
Maternal Diet Quality and Prenatal Depressive Symptoms: The Moderating Role of Economic Well-Being



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Procedures
2.2. Participants
2.3. Measures
2.3.1. Adapted Dietary Inflammatory Index (ADII)
2.3.2. Healthy Eating Index-2015 (HEI-2015)
2.3.3. Economic Well-Being
2.3.4. Prenatal Depressive Symptoms
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
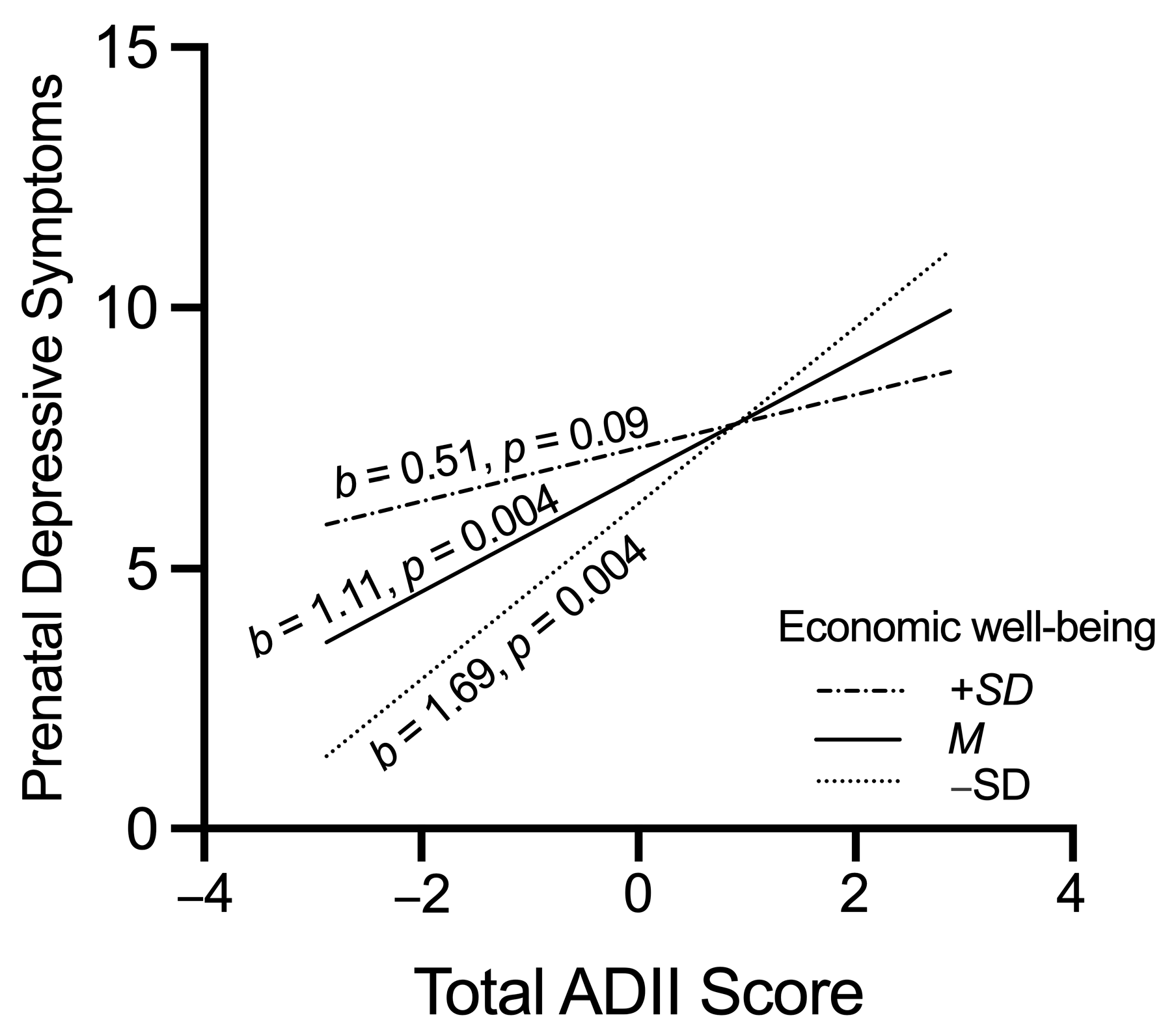
3.2. ADII, Economic Well-Being, and Prenatal Depressive Symptoms
3.3. HEI-2015, Economic Well-Being, and Prenatal Depressive Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Philipps, C.; Johnson, N. The impact of quality of diet and other factors on birth weight of infants. Am. J. Clin. Nutr. 1977, 30, 215–225. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.M.; McAuliffe, F.M. Impact of maternal nutrition on pregnancy outcome—Does it matter what pregnant women eat? Best Pract. Res. Clin. Obstet. Gynaecol. 2015, 29, 63–78. [Google Scholar] [CrossRef]
- Procter, S.B.; Campbell, C.G. Position of the Academy of Nutrition and Dietetics: Nutrition and Lifestyle for a Healthy Pregnancy Outcome. J. Acad. Nutr. Diet. 2014, 114, 1099–1103. [Google Scholar] [CrossRef] [PubMed]
- Yelverton, C.A.; Rafferty, A.A.; Moore, R.L.; Byrne, D.F.; Mehegan, J.; Cotter, P.D.; Van Sinderen, D.; Murphy, E.F.; Killeen, S.L.; McAuliffe, F.M. Diet and mental health in pregnancy: Nutrients of importance based on large observational cohort data. Nutrition 2022, 96, 111582. [Google Scholar] [CrossRef]
- Bennett, H.A.; Einarson, A.; Taddio, A.; Koren, G.; Einarson, T.R. Prevalence of Depression During Pregnancy: Systematic Review. Obstet. Gynecol. 2004, 103, 698–709. [Google Scholar] [CrossRef]
- Field, T. Prenatal depression effects on early development: A review. Infant Behav. Dev. 2011, 34, 1–14. [Google Scholar] [CrossRef]
- Field, T.; Diego, M.; Hernandez-Reif, M. Prenatal depression effects on the fetus and newborn: A review. Infant Behav. Dev. 2006, 29, 445–455. [Google Scholar] [CrossRef]
- Monk, C.; Georgieff, M.K.; Osterholm, E.A. Research review: Maternal prenatal distress and poor nutrition–mutually influencing risk factors affecting infant neurocognitive development. J. Child Psychol. Psychiatry 2013, 54, 115–130. [Google Scholar] [CrossRef]
