
Diet and Risk of Non-Alcoholic Fatty Liver Disease, Cirrhosis, and Liver Cancer: A Large Prospective Cohort Study in UK Biobank


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Assessment of Dietary Intake
2.3. Assessment of Dietary Patterns
2.4. Ascertainment of Outcomes
2.5. Covariates
2.6. Statistical Analysis
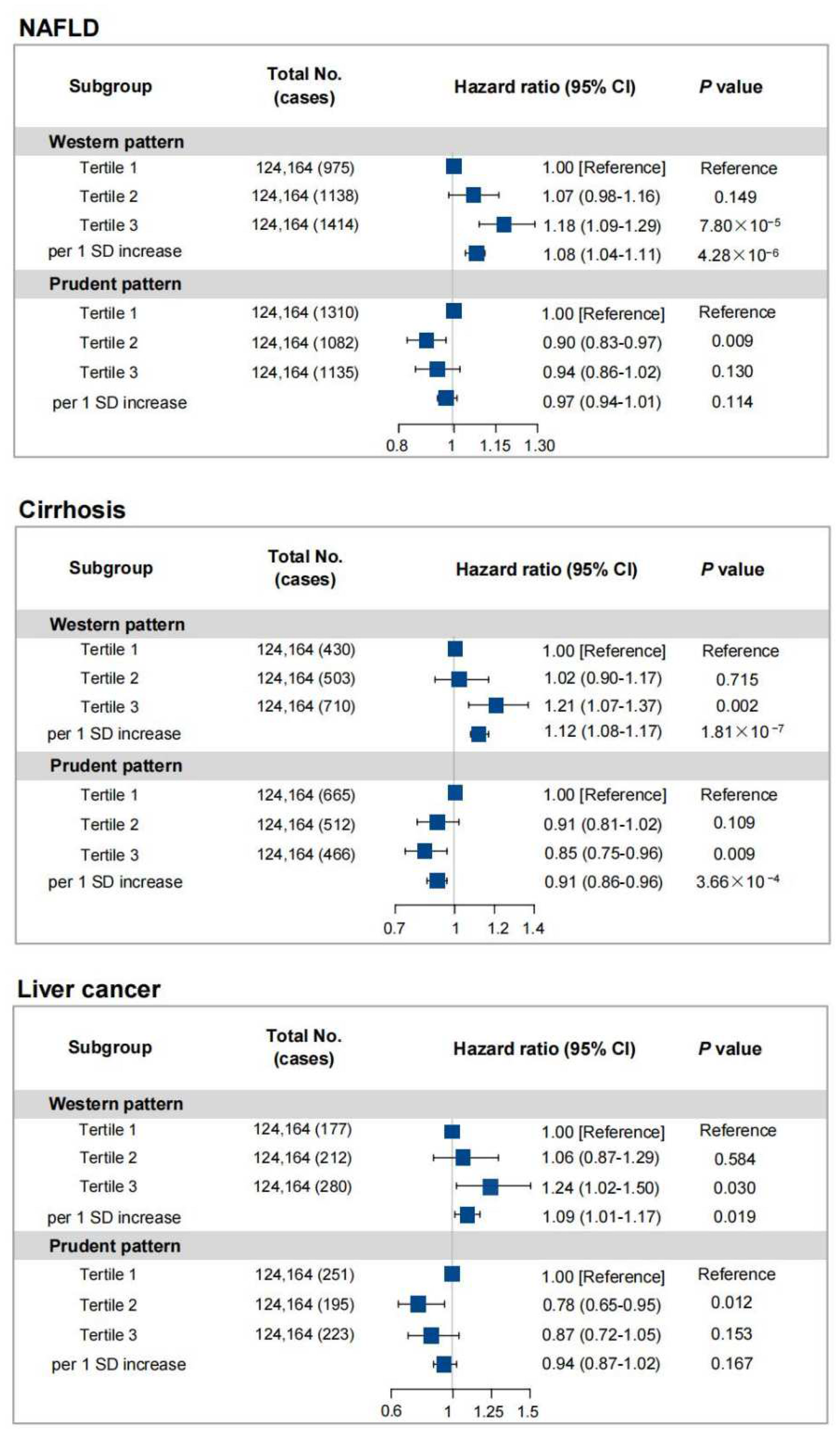
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethics Approval
References
- Paik, J.M.; Golabi, P.; Younossi, Y.; Mishra, A.; Younossi, Z.M. Changes in the Global Burden of Chronic Liver Diseases From 2012 to 2017: The Growing Impact of NAFLD. Hepatology 2020, 72, 1605–1616. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Wang, F.; Wong, N.-K.; He, J.; Zhang, R.; Sun, R.; Xu, Y.; Liu, Y.; Li, W.; Koike, K.; et al. Global liver disease burdens and research trends: Analysis from a Chinese perspective. J. Hepatol. 2019, 71, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.L.; Neuschwander-Tetri, B.A.; Rinella, M.; Sanyal, A.J. Mechanisms of NAFLD development and therapeutic strategies. Nat. Med. 2018, 24, 908–922. [Google Scholar] [CrossRef]
- Tsuchida, T.; Lee, Y.A.; Fujiwara, N.; Ybanez, M.; Allen, B.; Martins, S.; Fiel, M.I.; Goossens, N.; Chou, H.-I.; Hoshida, Y.; et al. A simple diet- and chemical-induced murine NASH model with rapid progression of steatohepatitis, fibrosis and liver cancer. J. Hepatol. 2018, 69, 385–395. [Google Scholar] [CrossRef]
- Li, R.; Li, J.; Huang, Y.; Li, H.; Yan, S.; Lin, J.; Chen, Y.; Wu, L.; Liu, B.; Wang, G.; et al. Polydatin attenuates diet-induced nonalcoholic steatohepatitis and fibrosis in mice. Int. J. Biol. Sci. 2018, 14, 1411–1425. [Google Scholar] [CrossRef]
- Jensen, T.; Abdelmalek, M.F.; Sullivan, S.; Nadeau, K.J.; Green, M.; Roncal, C.; Nakagawa, T.; Kuwabara, M.; Sato, Y.; Kang, D.-H.; et al. Fructose and sugar: A major mediator of non-alcoholic fatty liver disease. J. Hepatol. 2018, 68, 1063–1075. [Google Scholar] [CrossRef]
- Zhang, X.; Coker, O.O.; Chu, E.S.; Fu, K.; Lau, H.C.H.; Wang, Y.-X.; Chan, A.W.H.; Wei, H.; Yang, X.; Sung, J.J.Y.; et al. Dietary cholesterol drives fatty liver-associated liver cancer by modulating gut microbiota and metabolites. Gut 2021, 70, 761–774. [Google Scholar] [CrossRef]
- Vancells Lujan, P.; Viñas Esmel, E.; Sacanella Meseguer, E. Overview of Non-Alcoholic Fatty Liver Disease (NAFLD) and the Role of Sugary Food Consumption and Other Dietary Components in Its Development. Nutrients 2021, 13, 1442. [Google Scholar] [CrossRef]
