Abstract
The food system plays a crucial role in the relationship between environmental, population and individual health. While leading healthcare and environmental organizations call for urgent action to address climate–planetary–human health crises, it is often challenging for healthcare organizations to respond at a systems level to these concerns. Additionally, there is little consensus and limited research exploring how future health professionals should be trained in order to work at both the individual and systems level to address or prevent the negative health impacts related to the current food system. The intervention of a 6-week, hands-on cooking and nutrition course for graduate health professional students which examines these intersections and equips students with clinically applicable skills was examined using matched pre- and post-course surveys and thematic analysis of reflective assignments. Results indicate improved knowledge and confidence in areas including understanding the food system, guiding patients through dietary change, working interprofessionally, and applying basic nutrition concepts to clinical practice.
1. Introduction
The food system, including the interconnectedness of food and humans, communities and the environment, plays a crucial role in population and individual health [1,2,3]. While leading healthcare and environmental organizations call for urgent action to address climate–planetary–human health crises worldwide, there is little consensus and limited research exploring the best and most effective way to empower future health professionals to address the intersection of the food system and human health [4].
In the United States (US), over 15,000 new food products are created annually [5]. According to a study based on data from the National Health and Nutrition Examination Survey (NHANES), approximately 60% of caloric intake of adults in the US consists of ultra-processed foods, which can be defined as “essentially industrial formulations mostly or entirely made from industrial ingredients, with little or no whole foods” [6]. Recent analysis suggests the US food supply is close to 73% ultra-processed [7]. Industrially produced, ultra-processed foods (UPF) are linked to higher rates of cardiometabolic and inflammatory diseases [8].
In a systematic review conducted in 2020, among 43 studies reviewed, 37 found dietary UPF exposure was associated with at least one adverse health outcome. Among adults, these included overweight, obesity and cardio-metabolic risks; cancer, type-2 diabetes and cardiovascular diseases; irritable bowel syndrome, depression and frailty conditions; and all-cause mortality. Among children and adolescents, these included cardio-metabolic risks and asthma. No study reported an association between UPF and beneficial health outcomes [9]. In contrast, a growing number of studies support the power of cooking and home-preparation of food to improve dietary quality and chronic disease self-management [10,11].
Additionally, economic inequality is tied to disparities in food and land access, leading to disproportionate rates of chronic conditions among marginalized communities throughout the US. According to the Center on Budget and Policy Priorities (CBPP), a non-partisan research and policy institute, adults in households with very low food security are 53% more likely to be diagnosed with a chronic condition, such as hypertension, coronary heart disease, hepatitis or stroke, than adults in food-secure households [12]. Recent studies show that food skills education and home cooking not only improve health outcomes, but also improve food security [13,14].
Health sciences curricula increasingly include education linking the social determinants of health to clinical outcomes, but often fail to explore the upstream factors specific to the food system that have direct relationships to human health conditions; or the diverse experiences that play a role in shaping identities, preferences and behaviors related to food choices, food skills and food literacy.
While specific nutrition competencies for health professional students have not been officially determined, Lepre et al. conducted a critical synthesis of publications proposing nutrition competencies for medical education internationally, and identified five common themes: (1) clinical practice; (2) health promotion and disease prevention; (3) communication; (4) working as a team; and (5) professional practice [15].
We propose that clinically relevant experiential education including hands-on cooking and eating, self reflection and cross-disciplinary engagement is needed to translate awareness of system-level problems into actionable skills for future health professionals.
2. Materials and Methods
2.1. Setting and Participants
In 2016, a chef/public health nutrition expert (JB) and an Internal Medicine/Pediatrics physician (KS) with expertise in integrative medicine developed and began teaching a food-systems-focused, hands-on culinary nutrition course (Food Matters for Health Professionals, FMHP). Initially piloted with medical students, then expanded to include any health sciences graduate students, the course offers experiential, interprofessional, clinically oriented culinary nutrition and food systems education. The 1-credit, 18 h graduate level course continues to be offered 1–2 times/semester through the Earl E. Bakken Center for Spirituality and Healing at the University of Minnesota, Twin Cities Campus.
Quantitative data from optional, identical pre-/post-course surveys were collected starting in 2018, with the description of students’ demographics and fields of study summarized in Table 1. Students enrolled in FMHP who completed both pre- and post-course surveys were included in the data analysis (n = 65).

Table 1.
Participant demographics (n = 65).
2.2. Course Detail
The course is taught over 6 weekly three-hour sessions, each with experiential, hands-on cooking, a didactic segment with interprofessional discussion opportunities and application to clinical care or public health spheres. The curriculum includes basic, clinically oriented nutrition concepts and their relationship to health in the context of the social, structural and commercial determinants of health and various facets of the food system. Culinary skills are integrated to enhance learning about nutrition concepts (macronutrients, vitamin/mineral composition of foods, etc.). See Table 2 for the course outline.
Table 2.
Course content by week and Course Learning Objectives.
Students are invited to share their personal and cultural experiences with food, agriculture, cooking and community, as well as their experiences as graduate students in their respective health sciences fields, through an activity during the first class session called “The Food Story” [16]. Engaging with these stories fosters cultural humility (as explained by Kibakaya et al., “cultural humility incorporates elements of self-questioning, immersion into an individual patient’s point of view, active listening and flexibility, which all serve to confront and address personal and cultural biases or assumptions”), which is increasingly recognized as an important foundation of health equity [17] (Commentary, page 2). The Food Story activity also encourages deeper exploration of both the internal wisdom in each person, and the wisdom of traditional dietary patterns from across the globe [18,19,20]. These are important perspectives for future health professionals to consider in conversations about food values with patients and communities.
Weekly culinary experiences during class provide opportunities for students to practice foundational cooking skills, interact with relevant food ingredients, learn to cook with a range of whole foods and spices and sample delicious tastes from a diversity of flavor profiles. Additional culinary assignments outside of class complement the goal of improving food literacy around choosing, procuring, preparing and consuming nourishing food. Mindful eating practices are a recurring and foundational facet of the course’s experiential elements, allowing students to practice self-awareness, examine the relationships between food and mood and to explore resources which may be supportive to both self and patient care.
