
The Potential of Natural Oils to Improve Inflammatory Bowel Disease

 ,
,  , , and
, , and
Abstract
:1. Introduction
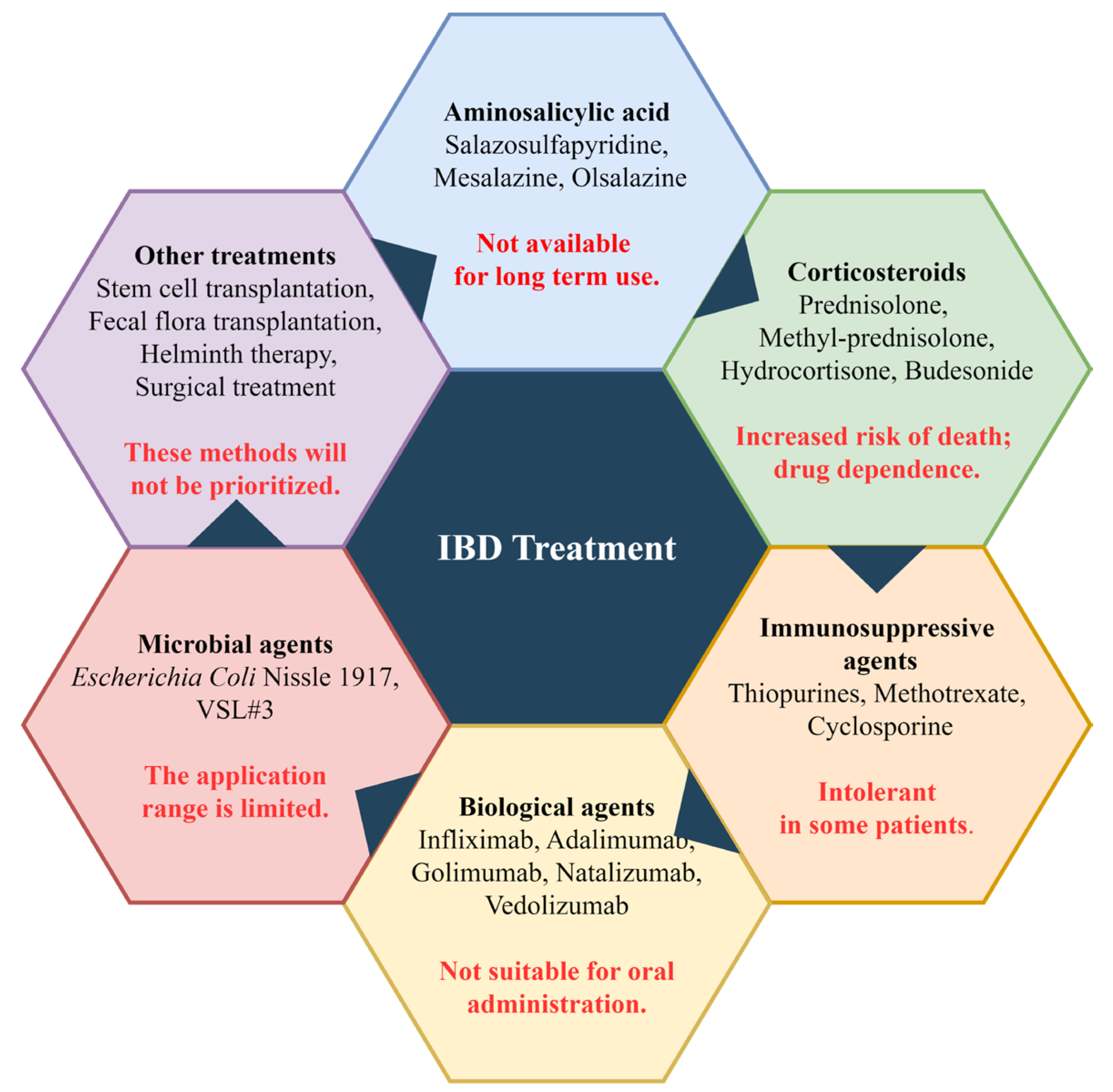
2. Current IBD Treatment Drugs and Methods
3. The Anti-Inflammatory Effects of Natural Oils
3.1. The Beneficial Effects of Plant Oils on IBD
3.1.1. Olive Oil
3.1.2. Perilla Oil
3.1.3. Garlic Oil
3.1.4. Flaxseed Oil
3.1.5. Walnut Oil
3.1.6. Yadanzi Oil
3.1.7. Grape Seed Oil
3.2. Improvement Effect of Animal Oil on Experimental IBD

{kind=link}
{kind=link}
| Oil | Source | Composition | Dosage | Model | Mechanism | Year | Reference |
|---|---|---|---|---|---|---|---|
| Yellow mealworm larva oil | Tenebrio molitor | Rich in oleic acid (45%), linoleic acid (20%), and polyunsaturated fatty acids (20%). | 50, 100 µL oral administration | DSS-induced colitis in ICR mice | Regulating the NF-κB signaling pathway to reduce inflammation. | 2022 | [110] |
| Fish oil | / | Rich in omega-3 fatty acids. | 10% | DSS-induced colitis in mice | Slowing down weight loss and colon bleeding. | 2013 | [111] |
| Emu oil | Dromaius novaehollandiae | Rich in oleic acid (42%), linoleic acid (21%), and palmitic acid (21%). | 80, 160 µL oral administration | DSS-induced chronic colitis in C57BL/6 mice | Reducing the severity of clinical and histological disease. | 2019 | [108] |
| Rich in oleic acid (42%), linoleic acid (21%), and palmitic acid (21%). | 0.5, 1 mL | DSS-induced colitis in SD rats | Improved tissue damage associated with colitis. | 2012 | [109] | ||
| Rich in docosahexaenoic acid and eicosapentaenoic acid. | 10 mL/kg | Acetic acid-induced colitis in Wistar rats | Regulating the expression of PPARγ and TNF-α. | 2015 | [107] | ||
| Rich in oleic acid (36.4%), linoleic acid (8%), and palmitic acid (6.3%). | 80, 160 µL by gavage | TNBS-induced colitis in ARC(s) mice | Reducing the severity of colitis and facial grimace scores. | 2020 | [106] | ||
| Rich in oleic acid, linoleic acid, linolenic acid, and palmitoleic acid. | 10 mL/kg BW | Indomethacin-induced colitis in Wistar albino rats | Inhibiting oxidation and improving colonic histological morphology. | 2016 | [105] |
4. The Clinical Improvement of Natural Oils in IBD
| Oil | Composition | Patients | Treatment Method | Effect | Year | References |
|---|---|---|---|---|---|---|
| Seal oil | Rich in n-3 fatty acids. | 21 had CD and 17 UC | Take 10 mL seal oil orally 3 times a day for 14 days. | Altering the fatty acid composition and n-3/n-6 ratio in blood and intestinal mucosa, improving disease activity and trend of IBD-related joint pain. | 2008 | [113,114] |
| Coconut oil | Rich in short-chain fatty acids. | DiversionColitis | 100 mL of pre-warmed coconut oil was given topically daily as a rectal enema. | After one week of treatment, abdominal pain and mucus secretion decreased. After six weeks, there was a significant improvement in inflammatory and histological symptoms. After twelve weeks, the patient had recovered. | 2018 | [117] |
| Extra virgin olive oil | 70.9% oleic acid, 9.7% linoleic acid, 14.8% palmitic acid, 2.1% stearic acid, and 0.5% alpha-linolenic acid. | 40 patients with UC | Take 50 mL orally with meals daily for 20 days. | After intervention, both erythrocyte sedimentation rate and high-sensitivity C-reactive protein were significantly reduced. Symptoms such as abdominal distension, constipation, fecal urgency, and incomplete bowel movements were alleviated. | 2020 | [116] |
| Flaxseed oil | Rich in omega-3 fatty acids, phytoestrogens, and soluble fiber. | 90 patients with UC | 10 g daily for 10 weeks. | It can significantly reduce inflammation markers, disease severity, blood pressure, and urine output in patients with colitis. | 2019 | [115] |
| Evening primrose oil | Rich in GLA (15.5%). | 43 patients with UC | Take 12 capsules per day for 1 month, then 6 capsules per day for 5 months (each capsule contains evening primrose oil 250 mg). | The red blood cell membrane concentration of dihomo-gamma-linolenic acid (DGLA) increased by 40%. | 1993 | [118] |
5. Main Pathways of Action
5.1. Regulating Intestinal Flora
5.2. Protecting the Intestinal Barrier
5.3. Reduces Inflammatory Response
5.4. Improve Oxidative Stress Levels
5.5. Regulation of Intestinal Immune Homeostasis
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aufses, A.H., Jr. The History of Crohn’s Disease. Surg. Clin. 2001, 81, 1–11. [Google Scholar] [CrossRef]
- Mulder, D.J.; Noble, A.J.; Justinich, C.J.; Duffin, J.M. A tale of two diseases: The history of inflammatory bowel disease. J. Crohn’s Colitis 2014, 8, 341–348. [Google Scholar] [CrossRef] [Green Version]
- Niu, W.; Chen, X.; Xu, R.; Dong, H.; Yang, F.; Wang, Y.; Zhang, Z.; Ju, J. Polysaccharides from natural resources exhibit great potential in the treatment of ulcerative colitis: A review. Carbohydr. Polym. 2021, 254, 117189. [Google Scholar] [CrossRef] [PubMed]
- Ramos, G.P.; Papadakis, K.A. Mechanisms of Disease: Inflammatory Bowel Diseases. Mayo Clin. Proc. 2019, 94, 155–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodson, R. Inflammatory bowel disease. Nature 2016, 540, S97. [Google Scholar] [CrossRef] [Green Version]
- Alatab, S.; Sepanlou, S.G.; Ikuta, K.; Vahedi, H.; Bisignano, C.; Safiri, S.; Sadeghi, A.; Nixon, M.R.; Abdoli, A.; Abolhassani, H.; et al. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 17–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, S.C.; Tang, W.; Ching, J.Y.; Wong, M.; Chow, C.M.; Hui, A.J.; Wong, T.C.; Leung, V.K.; Tsang, S.W.; Yu, H.H.; et al. Incidence and Phenotype of Inflammatory Bowel Disease Based on Results From the Asia-Pacific Crohn’s and Colitis Epidemiology Study. Gastroenterology 2013, 145, 158–165.e2. [Google Scholar] [CrossRef]
