
Efficacy of Donated Milk in Early Nutrition of Preterm Infants: A Meta-Analysis

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Date Extraction
2.4. Quality and Risk of Bias Assessment
2.5. Outcomes
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Included Studies
3.2. Primary Outcomes
3.2.1. Incidence of NEC
3.2.2. Length of Hospital Stay
3.2.3. Mortality
3.2.4. Incidence of Sepsis
3.2.5. Duration of Parenteral Nutrition
3.2.6. Incidence of Retinopathy of Prematurity
3.3. The Secondary Outcome
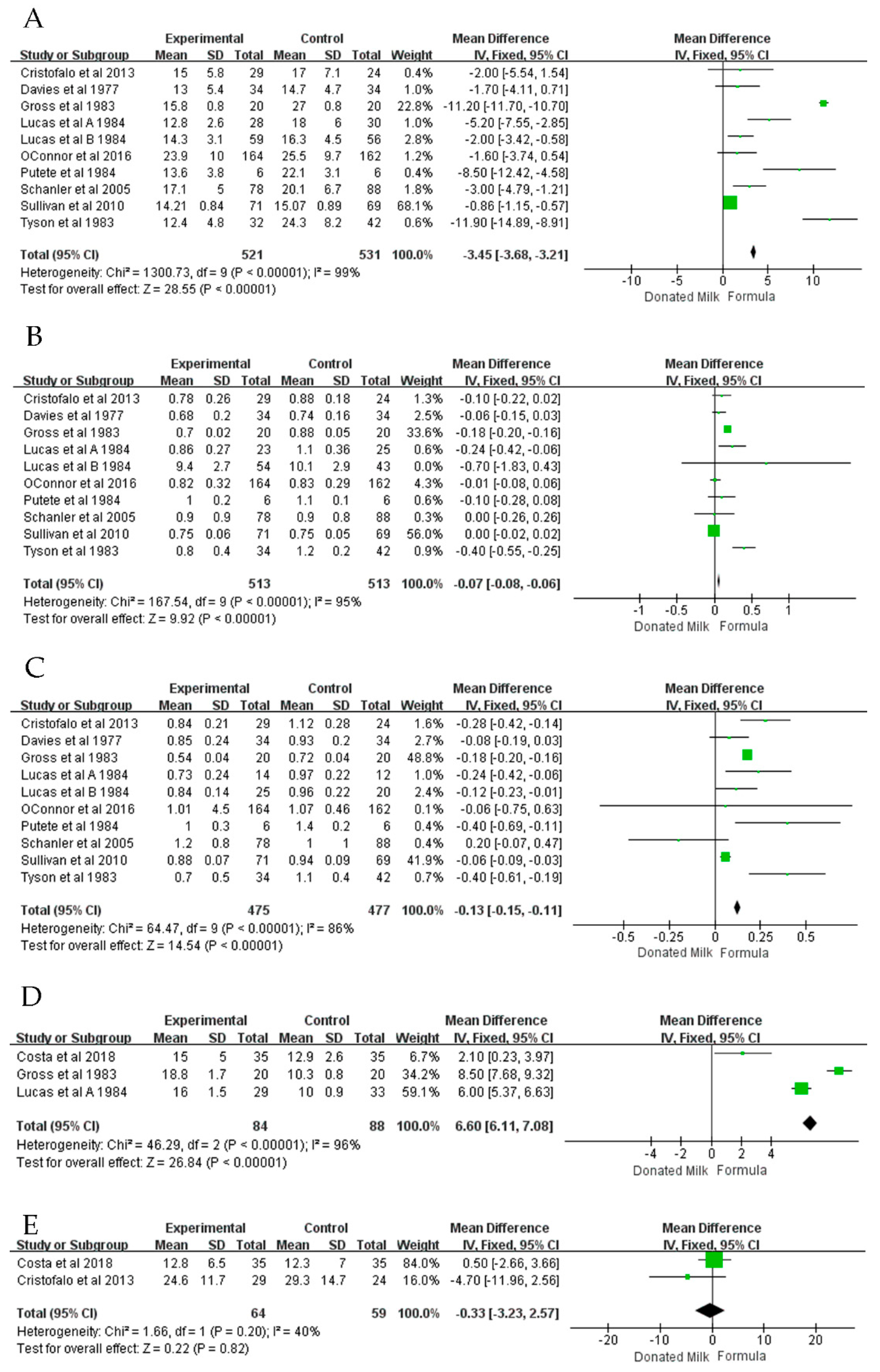
3.3.1. Weight Gain
3.3.2. Head Growth
3.3.3. Body Length Growth
3.3.4. Time to Regain Birth Weight
3.3.5. Time to Full Enteral Feed
3.4. Assessment of Risk of Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patel, R.M. Short-and Long-Term Outcomes for Extremely Preterm Infants. Am. J. Perinatol. 2016, 33, 318–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibson, A.; Carney, S.; Wales, J.K. Growth and the premature baby. Horm. Res. 2006, 65 (Suppl. 3), 75–81. [Google Scholar] [CrossRef] [PubMed]
- De Curtis, M.; Rigo, J. The nutrition of preterm infants. Early Hum. Dev. 2012, 88 (Suppl. 1), S5–S7. [Google Scholar] [CrossRef] [PubMed]
- Cerasani, J.; Ceroni, F.; De Cosmi, V.; Mazzocchi, A.; Morniroli, D.; Roggero, P.; Mosca, F.; Agostoni, C.; Giannì, M.L. Human Milk Feeding and Preterm Infants’ Growth and Body Composition: A Literature Review. Nutrients 2020, 12, 1155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flint, A.; New, K.; Davies, M.W. Cup feeding versus other forms of supplemental enteral feeding for newborn infants unable to fully breastfeed. Cochrane Database Syst. Rev. 2016, 2016, Cd005092. [Google Scholar] [CrossRef] [PubMed]
- Quigley, M.; Embleton, N.D.; McGuire, W. Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database Syst. Rev. 2018, 6, Cd002971. [Google Scholar] [CrossRef] [PubMed]
- Bertino, E.; Giuliani, F.; Baricco, M.; Di Nicola, P.; Peila, C.; Vassia, C.; Chiale, F.; Pirra, A.; Cresi, F.; Martano, C.; et al. Benefits of donor milk in the feeding of preterm infants. Early Hum. Dev. 2013, 89 (Suppl. 2), S3–S6. [Google Scholar] [CrossRef]
- Hanson, L.A.; Korotkova, M.; Telemo, E. Breast-feeding, infant formulas, and the immune system. Ann. Allergy Asthma Immunol. Off. Publ. Am. Coll. Allergy Asthma Immunol. 2003, 90, 59–63. [Google Scholar] [CrossRef]
- Schanler, R.J.; Shulman, R.J.; Lau, C. Feeding strategies for premature infants: Beneficial outcomes of feeding fortified human milk versus preterm formula. Pediatrics 1999, 103, 1150–1157. [Google Scholar] [CrossRef]