Between weekly sessions, students are expected to complete assignments involving personal reflection, mindful eating experiences, review of relevant medical and nutrition literature and an online discussion forum about a personal cooking experience. The final project involves a patient case representing common clinical conditions in which students, assigned to interprofessional groups, are asked to design a meal recommendation as well as a patient education handout. The group creates a teaching video demonstrating their meal suggestion, explaining the relevance to the patient’s condition(s) and describing the cost per serving. The group also submits a brief academic paper, with supporting literature, for the rationale of their meal suggestion pertaining to the patient’s specific condition(s).
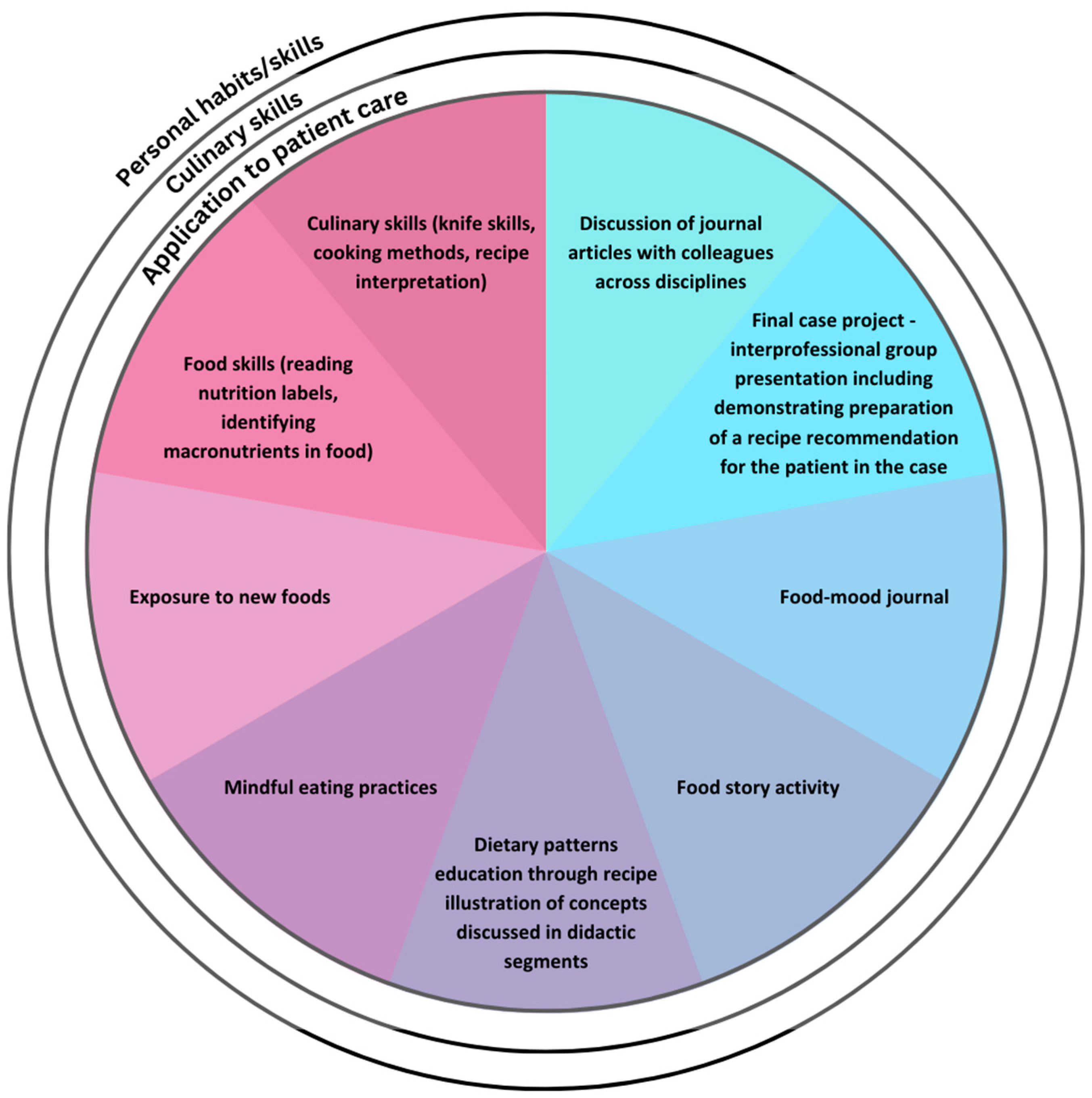
Of note, the elements of this course have been consistent throughout the last 7 years, though the delivery shifted to virtual due to the COVID-19 pandemic, and has continued as such based on feedback from students, as well as the increased access the virtual platform allows. See Figure 1 for the teaching methods used in the course.
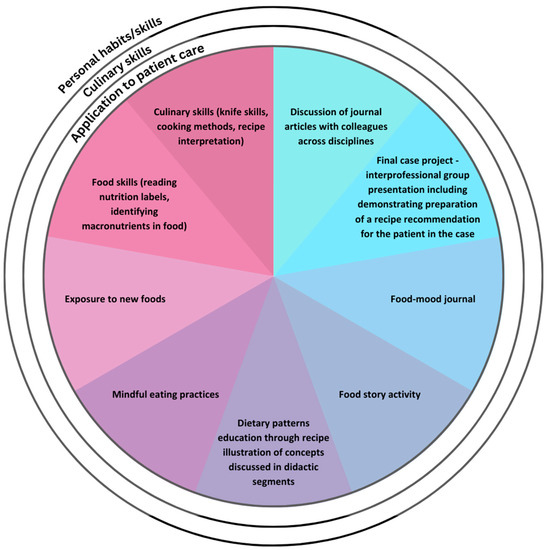
Figure 1.
Experiential methods employed in FMHP Course targeting personal, culinary and patient-care skills.
2.3. Data Collection and Statistical Analysis
Identical pre- and post-course surveys were administered through the REDCap® (Research Electronic Data Capture, version 13.1.37) system, hosted at the University of Minnesota, independent of the course evaluation process. Survey data, managed in REDCap, were de-identified and instructors were not aware of which students completed surveys. Completion of the surveys was optional for students and did not impact their grade. The study was determined to be exempt from full Institutional Review Board review.