- Lai, J.S.; Hiles, S.; Bisquera, A.; Hure, A.J.; McEvoy, M.; Attia, J. A systematic review and meta-analysis of dietary patterns and depression in community-dwelling adults. Am. J. Clin. Nutr. 2014, 99, 181–197. [Google Scholar] [CrossRef]
- Ljungberg, T.; Bondza, E.; Lethin, C. Evidence of the importance of dietary habits regarding depressive symptoms and depression. Int. J. Environ. Res. Public Health 2020, 17, 1616. [Google Scholar] [CrossRef] [PubMed]
- Leung, B.M.Y.; Kaplan, B.J. Perinatal Depression: Prevalence, Risks, and the Nutrition Link—A Review of the Literature. J. Am. Diet. Assoc. 2009, 109, 1566–1575. [Google Scholar] [CrossRef]
- Sparling, T.M.; Henschke, N.; Nesbitt, R.C.; Gabrysch, S. The role of diet and nutritional supplementation in perinatal depression: A systematic review. Matern. Child Nutr. 2017, 13, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.; Waqas, A.; Bilal, A.; Mustehsan, Z.H.; Omar, J.; Rahman, A. Association of Maternal depression with diet: A systematic review. Asian J. Psychiatr. 2020, 52, 102098. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, G.D.; Fraser, W.D.; Séguin, J.R. Emerging risk factors for postpartum depression: Serotonin transporter genotype and omega-3 fatty acid status. Can. J. Psychiatry 2012, 57, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Freeman, M.P. Omega-3 fatty acids and perinatal depression: A review of the literature and recommendations for future research. Prostaglandins Leukot. Essent. Fat. Acids 2006, 75, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Miyake, Y.; Sasaki, S.; Tanaka, K.; Yokoyama, T.; Ohya, Y.; Fukushima, W.; Saito, K.; Ohfuji, S.; Kiyohara, C.; Hirota, Y. Dietary folate and vitamins B12, B6, and B2 intake and the risk of postpartum depression in Japan: The Osaka Maternal and Child Health Study. J. Affect. Disord. 2006, 96, 133–138. [Google Scholar] [CrossRef]
- Singh, A.; Trumpff, C.; Genkinger, J.; Davis, A.; Spann, M.; Werner, E.; Monk, C. Micronutrient dietary intake in Latina pregnant adolescents and its association with level of depression, stress, and social support. Nutrients 2017, 9, 1212. [Google Scholar] [CrossRef]
