

Can Kindergarten Meals Improve the Daily Intake of Vegetables, Whole Grains, and Nuts among Preschool Children? A Randomized Controlled Evaluation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
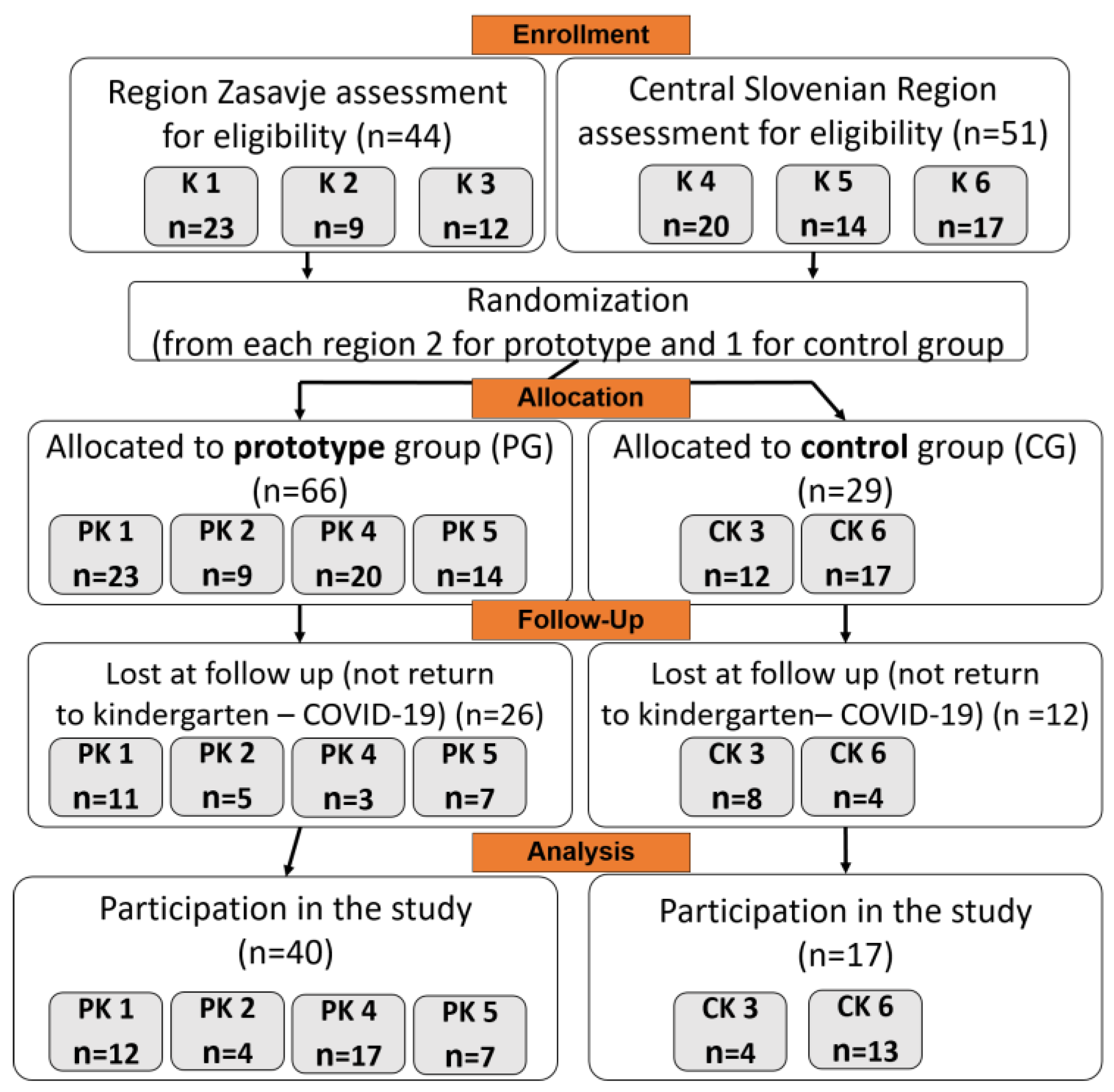
2.2. Participants
2.3. Anthropometric Measurements
2.4. Ethical Considerations
2.5. Dietary Survey
2.6. Dietary Intake Data Processing
2.7. Statistical Methods
3. Results
3.1. Participants and Settings
3.2. Anthropometric Measurements
3.3. Food Groups Offered in Kindergartens
3.4. Energy, Macronutrient, and Sodium Content in Kindergarten Meals
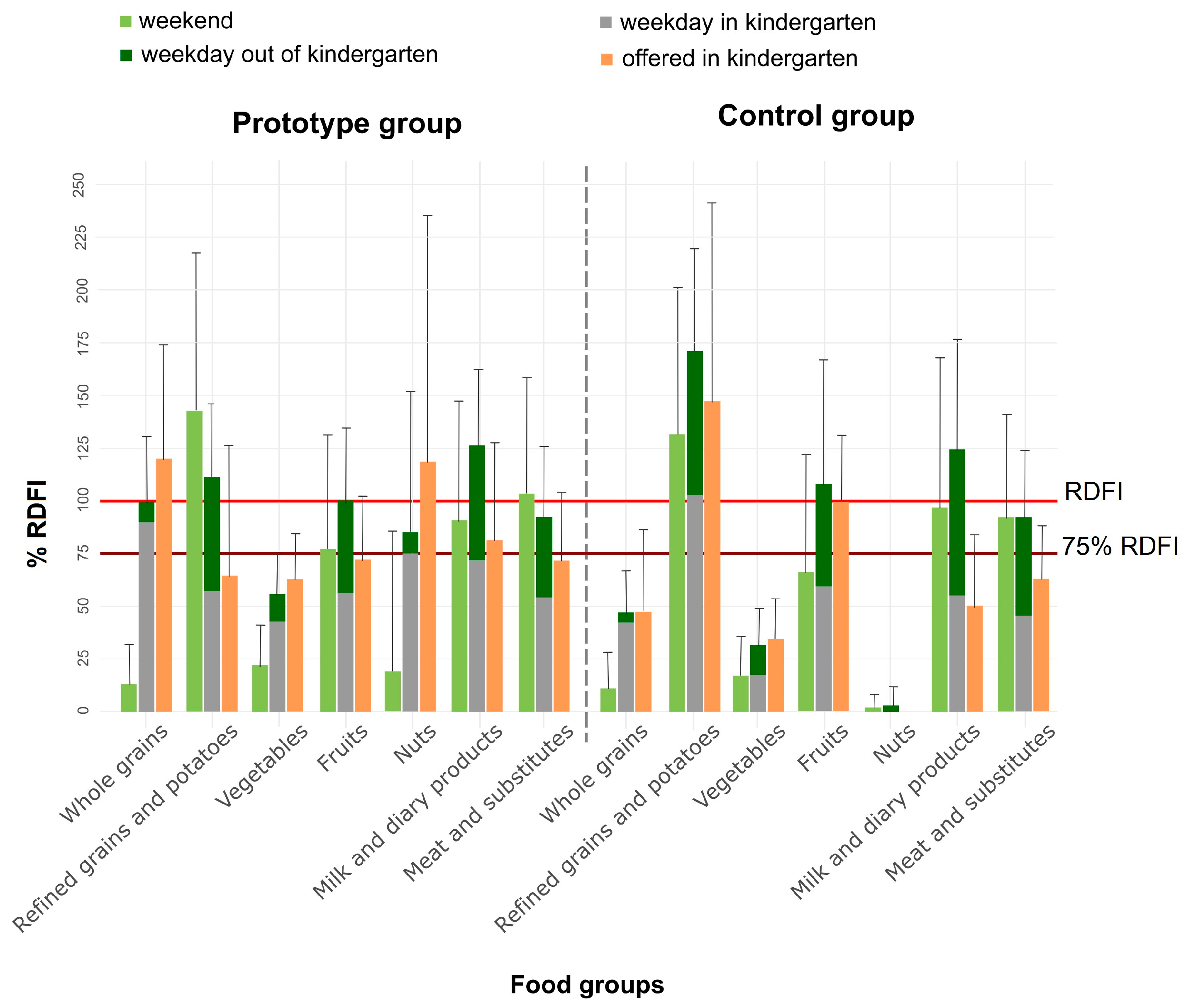
3.5. Food Intake in Kindergartens and Outside Kindergartens on Weekdays by the Prototype and Control Group Participants
3.6. Weekend food Intake among Participants in the Prototype and Control Group Compared with Weekday Intake
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Fernandez-Jimenez, R.; Al-Kazaz, M.; Jaslow, R.; Carvajal, I.; Fuster, V. Children present a window of opportunity for promoting health: JACC review topic of the week. J. Am. Coll. Cardiol. 2018, 72, 3310–3319. [Google Scholar] [CrossRef] [PubMed]
- Scaglioni, S.; Arrizza, C.; Vecchi, F.; Tedeschi, S. Determinants of children’s eating behavior. Am. J. Clin. Nutr. 2011, 94, 2006S–2011S. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. A World Ready to Learn: Prioritizing Quality Early Childhood Education. 2019. Available online: https://uni.cf/world-ready-to-learn-data (accessed on 8 July 2023).
- European Education and Culture Executive Agency/Eurydice. Eurydice Brief: Key Data on Early Childhood Education and Care in Europe; Publications Office of the European Union: Luxembourg, 2019; pp. 1–24. [Google Scholar] [CrossRef]
