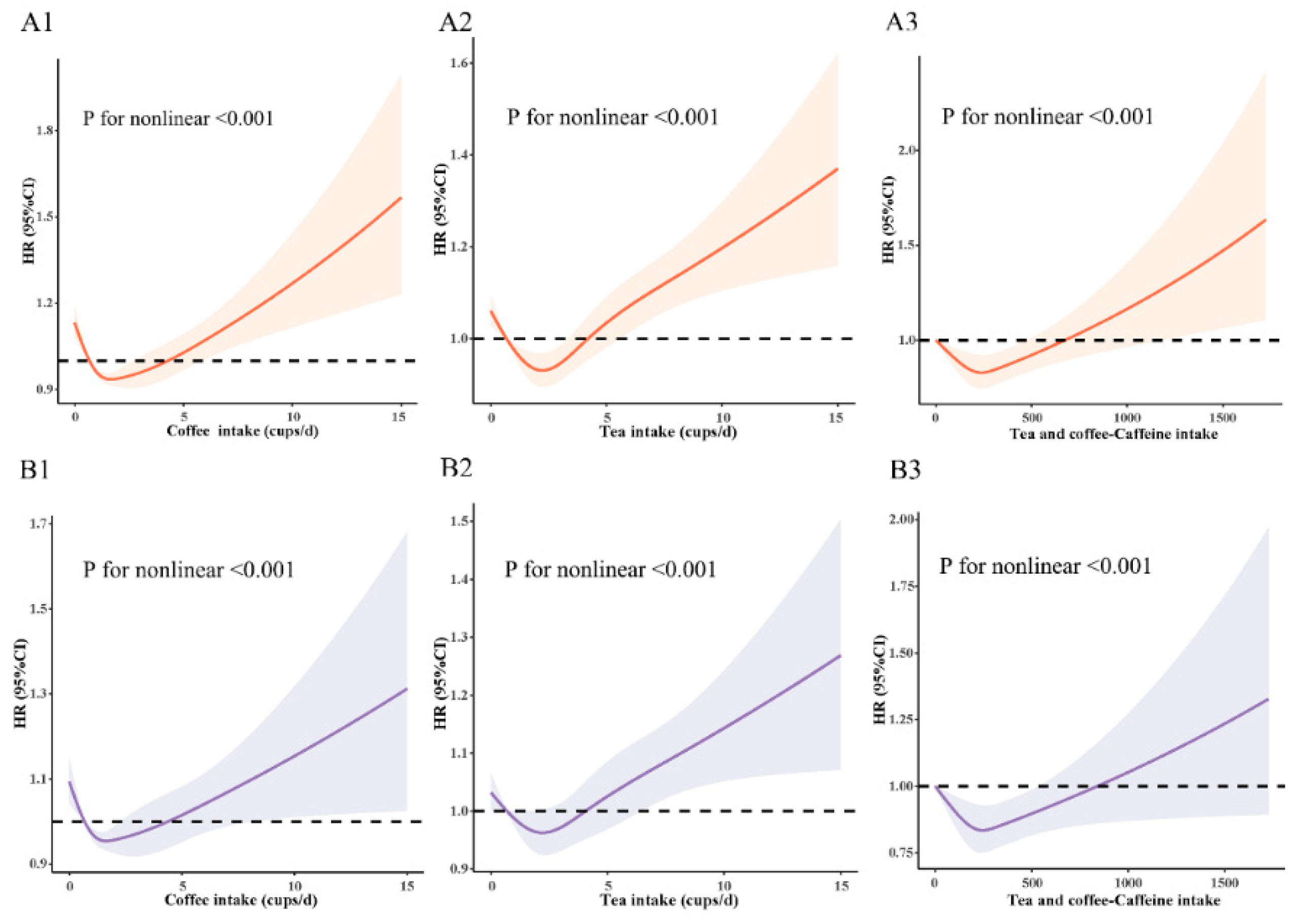
3.2. Nonlinear Association
3.3. Coffee Intake, Tea Intake, and Combined Caffeine Intake with Asthma Risk
3.4. Subgroup and Sensitivity Analyses
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| A | Advanced |
| AS | Advanced Subsidiary |
| BMI | body mass index (calculated as weight in kilograms divided by height in meters squared) |
| CI | confidence interval |
| CSE | Certificate of Secondary Education |
| GCSE | General Certificate of Secondary Education |
| HR | hazard ratio |
| HNC | Higher National Certificate |
| HND | Higher National Diploma |
| ICD-10 | International Classification of Diseases-10th revision |
| NVQ | National Vocational Qualification |
| O | Ordinary |
| Q | quartiles |
| SD | standard deviation |
| UK Biobank | United Kingdom Biobank |
References
- Global Asthma Network. The Global Asthma Report 2018; Global Asthma Network: Auckland, New Zealand, 2018. [Google Scholar]
- Soriano, J.B.; Kendrick, P.J.; Paulson, K.R.; Gupta, V.; Abrams, E.M.; Adedoyin, R.A.; Adhikari, T.B.; Advani, S.M.; Agrawal, A.; Ahmadian, E.; et al. Collaborators GBDCRD: Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2020, 8, 585–596. [Google Scholar] [CrossRef]
- Paiva, I.; Cellai, L.; Meriaux, C.; Poncelet, L.; Nebie, O.; Saliou, J.M.; Lacoste, A.S.; Papegaey, A.; Drobecq, H.; Le Gras, S.; et al. Caffeine intake exerts dual genome-wide effects on hippocampal metabolism and learning-dependent transcription. J. Clin. Investig. 2022, 132, e149371. [Google Scholar] [CrossRef] [PubMed]
- Poole, R.; Kennedy, O.J.; Roderick, P.; Fallowfield, J.A.; Hayes, P.C.; Parkes, J. Coffee consumption and health: Umbrella review of meta-analyses of multiple health outcomes. BMJ 2017, 359, j5024. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Micek, A.; Godos, J.; Sciacca, S.; Pajak, A.; Martinez-Gonzalez, M.A.; Giovannucci, E.L.; Galvano, F. Coffee consumption and risk of all-cause, cardiovascular, and cancer mortality in smokers and non-smokers: A dose-response meta-analysis. Eur. J. Epidemiol. 2016, 31, 1191–1205. [Google Scholar] [CrossRef]
- Ding, M.; Bhupathiraju, S.N.; Chen, M.; van Dam, R.M.; Hu, F.B. Caffeinated and decaffeinated coffee consumption and risk of type 2 diabetes: A systematic review and a dose-response meta-analysis. Diabetes Care 2014, 37, 569–586. [Google Scholar] [CrossRef]
- Zhang, Y.; Yang, H.; Li, S.; Li, W.D.; Wang, Y. Consumption of coffee and tea and risk of developing stroke, dementia, and poststroke dementia: A cohort study in the UK Biobank. PLoS Med. 2021, 18, e1003830. [Google Scholar] [CrossRef]
- Qi, H.; Li, S. Dose–response meta-analysis on coffee, tea and caffeine consumption with risk of P arkinson’s disease. Geriatr. Gerontol. Int. 2014, 14, 430–439. [Google Scholar] [CrossRef]