- Chong, M.F.; Wong, J.X.; Colega, M.; Chen, L.-W.; van Dam, R.M.; Tan, C.S.; Lim, A.L.; Cai, S.; Broekman, B.F.; Lee, Y.S. Relationships of maternal folate and vitamin B12 status during pregnancy with perinatal depression: The GUSTO study. J. Psychiatr. Res. 2014, 55, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Wirfält, E.; Drake, I.; Wallström, P. What do review papers conclude about food and dietary patterns? Food Nutr. Res. 2013, 57, 20523. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Lindsay, K.L.; Most, J.; Buehler, K.; Kebbe, M.; Altazan, A.D.; Redman, L.M. Maternal mindful eating as a target for improving metabolic outcomes in pregnant women with obesity. Front. Biosci. 2021, 26, 1548. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, K.L.; Buss, C.; Wadhwa, P.D.; Entringer, S. Maternal stress potentiates the effect of an inflammatory diet in pregnancy on maternal concentrations of tumor necrosis factor alpha. Nutrients 2018, 10, 1252. [Google Scholar] [CrossRef]
- Pick, M.E.; Edwards, M.; Moreau, D.; Ryan, E.A. Assessment of diet quality in pregnant women using the Healthy Eating Index. J. Am. Diet. Assoc. 2005, 105, 240–246. [Google Scholar] [CrossRef] [PubMed]
- van Woudenbergh, G.J.; Theofylaktopoulou, D.; Kuijsten, A.; Ferreira, I.; van Greevenbroek, M.M.; van der Kallen, C.J.; Schalkwijk, C.G.; Stehouwer, C.D.; Ocke, M.C.; Nijpels, G. Adapted dietary inflammatory index and its association with a summary score for low-grade inflammation and markers of glucose metabolism: The Cohort study on Diabetes and Atherosclerosis Maastricht (CODAM) and the Hoorn study. Am. J. Clin. Nutr. 2013, 98, 1533–1542. [Google Scholar] [CrossRef] [PubMed]
- Lahti-Pulkkinen, M.; Girchenko, P.; Robinson, R.; Lehto, S.M.; Toffol, E.; Heinonen, K.; Reynolds, R.M.; Kajantie, E.; Laivuori, H.; Villa, P.M.; et al. Maternal depression and inflammation during pregnancy. Psychol. Med. 2020, 50, 1839–1851. [Google Scholar] [CrossRef]
- Shrider, E.A.; Kollar, M.; Chen, F.; Semega, J. Income and Poverty in the United States: 2020; Current Population Reports; US Census Bureau: Washington, DC, USA, 2021.