Survey questions were developed after a pilot course indicated priority content including personal wellbeing; habits and approach to food; knowledge and skills to help a patient adapt a recipe according to dietary patterns or preferences; knowledge in relation to clinical practice; and application to clinical practice. Survey questions referenced specific topics or concepts that were addressed in the course, as well as knowledge or skills highlighted in the course objectives. By using an identical pre- and post-course survey, matched responses from students follow the same timeline relative to the intervention (the 6-week course). An appropriate five point Likert scale was created for each section of the survey. The draft survey questions were reviewed by three experts in the fields of medicine, nursing and public health, and validated for content. The complete survey questionnaire, “Food Matters for Health Professionals Survey”, is presented in the Supplementary Material section.
Participants’ demographics and characteristics were summarized using mean and standard deviation (SD) for continuous variables and frequency and percentage for categorical variables. Survey responses were summarized using mean and SD. Pre–post change was evaluated using a paired t test. Statistical analyses were performed in SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). P values of less than 0.05 were considered statistically significant.
Qualitative data were collected from a post-course reflective assignment which asks students to respond to the following prompts: (1) Choose one or two specific lessons or themes that resonated personally with you in some way. Write a 1–2 paragraph description of how this has or will impact your life or your eating in the days ahead. (2) Write a 1–2 paragraph description of how you can use what you learned from Food Matters in your professional context. De-identified, collated reflective assignments from six course cohorts (n = 69) were reviewed for frequency of codes derived through inductive coding.
