
Urinary Potential Renal Acid Load (uPRAL) among Vegans Versus Omnivores and Its Association with Bone Health in the Cross-Sectional Risks and Benefits of a Vegan Diet Study

 , , , and
, , , and
Abstract
1. Introduction
- (i)
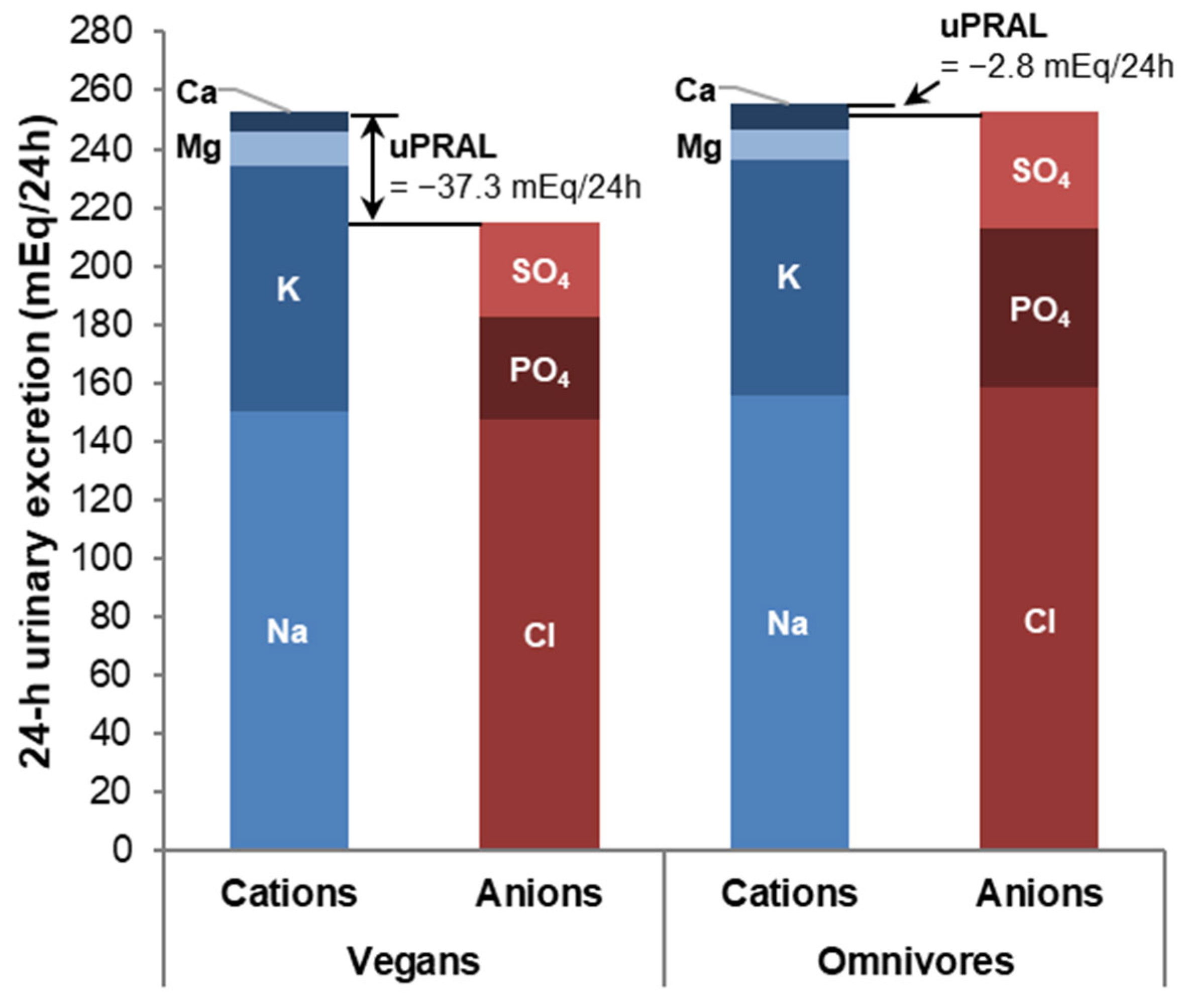
- Characterize uPRAL, 24 h urinary excretion profiles of acid-base relevant ions and urinary pH of vegans in comparison to omnivores.