- Everson, S.A.; Maty, S.C.; Lynch, J.W.; Kaplan, G.A. Epidemiologic evidence for the relation between socioeconomic status and depression, obesity, and diabetes. J. Psychosom. Res. 2002, 53, 891–895. [Google Scholar] [CrossRef]
- Bruce, M.L.; Takeuchi, D.T.; Leaf, P.J. Poverty and Psychiatric Status: Longitudinal Evidence from the New Haven Epidemiologic Catchment Area Study. Arch. Gen. Psychiatry 1991, 48, 470–474. [Google Scholar] [CrossRef]
- Letourneau, N.L.; Duffett-Leger, L.; Levac, L.; Watson, B.; Young-Morris, C. Socioeconomic status and child development: A meta-analysis. J. Emot. Behav. Disord. 2013, 21, 211–224. [Google Scholar] [CrossRef]
- O’Hara, M.W.; Wisner, K.L. Perinatal mental illness: Definition, description and aetiology. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 3–12. [Google Scholar] [CrossRef]
- Míguez, M.C.; Vázquez, M.B. Risk factors for antenatal depression: A review. World J. Psychiatry 2021, 11, 325–336. [Google Scholar] [CrossRef]
- Sarlio-Lahteenkorva, S.; Lahelma, E. Food Insecurity Is Associated with Past and Present Economic Disadvantage and Body Mass Index. J. Nutr. 2001, 131, 2880–2884. [Google Scholar] [CrossRef]
- Hanson, C.; Schumacher, M.V.; Lyden, E.; Su, D.; Furtado, J.; Cammack, R.; Bereitschaft, B.; Van Ormer, M.; Needelman, H.; McGinn, E.; et al. Fat-soluble vitamins A and E and health disparities in a cohort of pregnant women at delivery. J. Nutr. Sci. 2018, 7, e14. [Google Scholar] [CrossRef]
- Cohen, S.; Doyle, W.J.; Baum, A. Socioeconomic Status Is Associated with Stress Hormones. Psychosom. Med. 2006, 68, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Lancaster, C.A.; Gold, K.J.; Flynn, H.A.; Yoo, H.; Marcus, S.M.; Davis, M.M. Risk factors for depressive symptoms during pregnancy: A systematic review. Am. J. Obstet. Gynecol. 2010, 202, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Bublitz, M.H.; Vergara-Lopez, C.; O’Reilly Treter, M.; Stroud, L.R. Association of Lower Socioeconomic Position in Pregnancy with Lower Diurnal Cortisol Production and Lower Birthweight in Male Infants. Clin. Ther. 2016, 38, 265–274. [Google Scholar] [CrossRef]
- Garcia, E.R.; Yim, I.S. A systematic review of concepts related to women’s empowerment in the perinatal period and their associations with perinatal depressive symptoms and premature birth. BMC Pregnancy Childbirth 2017, 17, 347. [Google Scholar] [CrossRef] [PubMed]
- Feig, E.H.; Levy, D.E.; McCurley, J.L.; Rimm, E.B.; Anderson, E.M.; Gelsomin, E.D.; Thorndike, A.N. Association of work-related and leisure-time physical activity with workplace food purchases, dietary quality, and health of hospital employees. BMC Public Health 2019, 19, 1583. [Google Scholar] [CrossRef] [PubMed]
- Freedman, L.S.; Guenther, P.M.; Krebs-Smith, S.M.; Dodd, K.W.; Midthune, D. A Population’s Distribution of Healthy Eating Index-2005 Component Scores Can Be Estimated When More Than One 24-Hour Recall Is Available. J. Nutr. 2010, 140, 1529–1534. [Google Scholar] [CrossRef]
- Gibson, R.S.; Charrondiere, U.R.; Bell, W. Measurement Errors in Dietary Assessment Using Self-Reported 24-Hour Recalls in Low-Income Countries and Strategies for Their Prevention. Adv. Nutr. 2017, 8, 980–991. [Google Scholar] [CrossRef]
- Knüppel, S.; Norman, K.; Boeing, H. Is a Single 24-hour Dietary Recall per Person Sufficient to Estimate the Population Distribution of Usual Dietary Intake? J. Nutr. 2019, 149, 1491–1492. [Google Scholar] [CrossRef]
- Authority, E.F.S. General principles for the collection of national food consumption data in the view of a pan-European dietary survey. EFSA J. 2009, 7, 1435. [Google Scholar] [CrossRef]
- Brouwer, J.G.; Makama, M.; Van Woudenbergh, G.J.; Vasen, H.F.; Nagengast, F.M.; Kleibeuker, J.H.; Kampman, E.; Van Duijnhoven, F.J. Inflammatory potential of the diet and colorectal tumor risk in persons with Lynch syndrome. Am. J. Clin. Nutr. 2017, 106, 1287–1294. [Google Scholar] [CrossRef] [PubMed]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef] [PubMed]
- 2021 Poverty Guidelines. U.S. Federal Poverty Guidelines Used to Determine Financial Eligibility for Certain Federal Programs 2021. Available online: https://aspe.hhs.gov/2021-poverty-guidelines (accessed on 8 May 2023).