3. Results
Changes in attitudes and knowledge were statistically significant in all areas, including personal well-being; habits and approach to food; knowledge and ability related to food and culinary practices; knowledge of dietary patterns; knowledge and skills to help a patient adapt a recipe according to dietary patterns or preferences; knowledge in relation to clinical practice; and application to clinical practice.
Figure 2, Figure 3, Figure 4 and Figure 5 display the changes between participants’ pre- and post-course survey responses for the following categories: “Knowledge to discuss dietary patterns/styles with a patient” (Figure 2), “Knowledge and skills to help a patient adapt recipes to a specific diet” (Figure 3), “Clinical application of specific nutrition concepts” (Figure 4) and “Practices around culinary nutrition in the clinical setting”, (Figure 5).
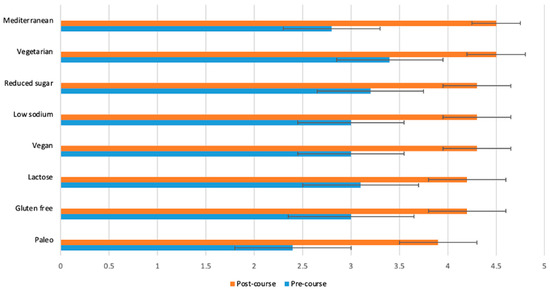
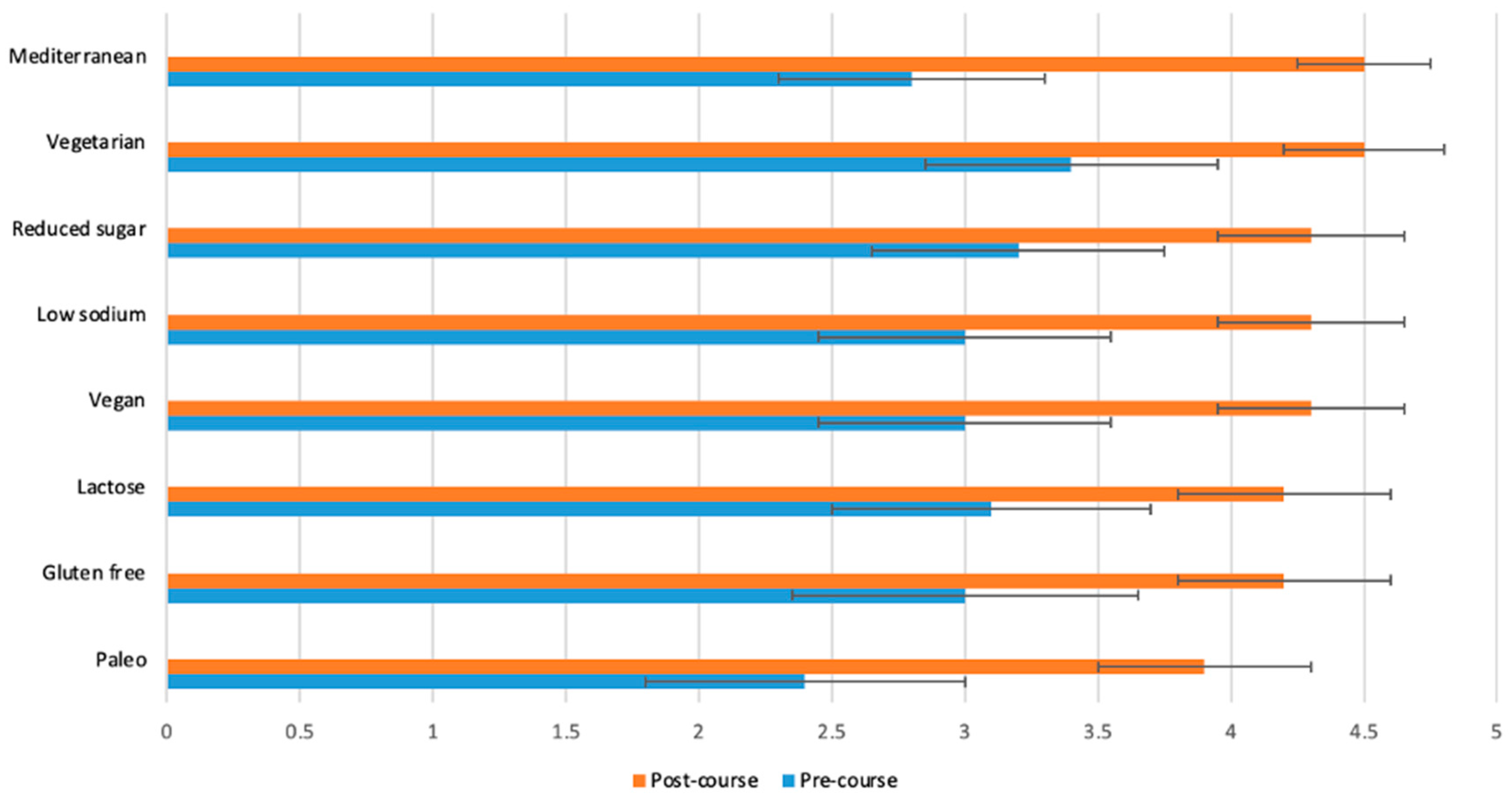
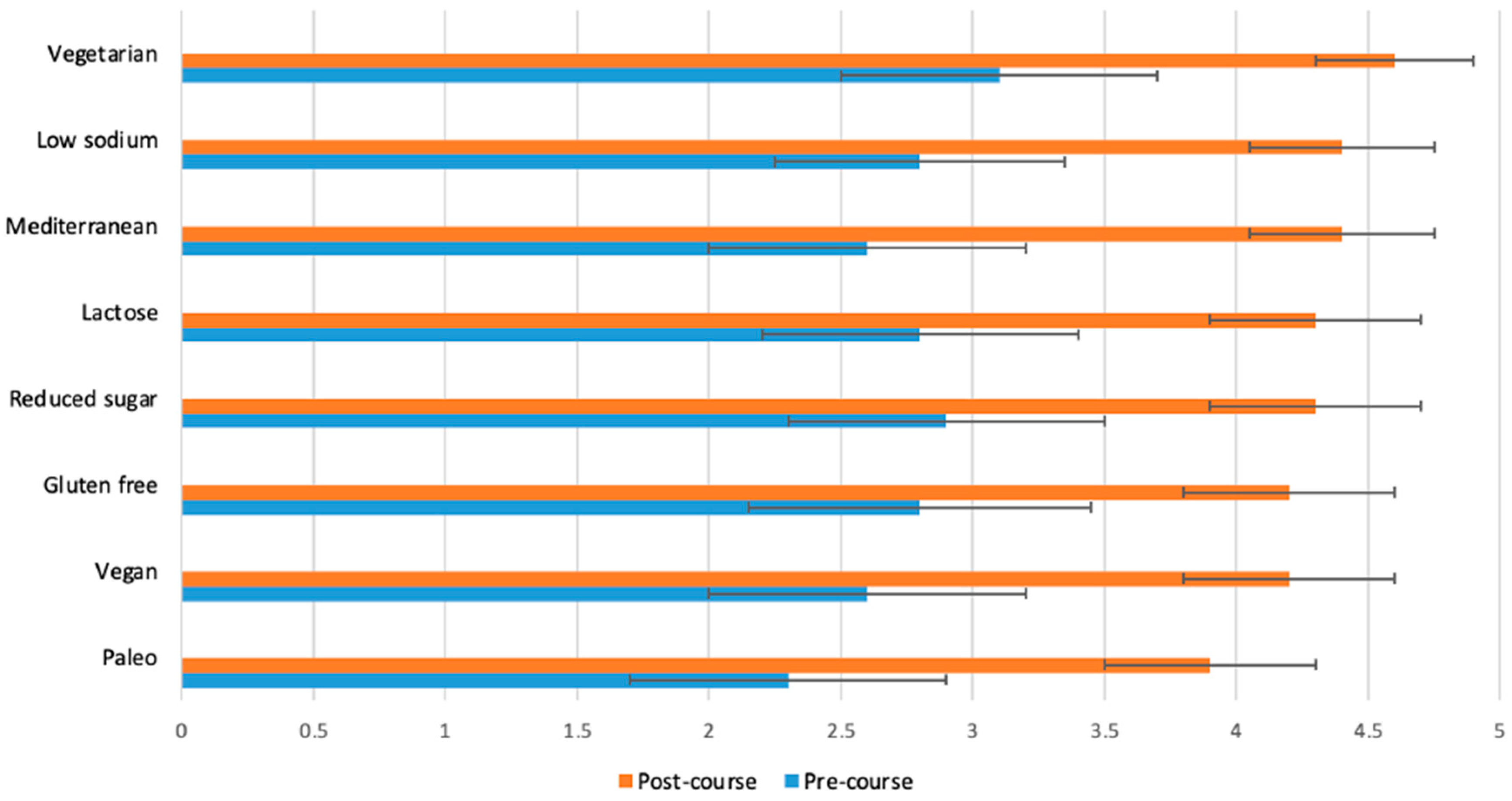
Figure 2.
Students (n = 65) were asked before and after the course to rate their response to the following statement on a scale from 1 (poor) to 5 (excellent): “I have sufficient knowledge to discuss each of the following diet styles with a patient or client”. The p-value for the change between pre- and post-course values was <0.0001 for all variables.
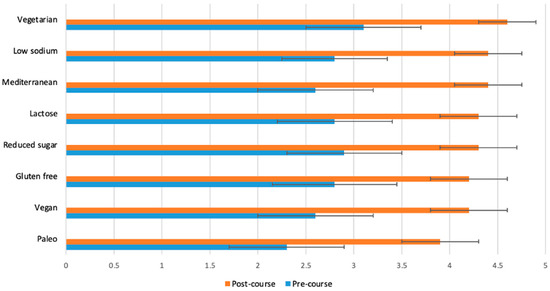
Figure 3.
Students (n = 65) were asked before and after the course to rate their response to the following statement on a scale from 1 (poor) to 5 (excellent): “I have sufficient knowledge and skills to help a patient adapt a recipe to each specific diet”. The p-value for the change between pre- and post-course values was <0.0001 for all variables.