- Yang, Y.; Owyang, C.; Wu, G.D. East Meets West: The Increasing Incidence of Inflammatory Bowel Disease in Asia as a Paradigm for Environmental Effects on the Pathogenesis of Immune-Mediated Disease. Gastroenterology 2016, 151, e1–e5. [Google Scholar] [CrossRef] [Green Version]
- Macpherson, A.J.; Harris, N.L. Interactions between commensal intestinal bacteria and the immune system. Nat. Rev. Immunol. 2004, 4, 478–485. [Google Scholar] [CrossRef]
- Mirkov, M.U.; Verstockt, B.; Cleynen, I. Genetics of inflammatory bowel disease: Beyond NOD2. Lancet Gastroenterol. Hepatol. 2017, 2, 224–234. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, D.; Yan, W. Treatment Effects of Natural Products on Inflammatory Bowel Disease In Vivo and Their Mechanisms: Based on Animal Experiments. Nutrients 2023, 15, 1031. [Google Scholar] [CrossRef]
- Pan, X.; Yin, M.; Guo, M.; Niu, X.; Han, L. The latest progress of natural food polysaccharides preventing ulcerative colitis by regulating intestinal microbiota. J. Funct. Foods 2022, 96, 105201. [Google Scholar] [CrossRef]
- Fernández-Tomé, S.; Hernández-Ledesma, B.; Chaparro, M.; Indiano-Romacho, P.; Bernardo, D.; Gisbert, J.P. Role of food proteins and bioactive peptides in inflammatory bowel disease. Trends Food Sci. Technol. 2019, 88, 194–206. [Google Scholar] [CrossRef]
- Ma, Y.; Yan, W.; Ding, S.; Fei, Y.; Liu, G.; Fang, J. Effects of Bioactive Peptide on Inflammatory Bowel Disease, Focus on Signal Transduction and Intestinal Microbiota. Curr. Pharm. Des. 2018, 24, 2782–2788. [Google Scholar] [CrossRef]
- Dijkstra, G.; Moshage, H.; Jansen, P.L.M. Blockade of NF-κB Activation and Donation of Nitric Oxide: New Treatment Options in Inflammatory Bowel Disease? Scand. J. Gastroenterol. 2002, 37, 37–41. [Google Scholar] [CrossRef]
- Sninsky, C.A.; Cort, D.H.; Shanahan, F.; Powers, B.J.; Sessions, J.T.; Pruitt, R.E.; Jacobs, W.H.; Lo, S.K.; Targan, S.R.; Cerda, J.J.; et al. Oral Mesalamine (Asacol) for Mildly to Moderately Active Ulcerative Colitis. Ann. Intern. Med. 1991, 115, 350–355. [Google Scholar] [CrossRef]
- Kane, S.; Huo, D.; Aikens, J.; Hanauer, S. Medication nonadherence and the outcomes of patients with quiescent ulcerative colitis. Am. J. Med. 2003, 114, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Dubois-Camacho, K.; Ottum, P.A.; Franco-Muñoz, D.; De la Fuente, M.; Torres-Riquelme, A.; Díaz-Jiménez, D.; Olivares-Morales, M.; Astudillo, G.; Quera, R.; Hermoso, M.A. Glucocorticosteroid therapy in inflammatory bowel diseases: From clinical practice to molecular biology. World J. Gastroenterol. 2017, 23, 6628. [Google Scholar] [CrossRef] [PubMed]
- Dorrington, A.M.; Selinger, C.P.; Parkes, G.C.; Smith, M.; Pollok, R.C.; Raine, T. The Historical Role and Contemporary Use of Corticosteroids in Inflammatory Bowel Disease. J. Crohn’s Colitis 2020, 14, 1316–1329. [Google Scholar] [CrossRef]
- Kim, K.-U.; Kim, J.; Kim, W.-H.; Min, H.; Choi, C.H. Treatments of inflammatory bowel disease toward personalized medicine. Arch. Pharmacal Res. 2021, 44, 293–309. [Google Scholar] [CrossRef]
- Sattler, L.; Hanauer, S.B.; Malter, L. Immunomodulatory Agents for Treatment of Patients with Inflammatory Bowel Disease (Review safety of anti-TNF, Anti-Integrin, Anti IL-12/23, JAK Inhibition, Sphingosine 1-Phosphate Receptor Modulator, Azathioprine/6-MP and Methotrexate). Curr. Gastroenterol. Rep. 2021, 23, 30. [Google Scholar] [CrossRef]
- Tominaga, K.; Sugaya, T.; Tanaka, T.; Kanazawa, M.; Iijima, M.; Irisawa, A. Thiopurines: Recent topics and their role in the treatment of inflammatory bowel diseases. Front. Pharmacol. 2021, 11, 582291. [Google Scholar] [CrossRef] [PubMed]
- Tedesco, D.; Haragsim, L. Cyclosporine: A Review. J. Transplant. 2012, 2012, 230386. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Michalowski, C.B.; Beloqui, A. Oral delivery of biologics in inflammatory bowel disease treatment. Front. Bioeng. Biotechnol. 2021, 9, 675194. [Google Scholar] [CrossRef]
- Elhag, D.A.; Kumar, M.; Saadaoui, M.; Akobeng, A.K.; Al-Mudahka, F.; Elawad, M.; Al Khodor, S. Inflammatory Bowel Disease Treatments and Predictive Biomarkers of Therapeutic Response. Int. J. Mol. Sci. 2022, 23, 6966. [Google Scholar] [CrossRef]
- Queiroz, N.S.F.; Regueiro, M. Safety considerations with biologics and new inflammatory bowel disease therapies. Curr. Opin. Gastroenterol. 2020, 36, 257–264. [Google Scholar] [CrossRef]
- Derikx, L.A.A.P.; Dieleman, L.A.; Hoentjen, F. Probiotics and prebiotics in ulcerative colitis. Best Pract. Res. Clin. Gastroenterol. 2016, 30, 55–71. [Google Scholar] [CrossRef]
- Zhang, H.-M.; Yuan, S.; Meng, H.; Hou, X.-T.; Li, J.; Xue, J.-C.; Li, Y.; Wang, Q.; Nan, J.-X.; Jin, X.-J.; et al. Stem Cell-Based Therapies for Inflammatory Bowel Disease. Int. J. Mol. Sci. 2022, 23, 8494. [Google Scholar] [CrossRef]
- Lalu, M.M.; McIntyre, L.; Pugliese, C.; Fergusson, D.; Winston, B.W.; Marshall, J.C.; Granton, J.; Stewart, D.J. Safety of Cell Therapy with Mesenchymal Stromal Cells (SafeCell): A Systematic Review and Meta-Analysis of Clinical Trials. PLoS ONE 2012, 7, e47559. [Google Scholar] [CrossRef]
- Guo, B.; Harstall, C.; Louie, T.; Veldhuyzen van Zanten, S.; Dieleman, L.A. Systematic review: Faecal transplantation for the treatment of Clostridium difficile-associated disease. Aliment. Pharmacol. Ther. 2012, 35, 865–875. [Google Scholar] [CrossRef] [PubMed]
- Hunter, M.M.; McKay, D.M. Helminths as therapeutic agents for inflammatory bowel disease. Aliment. Pharmacol. Ther. 2004, 19, 167–177. [Google Scholar] [CrossRef]