- United States Census Bureau. Poverty Thresholds by Size of Family and Number of Children. Available online: https://www.census.gov/data/tables/time-series/demo/income-poverty/historical-poverty-thresholds.html (accessed on 8 May 2023).
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression: Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef]
- Bosco, F.A.; Aguinis, H.; Singh, K.; Field, J.G.; Pierce, C.A. Correlational effect size benchmarks. J. Appl. Psychol. 2015, 100, 431–449. [Google Scholar] [CrossRef]
- Zhang, Y.; Hedo, R.; Rivera, A.; Rull, R.; Richardson, S.; Tu, X.M. Post hoc power analysis: Is it an informative and meaningful analysis? Gen. Psychiatr. 2019, 32, e100069. [Google Scholar] [CrossRef]
- Levine, M.; Ensom, M.H.H. Post Hoc Power Analysis: An Idea Whose Time Has Passed? Pharmacother. J. Hum. Pharmacol. Drug Ther. 2001, 21, 405–409. [Google Scholar] [CrossRef]
- Gilbert, G.E.; Prion, S. Making Sense of Methods and Measurement: The Danger of the Retrospective Power Analysis. Clin. Simul. Nurs. 2016, 12, 303–304. [Google Scholar] [CrossRef]
- Heckman, M.G.; Davis, J.M.; Crowson, C.S. Post Hoc power calculations: An inappropriate method for interpreting the findings of a research study. J. Rheumatol. 2022, 49, 867–870. [Google Scholar] [CrossRef]
- Bennett, H.A.; Einarson, A.; Taddio, A.; Koren, G.; Einarson, T.R. Depression during Pregnancy. Clin. Drug Investig. 2004, 24, 157–179. [Google Scholar] [CrossRef]
- Levis, B.; Negeri, Z.; Sun, Y.; Benedetti, A.; Thombs, B.D. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for screening to detect major depression among pregnant and postpartum women: Systematic review and meta-analysis of individual participant data. BMJ 2020, 371, m4022. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture, Food and Nutrition Service; Center for Nutrition Policy and Promotion. Average Healthy Eating Index-2015 Scores for Non-Pregnant Non-Lactating, Pregnant and Lactating Women 20–44 Years. Available online: https://fns-prod.azureedge.us/sites/default/files/media/file/HEI-2015_PregnantAndLactatingWomen20-44Years_NHANES2013-2018.pdf (accessed on 8 May 2023).
- Baskin, R.; Hill, B.; Jacka, F.N.; O’Neil, A.; Skouteris, H. The association between diet quality and mental health during the perinatal period. A systematic review. Appetite 2015, 91, 41–47. [Google Scholar] [CrossRef] [PubMed]
- King, J.C. The Risk of Maternal Nutritional Depletion and Poor Outcomes Increases in Early or Closely Spaced Pregnancies. J. Nutr. 2003, 133, 1732S–1736S. [Google Scholar] [CrossRef] [PubMed]
- Marx, W.; Moseley, G.; Berk, M.; Jacka, F. Nutritional psychiatry: The present state of the evidence. Proc. Nutr. Soc. 2017, 76, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Bao, J.; de Jong, V.; Atkinson, F.; Petocz, P.; Brand-Miller, J.C. Food insulin index: Physiologic basis for predicting insulin demand evoked by composite meals. Am. J. Clin. Nutr. 2009, 90, 986–992. [Google Scholar] [CrossRef]
- Merbis, M.A.E.; Snoek, F.J.; Kanc, K.; Heine, R.J. Hypoglycaemia induces emotional disruption. Patient Educ. Couns. 1996, 29, 117–122. [Google Scholar] [CrossRef]