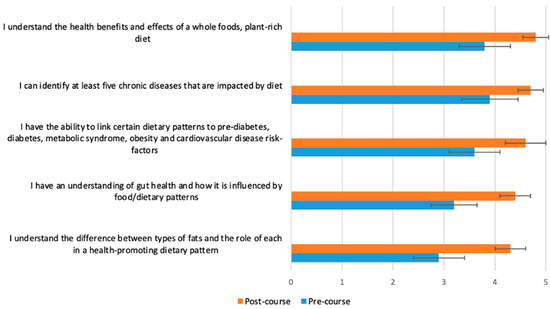
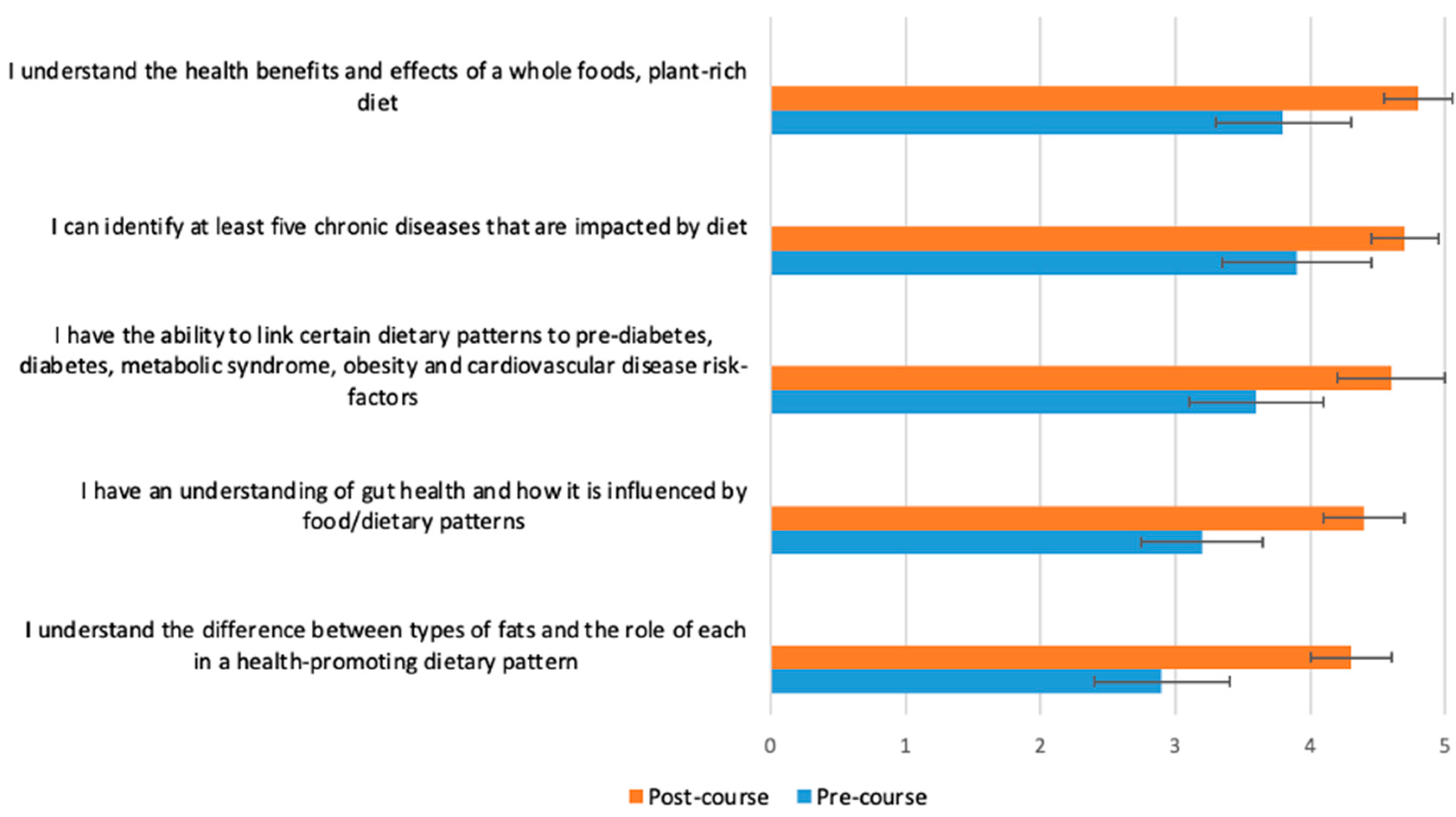
Figure 4.
Students (n = 65) were asked before and after the course to rate their response to the following statement on a scale from 1 (poor) to 5 (excellent): “Please rate your level of knowledge in the following areas”. The p-value for the change between pre- and post-course values was <0.0001 for all variables.
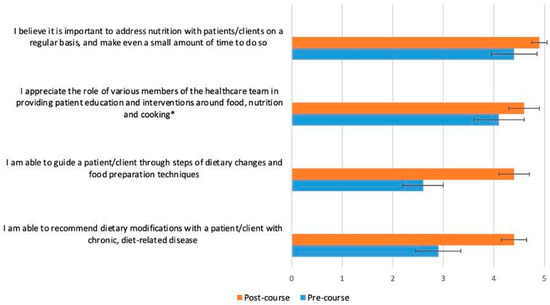
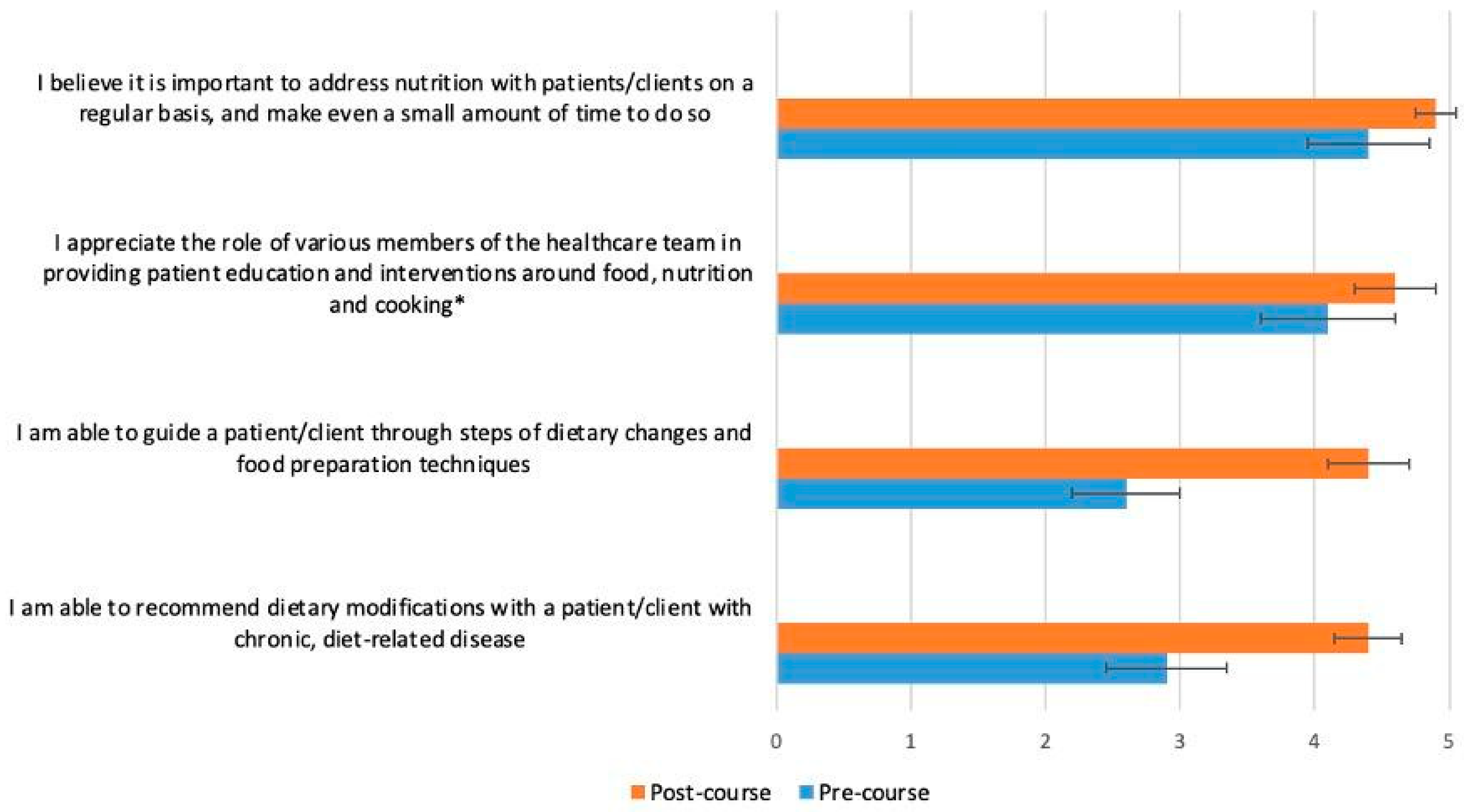
Figure 5.
Students (n = 65) were asked before and after the course to rate their response to the following statement on a scale from 1 (strongly disagree) to 5 (strongly agree), with intermediate choices of 2 (disagree), 3 (neutral) and 4 (agree): “Please rate your practices around culinary nutrition in the clinical setting”. The p-value for the change between pre- and post-course values was <0.0001 for all variables, except the one marked with an asterisk (*), which had a p-value of 0.0005.