- Dignass, A.; Lindsay, J.O.; Sturm, A.; Windsor, A.; Colombel, J.-F.; Allez, M.; D’Haens, G.; D’Hoore, A.; Mantzaris, G.; Novacek, G.; et al. Second European evidence-based consensus on the diagnosis and management of ulcerative colitis Part 2: Current management. J. Crohn’s Colitis 2012, 6, 991–1030. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Shen, Y.; Tang, N.; Zhu, J.; Xiao, J.; Cong, R.; Zhang, H.; Wu, G.; Qi, X. Ameliorative Role of Cabernet Sauvignon Seed Oil on Hyperlipidemia, Inflammation, and Oxidative Stress in Mice. Eur. J. Lipid Sci. Technol. 2019, 121, 1800454. [Google Scholar] [CrossRef]
- Skrzypczak-Wiercioch, A.; Sałat, K. Lipopolysaccharide-Induced Model of Neuroinflammation: Mechanisms of Action, Research Application and Future Directions for Its Use. Molecules 2022, 27, 5480. [Google Scholar] [CrossRef]
- El Kamouni, S.; El Kebbaj, R.; Andreoletti, P.; El Ktaibi, A.; Rharrassi, I.; Essamadi, A.; El Kebbaj, M.h.S.; Mandard, S.; Latruffe, N.; Vamecq, J.; et al. Protective Effect of Argan and Olive Oils against LPS-Induced Oxidative Stress and Inflammation in Mice Livers. Int. J. Mol. Sci. 2017, 18, 2181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, C.; Cao, Y.; Zhang, Z.; Nie, D.; Li, Y. Cinnamon and Eucalyptus Oils Suppress the Inflammation Induced by Lipopolysaccharide In Vivo. Molecules 2021, 26, 7410. [Google Scholar] [CrossRef] [PubMed]
- Ambulay, J.P.; Rojas, P.A.; Timoteo, O.S.; Barreto, T.V.; Colarossi, A. Effect of the emulsion of Sacha Inchi (Plukenetia huayabambana) oil on oxidative stress and inflammation in rats induced to obesity. J. Funct. Foods 2020, 64, 103631. [Google Scholar] [CrossRef]
- Fu, J.; Zeng, C.; Zeng, Z.; Wang, B.; Gong, D. Cinnamomum camphora Seed Kernel Oil Ameliorates Oxidative Stress and Inflammation in Diet-Induced Obese Rats. J. Food Sci. 2016, 81, H1295–H1300. [Google Scholar] [CrossRef]
- Ilak Peršurić, A.S.; Težak Damijanić, A. Connections between Healthy Behaviour, Perception of Olive Oil Health Benefits, and Olive Oil Consumption Motives. Sustainability 2021, 13, 7630. [Google Scholar] [CrossRef]
- Celano, R.; Piccinelli, A.L.; Pugliese, A.; Carabetta, S.; di Sanzo, R.; Rastrelli, L.; Russo, M. Insights into the Analysis of Phenolic Secoiridoids in Extra Virgin Olive Oil. J. Agric. Food Chem. 2018, 66, 6053–6063. [Google Scholar] [CrossRef]
- Pozzetti, L.; Ferrara, F.; Marotta, L.; Gemma, S.; Butini, S.; Benedusi, M.; Fusi, F.; Ahmed, A.; Pomponi, S.; Ferrari, S.; et al. Extra Virgin Olive Oil Extracts of Indigenous Southern Tuscany Cultivar Act as Anti-Inflammatory and Vasorelaxant Nutraceuticals. Antioxidants 2022, 11, 437. [Google Scholar] [CrossRef]
- Eidi, A.; Moghadam-kia, S.; Moghadam, J.Z.; Eidi, M.; Rezazadeh, S. Antinociceptive and anti-inflammatory effects of olive oil (Olea europeae L.) in mice. Pharm. Biol. 2012, 50, 332–337. [Google Scholar] [CrossRef]
- Otrante, A.; Trigui, A.; Walha, R.; Berrougui, H.; Fulop, T.; Khalil, A. Extra Virgin Olive Oil Prevents the Age-Related Shifts of the Distribution of HDL Subclasses and Improves Their Functionality. Nutrients 2021, 13, 2235. [Google Scholar] [CrossRef] [PubMed]
- Tanideh, N.; Sadeghi, F.; Amanat, S.; Firoozi, D.; Noorafshan, A.; Iraji, A.; Koohi-Hosseinabadi, O. Protection by pure and genistein fortified extra virgin olive oil, canola oil, and rice bran oil against acetic acid-induced ulcerative colitis in rats. Food Funct. 2020, 11, 860–870. [Google Scholar] [CrossRef] [PubMed]
- Takashima, T.; Sakata, Y.; Iwakiri, R.; Shiraishi, R.; Oda, Y.; Inoue, N.; Nakayama, A.; Toda, S.; Fujimoto, K. Feeding with olive oil attenuates inflammation in dextran sulfate sodium-induced colitis in rat. J. Nutr. Biochem. 2014, 25, 186–192. [Google Scholar] [CrossRef]
- Sánchez-Fidalgo, S.; Sánchez de Ibargüen, L.; Cárdeno, A.; Alarcón de la Lastra, C. Influence of extra virgin olive oil diet enriched with hydroxytyrosol in a chronic DSS colitis model. Eur. J. Nutr. 2012, 51, 497–506. [Google Scholar] [CrossRef]
- Sánchez-Fidalgo, S.; Cárdeno, A.; Sánchez-Hidalgo, M.; Aparicio-Soto, M.; Villegas, I.; Rosillo, M.A.; de la Lastra, C.A. Dietary unsaponifiable fraction from extra virgin olive oil supplementation attenuates acute ulcerative colitis in mice. Eur. J. Pharm. Sci. 2013, 48, 572–581. [Google Scholar] [CrossRef]
- Asif, M. Health effects of omega-3,6,9 fatty acids: Perilla frutescens is a good example of plant oils. Orient. Pharm. Exp. Med. 2011, 11, 51–59. [Google Scholar] [CrossRef] [Green Version]
- Tantipaiboonwong, P.; Chaiwangyen, W.; Suttajit, M.; Kangwan, N.; Kaowinn, S.; Khanaree, C.; Punfa, W.; Pintha, K. Molecular Mechanism of Antioxidant and Anti-Inflammatory Effects of Omega-3 Fatty Acids in Perilla Seed Oil and Rosmarinic Acid Rich Fraction Extracted from Perilla Seed Meal on TNF-α Induced A549 Lung Adenocarcinoma Cells. Molecules 2021, 26, 6757. [Google Scholar] [CrossRef]
- Paradee, N.; Koonyosying, P.; Kusirisin, W.; Janthip, R.; Kanjanapothi, D.; Pattanapanyasat, K.; Srichairatanakool, S. Analgesic, anti-inflammatory and anti-ulcer properties of Thai Perilla frutescence fruit oil in animals. Biosci. Rep. 2021, 41, BSR20203166. [Google Scholar] [CrossRef]
- Thomas, S.S.; Cha, Y.-S.; Kim, K.-A. Perilla Oil Alleviates High-Fat Diet-Induced Inflammation in the Colon of Mice by Suppressing Nuclear Factor-Kappa B Activation. J. Med. Food 2020, 23, 818–826. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.S.; Cha, Y.-S.; Kim, K.-A. Protective Effect of Diet-Supplemented and Endogenously Produced Omega-3 Fatty Acids against HFD-Induced Colon Inflammation in Mice. Foods 2022, 11, 2124. [Google Scholar] [CrossRef] [PubMed]