- Cardinal, P.; Monchaux de Oliveira, C.; Sauvant, J.; Foury, A.; Darnaudéry, M.; Vancassel, S.; Castanon, N.; Capuron, L. A new experimental design to study inflammation-related versus non-inflammation-related depression in mice. J. Neuroinflamm. 2021, 18, 290. [Google Scholar] [CrossRef]
- Noble, E.E.; Hsu, T.M.; Kanoski, S.E. Gut to Brain Dysbiosis: Mechanisms Linking Western Diet Consumption, the Microbiome, and Cognitive Impairment. Front. Behav. Neurosci. 2017, 11, 9. [Google Scholar] [CrossRef]
- Wärnberg, J.; Gomez-Martinez, S.; Romeo, J.; Díaz, L.-E.; Marcos, A. Nutrition, Inflammation, and Cognitive Function. Ann. N. Y. Acad. Sci. 2009, 1153, 164–175. [Google Scholar] [CrossRef]
- Rosenblat, J.D.; Cha, D.S.; Mansur, R.B.; McIntyre, R.S. Inflamed moods: A review of the interactions between inflammation and mood disorders. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2014, 53, 23–34. [Google Scholar] [CrossRef]
- Kheirouri, S.; Alizadeh, M. Dietary inflammatory potential and the risk of incident depression in adults: A systematic review. Adv. Nutr. 2019, 10, 9–18. [Google Scholar] [CrossRef]
- Wang, J.; Zhou, Y.; Chen, K.; Jing, Y.; He, J.; Sun, H.; Hu, X. Dietary inflammatory index and depression: A meta-analysis. Public Health Nutr. 2019, 22, 654–660. [Google Scholar] [CrossRef]
- Tolkien, K.; Bradburn, S.; Murgatroyd, C. An anti-inflammatory diet as a potential intervention for depressive disorders: A systematic review and meta-analysis. Clin. Nutr. 2019, 38, 2045–2052. [Google Scholar] [CrossRef]
- Lassale, C.; Batty, G.D.; Baghdadli, A.; Jacka, F.; Sánchez-Villegas, A.; Kivimäki, M.; Akbaraly, T. Healthy dietary indices and risk of depressive outcomes: Asystematic review and meta-analysis of observational studies. Mol. Psychiatry 2019, 24, 965–986. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, K.L.; Milone, G.F.; Grobman, W.A.; Haas, D.M.; Mercer, B.M.; Simhan, H.N.; Saade, G.R.; Silver, R.M.; Chung, J.H. Periconceptional diet quality is associated with gestational diabetes risk and glucose concentrations among nulliparous gravidas. Front. Endocrinol. 2022, 13, 940870. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Rifas-Shiman, S.L.; Ertel, K.A.; Rich-Edwards, J.; Kleinman, K.; Gillman, M.W.; Oken, E.; James-Todd, T. Pregnancy Hyperglycaemia and Risk of Prenatal and Postpartum Depressive Symptoms. Paediatr. Perinat. Epidemiol. 2015, 29, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Guenther, P.M.; Reedy, J.; Krebs-Smith, S.M. Development of the Healthy Eating Index-2005. J. Am. Diet. Assoc. 2008, 108, 1896–1901. [Google Scholar] [CrossRef]
- Mao, F.; Sun, Y.; Wang, J.; Huang, Y.; Lu, Y.; Cao, F. Sensitivity to change and minimal clinically important difference of Edinburgh postnatal depression scale. Asian J. Psychiatr. 2021, 66, 102873. [Google Scholar] [CrossRef]
- Matthey, S. Calculating clinically significant change in postnatal depression studies using the Edinburgh Postnatal Depression Scale. J. Affect. Disord. 2004, 78, 269–272. [Google Scholar] [CrossRef]
- Choi, S.K.; Park, Y.G.; Park, I.Y.; Ko, H.S.; Shin, J.C. Impact of antenatal depression on perinatal outcomes and postpartum depression in Korean women. J. Res. Med. Sci. 2014, 19, 807–812. [Google Scholar]