- (ii)
- Investigate if the expected very low acid, i.e., alkaline, loads of vegan diets may contribute to alleviating the unfavorable association of veganism with poor bone health.
2. Materials and Methods
2.1. Design and Study Population
2.2. Bone Strength and Microstructure Parameters
2.3. Urine Sampling and Analysis
2.4. Dietary Intake Assessment
2.5. Assessment of Covariates
2.6. Statistical Analyses
3. Results
4. Discussion
4.1. Acid Load of Vegan Diets
4.2. Bone Health
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ogilvie, A.R.; McGuire, B.D.; Meng, L.; Shapses, S.A. Fracture Risk in Vegetarians and Vegans: The Role of Diet and Metabolic Factors. Curr. Osteoporos. Rep. 2022, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ho-Pham, L.T.; Nguyen, N.D.; Nguyen, T.V. Effect of vegetarian diets on bone mineral density: A Bayesian meta-analysis. Am. J. Clin. Nutr. 2009, 90, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Iguacel, I.; Miguel-Berges, M.L.; Gomez-Bruton, A.; Moreno, L.A.; Julian, C. Veganism, vegetarianism, bone mineral density, and fracture risk: A systematic review and meta-analysis. Nutr. Rev. 2019, 77, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Burckhardt, P. The role of low acid load in vegetarian diet on bone health: A narrative review. Swiss Med. Wkly. 2016, 146, w14277. [Google Scholar] [CrossRef]
- Ausman, L.M.; Oliver, L.M.; Goldin, B.R.; Woods, M.N.; Gorbach, S.L.; Dwyer, J.T. Estimated net acid excretion inversely correlates with urine pH in vegans, lacto-ovo vegetarians, and omnivores. J. Ren. Nutr. 2008, 18, 456–465. [Google Scholar] [CrossRef]
- Cupisti, A.; D’Alessandro, C.; Gesualdo, L.; Cosola, C.; Gallieni, M.; Egidi, M.F.; Fusaro, M. Non-Traditional Aspects of Renal Diets: Focus on Fiber, Alkali and Vitamin K1 Intake. Nutrients 2017, 9, 444. [Google Scholar] [CrossRef]
- Johnston, C.S.; Bliss, C.; Knurick, J.R.; Scholtz, C. Rapid Eating Assessment for Participants [shortened version] scores are associated with Healthy Eating Index-2010 scores and other indices of diet quality in healthy adult omnivores and vegetarians. Nutr. J. 2018, 17, 89. [Google Scholar] [CrossRef]
- Knurick, J.R.; Johnston, C.S.; Wherry, S.J.; Aguayo, I. Comparison of correlates of bone mineral density in individuals adhering to lacto-ovo, vegan, or omnivore diets: A cross-sectional investigation. Nutrients 2015, 7, 3416–3426. [Google Scholar] [CrossRef]
- Remer, T.; Krupp, D.; Shi, L. Dietary protein’s and dietary acid load’s influence on bone health. Crit. Rev. Food. Sci. Nutr. 2014, 54, 1140–1150. [Google Scholar] [CrossRef]
- Carnauba, R.A.; Baptistella, A.B.; Paschoal, V.; Hubscher, G.H. Diet-Induced Low-Grade Metabolic Acidosis and Clinical Outcomes: A Review. Nutrients 2017, 9, 538. [Google Scholar] [CrossRef]
- Frassetto, L.; Banerjee, T.; Powe, N.; Sebastian, A. Acid Balance, Dietary Acid Load, and Bone Effects—A Controversial Subject. Nutrients 2018, 10, 517. [Google Scholar] [CrossRef] [PubMed]
- de Jonge, E.A.L.; Koromani, F.; Hofman, A.; Uitterlinden, A.G.; Franco, O.H.; Rivadeneira, F.; Kiefte-de Jong, J.C. Dietary acid load, trabecular bone integrity, and mineral density in an ageing population: The Rotterdam study. Osteoporos Int. 2017, 28, 2357–2365. [Google Scholar] [CrossRef] [PubMed]