- Aller, R.; Sigüenza, R.; Pina, M.; Laserna, C.; Antolín, B.; Burgueño, B.; Durà, M.; Izaola, O.; Primo, D.; de Luis, D.A. Insulin resistance is related with liver fibrosis in type 2 diabetic patients with non-alcoholic fatty liver disease proven biopsy and Mediterranean diet pattern as a protective factor. Endocrine 2020, 68, 557–563. [Google Scholar] [CrossRef]
- Ma, Y.; Yang, W.; Simon, T.G.; Smith-Warner, S.A.; Fung, T.T.; Sui, J.; Chong, D.; VoPham, T.; Meyerhardt, J.A.; Wen, D.; et al. Dietary Patterns and Risk of Hepatocellular Carcinoma Among U.S. Men and Women. Hepatology 2019, 70, 577–586. [Google Scholar] [CrossRef] [PubMed]
- George, E.S.; Sood, S.; Broughton, A.; Cogan, G.; Hickey, M.; Chan, W.S.; Sudan, S.; Nicoll, A.J. The Association between Diet and Hepatocellular Carcinoma: A Systematic Review. Nutrients 2021, 13, 172. [Google Scholar] [CrossRef] [PubMed]
- Neuhouser, M.L. The importance of healthy dietary patterns in chronic disease prevention. Nutr. Res. 2019, 70, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Sudlow, C.; Gallacher, J.; Allen, N.; Beral, V.; Burton, P.; Danesh, J.; Downey, P.; Elliott, P.; Green, J.; Landray, M.; et al. UK biobank: An open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 2015, 12, e1001779. [Google Scholar] [CrossRef] [PubMed]
- Bradbury, K.E.; Young, H.J.; Guo, W.; Key, T.J. Dietary assessment in UK Biobank: An evaluation of the performance of the touchscreen dietary questionnaire. J. Nutr. Sci. 2018, 7, e6. [Google Scholar] [CrossRef]
- Smith, A.D.; Emmett, P.M.; Newby, P.K.; Northstone, K. Dietary patterns obtained through principal components analysis: The effect of input variable quantification. Br. J. Nutr. 2013, 109, 1881–1891. [Google Scholar] [CrossRef]
- Yu, C.; Shi, Z.; Lv, J.; Du, H.; Qi, L.; Guo, Y.; Bian, Z.; Chang, L.; Tang, X.; Jiang, Q.; et al. Major Dietary Patterns in Relation to General and Central Obesity among Chinese Adults. Nutrients 2015, 7, 5834–5849. [Google Scholar] [CrossRef]
- Previdelli, Á.N.; de Andrade, S.C.; Fisberg, R.M.; Marchioni, D.M. Using Two Different Approaches to Assess Dietary Patterns: Hypothesis-Driven and Data-Driven Analysis. Nutrients 2016, 8, 593. [Google Scholar] [CrossRef]
- Strate, L.L.; Keeley, B.R.; Cao, Y.; Wu, K.; Giovannucci, E.L.; Chan, A.T. Western Dietary Pattern Increases, and Prudent Dietary Pattern Decreases, Risk of Incident Diverticulitis in a Prospective Cohort Study. Gastroenterology 2017, 152, 1023–1030.e1022. [Google Scholar] [CrossRef]