The greatest changes between pre- and post-course survey responses were found in the following areas: discuss different dietary patterns with a patient (Figure 2); adapt a recipe according to dietary patterns or needs (Figure 3); specific knowledge concerning the relationship of food, nutrition and clinical conditions (gut health and fats, Figure 4); recommend dietary modifications to a patient with a chronic disease; and guide a patient through steps of dietary changes and food preparation techniques (Figure 5).
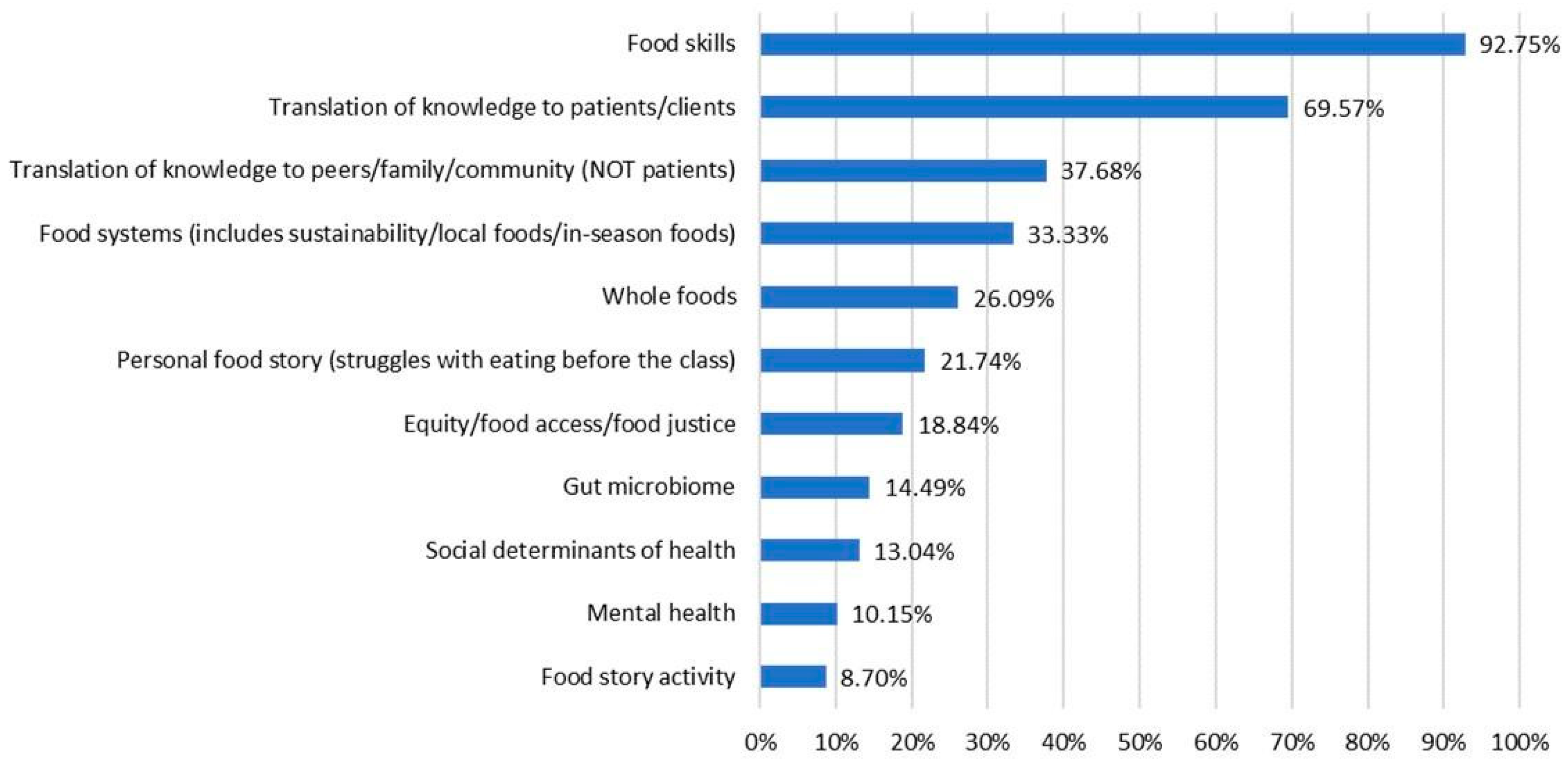
Inductive coding, starting with review of 10 post-course reflections to identify 11 codes, and subsequent coding of 69 student reflections yielded the highest frequency of references to the topic of food skills, followed by translation of knowledge to patients/clients, communicating with peers/family/community about what they learned and food systems concepts. Additional codes were found less frequently. Because this was a course assignment, these responses represent experiences from all students in the cohorts examined. The percentage of reflections mentioning each theme and example comments of each identified theme are provided in Figure 6 and Table 3.