- Napierala, M.; Merritt, T.A.; Miechowicz, I.; Mielnik, K.; Mazela, J.; Florek, E. The effect of maternal tobacco smoking and second-hand tobacco smoke exposure on human milk oxidant-antioxidant status. Environ. Res. 2019, 170, 110–121. [Google Scholar] [CrossRef]
- Aceti, A.; Beghetti, I.; Martini, S.; Faldella, G.; Corvaglia, L. Oxidative Stress and Necrotizing Enterocolitis: Pathogenetic Mechanisms, Opportunities for Intervention, and Role of Human Milk. Oxidative Med. Cell. Longev. 2018, 2018, 7397659. [Google Scholar] [CrossRef] [Green Version]
- Yu, F.; Cao, B.; Wen, Z.; Li, M.; Chen, H.; Xie, G. Is Donated Breast Milk Better Than Formula for Feeding Very Low Birth Weight Infants? A Systematic Review and Meta-Analysis. Worldviews Evid. Based Nurs. 2019, 16, 485–494. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ (Clin. Res. Ed.) 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Cristofalo, E.A.; Schanler, R.J.; Blanco, C.L.; Sullivan, S.; Trawoeger, R.; Kiechl-Kohlendorfer, U.; Dudell, G.; Rechtman, D.J.; Lee, M.L.; Lucas, A.; et al. Randomized trial of exclusive human milk versus preterm formula diets in extremely premature infants. J. Pediatr. 2013, 163, 1592–1595.e1. [Google Scholar] [CrossRef]
- Sullivan, S.; Schanler, R.J.; Kim, J.H.; Patel, A.L.; Trawöger, R.; Kiechl-Kohlendorfer, U.; Chan, G.M.; Blanco, C.L.; Abrams, S.; Cotten, C.M.; et al. An exclusively human milk-based diet is associated with a lower rate of necrotizing enterocolitis than a diet of human milk and bovine milk-based products. J. Pediatr. 2010, 156, 562–567.e1. [Google Scholar] [CrossRef] [Green Version]
- Lucas, A.; Gore, S.M.; Cole, T.J.; Bamford, M.F.; Dossetor, J.F.; Barr, I.; Dicarlo, L.; Cork, S.; Lucas, P.J. Multicentre trial on feeding low birthweight infants: Effects of diet on early growth. Arch. Dis. Child. 1984, 59, 722–730. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, D.L.; Gibbins, S.; Kiss, A.; Bando, N.; Brennan-Donnan, J.; Ng, E.; Campbell, D.M.; Vaz, S.; Fusch, C.; Asztalos, E.; et al. Effect of supplemental donor human milk compared with preterm formula on neurodevelopment of very low-birth-weight infants at 18 months: A randomized clinical trial. JAMA-J. Am. Med. Assoc. 2016, 316, 1897–1905. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Davies, D.P. Adequacy of expressed breast milk for early growth of preterm infants. Arch. Dis. Child. 1977, 52, 296–301. [Google Scholar] [CrossRef]