- Esche, J.; Johner, S.; Shi, L.; Schonau, E.; Remer, T. Urinary Citrate, an Index of Acid-Base Status, Predicts Bone Strength in Youths and Fracture Risk in Adult Females. J. Clin. Endocrinol. Metab. 2016, 101, 4914–4921. [Google Scholar] [CrossRef] [PubMed]
- Hayhoe, R.P.G.; Abdelhamid, A.; Luben, R.N.; Khaw, K.T.; Welch, A.A. Dietary acid-base load and its association with risk of osteoporotic fractures and low estimated skeletal muscle mass. Eur. J. Clin. Nutr. 2020, 74, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Jehle, S.; Hulter, H.N.; Krapf, R. Effect of potassium citrate on bone density, microarchitecture, and fracture risk in healthy older adults without osteoporosis: A randomized controlled trial. J. Clin. Endocrinol. Metab. 2013, 98, 207–217. [Google Scholar] [CrossRef]
- Galchenko, A.; Gapparova, K.; Sidorova, E. The influence of vegetarian and vegan diets on the state of bone mineral density in humans. Crit. Rev. Food Sci. Nutr. 2021, 1–17. [Google Scholar] [CrossRef]
- Frassetto, L.A.; Hardcastle, A.C.; Sebastian, A.; Aucott, L.; Fraser, W.D.; Reid, D.M.; Macdonald, H.M. No evidence that the skeletal non-response to potassium alkali supplements in healthy postmenopausal women depends on blood pressure or sodium chloride intake. Eur. J. Clin. Nutr. 2012, 66, 1315–1322. [Google Scholar] [CrossRef]
- Macdonald, H.M.; Black, A.J.; Aucott, L.; Duthie, G.; Duthie, S.; Sandison, R.; Hardcastle, A.C.; Lanham New, S.A.; Fraser, W.D.; Reid, D.M. Effect of potassium citrate supplementation or increased fruit and vegetable intake on bone metabolism in healthy postmenopausal women: A randomized controlled trial. Am. J. Clin. Nutr. 2008, 88, 465–474. [Google Scholar] [CrossRef]
- Weikert, C.; Trefflich, I.; Menzel, J.; Obeid, R.; Longree, A.; Dierkes, J.; Meyer, K.; Herter-Aeberli, I.; Mai, K.; Stangl, G.I.; et al. Vitamin and Mineral Status in a Vegan Diet. Dtsch. Arztebl. Int. 2020, 117, 575–582. [Google Scholar] [CrossRef]
- Menzel, J.; Abraham, K.; Stangl, G.I.; Ueland, P.M.; Obeid, R.; Schulze, M.B.; Herter-Aeberli, I.; Schwerdtle, T.; Weikert, C. Vegan Diet and Bone Health—Results from the Cross-Sectional RBVD Study. Nutrients 2021, 13, 685. [Google Scholar] [CrossRef]
- Remer, T.; Manz, F. Estimation of the renal net acid excretion by adults consuming diets containing variable amounts of protein. Am. J. Clin. Nutr. 1994, 59, 1356–1361. [Google Scholar] [CrossRef]
- Schofield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 1985, 39 (Suppl. 1), 5–41. [Google Scholar] [PubMed]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake:basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [PubMed]
- Johansson, L.; Solvoll, K.; Bjorneboe, G.E.; Drevon, C.A. Under- and overreporting of energy intake related to weight status and lifestyle in a nationwide sample. Am. J. Clin. Nutr. 1998, 68, 266–274. [Google Scholar] [CrossRef] [PubMed]
- InterAct, C.; Peters, T.; Brage, S.; Westgate, K.; Franks, P.W.; Gradmark, A.; Tormo Diaz, M.J.; Huerta, J.M.; Bendinelli, B.; Vigl, M.; et al. Validity of a short questionnaire to assess physical activity in 10 European countries. Eur. J. Epidemiol. 2012, 27, 15–25. [Google Scholar] [CrossRef]