- Kangwan, N.; Pintha, K.; Khanaree, C.; Kongkarnka, S.; Chewonarin, T.; Suttajit, M. Anti-inflammatory effect of Perilla frutescens seed oil rich in omega-3 fatty acid on dextran sodium sulfate-induced colitis in mice. Res. Pharm. Sci. 2021, 16, 464–473. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.S.; Cha, Y.-S.; Kim, K.-A. Protective Effect of Perilla Oil Against Dextran Sodium Sulfate-Induced Colitis in Mice Challenged with a High-Fat Diet. J. Med. Food 2022, 25, 1021–1028. [Google Scholar] [CrossRef]
- Li, W.-R.; Shi, Q.-S.; Liang, Q.; Huang, X.-M.; Chen, Y.-B. Antifungal effect and mechanism of garlic oil on Penicillium funiculosum. Appl. Microbiol. Biotechnol. 2014, 98, 8337–8346. [Google Scholar] [CrossRef] [PubMed]
- Ko, J.-W.; Jeong, S.-H.; Kwon, H.-J.; Shin, N.-R.; Seo, Y.-S.; Kim, J.-C.; Shin, I.-S.; Kim, J.-S. Preventive Effect of Garlic Oil and Its Organosulfur Component Diallyl-Disulfide on Cigarette Smoke-Induced Airway Inflammation in Mice. Nutrients 2018, 10, 1659. [Google Scholar] [CrossRef] [Green Version]
- Warriar, P.; Barve, K.; Prabhakar, B. Anti-Arthritic Effect of Garcinol Enriched Fraction Against Adjuvant Induced Arthritis. Recent Pat. Inflamm. Allergy Drug Discov. 2019, 13, 49–56. [Google Scholar] [CrossRef]
- Balaha, M.; Kandeel, S.; Elwan, W. Garlic oil inhibits dextran sodium sulfate-induced ulcerative colitis in rats. Life Sci. 2016, 146, 40–51. [Google Scholar] [CrossRef]
- Tanrıkulu, Y.; Şen Tanrıkulu, C.; Kılınç, F.; Can, M.; Köktürk, F. Effects of garlic oil (allium sativum) on acetic acid-induced colitis in rats: Garlic oil and experimental colitis. Ulus Travma Acil Cerrahi Derg 2020, 26, 503–508. [Google Scholar] [CrossRef]
- Bekhit, A.E.-D.A.; Shavandi, A.; Jodjaja, T.; Birch, J.; Teh, S.; Mohamed Ahmed, I.A.; Al-Juhaimi, F.Y.; Saeedi, P.; Bekhit, A.A. Flaxseed: Composition, detoxification, utilization, and opportunities. Biocatal. Agric. Biotechnol. 2018, 13, 129–152. [Google Scholar] [CrossRef]
- Carter, J.F. Potential of flaxseed and flaxseed oil in baked goods and other products in human nutrition. Cereal Foods World (USA) 1993, 38, 753–759. [Google Scholar]
- Moallem, U.; Lehrer, H.; Livshits, L.; Zachut, M. The effects of omega-3 α-linolenic acid from flaxseed oil supplemented to high-yielding dairy cows on production, health, and fertility. Livest. Sci. 2020, 242, 104302. [Google Scholar] [CrossRef]
- Tyagi, A.; Kumar, U.; Reddy, S.; Santosh, V.S.; Mohammed, S.B.; Ehtesham, N.Z.; Ibrahim, A. Attenuation of colonic inflammation by partial replacement of dietary linoleic acid with α-linolenic acid in a rat model of inflammatory bowel disease. Br. J. Nutr. 2012, 108, 1612–1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Q.; Ma, L.; Zhao, W.; Zhao, W.; Han, X.; Niu, J.; Li, R.; Zhao, C. Flaxseed oil alleviates dextran sulphate sodium-induced ulcerative colitis in rats. J. Funct. Foods 2020, 64, 103602. [Google Scholar] [CrossRef]
- Palla, A.H.; Gilani, A.-u.-H.; Bashir, S.; Ur Rehman, N. Multiple Mechanisms of Flaxseed: Effectiveness in Inflammatory Bowel Disease. Evid.-Based Complement. Altern. Med. 2020, 2020, 7974835. [Google Scholar] [CrossRef]
- Poggetti, L.; Ferfuia, C.; Chiabà, C.; Testolin, R.; Baldini, M. Kernel oil content and oil composition in walnut (Juglans regia L.) accessions from north-eastern Italy. J. Sci. Food Agric. 2018, 98, 955–962. [Google Scholar] [CrossRef] [Green Version]
- Hayes, D.; Angove, M.J.; Tucci, J.; Dennis, C. Walnuts (Juglans regia) Chemical Composition and Research in Human Health. Crit. Rev. Food Sci. Nutr. 2016, 56, 1231–1241. [Google Scholar] [CrossRef]
- Willis, L.M.; Bielinski, D.F.; Fisher, D.R.; Matthan, N.R.; Joseph, J.A. Walnut Extract Inhibits LPS-induced Activation of Bv-2 Microglia via Internalization of TLR4: Possible Involvement of Phospholipase D2. Inflammation 2010, 33, 325–333. [Google Scholar] [CrossRef]
- Laubertová, L.; Koňariková, K.; Gbelcová, H.; Ďuračková, Z.; Žitňanová, I. Effect of walnut oil on hyperglycemia-induced oxidative stress and pro-inflammatory cytokines production. Eur. J. Nutr. 2015, 54, 291–299. [Google Scholar] [CrossRef]
- Bartoszek, A.; Makaro, A.; Bartoszek, A.; Kordek, R.; Fichna, J.; Salaga, M. Walnut Oil Alleviates Intestinal Inflammation and Restores Intestinal Barrier Function in Mice. Nutrients 2020, 12, 1302. [Google Scholar] [CrossRef]
- Miao, F.; Shan, C.; Ma, T.; Geng, S.; Ning, D. Walnut oil alleviates DSS–induced colitis in mice by inhibiting NLRP3 inflammasome activation and regulating gut microbiota. Microb. Pathog. 2021, 154, 104866. [Google Scholar] [CrossRef] [PubMed]
- Sornwatana, T.; Roytrakul, S.; Wetprasit, N.; Ratanapo, S. Brucin, an antibacterial peptide derived from fruit protein of Fructus Bruceae, Brucea javanica (L.) Merr. Lett. Appl. Microbiol. 2013, 57, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Xu, H.-X.; Dou, Y.-X.; Huang, Q.-H.; Xian, Y.-F.; Lin, Z.-X. Major Constituents From Brucea javanica and Their Pharmacological Actions. Front. Pharmacol. 2022, 13, 853119. [Google Scholar] [CrossRef]
- Su, B.-N.; Chang, L.C.; Park, E.J.; Cuendet, M.; Santarsiero, B.D.; Mesecar, A.D.; Mehta, R.G.; Fong, H.H.S.; Pezzuto, J.M.; Kinghorn, A.D. Bioactive constituents of the seeds of Brucea javanica. Planta Med. 2002, 68, 730–733. [Google Scholar] [CrossRef] [PubMed]
- Yoon, B.K.; Lim, Z.Y.; Jeon, W.-Y.; Cho, N.-J.; Kim, J.H.; Jackman, J.A. Medicinal Activities and Nanomedicine Delivery Strategies for Brucea javanica Oil and Its Molecular Components. Molecules 2020, 25, 5414. [Google Scholar] [CrossRef]
- Huang, Y.-F.; Zhou, J.-T.; Qu, C.; Dou, Y.-X.; Huang, Q.-H.; Lin, Z.-X.; Xian, Y.-F.; Xie, J.-H.; Xie, Y.-L.; Lai, X.-P.; et al. Anti-inflammatory effects of Brucea javanica oil emulsion by suppressing NF-κB activation on dextran sulfate sodium-induced ulcerative colitis in mice. J. Ethnopharmacol. 2017, 198, 389–398. [Google Scholar] [CrossRef]