- Costa, S.; Maggio, L.; Alighieri, G.; Barone, G.; Cota, F.; Vento, G. Tolerance of preterm formula versus pasteurized donor human milk in very preterm infants: A randomized non-inferiority trial. Ital. J. Pediatr. 2018, 44, 96. [Google Scholar] [CrossRef]
- Corpeleijn, W.E.; de Waard, M.; Christmann, V.; van Goudoever, J.B.; Jansen-van der Weide, M.C.; Kooi, E.M.; Koper, J.F.; Kouwenhoven, S.M.; Lafeber, H.N.; Mank, E.; et al. Effect of Donor Milk on Severe Infections and Mortality in Very Low-Birth-Weight Infants: The Early Nutrition Study Randomized Clinical Trial. JAMA Pediatr. 2016, 170, 654–661. [Google Scholar] [CrossRef] [Green Version]
- Putet, G.; Senterre, J.; Rigo, J.; Salle, B. Nutrient balance, energy utilization, and composition of weight gain in very-low-birth-weight infants fed pooled human milk or a preterm formula. J. Pediatr. 1984, 105, 79–85. [Google Scholar] [CrossRef]
- Schanler, R.J.; Lau, C.; Hurst, N.M.; Smith, E.O. Randomized trial of donor human milk versus preterm formula as substitutes for mothers’ own milk in the feeding of extremely premature infants. Pediatrics 2005, 116, 400–406. [Google Scholar] [CrossRef]
- Tyson, J.E.; Lasky, R.E.; Mize, C.E.; Richards, C.J.; Blair-Smith, N.; Whyte, R.; Beer, A.E. Growth, metabolic response, and development in very-low-birth-weight infants fed banked human milk or enriched formula. I. Neonatal findings. J. Pediatr. 1983, 103, 95–104. [Google Scholar] [CrossRef]
- Gross, S.J. Growth and biochemical response of preterm infants fed human milk or modified infant formula. N. Engl. J. Med. 1983, 308, 237–241. [Google Scholar] [CrossRef]
- Nolan, L.S.; Parks, O.B.; Good, M. A Review of the Immunomodulating Components of Maternal Breast Milk and Protection Against Necrotizing Enterocolitis. Nutrients 2019, 12, 14. [Google Scholar] [CrossRef] [Green Version]
- Hsu, Y.C.; Chen, C.H.; Lin, M.C.; Tsai, C.R.; Liang, J.T.; Wang, T.M. Changes in preterm breast milk nutrient content in the first month. Pediatr. Neonatol. 2014, 55, 449–454. [Google Scholar] [CrossRef] [Green Version]
- Cooper, A.R.; Barnett, D.; Gentles, E.; Cairns, L.; Simpson, J.H. Macronutrient content of donor human breast milk. Arch. Dis. Child. Fetal Neonatal Ed. 2013, 98, F539–F541. [Google Scholar] [CrossRef]
- Jain, L.; Vidyasagar, D.; Xanthou, M.; Ghai, V.; Shimada, S.; Blend, M. In vivo distribution of human milk leucocytes after ingestion by newborn baboons. Arch. Dis. Child. 1989, 64, 930–933. [Google Scholar] [CrossRef] [Green Version]
- Hosea Blewett, H.J.; Cicalo, M.C.; Holland, C.D.; Field, C.J. The immunological components of human milk. Adv. Food Nutr. Res. 2008, 54, 45–80. [Google Scholar] [CrossRef] [PubMed]