- Ströhle, A.; Waldmann, A.; Koschizke, J.; Leitzmann, C.; Hahn, A. Diet-dependent net endogenous acid load of vegan diets in relation to food groups and bone health-related nutrients: Results from the German Vegan Study. Ann. Nutr. Metab. 2011, 59, 117–126. [Google Scholar] [CrossRef]
- Tong, T.Y.N.; Appleby, P.N.; Armstrong, M.E.G.; Fensom, G.K.; Knuppel, A.; Papier, K.; Perez-Cornago, A.; Travis, R.C.; Key, T.J. Vegetarian and vegan diets and risks of total and site-specific fractures: Results from the prospective EPIC-Oxford study. BMC Med. 2020, 18, 353. [Google Scholar] [CrossRef]
- Mitch, W.E. Metabolic and clinical consequences of metabolic acidosis. J. Nephrol. 2006, 19 (Suppl. 9), S70–S75. [Google Scholar]
- Raphael, K.L. Metabolic Acidosis in CKD: Core Curriculum 2019. Am. J. Kidney Dis. 2019, 74, 263–275. [Google Scholar] [CrossRef]
- Esche, J.; Shi, L.; Sanchez-Guijo, A.; Hartmann, M.F.; Wudy, S.A.; Remer, T. Higher diet-dependent renal acid load associates with higher glucocorticoid secretion and potentially bioactive free glucocorticoids in healthy children. Kidney Int. 2016, 90, 325–333. [Google Scholar] [CrossRef]
- Remer, T.; Manz, F.; Alexy, U.; Schoenau, E.; Wudy, S.A.; Shi, L. Long-term high urinary potential renal acid load and low nitrogen excretion predict reduced diaphyseal bone mass and bone size in children. J. Clin. Endocrinol. Metab. 2011, 96, 2861–2868. [Google Scholar] [CrossRef] [PubMed]
- Dawson-Hughes, B. Acid-base balance of the diet-implications for bone and muscle. Eur. J. Clin. Nutr. 2020, 74, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Alexy, U.; Remer, T.; Manz, F.; Neu, C.M.; Schoenau, E. Long-term protein intake and dietary potential renal acid load are associated with bone modeling and remodeling at the proximal radius in healthy children. Am. J. Clin. Nutr. 2005, 82, 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- Thorpe, M.; Mojtahedi, M.C.; Chapman-Novakofski, K.; McAuley, E.; Evans, E.M. A positive association of lumbar spine bone mineral density with dietary protein is suppressed by a negative association with protein sulfur. J. Nutr. 2008, 138, 80–85. [Google Scholar] [CrossRef]
- Chin, K.Y.; Ima-Nirwana, S. Calcaneal quantitative ultrasound as a determinant of bone health status: What properties of bone does it reflect? Int. J. Med. Sci. 2013, 10, 1778–1783. [Google Scholar] [CrossRef]
- Gonnelli, S.; Cepollaro, C. The use of ultrasound in the assessment of bone status. J. Endocrinol. Invest. 2002, 25, 389–397. [Google Scholar] [CrossRef]
- Guglielmi, G.; Adams, J.; Link, T.M. Quantitative ultrasound in the assessment of skeletal status. Eur. Radiol. 2009, 19, 1837–1848. [Google Scholar] [CrossRef] [PubMed]
- Hart, N.H.; Newton, R.U.; Tan, J.; Rantalainen, T.; Chivers, P.; Siafarikas, A.; Nimphius, S. Biological basis of bone strength: Anatomy, physiology and measurement. J. Musculoskelet Neuronal. Interact. 2020, 20, 347–371. [Google Scholar]