- Nordestgaard, A.T. Causal relationship from coffee consumption to diseases and mortality: A review of observational and Mendelian randomization studies including cardiometabolic diseases, cancer, gallstones and other diseases. Eur. J. Nutr. 2022, 61, 573–587. [Google Scholar] [CrossRef]
- Tang, G.Y.; Meng, X.; Gan, R.Y.; Zhao, C.N.; Liu, Q.; Feng, Y.B.; Li, S.; Wei, X.L.; Atanasov, A.G.; Corke, H.; et al. Health functions and related molecular mechanisms of tea components: An update review. Int. J. Mol. Sci. 2019, 20, 6196. [Google Scholar] [CrossRef]
- Pagano, R.; Negri, E.; Decarli, A.; La Vecchia, C. Coffee drinking and prevalence of bronchial asthma. Chest 1988, 94, 386–389. [Google Scholar] [CrossRef]
- Wee, J.H.; Yoo, D.M.; Byun, S.H.; Song, C.M.; Lee, H.J.; Park, B.; Park, M.W.; Choi, H.G. Analysis of the relationship between asthma and coffee/green tea/soda intake. Int. J. Environ. Res. Public Health 2020, 17, 7471. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.; Weiss, S.T. Caffeine intake and asthma symptoms. Ann. Epidemiol. 1992, 2, 627–635. [Google Scholar] [CrossRef]
- Annesi, I.; Kauffmann, F.; Oryszczyn, M.P.; Neukirch, F.; Dore, M.F. Coffee drinking and prevalence of bronchial asthma. Chest 1990, 97, 1268–1269. [Google Scholar] [CrossRef] [PubMed]
- Alfaro, T.M.; Monteiro, R.A.; Cunha, R.A.; Cordeiro, C.R. Chronic coffee consumption and respiratory disease: A systematic review. Clin. Respir. J. 2018, 12, 1283–1294. [Google Scholar] [CrossRef]
- Hayakawa, S.; Ohishi, T.; Miyoshi, N.; Oishi, Y.; Nakamura, Y.; Isemura, M. Anti-cancer effects of green tea epigallocatchin-3-gallate and coffee chlorogenic acid. Molecules 2020, 25, 4553. [Google Scholar] [CrossRef]
- Yashima, M.; Sato, Y.; Kazama, I. Catechin synergistically potentiates mast cell-stabilizing property of caffeine. Allergy Asthma Clin. Immunol. 2021, 17, 1–7. [Google Scholar] [CrossRef]
- Croft, K.D. The chemistry and biological effects of flavonoids and phenolic acids. Ann. N. Y. Acad. Sci. 1998, 854, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Gong, H., Jr.; Simmons, M.S.; Tashkin, D.P.; Hui, K.K.; Lee, E.Y. Bronchodilator effects of caffeine in coffee. A dose-response study of asthmatic subjects. Chest 1986, 89, 335–342. [Google Scholar] [CrossRef]
- Banner, K.H.; Page, C.P. Theophylline and selective phosphodiesterase inhibitors as anti-inflammatory drugs in the treatment of bronchial asthma. Eur. Respir. J. 1995, 8, 996–1000. [Google Scholar]
- Bloom, C.I.; de Preux, L.; Sheikh, A.; Quint, J.K. Health and cost impact of stepping down asthma medication for UK patients, 2001-2017: A population-based observational study. PLoS Med. 2020, 17, e1003145. [Google Scholar] [CrossRef]
- Cox, N. UK Biobank shares the promise of big data. Nature 2018, 562, 194–195. [Google Scholar] [CrossRef] [Green Version]