- Kontopodi, E.; Boeren, S.; Stahl, B.; van Goudoever, J.B.; van Elburg, R.M.; Hettinga, K. High-Temperature Short-Time Preserves Human Milk’s Bioactive Proteins and Their Function Better Than Pasteurization Techniques With Long Processing Times. Front. Pediatr. 2021, 9, 798609. [Google Scholar] [CrossRef] [PubMed]
- Wesolowska, A.; Sinkiewicz-Darol, E.; Barbarska, O.; Strom, K.; Rutkowska, M.; Karzel, K.; Rosiak, E.; Oledzka, G.; Orczyk-Pawilowicz, M.; Rzoska, S.; et al. New Achievements in High-Pressure Processing to Preserve Human Milk Bioactivity. Front. Pediatr. 2018, 6, 323. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| First Author | Country | Year | Intervention Methods | Gestational Age, Weeks (Intervention/Control) | Birth Weight, g (Intervention/Control) | Number of Patients (Intervention/Control) | Gender (Male/Female) | JADAD Score | Outcomes | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Breast Milk Type | Sterilisation & Preservation | Control Group | |||||||||
| Corpeleijn | Netherlands | 2016 | Donated Milk | Pasteurized Holder method, 62.5 °C for 30 min | preterm formula | 28.3 ± 2.3/28.6 ± 2.2 | 1064 ± 80/1076 ± 77 | 373 (183/190) | 196/177 | 6 | Incidence of necrotizing enterocolitis (NEC), sepsis, mortality, Incidence of surgery due to NEC |
| Costa | Italy | 2018 | Donated Milk | Refrigerate at 4 °C for 24 h, pasteurized Holder method (+62.5 °C for 30 min) | Premature formula, 3.5 g of protein/100 Kcal formula (Plasmon PreZero, Plasmon, Italy). | 30 ± 1.9/30.2/1.7 | 1365 ± 332/1342 ± 275 | 70 (35/35) | 32/38 | 4 | length of hospital stays, sepsis, mortality, time to regain birthweight |
| Cristofalo | USA | 2013 | Donated Milk | Pasteurization | Bovine milk based preterm formula (BOV) | 27.7 ± 1.5/27.5 ± 2.4 | 983 ± 207/996 ± 152 | 53 (29/24) | 23/30 | 6 | length of hospital stays, incidence of NEC, sepsis, mortality, retinopathy of prematurity, weight gain, head growth, Linear growth |
| O’Connor | Canada | 2016 | Donated Milk | Pasteurized Holder method, 62.5 °C for 30 min | Premature formula (20 or 24 kcal/oz, with 3.0 g of protein/100 kcal). | 27.5 ± 2.4/27.8 ± 2.7 | 995 ± 273/996 ± 272 | 363 (181/182) | 195/168 | 7 | Incidence of NEC, sepsis, mortality, retinopathy of prematurity, weight gain, head growth, Linear growth |
| Sullivan | USA | 2010 | Donated Milk | Pasteurization | Bovine milk–based HMF, the enteral intake was 100 mL/kg/d and preterm formula | 27.1 ± 2.3/27.3 ± 2.0 | 909 ± 193/922 ± 197 | 140 (71/69) | 61/79 | 6 | length of hospital stays, incidence of NEC, sepsis, retinopathy of prematurity, bronchopulmonary dysplasia, weight gain, head growth, Linear growth |