- Emdin, C.A.; Haas, M.; Ajmera, V.; Simon, T.G.; Homburger, J.; Neben, C.; Jiang, L.; Wei, W.-Q.; Feng, Q.; Zhou, A.; et al. Association of Genetic Variation With Cirrhosis: A Multi-Trait Genome-Wide Association and Gene-Environment Interaction Study. Gastroenterology 2021, 160, 1620–1633.e13. [Google Scholar] [CrossRef]
- Zhou, F.; Zhou, J.; Wang, W.; Zhang, X.-J.; Ji, Y.-X.; Zhang, P.; She, Z.-G.; Zhu, L.; Cai, J.; Li, H. Unexpected Rapid Increase in the Burden of NAFLD in China From 2008 to 2018: A Systematic Review and Meta-Analysis. Hepatology 2019, 70, 1119–1133. [Google Scholar] [CrossRef] [PubMed]
- Zelber-Sagi, S.; Ivancovsky-Wajcman, D.; Fliss Isakov, N.; Webb, M.; Orenstein, D.; Shibolet, O.; Kariv, R. High red and processed meat consumption is associated with non-alcoholic fatty liver disease and insulin resistance. J. Hepatol. 2018, 68, 1239–1246. [Google Scholar] [CrossRef] [PubMed]
- Rahimi-Sakak, F.; Maroofi, M.; Emamat, H.; Hekmatdoost, A. Red and Processed Meat Intake in Relation to Non-Alcoholic Fatty Liver Disease Risk: Results from a Case-Control Study. Clin. Nutr. Res. 2022, 11, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Lee, H.S.; Ahn, S.B.; Kwon, Y.-J. Dairy protein intake is inversely related to development of non-alcoholic fatty liver disease. Clin. Nutr. 2021, 40, 5252–5260. [Google Scholar] [CrossRef]
- Kim, S.-A.; Shin, S. Fruit and vegetable consumption and non-alcoholic fatty liver disease among Korean adults: A prospective cohort study. J. Epidemiol. Community Health 2020, 74, 1035–1042. [Google Scholar] [CrossRef]
- Li, H.; Wang, X.; Ye, M.; Zhang, S.; Zhang, Q.; Meng, G.; Liu, L.; Wu, H.; Gu, Y.; Wang, Y.; et al. Does a high intake of green leafy vegetables protect from NAFLD? Evidence from a large population study. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1691–1701. [Google Scholar] [CrossRef]
- Boeing, H.; Bechthold, A.; Bub, A.; Ellinger, S.; Haller, D.; Kroke, A.; Leschik-Bonnet, E.; Müller, M.J.; Oberritter, H.; Schulze, M.; et al. Critical review: Vegetables and fruit in the prevention of chronic diseases. Eur. J. Nutr. 2012, 51, 637–663. [Google Scholar] [CrossRef]
- Wei, X.; Zhu, C.; Ji, M.; Fan, J.; Xie, J.; Huang, Y.; Jiang, X.; Xu, J.; Yin, R.; Du, L.; et al. Diet and Risk of Incident Lung Cancer: A Large Prospective Cohort Study in UK Biobank. Am. J. Clin. Nutr. 2021, 114, 2043–2051. [Google Scholar] [CrossRef]
- Salehi-Sahlabadi, A.; Sadat, S.; Beigrezaei, S.; Pourmasomi, M.; Feizi, A.; Ghiasvand, R.; Hadi, A.; Clark, C.C.T.; Miraghajani, M. Dietary patterns and risk of non-alcoholic fatty liver disease. BMC Gastroenterol. 2021, 21, 41. [Google Scholar] [CrossRef]