- Eastwood, J.; Ogbo, F.A.; Hendry, A.; Noble, J.; Page, A.; Group, E.Y.R. The impact of antenatal depression on perinatal outcomes in Australian women. PLoS ONE 2017, 12, e0169907. [Google Scholar] [CrossRef]
- Al Rawahi, A.; Al Kiyumi, M.H.; Al Kimyani, R.; Al-Lawati, I.; Murthi, S.; Davidson, R.; Al Maniri, A.; Al Azri, M. The Effect of Antepartum Depression on the Outcomes of Pregnancy and Development of Postpartum Depression: A prospective cohort study of Omani women. Sultan Qaboos Univ. Med. J. 2020, 20, e179–e186. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.L.; Li, J.Q.; Pu, Y.Q.; Zhou, C.; Feng, S.W.; Luo, Q. Effect of prenatal depression during late pregnancy on maternal and neonatal outcomes. Clin. Exp. Obstet. Gynecol. 2020, 47, 681–686. [Google Scholar] [CrossRef]
- Friedman, E.M.; Herd, P. Income, education, and inflammation: Differential associations in a national probability sample (The MIDUS study). Psychosom. Med. 2010, 72, 290–300. [Google Scholar] [CrossRef]
- Gowda, C.; Hadley, C.; Aiello, A.E. The association between food insecurity and inflammation in the US adult population. Am. J. Public Health 2012, 102, 1579–1586. [Google Scholar] [CrossRef]
- Kelli, H.M.; Hammadah, M.; Ahmed, H.; Ko, Y.-A.; Topel, M.; Samman-Tahhan, A.; Awad, M.; Patel, K.; Mohammed, K.; Sperling, L.S. Association between living in food deserts and cardiovascular risk. Circ. Cardiovasc. Qual. Outcomes 2017, 10, e003532. [Google Scholar] [CrossRef]
- Marmot, M.; Wilkinson, R. Social Determinants of Health; OUP: Oxford, UK, 2005. [Google Scholar]
- Adler, N.E.; Boyce, T.; Chesney, M.A.; Cohen, S.; Folkman, S.; Kahn, R.L.; Syme, S.L. Socioeconomic status and health. The challenge of the gradient. Am. Psychol. 1994, 49, 15–24. [Google Scholar] [CrossRef]
- Owen, N.; Poulton, T.; Hay, F.C.; Mohamed-Ali, V.; Steptoe, A. Socioeconomic status, C-reactive protein, immune factors, and responses to acute mental stress. Brain. Behav. Immun. 2003, 17, 286–295. [Google Scholar] [CrossRef]
- Kimerling, R.; Baumrind, N. Access to specialty mental health services among women in California. Psychiatr. Serv. 2005, 56, 729–734. [Google Scholar] [CrossRef]
- Colasanto, M.; Madigan, S.; Korczak, D.J. Depression and inflammation among children and adolescents: A meta-analysis. J. Affect. Disord. 2020, 277, 940–948. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Overall | Study 1 (n = 17) | Study 2 (n = 26) | Non-Hispanic (n = 12) | Hispanic (n = 31) | |||
|---|---|---|---|---|---|---|---|
| M (SD) or n (%) | M (SD) or n (%) | M (SD) or n (%) | p | M (SD) or n (%) | M (SD) or n (%) | p | |
| Participant Characteristics: | |||||||
| Age | 28.84 (5.72) | 29.41 (5.21) | 28.46 (6.10) | 0.60 | 32.75 (4.31) | 27.32 (5.52) | 0.004 |
| Gestational age | 130.70 (20.98) | 116.47 (26.36) | 140.00 (8.19) | 0.002 | 128.17 (26.35) | 131.68 (18.93) | 0.68 |
| Pre-pregnancy BMI | 31.07 (4.97) | 30.86 (6.35) | 31.21 (3.96) | 0.83 | 28.99 (4.89) | 31.88 (4.84) | 0.09 |
| Ethnicity | 0.38 | – | |||||
| Non-Hispanic | 12 (27.9) | 6 (35.3) | 6 (23.1) | – | – | – | |