- Zheng, X.; Mai, L.; Wang, T.; Xu, Y.; Su, Z.; Chen, J.; Zeng, H.; Xie, Y. Brusatol-Enriched Brucea javanica Oil Ameliorated Dextran Sulfate Sodium-Induced Colitis in Mice: Involvement of NF-κB and RhoA/ROCK Signaling Pathways. BioMed Res. Int. 2021, 2021, 5561221. [Google Scholar] [CrossRef]
- Garavaglia, J.; Markoski, M.M.; Oliveira, A.; Marcadenti, A. Grape seed oil compounds: Biological and chemical actions for health. Nutr. Metab. Insights 2016, 9, 59–64. [Google Scholar] [CrossRef] [Green Version]
- Martin, M.E.; Grao-Cruces, E.; Millan-Linares, M.C.; Montserrat-de la Paz, S. Grape (Vitis vinifera L.) Seed Oil: A Functional Food from the Winemaking Industry. Foods 2020, 9, 1360. [Google Scholar] [CrossRef] [PubMed]
- Niknami, E.; Sajjadi, S.-E.; Talebi, A.; Minaiyan, M. Protective effect of Vitis vinifera (black grape) seed extract and oil on acetic acid-induced colitis in rats. Int. J. Prev. Med. 2020, 11, 102. [Google Scholar] [PubMed]
- Hosseinzadeh, F.; Salehi, M.; Tanideh, N.; Mehrabani, D.; Sayarifard, A.; Sedighi, A. The Healing effect of grape seed oil enema with or without sesame oil in acetic acid induced ulcerative colitis of rats. World J. Plast. Surg. 2017, 6, 176–182. [Google Scholar] [PubMed]
- Lazcano-Silveira, R.; Jia, X.; Liu, K.; Liu, H.; Li, X.; Hui, M. Carbon 60 dissolved in grapeseed oil inhibits dextran sodium sulfate-induced experimental colitis. J. Inflamm. Res. 2022, 15, 4185–4198. [Google Scholar] [CrossRef] [PubMed]
- Naouar, M.S.; Mekki, L.Z.; Charfi, L.; Boubaker, J.; Filali, A. Preventive and curative effect of Pistacia lentiscus oil in experimental colitis. Biomed. Pharmacother. 2016, 83, 577–583. [Google Scholar] [CrossRef]
- Lee, W.-T.; Tung, Y.-T.; Wu, C.-C.; Tu, P.-S.; Yen, G.-C. Camellia Oil (Camellia oleifera Abel.) Modifies the Composition of Gut Microbiota and Alleviates Acetic Acid-Induced Colitis in Rats. J. Agric. Food Chem. 2018, 66, 7384–7392. [Google Scholar] [CrossRef]
- Wu, C.-C.; Tung, Y.-T.; Chen, S.-Y.; Lee, W.-T.; Lin, H.-T.; Yen, G.-C. Anti-Inflammatory, Antioxidant, and Microbiota-Modulating Effects of Camellia Oil from Camellia brevistyla on Acetic Acid-Induced Colitis in Rats. Antioxidants 2020, 9, 58. [Google Scholar] [CrossRef] [Green Version]
- Moreno, L.G.; Evangelista-Silva, P.H.; Santos, E.C.; Prates, R.P.; Lima, A.C.; Mendes, M.F.; Ottone, V.O.; Ottoni, M.H.F.; Pereira, W.F.; Melo, G.E.B.A.; et al. Pequi Oil, a MUFA/Carotenoid-Rich Oil, Exhibited Protective Effects against DSS-Induced Ulcerative Colitis in Mice. Eur. J. Lipid Sci. Technol. 2021, 123, 2000332. [Google Scholar] [CrossRef]
- Xu, Z.; Tang, H.; Huang, F.; Qiao, Z.; Wang, X.; Yang, C.; Deng, Q. Algal Oil Rich in n-3 PUFA Alleviates DSS-Induced Colitis via Regulation of Gut Microbiota and Restoration of Intestinal Barrier. Front. Microbiol. 2020, 11, 615404. [Google Scholar] [CrossRef]
- Genc, Z.; Yarat, A.; Tunali-Akbay, T.; Sener, G.; Cetinel, S.; Pisiriciler, R.; Caliskan-Ak, E.; Altıntas, A.; Demirci, B. The Effect of Stinging Nettle (Urtica dioica) Seed Oil on Experimental Colitis in Rats. J. Med. Food 2011, 14, 1554–1561. [Google Scholar] [CrossRef]
- Bujňáková, D.; Juhás, Š.; Faix, Š. The anti-translocation and anti-inflammatory effect of cinnamon oil in mice with TNBS induced colitis. Biologia 2013, 68, 1000–1003. [Google Scholar] [CrossRef]
- Alliger, K.; Khalil, M.; König, B.; Weisenburger, S.; Koch, E.; Engel, M. Menthacarin attenuates experimental colitis. Phytomedicine 2020, 77, 153212. [Google Scholar] [CrossRef]
- Liu, C.; He, Y.-X.; Zhang, J.-N.; Yang, F.; Wang, S.-Y.; Hu, J.-L.; Yu, Y. Angelica oil restores the intestinal barrier function by suppressing S100A8/A9 signalling in mice with ulcerative colitis. Phytomedicine 2023, 108, 154490. [Google Scholar] [CrossRef] [PubMed]
- Abu-Gharbieh, E.; Bayoumi, F.A.; Ahmed, N.G. Alleviation of Antioxidant Defense System by Ozonized Olive Oil in DNBS-Induced Colitis in Rats. Mediat. Inflamm. 2014, 2014, 967205. [Google Scholar] [CrossRef] [Green Version]
- Isik, F.; Tunali Akbay, T.; Yarat, A.; Genc, Z.; Pisiriciler, R.; Caliskan-Ak, E.; Cetinel, S.; Altıntas, A.; Sener, G. Protective Effects of Black Cumin (Nigella sativa) Oil on TNBS-Induced Experimental Colitis in Rats. Dig. Dis. Sci. 2011, 56, 721–730. [Google Scholar] [CrossRef]
- Camuesco, D.e.; Gálvez, J.; Nieto, A.; Comalada, M.n.; Rodríguez-Cabezas, M.E.; Concha, A.; Xaus, J.; Zarzuelo, A. Dietary Olive Oil Supplemented with Fish Oil, Rich in EPA and DHA (n-3) Polyunsaturated Fatty Acids, Attenuates Colonic Inflammation in Rats with DSS-Induced Colitis. J. Nutr. 2005, 135, 687–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coursodon-Boyiddle, C.F.; Snarrenberg, C.L.; Adkins-Rieck, C.K.; Bassaganya-Riera, J.; Hontecillas, R.; Lawrence, P.; Brenna, J.T.; Jouni, Z.E.; Dvorak, B. Pomegranate seed oil reduces intestinal damage in a rat model of necrotizing enterocolitis. Am. J. Physiol.-Gastrointest. Liver Physiol. 2012, 303, G744–G751. [Google Scholar] [CrossRef] [Green Version]
- Mohamed, M.E.; Elsayed, S.A.; Madkor, H.R.; Eldien, H.M.S.; Mohafez, O.M. Yarrow oil ameliorates ulcerative colitis in mice model via regulating the NF-κB and PPAR-γ pathways. Intest. Res. 2021, 19, 194–205. [Google Scholar] [CrossRef]
- Park, J.-S.; Choi, J.; Hwang, S.-H.; Kim, J.-K.; Kim, E.-K.; Lee, S.-Y.; Lee, B.-I.; Park, S.-H.; Cho, M.-L. Cottonseed Oil Protects Against Intestinal Inflammation in Dextran Sodium Sulfate-Induced Inflammatory Bowel Disease. J. Med. Food 2019, 22, 672–679. [Google Scholar] [CrossRef]
- Reddy, K.V.K.; Maheswaraiah, A.; Naidu, K.A. Rice bran oil and n-3 fatty acid-rich garden cress (Lepidium sativum) seed oil attenuate murine model of ulcerative colitis. Int. J. Color. Dis. 2014, 29, 267–269. [Google Scholar] [CrossRef]