- Hassani Zadeh, S.; Mansoori, A.; Hosseinzadeh, M. Relationship between dietary patterns and non-alcoholic fatty liver disease: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2021, 36, 1470–1478. [Google Scholar] [CrossRef]
- Ginès, P.; Krag, A.; Abraldes, J.G.; Solà, E.; Fabrellas, N.; Kamath, P.S. Liver cirrhosis. Lancet 2021, 398, 1359–1376. [Google Scholar] [CrossRef] [PubMed]
- Ganguly, S.; Muench, G.A.; Shang, L.; Rosenthal, S.B.; Rahman, G.; Wang, R.; Wang, Y.; Kwon, H.C.; Diomino, A.M.; Kisseleva, T.; et al. Nonalcoholic Steatohepatitis and HCC in a Hyperphagic Mouse Accelerated by Western Diet. Cell. Mol. Gastroenterol. Hepatol. 2021, 12, 891–920. [Google Scholar] [CrossRef] [PubMed]
- Amodio, P.; Bemeur, C.; Butterworth, R.; Cordoba, J.; Kato, A.; Montagnese, S.; Uribe, M.; Vilstrup, H.; Morgan, M.Y. The nutritional management of hepatic encephalopathy in patients with cirrhosis: International Society for Hepatic Encephalopathy and Nitrogen Metabolism Consensus. Hepatology 2013, 58, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Yang, Y.; Liu, J.; Lu, K.; Tang, Z.; Liu, P.; Liu, L.; Zhu, Y. Systematic review with meta-analysis: Meat consumption and the risk of hepatocellular carcinoma. Aliment. Pharmacol. Ther. 2014, 39, 913–922. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.-F.; Shao, X.-F.; Li, J.-M.; Li, S.; Li, K.-L.; Li, D. Fruit and vegetable intake and liver cancer risk: A meta-analysis of prospective cohort studies. Food Funct. 2019, 10, 4478–4485. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Tamakoshi, A.; Sugawara, Y.; Mizoue, T.; Inoue, M.; Sawada, N.; Matsuo, K.; Ito, H.; Naito, M.; Nagata, C.; et al. Coffee, green tea and liver cancer risk: An evaluation based on a systematic review of epidemiologic evidence among the Japanese population. Jpn. J. Clin. Oncol. 2019, 49, 972–984. [Google Scholar] [CrossRef]
- Yang, W.; Ma, Y.; Liu, Y.; Smith-Warner, S.A.; Simon, T.G.; Chong, D.Q.; Qi, Q.; Meyerhardt, J.A.; Giovannucci, E.L.; Chan, A.T.; et al. Association of Intake of Whole Grains and Dietary Fiber With Risk of Hepatocellular Carcinoma in US Adults. JAMA Oncol. 2019, 5, 879–886. [Google Scholar] [CrossRef]
- Quesada-Vázquez, S.; Aragonès, G.; Del Bas, J.M.; Escoté, X. Diet, Gut Microbiota and Non-Alcoholic Fatty Liver Disease: Three Parts of the Same Axis. Cells 2020, 9, 176. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Total (n = 372,492) | NAFLD | Cirrhosis | Liver Cancer | |||
|---|---|---|---|---|---|---|---|