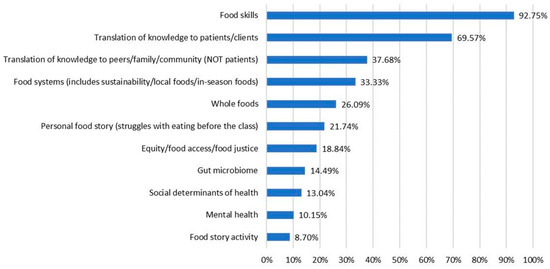
Figure 6.
Themes from reflective assignments and percentage of assignments mentioning each theme (n = 69). Students were instructed to reflect on two questions: “(1) Choose one or two specific lessons or themes that resonated personally with you in some way. Write a 1–2 paragraph description of how this has or will impact your life or your eating in the days ahead. (2) Write a 1–2 paragraph description of how you can use what you learned from Food Matters in your professional context”. De-identified, collated reflective assignments from six course cohorts (n = 69) were examined through an inductive coding process.
Table 3.
Selected quotes from each theme identified in students’ reflective assignments. (n = 69).
4. Discussion
Based on the quantitative and qualitative data gathered, experiential culinary education improved food skills and self-efficacy among survey respondents. Students reported improved knowledge of food systems, food skills, basic nutrition concepts and relationship to chronic disease conditions. Understanding and recognizing the spectrum of quality of foods and food products through a critical review of nutrition labels and ingredient lists, and having practical food skills to improve dietary quality, equips future health professionals to support patients and communities as they navigate the complexity of today’s food landscape.
Through our data analysis from both surveys and reflective responses, we see that not only did students’ knowledge of basic nutritional and culinary concepts increase between pre- and post-course, but their ability to apply the knowledge to clinical or professional practice also increased. An increase in self-perceived abilities and self-efficacy translates into confidence in practice [21].
This study has the following limitations: The pre-/post-course survey was optional for students enrolled in the course, and only survey responses with both pre- and post-course responses were used. The course is only required for the Integrative Health and Healing Doctorate of Nursing Practice (DNP) students, so for the majority of students, the course is elective. Self-selection or a predetermined interest in the subject matter could also influence students’ enrollment in the class, as well as pre- and post-survey responses. The majority of students responding to the survey identified as female, with only a small portion indicating male gender. There was no control group, so there is no standard of comparison with which to measure knowledge or attitudes on the topic areas. Because of these factors, the results of this study may not necessarily be generalized to a larger or more diverse population of graduate health sciences students.
Despite these limitations in the quantitative data, the qualitative data reflect the experience of all students enrolled in the cohorts examined and ultimately complement the survey results. Among the strengths of this study are the length of time over which the data have been collected, the diversity of health sciences fields represented and the alignment of the findings from qualitative and quantitative data.
Given that the qualitative data show a high frequency of “food skills” and “translation of knowledge to patients/clients” themes, an area of future research could explore the impact of an experiential food systems and nutrition course as a required part of health sciences curricula.
5. Conclusions
Health Sciences educators, major medical journals, Congress (see 2022 House Resolution 1118 that called “on medical schools, graduate medical education programs, and other health professional training programs to provide meaningful physician and health professional education on nutrition and diet”) and the larger public are calling for improved nutrition education for future physicians and health professionals [22,23].
We suggest that sharing experiences around food with other people from diverse fields of study and/or backgrounds promotes the development of cultural humility—a key ingredient for compassionate, informed and well-rounded health professionals, as well as humans. The benefit of an interprofessional course combined with elements such as hands-on cooking, the Food Story activity and examination of various dietary patterns appears to make an impact on students’ self-reported confidence and knowledge of food preparation and nutrition information.
These findings align with the growing body of literature supporting culinary and nutrition education for health professionals, yet includes the unique elements of food systems and interprofessional education. In order for nutrition education to be meaningful and memorable (and therefore effective), we believe our research indicates that such education needs to be experiential, clinically relevant, interprofessional and systems-oriented.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nu15183994/s1, The complete Pre-/Post Course Survey Tool “Food Matters for Health Professionals” used in this study is available in Supplementary Materials.
Author Contributions
Conceptualization, K.S. and J.B.; methodology, K.S. and J.B.; software, Q.W.; formal analysis, Q.W. and J.B.; data curation, Q.W.; visualization, Q.W. and N.V.; writing—original draft preparation, K.S., J.B., N.V. and Q.W.; writing—review and editing, K.S., J.B., N.V. and Q.W. All authors have read and agreed to the published version of the manuscript.