| Hispanic | 31 (72.1) | 11 (64.7) | 20 (76.9) | – | – | – | |
| Main Study Variables: | |||||||
| ADII | 0.03 (2.91) | 0.07 (2.25) | 0.00 (3.39) | 0.95 | 0.05 (2.46) | 0.02 (3.12) | 0.98 |
| HEI-2015 | 60.63 (13.37) | 64.84 (11.18) | 57.39 (14.25) | 0.08 | 64.41 (14.87) | 59.15 (12.71) | 0.27 |
| Economic well-being | 3.15 (3.26) | 2.88 (2.92) | 3.37 (3.57) | 0.65 | 5.05 (3.65) | 2.38 (2.81) | 0.02 |
| EPDS score | 7.07 (4.19) | 7.18 (4.61) | 7.00 (3.99) | 0.90 | 7.00 (3.16) | 7.10 (4.58) | 0.95 |
| 1. | 2. | 3. | 4. | 5. | 6. | |
|---|---|---|---|---|---|---|
| 1. ADII | ||||||
| 2. HEI-2015 | −0.65 *** | |||||
| 3. Income-to-poverty ratio | −0.29 | 0.06 | ||||
| 4. EDPS score | 0.36 * | −0.42 ** | 0.22 | |||
| 5. Age | −0.62 *** | 0.44 ** | 0.39 * | −0.15 | ||
| 6. GA | 0.02 | −0.27 | 0.15 | 0.05 | −0.00 | |
| 7. Pre-pregnancy BMI | 0.02 | 0.03 | −0.30 | −0.20 | −0.14 | −0.13 |
| Model 1 | |||||
| b | Beta | p | 95% CI | ||
| Step 1 | R2 = 0.08; adj.R2 = −0.01; F(3, 30) = 0.85, p = 0.48 | ||||
| Age | −0.16 | −0.20 | 0.26 | [−0.44, 0.12] | |
| Gestational age | 0.00 | 0.01 | 0.97 | [−0.07, 0.07] | |
| Pre-pregnancy BMI | −0.19 | −0.23 | 0.22 | [−0.50, 0.12] | |
| Step 2 | R2 = 0.23; adj.R2 = 0.09; Fchange(2, 28) = 2.72, p = 0.08 | ||||
| ADII | 0.60 | 0.40 | 0.06 | [−0.03, 1.23] | |
| Economic well-being | 0.36 | 0.28 | 0.15 | [−0.14, 0.87] | |
| Step 3 | R2 = 0.36; adj.R2 = 0.22; Fchange(1, 27) = 5.75, p = 0.02 | ||||
| ADII × Economic well-being | −0.18 | −0.52 | 0.02 | [−0.33, −0.03] | |
| Overall R2 = 0.36; adj.R2 = 0.22; F(6, 27) = 2.57, p = 0.04 | |||||
| Model 2 | |||||
| b | Beta | p | 95% CI | ||
| Step 1 | R2 = 0.08; adj.R2 = −0.01; F(3, 30) = 0.85, p = 0.48 | ||||
| Age | −0.16 | −0.20 | 0.26 | [−0.44, 0.12] | |
| Gestational age | 0.00 | 0.01 | 0.97 | [−0.07, 0.07] | |
| Pre-pregnancy BMI | −0.19 | −0.23 | 0.22 | [−0.50, 0.12] | |
| Step 2 | R2 = 0.32; adj.R2 = 0.20; Fchange(2, 28) = 4.92, p = 0.02 | ||||
| HEI-2015 | −0.18 | −0.53 | 0.01 | [−0.30, −0.05] | |
| Economic well-being | 0.31 | 0.24 | 0.19 | [−0.16, 0.78] | |
| Step 3 | R2 = 0.34; adj.R2 = 0.20; Fchange(1, 27) = 1.00, p = 0.33 | ||||
| HEI-2015 × Economic well-being | 0.02 | 0.16 | 0.33 | [−0.02, 0.06] | |
| Overall R2 = 0.34; adj.R2 = 0.20; F(6, 27) = 2.34, p = 0.06 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, P.; Yim, I.S.; Lindsay, K.L. Maternal Diet Quality and Prenatal Depressive Symptoms: The Moderating Role of Economic Well-Being. Nutrients 2023, 15, 2809. https://doi.org/10.3390/nu15122809
Wang P, Yim IS, Lindsay KL. Maternal Diet Quality and Prenatal Depressive Symptoms: The Moderating Role of Economic Well-Being. Nutrients. 2023; 15(12):2809. https://doi.org/10.3390/nu15122809
Chicago/Turabian StyleWang, Peiyi, Ilona S. Yim, and Karen L. Lindsay. 2023. "Maternal Diet Quality and Prenatal Depressive Symptoms: The Moderating Role of Economic Well-Being" Nutrients 15, no. 12: 2809. https://doi.org/10.3390/nu15122809
APA StyleWang, P., Yim, I. S., & Lindsay, K. L. (2023). Maternal Diet Quality and Prenatal Depressive Symptoms: The Moderating Role of Economic Well-Being. Nutrients, 15(12), 2809. https://doi.org/10.3390/nu15122809