| Case (n = 3527) | Non-Case (n = 368,965) | Case (n = 1643) | Non-Case (n = 370,849) | Case (n = 669) | Non-Case (n = 371,823) | ||
| Age (years), mean (sd) | 56.73 (8.10) | 57.22 (7.88) | 56.73 (8.10) | 59.14 (7.44) | 56.72 (8.10) | 61.84 (6.18) | 56.73 (8.10) |
| Gender, % | |||||||
| Male | 176,327 (47.34) | 1751 (49.65) | 174,576 (47.32) | 1105 (67.26) | 175,222 (47.25) | 412 (61.58) | 175,915 (47.31) |
| Female | 196,165 (52.66) | 1776 (50.35) | 194,389 (52.68) | 538 (32.74) | 195,627 (52.75) | 257 (38.42) | 195,908 (52.69) |
| White ethnicity, % | |||||||
| Yes | 355,879 (95.54) | 3342 (94.75) | 352,537 (95.55) | 1589 (96.71) | 354,290 (95.53) | 650 (97.16) | 355,229 (95.54) |
| No | 16613 (4.46) | 185 (5.25) | 16428 (4.45) | 54 (3.29) | 16559 (4.47) | 19 (2.84) | 16594 (4.46) |
| Education level, % | |||||||
| College or University degree | 133,579 (35.86) | 874 (24.78) | 132,705 (35.97) | 411 (25.02) | 133,168 (35.91) | 182 (27.20) | 133,397 (35.88) |
| Other levels | 238,913 (64.14) | 2653 (75.22) | 236,260 (64.03) | 1232 (74.98) | 237,681 (64.09) | 487 (72.80) | 238,426 (64.12) |
| Townsend deprivation index, % | |||||||
| Quartile 1 | 936,65 (25.15) | 675 (19.14) | 92,990 (25.21) | 308 (18.75) | 93,357 (25.17) | 152 (22.72) | 93,513 (25.15) |
| Quartile 2 | 925,55 (24.85) | 722 (20.47) | 91,833 (24.89) | 320 (19.48) | 92,235 (24.87) | 164 (24.51) | 92,391 (24.85) |
| Quartile 3 | 932,11 (25.02) | 849 (24.07) | 92,362 (25.03) | 386 (23.49) | 92,825 (25.03) | 160 (23.92) | 93,051 (25.03) |
| Quartile 4 | 930,61 (24.98) | 1281 (36.32) | 91,780 (24.87) | 629 (38.28) | 92,432 (24.92) | 193 (28.85) | 92,868 (24.98) |
| Regular exercise, % | |||||||
| Yes | 202,347 (54.32) | 1623 (46.02) | 200,724 (54.40) | 751 (45.71) | 201,596 (54.36) | 336 (50.22) | 202,011 (54.33) |
| No | 170,145 (45.68) | 1904 (53.98) | 168,241 (45.60) | 892 (54.29) | 169,253 (45.64) | 333 (49.78) | 169,812 (45.67) |
| Drinking status, % | |||||||
| Never | 13,726 (3.68) | 205 (5.81) | 13,521 (3.66) | 67 (4.08) | 13,659 (3.68) | 29 (4.33) | 13,697 (3.68) |
| Former | 11,802 (3.17) | 225 (6.38) | 11,577 (3.14) | 123 (7.49) | 11,679 (3.15) | 23 (3.44) | 11,779 (3.17) |
| Current | 346,964 (93.15) | 3097 (87.81) | 343,867 (93.20) | 1453 (88.44) | 345,511 (93.17) | 617 (92.23) | 346,347 (93.15) |
| Smoking status, % | |||||||
| Never | 205,007 (55.04) | 1581 (44.83) | 203,426 (55.13) | 626 (38.10) | 204,381 (55.11) | 278 (41.55) | 204,729 (55.06) |
| Former | 130,392 (35.01) | 1424 (40.37) | 128,968 (34.95) | 702 (42.73) | 129,690 (34.97) | 295 (44.10) | 130,097 (34.99) |