Funding
Clinical and Translational Science Institute, University of Minnesota, and the statistical analysis done by QW, is supported by the National Center for Advancing Translational Sciences of the National Institutes of Health Award Number UL1-TR002494. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the survey used for this study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy restrictions.
Acknowledgments
The authors would like to thank Mary Jo Kreitzer who served as a reviewer of this manuscript, and Christina Bushinger MPH Candidate (2023) who served as a graduate research assistant.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Food Systems—OECD. Available online: https://www.oecd.org/food-systems/ (accessed on 13 August 2023).
- Nguyen, H. Sustainable Food Systems: Concept and Framework; Food and Agriculture Organization of the United Nations: Rome, Italy, 2018. [Google Scholar]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT–Lancet Commission on Healthy Diets from Sustainable Food Systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Haines, A.; Ebi, K. The Imperative for Climate Action to Protect Health. N. Engl. J. Med. 2019, 380, 263–273. [Google Scholar] [CrossRef]
- Food Product Development. Available online: https://www.ksre.k-state.edu/kvafl/development.html (accessed on 15 August 2023).
- Zheng, L.; Sun, J.; Yu, X.; Zhang, D. Ultra-Processed Food Is Positively Associated With Depressive Symptoms Among United States Adults. Front. Nutr. 2020, 7, 600449. [Google Scholar] [CrossRef]
- Menichetti, G.; Ravandi, B.; Mozaffarian, D.; Barabási, A.-L. Machine Learning Prediction of the Degree of Food Processing. Nat. Commun. 2023, 14, 2312. [Google Scholar] [CrossRef] [PubMed]
- Juul, F.; Vaidean, G.; Lin, Y.; Deierlein, A.L.; Parekh, N. Ultra-Processed Foods and Incident Cardiovascular Disease in the Framingham Offspring Study. J. Am. Coll. Cardiol. 2021, 77, 1520–1531. [Google Scholar] [CrossRef] [PubMed]
- Elizabeth, L.; Machado, P.; Zinöcker, M.; Baker, P.; Lawrence, M. Ultra-Processed Foods and Health Outcomes: A Narrative Review. Nutrients 2020, 12, 1955. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.; Kurmas, N.; Burant, C.J.; Utech, A.; Steiber, A.; Julius, M. Cooking Classes: A Diabetes Self-Management Support Intervention Enhancing Clinical Values. Diabetes Educ. 2017, 43, 600–607. [Google Scholar] [CrossRef]
- Wolfson, J.A.; Bleich, S.N. Is Cooking at Home Associated with Better Diet Quality or Weight-Loss Intention? Public Health Nutr. 2015, 18, 1397–1406. [Google Scholar] [CrossRef]
- Gregory, C.A. Food Insecurity, Chronic Disease, and Health Among Working-Age Adults. Economic Research Report, 31 July 2017. [Google Scholar]
- Rivera, R.L.; Adams, M.; Dawkins, E.; Carter, A.; Zhang, X.; Tu, W.; Peña, A.; Holden, R.J.; Clark, D.O. Delivering Food Resources and Kitchen Skills (FoRKS) to Adults with Food Insecurity and Hypertension: A Pilot Study. Nutrients 2023, 15, 1452. [Google Scholar] [CrossRef] [PubMed]
- Pooler, J.A.; Srinivasan, M.; Wong, K.; Blitstein, J.L. Food Skills Education and Low-Income Adults’ Healthy Food Choices. Community Health Equity Res. Policy 2022, 43, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Lepre, B.; Mansfield, K.J.; Ray, S.; Beck, E.J. Nutrition Competencies for Medicine: An Integrative Review and Critical Synthesis. BMJ Open 2021, 11, e043066. [Google Scholar] [CrossRef] [PubMed]
- Teaching Kitchen Collaborative Research Day Abstracts. The Estate Yountville, Napa Valley, CA, USA February 7, 2018 A Day of Original Research and Innovative Strategies Involving Teaching Kitchens and Their Potential to Positively Impact Behaviors, Improve Health Outcomes, and Reduce Costs. J. Altern. Complement. Med. 2018, 24, A1–A21. [CrossRef]
- Kibakaya, E.C.; Oyeku, S.O. Cultural Humility: A Critical Step in Achieving Health Equity. Pediatrics 2022, 149, e2021052883. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, L.; Shatila, H.; Itani, L.; Hwalla, N.; Jomaa, L.; Naja, F. A Traditional Dietary Pattern Is Associated with Lower Odds of Overweight and Obesity among Preschool Children in Lebanon: A Cross-Sectional Study. Eur. J. Nutr. 2019, 58, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Why Traditional Diets? Available online: https://oldwayspt.org/traditional-diets/why-traditional-diets (accessed on 23 August 2023).
- Kromhout, D.; Menotti, A.; Alberti-Fidanza, A.; Puddu, P.E.; Hollman, P.; Kafatos, A.; Tolonen, H.; Adachi, H.; Jacobs, D.R. Comparative Ecologic Relationships of Saturated Fat, Sucrose, Food Groups, and a Mediterranean Food Pattern Score to 50-Year Coronary Heart Disease Mortality Rates among 16 Cohorts of the Seven Countries Study. Eur. J. Clin. Nutr. 2018, 72, 1103–1110. [Google Scholar] [CrossRef] [PubMed]
- “Confidence”. Available online: https://dictionary.cambridge.org/us/dictionary/english/confidence (accessed on 6 September 2023).
- Crowley, J.; Ball, L.; Hiddink, G.J. Nutrition in Medical Education: A Systematic Review. Lancet Planet. Health 2019, 3, e379–e389. [Google Scholar] [CrossRef] [PubMed]
- Rep. McGovern, J.P. [D-M.-2 Text—H.Res.1118—117th Congress (2021–2022): Expressing the Sense of the House of Representatives That the United States Recognizes the Mounting Personal and Financial Burden of Diet-Related Disease in the United States and Calls on Medical Schools, Graduate Medical Education Programs, and Other Health Professional Training Programs to Provide Meaningful Physician and Health Professional Education on Nutrition and Diet. Available online: http://www.congress.gov/bill/117th-congress/house-resolution/1118/text (accessed on 23 August 2023).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).