- Kang, J.; Park, J.; Seo, J.-K.; Choi, W.; Choi, S.; Kim, J.-H.; Lee, I.-A. Intestinal anti-inflammatory activity of Ulva ohnoi oil in DSS-induced experimental mouse model. Sci. Rep. 2021, 11, 15087. [Google Scholar] [CrossRef] [PubMed]
- Patil, N.R.; Rasal, V.P.; Malabade, R.H. Screening of mandarin oil on indomethcin induced inflammatory bowel disease in wistar rats. Indian J. Pharm. Educ. Res. 2014, 48, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Barbosa, M.M.C.; Vicentini, F.A.; Castro-Ghizoni, C.V.; Lameira, O.A.; Sa-Nakanishi, A.B.; Bracht, L.; Peralta, R.M.; Natali, M.R.M.; Bracht, A.; Comar, J.F. Copaiba Oil Decreases Oxidative Stress and Inflammation But not Colon Damage in Rats with TNBS-Induced Colitis. Endocr. Metab. Immune Disord.-Drug Targets 2018, 18, 268–280. [Google Scholar] [CrossRef]
- Whitehouse, M.W.; Turner, A.G.; Davis, C.K.C.; Roberts, M.S. Emu oil(s): A source of non-toxic transdermal anti-inflammatory agents in aboriginal medicine. Inflamm. Pharmacol. 1998, 6, 1–8. [Google Scholar] [CrossRef]
- Vemu, B.; Selvasubramanian, S.; Pandiyan, V. Anti-inflammatory Activity of Emu Oil in Indomethacin Induced Inflammatory Bowel Disease in Rats. Proc. Natl. Acad. Sci. India Sect. B Biol. Sci. 2015, 85, 831–837. [Google Scholar] [CrossRef]
- Lindsay, R.J.; Geier, M.S.; Yazbeck, R.; Butler, R.N.; Howarth, G.S. Orally administered emu oil decreases acute inflammation and alters selected small intestinal parameters in a rat model of mucositis. Br. J. Nutr. 2010, 104, 513–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vemu, B.; Selvasubramanian, S.; Pandiyan, V. Emu oil offers protection in Crohn’s disease model in rats. BMC Complement. Altern. Med. 2016, 16, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, C.J.; Howarth, G.S.; Chartier, L.C.; Trinder, D.; Lawrance, I.C.; Huang, L.S.; Mashtoub, S. Orally administered emu oil attenuates disease in a mouse model of Crohn’s-like colitis. Exp. Biol. Med. 2020, 245, 1697–1707. [Google Scholar] [CrossRef]
- Sethuraman, S.N.; Swaminathan, S.; Nelson, S.B.; Palaninathan, P.S.; Gopalan, T.K.; Velayudham, P. Modulation of PPARγ and TNFα by emu oil and glycyrrhizin in ulcerative colitis. Inflammopharmacology 2015, 23, 47–56. [Google Scholar] [CrossRef]
- Safaeian, R.; Howarth, G.S.; Lawrance, I.C.; Trinder, D.; Mashtoub, S. Emu oil reduces disease severity in a mouse model of chronic ulcerative colitis. Scand. J. Gastroenterol. 2019, 54, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Abimosleh, S.M.; Lindsay, R.J.; Butler, R.N.; Cummins, A.G.; Howarth, G.S. Emu Oil Increases Colonic Crypt Depth in a Rat Model of Ulcerative Colitis. Dig. Dis. Sci. 2012, 57, 887–896. [Google Scholar] [CrossRef]
- Park, B.M.; Lee, J.; Jung, B.G.; Lee, B.J. Validation of the Anti-Inflammatory Effect of Tenebrio Molitor Larva Oil in a Colitis Mouse Model. Folia Biol. 2022, 68, 50–58. [Google Scholar]
- Somara, S.; Zakhem, E.; Raghavan, S.; Gilmont, R.R.; Bitar, K.N. FISH Oil Aids in Treatment of Colonic Dysmotility in Mice With DSS-Induced Colitis. Gastroenterology 2013, 5, S-672–S–673. [Google Scholar] [CrossRef]
- Valatas, V.; Bamias, G.; Kolios, G. Experimental colitis models: Insights into the pathogenesis of inflammatory bowel disease and translational issues. Eur. J. Pharmacol. 2015, 759, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Brunborg, L.A.; Madland, T.M.; Lind, R.A.; Arslan, G.; Berstad, A.; Frøyland, L. Effects of short-term oral administration of dietary marine oils in patients with inflammatory bowel disease and joint pain: A pilot study comparing seal oil and cod liver oil. Clin. Nutr. 2008, 27, 614–622. [Google Scholar] [CrossRef]
- Arslan, G.; Bjorkkjaer, T.; Brunborg, L.A.; Lind, R.; Valen, M.; Brun, J.; Froyland, L.; Berstad, A. Seal oil copared to soy oil in patients with joint pain and inflammatory bowel disease (IBD). Gastroenterology 2003, 4, A67. [Google Scholar] [CrossRef]
- Morshedzadeh, N.; Shahrokh, S.; Aghdaei, H.A.; Amin Pourhoseingholi, M.; Chaleshi, V.; Hekmatdoost, A.; Karimi, S.; Zali, M.R.; Mirmiran, P. Effects of flaxseed and flaxseed oil supplement on serum levels of inflammatory markers, metabolic parameters and severity of disease in patients with ulcerative colitis. Complement. Ther. Med. 2019, 46, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Morvaridi, M.; Jafarirad, S.; Seyedian, S.S.; Alavinejad, P.; Cheraghian, B. The effects of extra virgin olive oil and canola oil on inflammatory markers and gastrointestinal symptoms in patients with ulcerative colitis. Eur. J. Clin. Nutr. 2020, 74, 891–899. [Google Scholar] [CrossRef]
- Zundler, S.; Dietz, L.; Matzel, K.E.; Geppert, C.-I.; Becker, E.; Rath, T.; Neurath, M.F.; Atreya, R. Successful Long-term Treatment of Diversion Colitis with Topical Coconut Oil Application. Off. J. Am. Coll. Gastroenterol. 2018, 113, 1908–1910. [Google Scholar] [CrossRef]
- Greenfield, S.M.; Green, A.T.; Teare, J.P.; Jenkins, A.P.; Punchard, N.A.; Ainley, C.C.; Thompson, R.P.H. A randomized controlled study of evening primrose oil and fish oil in ulcerative colitis. Aliment. Pharmacol. Ther. 1993, 7, 159–166. [Google Scholar] [CrossRef]
- Chen, L.; Wang, J. Gut microbiota and inflammatory bowel disease. WIREs Mech. Dis. 2022, 14, e1540. [Google Scholar] [CrossRef]
- Franzosa, E.A.; Sirota-Madi, A.; Avila-Pacheco, J.; Fornelos, N.; Haiser, H.J.; Reinker, S.; Vatanen, T.; Hall, A.B.; Mallick, H.; McIver, L.J.; et al. Gut microbiome structure and metabolic activity in inflammatory bowel disease. Nat. Microbiol. 2019, 4, 293–305. [Google Scholar] [CrossRef]