| Schanler | USA | 2005 | Donated Milk | Holder pasteurization process (62.5 °C for 30 min), kept in −20 °C | Premature formula (100 kJ/oz; Mead Johnson Nutritional Division, Evansville, IN) | 27 ± 2/27 ± 2 | 947 ± 233/957 ± 267 | 173 (81/92) | 92/81 | 5 | Incidence of NEC, sepsis, mortality, meningitis, weight gain, head growth, Linear growth |
| Putet | France | 1984 | Donated Milk | Oral feeding was started within 24 to 48 h with pasteurized | Premature formul, containing medium-chain triglycerides (Pregallia, Gallia, France) | 30.5 ± 1.5/29.9 ± 1.5 | 1318 ± 142/1302 ± 269 | 12 (6/6) | N/A | 2 | Weight gain, head growth, Linear growth |
| Lucas | UK | 1984 | Donated Milk | N/A | Preterm formula | 30.8 ± 3.0/31.6 ± 3.1 | 1431 ± 325/1371 ± 292 | 62 (29/33) | N/A | 5 | Weight gain, head growth, Linear growth |
| Tyson | USA | 1983 | Donated Milk | Cryopreservation | Preterm formula | 29.4 ± 3.1/29.4 ± 2.4 | 1238 ± 190/1226 ± 197 | 76 (34/42) | 29/47 | 4 | Weight gain, head growth, Linear growth |
| Gross | USA | 1983 | Donated Milk | Pasteurized (Holder method, 62.5 °C for 30 min, refrigerated at −20 °C for four months | Preterm formula, 67 kilocalories per deciliter | N/A | N/A | 40 (20/20) | N/A | 4 | Weight gain, head growth, Linear growth, time to regain birthweight |
| Davies | UK | 1977 | Donated Milk | Pasteurized (Holder method, 62.5 °C for 30 min, refrigerated at −20 °C | Preterm formula | 30.8 ± 0.35/30.4 ± 0.45 | 1680 ± 0.11/1689 ± 0.11 | 28 (14/14) | N/A | 4 | Weight gain, head growth, Linear growth |
| Subgroups | Length of Hospital Stay | Incidence of NEC | ||||||||||||
| Studies, n | Participants, n | I2 | Q-Test | Mean Difference | 95% CI | p | Studies, n | Participants, n | I2 | Q-Test | Mean Difference | 95% CI | p | |
| Fortifiers | ||||||||||||||
| YES | 2 | 210 | 0 | 0.93 | 1.45 | −1.18, 4.07 | 0.28 | 2 | 539 | 0 | 0.32 | 0.87 | 0.51, 1.49 | 0.60 |
| NO | 2 | 416 | 83 | 0.01 | −4.01 | −9.44, 1.42 | 0.15 | 3 | 563 | 59 | 0.09 | 0.56 | 0.37, 0.86 | 0.01 |
| Number of participants | ||||||||||||||
| Single | 2 | 276 | 0.00 | 0.63 | 1.63 | −0.99, 4.24 | 0.22 | |||||||
| Multiple | 2 | 123 | 77.00 | 0.04 | −5.08 | −10.63, 0.48 | 0.07 | |||||||
| Subgroups | Incidence of sepsis | Mortality | ||||||||||||
| Studies, n | Participants, n | I2 | Q-test | Mean difference | 95% CI | p | Studies, n | Participants, n | I2 | Q-test | Mean difference | 95% CI | p | |