- Sudlow, C.; Gallacher, J.; Allen, N.; Beral, V.; Burton, P.; Danesh, J.; Downey, P.; Elliott, P.; Green, J.; Landray, M.; et al. UK biobank: An open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 2015, 12, e1001779. [Google Scholar] [CrossRef] [PubMed]
- Orazi, C.; Fariello, G.; Malena, S.; Caterino, S.; Ferro, F. Torsion of paradidymis or Giraldes’ organ: An uncommon cause of acute scrotum in pediatric age group. J. Clin. Ultrasound 1989, 17, 598–601. [Google Scholar] [CrossRef] [PubMed]
- Zhou, A.; Hyppönen, E. Long-term coffee consumption, caffeine metabolism genetics, and risk of cardiovascular disease: A prospective analysis of up to 347,077 individuals and 8368 cases. Am. J. Clin. Nutr. 2019, 109, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Cornelis, M.C.; Weintraub, S.; Morris, M.C. Caffeinated Coffee and Tea Consumption, Genetic Variation and Cognitive Function in the UK Biobank. J. Nutr. 2020, 150, 2164–2174. [Google Scholar] [CrossRef]
- Liu, D.; Li, Z.H.; Shen, D.; Zhang, P.D.; Song, W.Q.; Zhang, W.T.; Huang, Q.M.; Chen, P.L.; Zhang, X.R.; Mao, C. Association of sugar-sweetened, artificially sweetened, and unsweetened coffee consumption with all-cause and cause-specific mortality: A large prospective cohort study. Ann. Intern. Med. 2022, 175, 909–917. [Google Scholar] [CrossRef]
- Welsh, E.J.; Bara, A.; Barley, E.; Cates, C.J. Caffeine for asthma. Cochrane Database Syst. Rev. 2010, 2010, CD001112. [Google Scholar] [CrossRef]
- Ruiz-Moreno, C.; Lara, B.; Brito de Souza, D.; Gutierrez-Hellin, J.; Romero-Moraleda, B.; Cuellar-Rayo, A.; Del Coso, J. Acute caffeine intake increases muscle oxygen saturation during a maximal incremental exercise test. Br. J. Clin. Pharmacol. 2020, 86, 861–867. [Google Scholar] [CrossRef]
- Musgrave, I.F.; Farrington, R.L.; Hoban, C.; Byard, R.W. Caffeine toxicity in forensic practice: Possible effects and under-appreciated sources. Forensic Sci. Med. Pathol. 2016, 12, 299–303. [Google Scholar] [CrossRef]
- Wikoff, D.; Welsh, B.T.; Henderson, R.; Brorby, G.P.; Britt, J.; Myers, E.; Goldberger, J.; Lieberman, H.R.; O’Brien, C.; Peck, J.; et al. Systematic review of the potential adverse effects of caffeine consumption in healthy adults, pregnant women, adolescents, and children. Food Chem. Toxicol. 2017, 109 Pt 1, 585–648. [Google Scholar] [CrossRef]
- Verster, J.C.; Koenig, J. Caffeine intake and its sources: A review of national representative studies. Crit. Rev. Food Sci. Nutr. 2018, 58, 1250–1259. [Google Scholar] [CrossRef]
- Rodak, K.; Kokot, I.; Kratz, E.M. Caffeine as a Factor Influencing the Functioning of the Human Body-Friend or Foe? Nutrients 2021, 13, 3088. [Google Scholar] [CrossRef]
- Wu, W.; Tong, Y.; Zhao, Q.; Yu, G.; Wei, X.; Lu, Q. Coffee consumption and bladder cancer: A meta-analysis of observational studies. Sci. Rep. 2015, 5, 9051. [Google Scholar] [CrossRef]