- Martini, E.; Krug, S.M.; Siegmund, B.; Neurath, M.F.; Becker, C. Mend Your Fences: The Epithelial Barrier and its Relationship With Mucosal Immunity in Inflammatory Bowel Disease. Cell. Mol. Gastroenterol. Hepatol. 2017, 4, 33–46. [Google Scholar] [CrossRef] [Green Version]
- Iyer, N.; Corr, S.C. Gut Microbial Metabolite-Mediated Regulation of the Intestinal Barrier in the Pathogenesis of Inflammatory Bowel Disease. Nutrients 2021, 13, 4259. [Google Scholar] [CrossRef]
- McDaniel, D.K.; Eden, K.; Ringel, V.M.; Allen, I.C. Emerging Roles for Noncanonical NF-κB Signaling in the Modulation of Inflammatory Bowel Disease Pathobiology. Inflamm. Bowel Dis. 2016, 22, 2265–2279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, J.; Feng, J. Signaling Pathways Associated with Inflammatory Bowel Disease. Recent Pat. Inflamm. Allergy Drug Discov. 2010, 4, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Peng, P.; Ding, N.; Jia, W.; Huang, C.; Tang, Y. Oxidative Stress, Inflammation, Gut Dysbiosis: What Can Polyphenols Do in Inflammatory Bowel Disease? Antioxidants 2023, 12, 967. [Google Scholar] [CrossRef]
- Yuksel, M.; Ates, I.; Kaplan, M.; Arikan, M.F.; Ozin, Y.O.; Kilic, Z.M.Y.; Topcuoglu, C.; Kayacetin, E. Is oxidative stress associated with activation and pathogenesis of inflammatory bowel disease? J. Med. Biochem. 2017, 36, 341–348. [Google Scholar] [CrossRef]
- De Kivit, S.; Tobin, M.C.; Forsyth, C.B.; Keshavarzian, A.; Landay, A.L. Regulation of intestinal immune responses through TLR activation: Implications for pro-and prebiotics. Front. Immunol. 2014, 5, 60. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Shan, Q.; Sang, X.; Zhu, R.; Chen, X.; Cao, G. Total glycosides of peony protects against inflammatory bowel disease by regulating IL-23/IL-17 axis and Th17/Treg balance. Am. J. Chin. Med. 2019, 47, 177–201. [Google Scholar] [CrossRef]
- Ma, C.; Vasu, R.; Zhang, H. The Role of Long-Chain Fatty Acids in Inflammatory Bowel Disease. Mediat. Inflamm. 2019, 2019, 8495913. [Google Scholar] [CrossRef]
- Charpentier, C.; Chan, R.; Salameh, E.; Mbodji, K.; Ueno, A.; Coëffier, M.; Guérin, C.; Ghosh, S.; Savoye, G.; Marion-Letellier, R. Dietary n-3 PUFA May Attenuate Experimental Colitis. Mediat. Inflamm. 2018, 2018, 8430614. [Google Scholar] [CrossRef]
- Uchiyama, K.; Nakamura, M.; Odahara, S.; Koido, S.; Katahira, K.; Shiraishi, H.; Ohkusa, T.; Fujise, K.; Tajiri, H. N-3 polyunsaturated fatty acid diet therapy for patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2010, 16, 1696–1707. [Google Scholar] [CrossRef] [PubMed]

| Oil | Source | Composition | Dosage | Model | Mechanism | Year | Reference |
|---|---|---|---|---|---|---|---|
| Lentisc oil | Pistacia lentiscus | Oleic acid (47.96%), palmitic acid (27.94%), and linoleic acid (20.22%). | 30 mg oil/100 g of food/rat | TNBS-induced colitis in Wistar rats | Modification of arachidonic acid metabolism. | 2016 | [83] |
| Camellia oil | Camellia oleifera Abel. | Rich in oleic acid, linoleic acid, and palmitic acid. | 2 mL/kg BW | Acetic acid-induced colitis in SD rats | Modulation of gut microbiota; significant reduction in inflammatory injury and lipid peroxidation. | 2018 | [84] |
| / | 2 mL/kg BW | Acetic acid-induced colitis in SD rats | Modulation of gut microbiota, reduction in oxidative stress, and inhibition of inflammatory responses. | 2020 | [85] | ||
| Flaxseed oil | Linum usitatissimum L. | Rich in omega-3 fatty acids. | 400, 800 and 1600 mg/kg BW | DSS-induced colitis in SD rats | Modulation of oxidative conditions, inflammatory factors, and cecal microbiota. | 2020 | [64] |
| 100, 300 and 500 mg/kg BW | Acetic acid-induced colitis in SD rats | Improvement of immune dysregulation, barrier defect, and microbial imbalance in colitis rats. | 2020 | [65] | |||
| Garlic oil | Allium sativum | / | 25, 50 and 100 mg/kg/day | DSS-induced colitis in Wistar rats | Improvement of colitis in rats through its antioxidant, anti-inflammatory, and immunomodulatory properties. | 2016 | [58] |
| / | 5 mL/kg | Acetic acid-induced colitis in Wistar rats | Alleviation of colon damage and inflammatory response in a model of acetic acid-induced colitis. | 2020 | [59] | ||
| Perilla oil | Perilla frutescens | Rich in omega-3 fatty acids (ranging from 54% to 60%). | Supplementation with perilla oil for 16 weeks. | High-fat diet-induced inflammation in the colon of C57BL/6J mice | Inhibition of the activation of the NF-κB pathway. | 2020 | [51] |
| Rich in omega-3 fatty acids (59.7%). | 8% | High-fat diet-induced inflammation in the colon of C57BL/6J mice | Protecting the intestinal barrier, inhibiting NF-κB pathway, reducing the expression of pro-inflammatory genes. | 2022 | [52] | ||
| Rich in alpha-linolenic acid (61.51%). | 20, 100, 200 mg/kg BW | DSS-induced colitis in C57BL/6 mice | Significantly reducing inflammation in colon tissues. | 2021 | [53] | ||
| Rich in polyunsaturated fatty acids. | 8% | High-fat diet-induced inflammation in the colon of C57BL/6J mice | Significantly reducing levels of inflammatory factors in both the serum and colon. | 2022 | [54] | ||
| Pequi oil | Caryocar brasiliense | Rich in oleic acid and carotenoids. | 280 mg of pequi oil was homogenized in 1.1 g of chow. | DSS-induced colitis in C57BL/6 mice | Impact on the intestinal immune system and improvement of DSS-induced intestinal immune injury. | 2021 | [86] |
| Grape seed oil | / | / | 1 mL enema therapy. | Acetic acid-induced colitis in SD rats | The antioxidant properties of grape seed oil improve colitis. | 2017 | [81] |
| Rich in Carbon 60. | 1 mL/kg | DSS-induced colitis in Wistar rats | Improvement of clinical symptoms in rats with colitis. | 2022 | [82] | ||