| Fortifiers | ||||||||||||||
| YES | 4 | 955 | 58 | 0.07 | 1.01 | 0.83, 1.23 | 0.93 | |||||||
| NO | 2 | 210 | 0 | 0.35 | 1.30 | 0.71, 2.39 | 0.39 | |||||||
| Birth weight | ||||||||||||||
| 1000–1500 g | 2 | 443 | 6 | 0.30 | 1.15 | 0.77, 1.73 | 0.50 | 2 | 443 | 0 | 0.55 | 1.17 | 0.70, 1.97 | 0.56 |
| <1000 g | 4 | 722 | 58 | 0.07 | 0.99 | 0.68, 1.44 | 0.94 | 3 | 582 | 0 | 0.53 | 0.81 | 0.47, 1.41 | 0.49 |
| Countries | ||||||||||||||
| European | 2 | 443 | 6 | 0.30 | 1.15 | 0.77, 1.73 | 0.50 | 2 | 443 | 0 | 0.55 | 1.17 | 0.70, 1.97 | 0.56 |
| USA | 3 | 359 | 49 | 0.14 | 0.64 | 0.36, 1.16 | 0.14 | 2 | 219 | 21 | 0.26 | 0.66 | 0.18, 2.37 | 0.52 |
| Number of centers | ||||||||||||||
| Single | 3 | 609 | 46 | 0.16 | 1.02 | 0.78, 1.32 | 0.90 | 3 | 609 | 0 | 0.84 | 1.16 | 0.71, 1.91 | 0.55 |
| Multiple | 3 | 556 | 63 | 0.07 | 1.07 | 0.81, 1.40 | 0.65 | 2 | 416 | 10 | 0.29 | 0.77 | 0.43, 1.39 | 0.39 |
| Number of participants | ||||||||||||||
| >100 | 4 | 1042 | 12 | 0.33 | 1.11 | 0.83, 1.48 | 0.50 | 3 | 902 | 0 | 0.79 | 1.01 | 0.65, 1.56 | 0.97 |
| <100 | 2 | 123 | 75 | 0.05 | 0.70 | 0.28, 1.74 | 0.44 | 2 | 123 | 43 | 0.19 | 0.60 | 0.10, 3.56 | 0.57 |
| Subgroups | Weight Gain | Head Growth | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Studies, n | Participants, n | I2 | Q-Test | Mean Difference | 95% CI | p | Studies, n | Participants, n | I2 | Q-Test | Mean Difference | 95% CI | p | |
| Fortifiers | ||||||||||||||
| YES | 3 | 545 | 0 | 0.60 | −2.37 | −3.65, −1.09 | 0.0003 | 3 | 545 | 0 | 0.42 | −0.03 | −0.09, 0.03 | 0.3 |
| NO | 6 | 507 | 100 | <0.00001 | −3.49 | −3.73, −3.24 | <0.00001 | 6 | 507 | 96 | <0.00001 | −0.07 | −0.09, −0.06 | <0.00001 |
| Birth weight | ||||||||||||||
| 1000–1500 g | 3 | 259 | 92 | <0.00001 | −4.47 | −5.55, −3.39 | <0.00001 | 3 | 259 | 58 | 0.17 | −0.27 | −0.37, −0.17 | <0.00001 |
| <1000 g | 4 | 685 | 51 | 0.11 | −0.93 | −1.21, −0.65 | <0.00001 | 4 | 685 | 0 | 0.44 | 0.00 | −0.02, 0.01 | 0.75 |
| Countries | ||||||||||||||
| European | 3 | 253 | 78 | 0.003 | −3.04 | −4.08, −1.99 | <0.00001 | 3 | 225 | 30 | 0.23 | −0.10 | −0.17, −0.03 | 0.007 |
| USA | 5 | 473 | 100 | <0.00001 | −3.49 | −3.74, −3.25 | <0.00001 | 5 | 475 | 97 | <0.00001 | −0.07 | −0.09, −0.06 | <0.00001 |
| Number of centers | ||||||||||||||
| Single | 4 | 348 | 98 | <0.00001 | −10.31 | −10.78, −9.85 | <0.00001 | 4 | 348 | 83 | 0.0005 | −0.18 | −0.20, −0.15 | <0.00001 |
| Multiple | 4 | 692 | 74 | 0.004 | −0.98 | −1.26, −0.71 | <0.00001 | 4 | 692 | 63 | 0.03 | −0.01 | −0.02, 0.01 | 0.55 |
| Number of participants | ||||||||||||||