- Dunn, R.M.; Busse, P.J.; Wechsler, M.E. Asthma in the elderly and late-onset adult asthma. Allergy 2018, 73, 284–294. [Google Scholar] [CrossRef]
- Shadyab, A.H.; Manson, J.E.; Luo, J.; Haring, B.; Saquib, N.; Snetselaar, L.G.; Chen, J.C.; Groessl, E.J.; Wassertheil-Smoller, S.; Sun, Y.; et al. Associations of coffee and tea consumption with survival to age 90 years among older women. J. Am. Geriatr. Soc. 2020, 68, 1970–1978. [Google Scholar] [CrossRef]
- Dharmage, S.C.; Perret, J.L.; Custovic, A. Epidemiology of asthma in children and adults. Front. Pediatr. 2019, 7, 246. [Google Scholar] [CrossRef]
- Nwaru, B.I.; Ohlsson, C.; Bygdell, M.; Martikainen, J.; Kindblom, J.M. Pubertal BMI change and adult-onset asthma in men: Population-based cohort study in Sweden. Clin. Exp. Allergy 2020, 50, 51–60. [Google Scholar] [CrossRef]
- Guerra, S.; Wright, A.L.; Morgan, W.J.; Sherrill, D.L.; Holberg, C.J.; Martinez, F.D. Persistence of asthma symptoms during adolescence: Role of obesity and age at the onset of puberty. Am. J. Respir. Crit. Care Med. 2004, 170, 78–85. [Google Scholar] [CrossRef]
- Coogan, P.F.; Castro-Webb, N.; Yu, J.; O’Connor, G.T.; Palmer, J.R.; Rosenberg, L. Active and passive smoking and the incidence of asthma in the Black Women’s Health Study. Am. J. Respir. Crit. Care Med. 2015, 191, 168–176. [Google Scholar] [CrossRef]
- Jabre, N.A.; Keet, C.A.; McCormack, M.; Peng, R.; Balcer-Whaley, S.; Matsui, E.C. Material Hardship and Indoor Allergen Exposure among Low-Income, Urban, Minority Children with Persistent Asthma. J. Community Health 2020, 45, 1017–1026. [Google Scholar] [CrossRef]
- Zhu, Y.; Jing, D.; Liang, H.; Li, D.; Chang, Q.; Shen, M.; Pan, P.; Liu, H.; Zhang, Y. Vitamin D status and asthma, lung function, and hospitalization among British adults. Front. Nutr. 2022, 9, 954768. [Google Scholar] [CrossRef] [PubMed]
- Loftfield, E.; Freedman, N.D.; Dodd, K.W.; Vogtmann, E.; Xiao, Q.; Sinha, R.; Graubard, B.I. Coffee Drinking Is Widespread in the United States, but Usual Intake Varies by Key Demographic and Lifestyle Factors. J. Nutr. 2016, 146, 1762–1768. [Google Scholar] [CrossRef] [PubMed]
- Vieux, F.; Maillot, M.; Rehm, C.D.; Drewnowski, A. Tea Consumption Patterns in Relation to Diet Quality among Children and Adults in the United States: Analyses of NHANES 2011–2016 Data. Nutrients 2019, 11, 2635. [Google Scholar] [CrossRef] [PubMed]
- Creed, J.H.; Smith-Warner, S.A.; Gerke, T.A.; Egan, K.M. A prospective study of coffee and tea consumption and the risk of glioma in the UK Biobank. Eur. J. Cancer 2020, 129, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, C.R.; Giles, G.E.; Marriott, B.P.; Judelson, D.A.; Glickman, E.L.; Geiselman, P.J.; Lieberman, H.R. Intake of caffeine from all sources and reasons for use by college students. Clin. Nutr. 2019, 38, 668–675. [Google Scholar] [CrossRef]