| Current | 37,093 (9.96) | 522 (14.80) | 36,571 (9.91) | 315 (19.17) | 36,778 (9.92) | 96 (14.35) | 36,997 (9.95) |
| BMI, % | |||||||
| Normal | 126,020 (33.83) | 357 (10.12) | 125,663 (34.06) | 317 (19.29) | 125,703 (33.90) | 162 (24.22) | 125,858 (33.85) |
| Overweight | 160,163 (43.00) | 1286 (36.46) | 158,877 (43.06) | 591 (35.97) | 159,572 (43.03) | 264 (39.46) | 159,899 (43.00) |
| Obesity | 86,309 (23.17) | 1884 (53.42) | 84,425 (22.88) | 735 (44.74) | 85,574 (23.08) | 243 (36.32) | 86,066 (23.15) |
| Diabetes, % | |||||||
| Yes | 17,869 (4.80) | 588 (16.67) | 17,281 (4.68) | 346 (21.06) | 17,523 (4.73) | 121 (18.09) | 17,748 (4.77) |
| No | 354,623 (95.20) | 2939 (83.33) | 351,684 (95.32) | 1297 (78.94) | 353,326 (95.27) | 548 (81.91) | 354,075 (95.23) |
| Components | Prudent Pattern | Western Pattern |
|---|---|---|
| Salad raw vegetables | 0.64 | 0.02 |
| Cooked vegetables | 0.57 | 0.12 |
| Fresh fruit | 0.59 | −0.07 |
| Dried fruit | 0.43 | −0.07 |
| Oily fish | 0.52 | 0.08 |
| Non-oily fish | 0.39 | 0.16 |
| Processed meat | −0.31 | 0.49 |
| Poultry | 0.10 | 0.44 |
| Beef | −0.09 | 0.64 |
| Lamb/mutton | 0.02 | 0.66 |
| Pork | −0.05 | 0.66 |
| Bread | −0.24 | 0.16 |
| Cheese | −0.14 | 0.03 |
| Tea | 0.01 | 0.08 |
| Cereal | 0.18 | −0.13 |
| Variance explained [%] | 13 | 12 |
| Cumulative Var [%] | 13 | 25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, W.; Ge, X.; Lu, J.; Xu, X.; Gao, J.; Wang, Q.; Song, C.; Zhang, Q.; Yu, C. Diet and Risk of Non-Alcoholic Fatty Liver Disease, Cirrhosis, and Liver Cancer: A Large Prospective Cohort Study in UK Biobank. Nutrients 2022, 14, 5335. https://doi.org/10.3390/nu14245335
Guo W, Ge X, Lu J, Xu X, Gao J, Wang Q, Song C, Zhang Q, Yu C. Diet and Risk of Non-Alcoholic Fatty Liver Disease, Cirrhosis, and Liver Cancer: A Large Prospective Cohort Study in UK Biobank. Nutrients. 2022; 14(24):5335. https://doi.org/10.3390/nu14245335
Chicago/Turabian StyleGuo, Wen, Xinyuan Ge, Jing Lu, Xin Xu, Jiaxin Gao, Quanrongzi Wang, Ci Song, Qun Zhang, and Chengxiao Yu. 2022. "Diet and Risk of Non-Alcoholic Fatty Liver Disease, Cirrhosis, and Liver Cancer: A Large Prospective Cohort Study in UK Biobank" Nutrients 14, no. 24: 5335. https://doi.org/10.3390/nu14245335
APA StyleGuo, W., Ge, X., Lu, J., Xu, X., Gao, J., Wang, Q., Song, C., Zhang, Q., & Yu, C. (2022). Diet and Risk of Non-Alcoholic Fatty Liver Disease, Cirrhosis, and Liver Cancer: A Large Prospective Cohort Study in UK Biobank. Nutrients, 14(24), 5335. https://doi.org/10.3390/nu14245335