- Link, T.M.; Kazakia, G. Update on Imaging-Based Measurement of Bone Mineral Density and Quality. Curr. Rheumatol. Rep. 2020, 22, 13. [Google Scholar] [CrossRef]
- Gasser, J.A.; Hulter, H.N.; Imboden, P.; Krapf, R. Effect of chronic metabolic acidosis on bone density and bone architecture in vivo in rats. Am. J. Physiol. Renal. Physiol. 2014, 306, F517–F524. [Google Scholar] [CrossRef]
- Riggs, B.L.; Melton, L.J.; Robb, R.A.; Camp, J.J.; Atkinson, E.J.; McDaniel, L.; Amin, S.; Rouleau, P.A.; Khosla, S. A population-based assessment of rates of bone loss at multiple skeletal sites: Evidence for substantial trabecular bone loss in young adult women and men. J. Bone Miner Res. 2008, 23, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Pedone, C.; Napoli, N.; Pozzilli, P.; Lauretani, F.; Bandinelli, S.; Ferrucci, L.; Antonelli-Incalzi, R. Quality of diet and potential renal acid load as risk factors for reduced bone density in elderly women. Bone 2010, 46, 1063–1067. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Welch, A.A.; Bingham, S.A.; Reeve, J.; Khaw, K.T. More acidic dietary acid-base load is associated with reduced calcaneal broadband ultrasound attenuation in women but not in men: Results from the EPIC-Norfolk cohort study. Am. J. Clin. Nutr. 2007, 85, 1134–1141. [Google Scholar] [CrossRef] [PubMed]
- Wynn, E.; Lanham-New, S.A.; Krieg, M.A.; Whittamore, D.R.; Burckhardt, P. Low estimates of dietary acid load are positively associated with bone ultrasound in women older than 75 years of age with a lifetime fracture. J. Nutr. 2008, 138, 1349–1354. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | n | Vegans | Omnivores | p |
|---|---|---|---|---|
| n | 69 | 34 | 35 | |
| Sex (n, % females) | 69 | 17 (50%) | 17 (48.6%) | 0.9 |
| Age (years) | 69 | 36.5 (32.0, 41.0) | 38.0 (32.0, 46.0) | 0.7 |
| Anthropometric data | ||||
| BMI (kg/m2) | 69 | 22.2 (20.3, 24.9) | 23.7 (22.3, 25.2) | 0.034 |
| Socioeconomic status and lifestyle data | ||||
| High educational attainment (n, %) | 69 | 23 (67.6%) | 24 (68.6%) | >0.9 |
| Duration of veganism (years) | 69 | 4.9 (3.1, 11.1) | 0 | |
| Physical activity (n, %) a | 69 | 0.7 | ||
| Inactive | 5 (14.7%) | 4 (11.4%) | ||
| Active | 29 (85.3%) | 31 (88.6%) | ||
| Smoking status (n, %) | 69 | 0.2 | ||
| Non-smoker | 23 (67.6%) | 21 (60.0%) | ||
| Ex-smoker | 8 (23.5%) | 5 (14.3%) | ||
| Current smoker | 3 (8.8%) | 9 (25.7%) | ||
| Menopausal status (n, %) b | 33 | 0.5 | ||
| Pre/peri | 13 (76.5%) | 14 (82.4%) | ||
| Post | 3 (17.6%) | 3 (17.6%) | ||
| Dietary intake data | ||||
| Total energy (MJ/d) | 69 | 9.6 (7.7, 11.7) | 10.0 (8.9, 11.5) | 0.4 |
| Protein (%en) | 69 | 12.2 (10.9, 15.7) | 14.6 (12.3, 16.6) | 0.019 |
| Protein (g/kg body weight/d) | 69 | 1.0 (0.9, 1.4) | 1.2 (1.1, 1.5) | 0.06 |
| Alcohol (g/d) | 69 | 0.05 (0.00, 2.00) | 1.16 (0.02, 13.7) | 0.026 |
| 24 h urinary excretion data | ||||
| uPRAL (mEq/24 h) | 69 | −37.3 ± 31.5 | −2.8 ± 22.5 | <0.0001 |
| Urine volume (L/24 h) | 69 | 2.2 (1.6, 2.9) | 1.9 (1.5, 2.6) | 0.3 |
| Chloride (mmol/24 h) | 69 | 132 (94, 190) | 147 (102, 203) | 0.6 |
| Sulfate (mmol/24 h) | 69 | 14.7 (10.1, 18.9) | 20.8 (13.6, 24.2) | 0.012 |
| Phosphate (mmol/24 h) | 69 | 18.9 (14.1, 24.0) | 26.5 (21.1, 39.0) | 0.0004 |