- Heckman, M.A.; Weil, J.; Gonzalez de Mejia, E. Caffeine (1,3,7-trimethylxanthine) in foods: A comprehensive review on consumption, functionality, safety, and regulatory matters. J. Food Sci. 2010, 75, R77–R87. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Coffee Intake, cups/day, No. (%) | Tea Intake, cups/day, No. (%) | Caffeine Intake, mg/day, No. (%) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | All Participants | 0 | 0.5 to 1 | 2 to 3 | ≥4 | 0 | 0.5 to 1 | 2 to 3 | ≥4 | Q1(≤160.0) | Q2 (160.0–235.0) | Q3 (235.0–305.0) | Q4 (305.0–390.0) | Q5 (≥390.0) |
| Total number, No. (%) | 424,725 | 93,503 (22.0) | 115,909 (27.3) | 132,751 (31.3) | 82,562 (19.4) | 61,993 (14.6) | 48,852 (11.5) | 125,407 (29.5) | 188,473 (44.4) | 93,308 (22.0) | 84,391 (19.9) | 81,117 (19.1) | 86,317 (20.3) | 79,592 (18.7) |
| Asthma cases, No. (%) | 8680 (2.0) | 2130 (2.3) | 2305 (2.0) | 2476 (1.9) | 1769 (2.1) | 1371 (2.2) | 889 (1.8) | 2417 (1.9) | 4003 (2.1) | 1991 (2.1) | 1602 (1.9) | 1597 (2.0) | 1764 (2.0) | 1757 (2.2) |
| Age, mean (SD), y | 56.61 (8.06) | 55.52 (8.21) | 57.09 (8.02) | 57.16 (7.97) | 56.30 (7.95) | 55.52 (8.22) | 55.60 (8.32) | 56.75 (8.10) | 57.14 (7.85) | 55.29 (8.39) | 57.00 (8.10) | 57.11 (7.90) | 57.34 (7.79) | 56.45 (7.88) |
| Gender | ||||||||||||||
| Male, n (%) | 195,568 (46.0) | 39,726 (42.5) | 50,681 (43.7) | 62,304 (46.9) | 42,857 (51.9) | 27,370 (44.2) | 23,580 (48.3) | 57,911 (46.2) | 86,707 (46.0) | 39,342 (42.2) | 37,471 (44.4) | 36,365 (44.8) | 40,319 (46.7) | 42,071 (52.9) |
| Female, n (%) | 229,157 (54.0) | 53,777 (57.5) | 65,228 (56.3) | 70,712 (53.1) | 39,705 (48.1) | 34,623 (55.8) | 25,272 (51.7) | 67,496 (53.8) | 101,766 (54.0) | 53,966 (57.8) | 46,920 (55.6) | 44,725 (55.2) | 45,998 (53.3) | 37,521 (47.1) |
| Race | ||||||||||||||
| White, n (%) | 385,709 (90.8) | 82,724 (88.5) | 104,622 (90.3) | 121,406 (91.5) | 76,957 (93.2) | 56,422 (91.0) | 42,401 (86.8) | 112,582 (89.8) | 174,304 (92.5) | 79,931 (85.7) | 76,349 (90.5) | 74,983 (92.4) | 80,425 (93.2) | 74,021 (93.0) |
| Non-white, n (%) | 39,016 (9.2) | 10,779 (11.5) | 11,287 (9.7) | 11,345 (8.5) | 5605 (6.8) | 5571 (9.0) | 6451 (13.2) | 12,825 (10.2) | 14,169 (7.5) | 13,377 (14.3) | 8042 (9.5) | 6134 (7.6) | 5892 (6.8) | 5571 (7.0) |
| Coffee intake, mean (SD) | 2.02 (2.07) | 0 (0) | 0.87 (0.22) | 2.39 (0.49) | 5.30 (2.03) | 3.47 (2.77) | 2.78 (2.11) | 1.97 (1.67) | 1.37 (1.69) | 0.50 (0.63) | 1.33 (0.91) | 1.70 (1.37) | 2.42 (1.39) | 4.42 (2.88) |
| Tea intake, mean (SD) | 3.42 (2.86) | 4.52 (3.29) | 4.03 (2.59) | 2.97 (2.36) | 2.03 (2.72) | 0 (0) | 0.87 (0.22) | 2.51 (0.50) | 5.81 (2.54) | 1.80 (1.40) | 2.81 (1.60) | 3.60 (2.23) | 4.11 (2.33) | 5.02 (4.59) |
| Smoking status | ||||||||||||||
| Never, n (%) | 232,699 (54.8) | 55,079 (58.9) | 67,175 (58.0) | 72,692 (54.8) | 37,753 (45.7) | 32,324 (52.1) | 26,598 (54.4) | 71,033 (56.6) | 102,744 (54.5) | 57,178 (61.3) | 47,934 (56.8) | 45,268 (55.8) | 46,339 (53.7) | 35,980 (45.2) |