| Algal oil | / | Rich in docosahexaenoic acid. | 250 or 500 mg/kg/day | DSS-induced colitis in C57BL/6 mice | Modulating the gut microbiota and metabolites to restore the intestinal barrier. | 2020 | [87] |
| Walnut oil | / | Rich in linoleic acid and alpha-linolenic acid. | 2.5 mL/kg/day | DSS-induced colitis in C57BL/6 mice | Inhibiting the activation of NLRP3 inflammasome and modulating the gut microbiota. | 2021 | [71] |
| Rich in linoleic (55–70%) and α-linolenic (10–18%) acids. | 7% | DSS-induced colitis in C57BL/6 mice | Alleviating mouse intestinal inflammation and restoring intestinal barrier function. | 2020 | [70] | ||
| Yadanzi oil | Brucea javanica | Rich in hexadecanoic acid, linoleic acid, oleic acid. | 0.5, 1 and 2 g/kg | DSS-induced colitis in Balb/C mice | Inhibition of NF-κB activation. | 2017 | [76] |
| Rich in brusatol, oleic acid and fatty acids. | 152.5, 305, 610 mg/kg/day | DSS-induced colitis in Balb/C mice | Inhibition of NF-κB and RhoA/ROCK signaling pathways. | 2021 | [77] | ||
| Stinging nettle seed oil | Urtica dioica | Rich in palmitic acid, oleic acid, and linoleic acid. | 2.5 mL/kg | TNBS-induced colitis in Wistar rats | Improving colitis through its anti-inflammatory and antioxidant effects. | 2011 | [88] |
| Cinnamon oil | Cinnamomum zeylanicum | / | 630, 1250, 2500, 5000 ppm | TNBS-induced colitis in ICR rats | Modulating intestinal bacteria to improve intestinal wall injury. | 2013 | [89] |
| Menthacarin | Mentha piperita L.; Carum carvi L. | Peppermint oil and caraway oil | 1, 3, 6, and 12 µg/µL | DSS-induced colitis in C57BL/6 mice | Improving clinical symptoms of colitis in mice through its anti-inflammatory effect. | 2020 | [90] |
| Angelica oil | Angelica sinensis | Rich in ligustilide and linoleic acid. | 10, 20, and 40 mg/kg | DSS-induced colitis in C57BL/6J mice | Restoring intestinal barrier function by inhibiting the S100A8/A9 signaling pathway. | 2023 | [91] |
| Ozonized olive oil | / | Rich in oxygenated triglyceride. | 3 and 6 mg/kg | DNBS-induced colitis in albino rats | CAT, GSH-Px, and SOD activities in the colon were significantly increased in a dose-dependent manner compared to the control group. | 2014 | [92] |
| Black cumin oil | Nigella sativa | Rich in linoleic and oleic acids. | 2.5 mL/kg | TNBS-induced colitis in Wistar albino rats | Reduced pro-inflammatory cytokines, lactate dehydrogenase, triglycerides, and cholesterol. | 2011 | [93] |
| Olive oil | / | Rich in EPA and DHA polyunsaturated fatty acids. | 4% | DSS-induced colitis in Wistar rats | Reduced colonic inflammation. | 2005 | [94] |
| Extra virgin olive oil | / | / | 5 mL/Kg BW | Acetic acid-induced colitis in SD rats | Alleviated the elevated levels of IL-1β and oxidative damage in colitis. | 2020 | [44] |
| / | 5% | DSS-induced colitis in SD rats | Reduced the expression of STAT3, pSTAT3, COX-2, and iNOS in colitic rats, inhibiting chronic inflammation. | 2014 | [45] | ||
| Enriched with hydroxytyrosol. | 40 mg/kg | DSS-induced colitis in C57BL/6 mice | Improving colitis by modulating the cytokines COX-2 and iNOS. | 2012 | [46] | ||
| Unsaponifiable. | / | DSS-induced colitis in C57BL/6 mice | Improving colitis by modulating the p38 MAPK and NFκB signaling pathways. | 2013 | [47] | ||
| Pomegranate seed oil | Punica granatum | Rich in conjugated linolenic acids, oleic acid, linoleic acid. | 1.5% | Necrotizing enterocolitis in SD rats | Improving intestinal epithelial homeostasis and mucosal inflammation. | 2012 | [95] |
| Black grape oil | Vitis vinifera | Rich in unsaturated fatty acids. | 2, 4, and 8 mL/kg | Acetic acid-induced colitis in Wistar rats | Improving oxidative stress. | 2020 | [80] |
| Yarrow oil | Achillea millefolium | Rich in sabinene and pinene. | 100 mg/kg | DSS-induced colitis in C57BL/6 mice | Mitigating UC symptoms and regulating the secretion of inflammatory cytokines by modulating the NF-κB and PPAR-γ pathways. | 2021 | [96] |
| Cottonseed oil | / | / | 200 μL/day | DSS-induced colitis in C57BL/6 mice | Improving intestinal inflammation by reducing inflammatory cytokines and oxidative stress markers. | 2019 | [97] |
| Garden cress seed oil | Lepidium sativum | Rich in n-3 fatty acid. | 10% | DSS-induced colitis in Wistar rats | Reduce oxidative damage, inhibit inflammatory mediators, and decrease damage to the colon. | 2014 | [98] |
| Rice bran oil | / | Rich in oryzanol (1.2%). | 10% | DSS-induced colitis in Wistar rats | Reduced oxidative damage, inhibition of inflammatory mediators, and decreased damage to the colon. | 2014 | [98] |
| Ulvaceae oil | Ulva ohnoi | / | 25 mg/kg | DSS-induced colitis in ICR mice | Reduced expression of inflammatory cytokines. | 2021 | [99] |
| Mandarin oil | / | / | 200, 400 mg/kg | Indomethacin-induced colitis in Wistar rats | Exhibit antioxidant and anti-inflammatory effects against rat enterocolitis. | 2014 | [100] |
| Copaiba oil | Copaifera reticulata | Rich in β-caryophyllene (37.6%), β-bisabolene (13.9%). | 1.15 g/kg | TNBS-induced colitis in Wistar rats | Reduce oxidative stress and inflammation. | 2018 | [101] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, Y.; Wang, D.; Duan, H.; Zhou, S.; Guo, J.; Yan, W. The Potential of Natural Oils to Improve Inflammatory Bowel Disease. Nutrients 2023, 15, 2606. https://doi.org/10.3390/nu15112606
Zhou Y, Wang D, Duan H, Zhou S, Guo J, Yan W. The Potential of Natural Oils to Improve Inflammatory Bowel Disease. Nutrients. 2023; 15(11):2606. https://doi.org/10.3390/nu15112606
Chicago/Turabian StyleZhou, Yaxi, Diandian Wang, Hao Duan, Shiqi Zhou, Jinhong Guo, and Wenjie Yan. 2023. "The Potential of Natural Oils to Improve Inflammatory Bowel Disease" Nutrients 15, no. 11: 2606. https://doi.org/10.3390/nu15112606