| Sodium (mmol/24 h) | 69 | 143 (102, 184) | 138 (100, 198) | 0.9 |
| Potassium (mmol/24 h) | 69 | 82 (59, 106) | 69 (61, 107) | 0.7 |
| Calcium (mmol/24 h) | 69 | 2.9 (1.8, 4.5) | 4.1 (3.1, 5.8) | 0.046 |
| Magnesium (mmol/24 h) | 69 | 5.4 (4.0, 7.1) | 4.2 (3.3, 6.8) | 0.1 |
| Urinary pH | 69 | 6.7 (6.4, 7.1) | 6.2 (5.9, 6.4) | <0.0001 |
| Bone health parameters c | ||||
| BUA (dB/MHz) | 68 | 112 ± 11 | 118 ± 11 | 0.037 |
| SOS (m/s) | 68 | 1584 ± 27 | 1593 ± 40 | 0.3 |
| SI | 68 | 98 ± 13 | 104 ± 17 | 0.1 |
| Predictor: uPRAL | ||||||
|---|---|---|---|---|---|---|
| T1 (n = 22) −53.6 (−67.0, −44.1) a | T2 (n = 24) −15.2 (−21.5, −10.9) a | T3 (n = 22) 14.1 (4.0, 20.2) a | βtrend | SEtrend | ptrend | |
| Vegans/Omnivores b | 19/3 | 10/14 | 5/17 | |||
| BUA (dB/MHz) | ||||||
| Model A | 114 (109–119) | 113 (109–117) | 118 (113–123) | +0.024 | 0.042 | 0.6 |
| Model B | 116 (111–121) | 112 (108–117) | 116 (111–121) | −0.031 | 0.048 | 0.5 |
| Model C | 116 (111–121) | 113 (109–117) | 116 (111–121) | −0.041 | 0.046 | 0.4 |
| Model D | 116 (111–121) | 114 (109–118) | 115 (111–120) | −0.030 | 0.048 | 0.5 |
| SOS (m/s) | ||||||
| Model A | 1584 (1570–1599) | 1584 (1570–1598) | 1597 (1583–1611) | +0.166 | 0.128 | 0.2 |
| Model B | 1586 (1570–1603) | 1584 (1570–1598) | 1595 (1580–1611) | +0.129 | 0.152 | 0.4 |
| Model C | 1587 (1571–1602) | 1585 (1572–1599) | 1593 (1578–1608) | +0.100 | 0.147 | 0.5 |
| Model D | 1587 (1571–1604) | 1586 (1572–1600) | 1592 (1576–1607) | +0.127 | 0.159 | 0.4 |
| SI | ||||||
| Model A | 100 (93–106) | 99 (92–105) | 106 (99–112) | +0.062 | 0.058 | 0.3 |
| Model B | 102 (94–109) | 98 (92–104) | 104 (97–111) | +0.015 | 0.068 | 0.8 |
| Model C | 102 (95–109) | 99 (93–105) | 103 (96–110) | +0.001 | 0.065 | >0.9 |
| Model D | 102 (95–109) | 100 (94–106) | 102 (96–109) | +0.015 | 0.069 | 0.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Penczynski, K.J.; Remer, T.; Menzel, J.; Abraham, K.; Weikert, C. Urinary Potential Renal Acid Load (uPRAL) among Vegans Versus Omnivores and Its Association with Bone Health in the Cross-Sectional Risks and Benefits of a Vegan Diet Study. Nutrients 2022, 14, 4468. https://doi.org/10.3390/nu14214468
Penczynski KJ, Remer T, Menzel J, Abraham K, Weikert C. Urinary Potential Renal Acid Load (uPRAL) among Vegans Versus Omnivores and Its Association with Bone Health in the Cross-Sectional Risks and Benefits of a Vegan Diet Study. Nutrients. 2022; 14(21):4468. https://doi.org/10.3390/nu14214468
Chicago/Turabian StylePenczynski, Katharina J., Thomas Remer, Juliane Menzel, Klaus Abraham, and Cornelia Weikert. 2022. "Urinary Potential Renal Acid Load (uPRAL) among Vegans Versus Omnivores and Its Association with Bone Health in the Cross-Sectional Risks and Benefits of a Vegan Diet Study" Nutrients 14, no. 21: 4468. https://doi.org/10.3390/nu14214468
APA StylePenczynski, K. J., Remer, T., Menzel, J., Abraham, K., & Weikert, C. (2022). Urinary Potential Renal Acid Load (uPRAL) among Vegans Versus Omnivores and Its Association with Bone Health in the Cross-Sectional Risks and Benefits of a Vegan Diet Study. Nutrients, 14(21), 4468. https://doi.org/10.3390/nu14214468