| Previous, n (%) | 147,129 (34.6) | 29,361 (31.4) | 40,004 (34.5) | 47,618 (35.9) | 30,146 (36.5) | 21,078 (34.0) | 16,857 (34.5) | 43,786 (34.9) | 65,408 (34.7) | 29,346 (31.5) | 30,054 (35.3) | 28,649 (35.3) | 30,854 (35.7) | 28,226 (35.5) |
| Current, n (%) | 44,897 (10.6) | 9063 (9.7) | 8730 (7.5) | 12,441 (9.4) | 14,663 (17.8) | 8591 (13.9) | 5397 (11.0) | 10,588 (8.4) | 20,321 (10.8) | 6784 (7.3) | 6403 (7.6) | 7200 (8.9) | 9124 (10.6) | 15,386 (19.3) |
| Body mass index, mean (SD) | 27.31 (4.69) | 27.37 (4.90) | 26.96 (4.60) | 27.19 (4.53) | 27.92 (4.76) | 27.97 (5.16) | 27.32 (4.78) | 27.10 (4.57) | 27.23 (4.56) | 27.26 (4.99) | 27.07 (4.61) | 27.20 (4.57) | 27.31 (4.50) | 27.74 (4.70) |
| BMI category, n (%) | ||||||||||||||
| <25 | 142,884 (33.6) | 31,945 (34.2) | 42,783 (36.9) | 45,142 (34.0) | 23,014 (27.9) | 18,738 (30.2) | 16,653 (34.1) | 44,083 (35.2) | 63,410 (33.6) | 33,631 (36.0) | 30,291 (35.9) | 27,604 (34.0) | 28,125 (32.6) | 23,233 (29.2) |
| 25 to <30 | 181,689 (42.8) | 38,480 (41.1) | 48,638 (42.0) | 57,957 (43.7) | 36,614 (44.3) | 25,301 (40.8) | 20,541 (42.0) | 53,782 (42.9) | 82,065 (43.5) | 37,265 (39.9) | 35,643 (42.2) | 35,294 (43.5) | 38,153 (44.2) | 35,334 (44.4) |
| ≥30 | 100,152 (23.6) | 23,078 (24.7) | 24,488 (21.1) | 29,652 (22.3) | 22,934 (27.8) | 17,954 (29.0) | 11,658 (23.9) | 27,542 (22.0) | 42,998 (22.8) | 22,412 (24.0) | 18,457 (21.9) | 18,219 (22.5) | 20,039 (23.2) | 21,025 (26.4) |
| Education | ||||||||||||||
| College or University Degree | 137,939 (32.5) | 25,112 (26.9) | 39,162 (33.8) | 47,804 (36.0) | 25,861 (31.3) | 18,838 (30.4) | 19,577 (40.1) | 43,705 (34.9) | 55,819 (29.6) | 30,410 (32.6) | 28,631 (33.9) | 26,548 (32.7) | 28,291 (32.8) | 24,059 (30.2) |
| Professional Qualifications | 50,080 (11.8) | 11,371 (12.2) | 13,369 (11.5) | 15,054 (11.3) | 10,286 (12.5) | 7296 (11.8) | 4937 (10.1) | 14,061 (11.2) | 23,786 (12.6) | 10,226 (11.0) | 9514 (11.3) | 9531 (11.7) | 10,631 (12.3) | 10,178 (12.8) |
| A Levels/AS Levels or Equivalent | 475,04 (11.2) | 9799 (10.5) | 13,452 (11.6) | 15,247 (11.5) | 9006 (10.9) | 7185 (11.6) | 6121 (12.5) | 14,241 (11.4) | 19,957 (10.6) | 10,820 (11.6) | 9583 (11.4) | 9207 (11.4) | 9460 (11.0) | 8434 (10.6) |
| O Levels/GCSEs or Equivalent | 113,778 (26.8) | 26,311 (28.1) | 30,201 (26.1) | 34,284 (25.8) | 22,982 (27.8) | 17,969 (29.0) | 12,180 (24.9) | 33,093 (26.4) | 50,535 (26.8) | 25,308 (27.1) | 22,378 (26.5) | 21,653 (26.7) | 22,911 (26.5) | 21,527 (27.0) |
| None of the above | 75,424 (17.8) | 20,910 (22.4) | 19,725 (17.0) | 20,362 (15.3) | 14,427 (1.7) | 10,704 (17.3) | 6036 (12.4) | 20,307 (16.2) | 38,376 (20.4) | 16,544 (17.7) | 14,285 (16.9) | 14,178 (17.5) | 15,024 (17.4) | 15,393 (19.3) |