| >100 | 4 | 685 | 51 | 0.11 | −0.93 | −1.21, −0.65 | <0.00001 | 4 | 685 | 0 | 0.44 | 0.00 | −0.02, 0.01 | 0.75 |
| <100 | 5 | 367 | 98 | <0.00001 | −9.75 | −10.19, −9.31 | <0.00001 | 5 | 341 | 72 | 0.003 | −0.18 | −0.20, −0.15 | <0.00001 |
| Date of publication | ||||||||||||||
| <2010 | 6 | 533 | 98 | <0.00001 | −9.36 | −9.79, −8.93 | <0.00001 | 6 | 507 | 70 | 0.003 | −0.18 | −0.20, −0.15 | <0.00001 |
| ≥2010 | 3 | 519 | 0 | 0.66 | −0.88 | −1.16, −0.60 | <0.00001 | 3 | 519 | 26 | 0.75 | 0.00 | −0.02, 0.01 | 0.75 |
| Subgroups | Body Length Growth | ||||||
|---|---|---|---|---|---|---|---|
| Studies, n | Participants, n | I2 | Q-Test | Mean Difference | 95% CI | p | |
| Fortifiers | |||||||
| YES | 3 | 545 | 79 | 0.01 | −0.18 | −0.30, −0.06 | 0.003 |
| NO | 6 | 507 | 89 | <0.00001 | −0.13 | −0.14, −0.11 | <0.00001 |
| Birth weight | |||||||
| 1000–1500 g | 3 | 259 | 60 | 0.06 | -0.21 | -0.29,-0.13 | <0.00001 |
| <1000 g | 4 | 685 | 78 | 0.004 | −0.07 | −0.09, −0.04 | <0.00001 |
| Countries | |||||||
| European | 3 | 151 | 48 | 0.13 | −0.14 | −0.20, −0.07 | <0.00001 |
| USA | 5 | 475 | 93 | <0.00001 | −0.13 | −0.15, −0.11 | <0.00001 |
| Number of centers | |||||||
| Single | 4 | 350 | 80 | 0.0020 | −0.17 | −0.20, −0.15 | <0.00001 |
| Multiple | 4 | 590 | 71 | 0.01 | −0.07 | −0.10, −0.05 | <0.00001 |
| Number of participants | |||||||
| >100 | 4 | 685 | 78 | 0.004 | −0.07 | −0.09, −0.04 | <0.00001 |
| <100 | 5 | 267 | 57 | 0.040 | −0.18 | −0.20, −0.15 | <0.00001 |
| Date of publication | |||||||
| <2010 | 6 | 433 | 68 | 0.004 | −0.18 | −0.20, −0.15 | <0.00001 |
| ≥2010 | 3 | 522 | 79 | 0.008 | −0.07 | −0.09, −0.04 | <0.00001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Chi, C.; Li, C.; Song, J.; Song, Z.; Wang, W.; Sun, J. Efficacy of Donated Milk in Early Nutrition of Preterm Infants: A Meta-Analysis. Nutrients 2022, 14, 1724. https://doi.org/10.3390/nu14091724
Li Y, Chi C, Li C, Song J, Song Z, Wang W, Sun J. Efficacy of Donated Milk in Early Nutrition of Preterm Infants: A Meta-Analysis. Nutrients. 2022; 14(9):1724. https://doi.org/10.3390/nu14091724
Chicago/Turabian StyleLi, Yu, Cheng Chi, Cheng Li, Junyan Song, Zanmin Song, Wenjun Wang, and Jing Sun. 2022. "Efficacy of Donated Milk in Early Nutrition of Preterm Infants: A Meta-Analysis" Nutrients 14, no. 9: 1724. https://doi.org/10.3390/nu14091724
APA StyleLi, Y., Chi, C., Li, C., Song, J., Song, Z., Wang, W., & Sun, J. (2022). Efficacy of Donated Milk in Early Nutrition of Preterm Infants: A Meta-Analysis. Nutrients, 14(9), 1724. https://doi.org/10.3390/nu14091724