| Townsend deprivation, mean (SD) | −1.36 (3.06) | −0.92 (3.25) | −1.45 (3.01) | −1.58 (2.95) | −1.40 (3.02) | −1.14 (3.15) | −1.19 (3.14) | −1.42 (3.04) | −1.44 (3.01) | −0.90 (3.27) | −1.45 (3.00) | −1.58 (2.92) | −1.64 (2.90) | −1.29 (3.09) |
| Townsend deprivation index quartiles | ||||||||||||||
| Q1 (lowest) | 106,212 (25.0) | 20,129 (21.5) | 29,759 (25.7) | 35,562 (26.8) | 20,762 (25.1) | 14,232 (23.0) | 11,680 (23.9) | 32,385 (25.8) | 47,915 (25.4) | 20,285 (21.7) | 21,580 (25.6) | 21,516 (26.5) | 23,309 (27.0) | 19,523 (24.5) |
| Q2 | 106,166 (25.0) | 21,511 (23.0) | 29,219 (25.2) | 34,424 (25.9) | 21,013 (25.5) | 15,010 (24.2) | 11,668 (23.9) | 31,288 (24.9) | 48,200 (25.6) | 20,942 (22.4) | 21,448 (25.4) | 21,178 (26.1) | 23,015 (26.7) | 19,583 (24.6) |
| Q3 | 106,173 (25.0) | 23,525 (25.2) | 29,137 (25.1) | 33,064 (24.9) | 20,447 (24.8) | 15,560 (25.1) | 12,331 (25.2) | 31,156 (24.8) | 47,126 (25.0) | 23,521 (25.2) | 21,228 (25.2) | 20,389 (25.1) | 21,320 (24.7) | 19,714 (24.8) |
| Q4 (highest) | 106,174 (25.0) | 28,338 (30.3) | 27,794 (24.0) | 29,701 (22.4) | 20,340 (24.6) | 17,190 (27.7) | 13,173 (27.0) | 30,578 (24.4) | 45,232 (24.0) | 28,559 (30.6) | 20,135 (23.9) | 18,035 (22.2) | 18,673 (21.6) | 20,772 (26.1) |
| Types of most commonly consumed coffee | ||||||||||||||
| Coffee drinkers, n (%) | 331,222 (78.0) | NA | 115,909 (100.0) | 132,751 (100.0) | 82,562 (100.0) | 52,278 (84.3) | 43,979 (90.0) | 104,787 (83.6) | 130,178 (69.1) | 43,791 (46.9) | 70,465 (83.5) | 63,568 (78.4) | 79,968 (92.6) | 73,430 (92.3) |
| Decaffeinated, n (%) | 63,810 (19.3) | NA | 22,792 (19.7) | 24,755 (18.6) | 16,263 (19.7) | 10,353 (19.8) | 7338 (16.7) | 19,553 (18.7) | 26,566 (20.4) | 8509 (19.4) | 12,579 (17.9) | 11,760 (18.4) | 16,234 (20.3) | 14,728 (20.1) |
| Instant, n (%) | 185,657 (56.1) | NA | 59,075 (51.0) | 73,168 (55.1) | 53,414 (64.7) | 31,757 (60.7) | 24,044 (54.7) | 57,380 (54.8) | 72,476 (55.7) | 20,701 (47.3) | 37,121 (52.7) | 35,252 (19.0) | 46,250 (57.8) | 46,333 (63.1) |
| Ground, n (%) | 75,748 (22.9) | NA | 30,729 (26.5) | 33,009 (24.9) | 12,010 (14.5) | 9371 (17.9) | 11,910 (27.1) | 26,030 (24.8) | 28,437 (21.8) | 13,249 (30.3) | 19,289 (27.4) | 15,497 (20.5) | 16,341 (20.4) | 11,372 (15.5) |
| Other, n (%) | 6007 (1.8) | NA | 3313 (2.9) | 1819 (1.4) | 875 (1.1) | 797 (1.5) | 687 (1.6) | 1824 (1.7) | 2699 (2.1) | 1332 (3.0) | 1476 (2.1) | 1059 (17.6) | 1143 (1.4) | 997 (1.4) |
| Characteristics | Hazard Ratio for Asthma | |||||||
|---|---|---|---|---|---|---|---|---|
| HR (95%CI) from Crude Model a | p-Value | HR (95%CI) from Model 1 b | p-Value | HR (95%CI) from Model 2 c | p-Value | HR (95%CI) from Model 3 d | p-Value | |
| Coffee (cups/day) | ||||||||
| 0 | Ref | Ref | Ref | Ref | ||||
| 0.5 to 1 | 0.872 (0.822~0.925) | <0.001 | 0.849 (0.800~0.901) | <0.001 | 0.912 (0.859~0.967) | 0.002 | 0.919 (0.866~0.976) | 0.006 |
| 2 to3 | 0.817 (0.771~0.866) | <0.001 | 0.800 (0.755~0.848) | <0.001 | 0.855 (0.807~0.907) | <0.001 | 0.877 (0.826~0.931) | <0.001 |
| ≥4 | 0.940 (0.882~1.001) | 0.054 | 0.944 (0.886~1.005) | 0.072 | 0.932 (0.874~0.993) | 0.03 | 0.970 (0.908~1.037) | 0.376 |
| Ptrend = 0.002 | Ptrend = 0.003 | Ptrend = 0.002 | Ptrend = 0.090 | |||||
| Tea (cups/day) | ||||||||
| 0 | Ref | Ref | Ref | Ref | ||||
| 0.5 to 1 | 0.822 (0.755~0.894) | <0.001 | 0.827 (0.760~0.900) | <0.001 | 0.891 (0.819~0.970) | 0.008 | 0.889 (0.816~0.968) | 0.007 |
| 2 to3 | 0.870 (0.815~0.930) | <0.001 | 0.856 (0.801~0.914) | <0.001 | 0.935 (0.875~1.000) | 0.049 | 0.929 (0.868~0.995) | 0.037 |
| ≥4 | 0.870 (0.815~0.930) | 0.195 | 0.938 (0.882~0.997) | 0.041 | 1.000 (0.940~1.064) | 0.996 | 0.991 (0.928~1.059) | 0.799 |
| Ptrend = 0.588 | Ptrend = 0.701 | Ptrend = 0.248 | Ptrend = 0.417 | |||||
| Coffee—caffeinated only (cups/day) | ||||||||
| 0 | Ref | Ref | Ref | Ref | ||||
| 0.5 to 1 | 0.837 (0.786~0.892) | <0.001 | 0.820 (0.770~0.870) | <0.001 | 0.876 (0.822~0.933) | <0.001 | 0.883 (0.829~0.941) | <0.001 |
| 2 to3 | 0.796 (0.749~0.846) | <0.001 | 0.911 (0.851~0.975) | <0.001 | 0.837 (0.786~0.890) | <0.001 | 0.858 (0.806~0.915) | <0.001 |
| ≥4 | 0.901 (0.842~0.965) | 0.003 | 0.911 (0.851~0.975) | 0.007 | 0.896 (0.836~0.960) | 0.002 | 0.933 (0.868~1.003) | 0.059 |
| Ptrend < 0.001 | Ptrend < 0.001 | Ptrend < 0.001 | Ptrend = 0.006 | |||||
| Tea and coffee—Caffeine intake quintiles | ||||||||
| Q1(≤160.0) | Ref | Ref | Ref | |||||
| Q2(160.0–235.0) | 0.889 (0.832~0.949) | <0.001 | 0.866 (0.811~0.925) | <0.001 | 0.899 (0.842~0.961) | 0.002 | NA | |
| Q3(235.0–305.0) | 0.922 (0.863~0.985) | 0.016 | 0.898 (0.840~0.959) | 0.001 | 0.926 (0.867~0.990) | 0.023 | NA | |
| Q4 (305.0–390.0) | 0.940 (0.882~1.003) | 0.061 | 0.915 (0.858~0.976) | 0.007 | 0.940 (0.881~1.003) | 0.062 | NA | |
| Q5 (≥390.0) | 1.035 (0.971~1.103) | 0.295 | 1.037 (0.972~1.105) | 0.274 | 0.999 (0.936~1.066) | 0.979 | NA | |
| Ptrend = 0.161 | Ptrend = 0.168 | Ptrend = 0.719 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, F.; Zhu, Y.; Liang, H.; Li, D.; Jing, D.; Liu, H.; Pan, P.; Zhang, Y. Association of Coffee and Tea Consumption with the Risk of Asthma: A Prospective Cohort Study from the UK Biobank. Nutrients 2022, 14, 4039. https://doi.org/10.3390/nu14194039
Lin F, Zhu Y, Liang H, Li D, Jing D, Liu H, Pan P, Zhang Y. Association of Coffee and Tea Consumption with the Risk of Asthma: A Prospective Cohort Study from the UK Biobank. Nutrients. 2022; 14(19):4039. https://doi.org/10.3390/nu14194039
Chicago/Turabian StyleLin, Fengyu, Yiqun Zhu, Huaying Liang, Dianwu Li, Danrong Jing, Hong Liu, Pinhua Pan, and Yan Zhang. 2022. "Association of Coffee and Tea Consumption with the Risk of Asthma: A Prospective Cohort Study from the UK Biobank" Nutrients 14, no. 19: 4039. https://doi.org/10.3390/nu14194039