- Bowen, K.J.; Sullivan, V.K.; Kris-Etherton, P.M.; Petersen, K.S. Nutrition and cardiovascular disease—An update. Curr. Atheroscler Rep. 2018, 20, 8. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Noncommunicable Diseases Progress Monitor 2020. 2020. Available online: https://www.who.int/publications/i/item/9789240000490 (accessed on 15 September 2022).
- GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global burden of disease study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Miguel, M.; Oliveira, A.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Pozuelo-Carrascosa, D.P.; Soriano-Cano, A.; Martínez-Vizcaíno, V. Prevalence of overweight and obesity among European preschool children: A systematic review and meta-regression by food group consumption. Nutrients 2019, 11, 1698. [Google Scholar] [CrossRef]
- Liberali, R.; Kupek, E.; Assis, M.A.A. Dietary patterns and childhood obesity risk: A systematic review. Child. Obes. 2020, 16, 70–85. [Google Scholar] [CrossRef]
- Wall, C.R.; Stewart, A.W.; Hancox, R.J.; Murphy, R.; Braithwaite, I.; Beasley, R.; Mitchell, E. Association between frequency of consumption of fruit, vegetables, nuts and pulses and BMI: Analyses of the International study of asthma and allergies in childhood (ISAAC). Nutrients 2018, 10, 316. [Google Scholar] [CrossRef]
- Kovacs, V.A.; Messing, S.; Sandu, P.; Nardone, P.; Pizzi, E.; Hassapidou, M.; Brukalo, K.; Tecklenburg, E.; Abu-Omar, K. Improving the food environment in kindergartens and schools: An overview of policies and policy opportunities in Europe. Food Policy 2020, 96, 101848. [Google Scholar] [CrossRef]
- EFSA. Food Consumption Data. 2022. Available online: https://www.efsa.europa.eu/en/data-report/food-consumption-data (accessed on 3 January 2023).
- Blenkuš, M.G.; Pograjc, L.; Gregorčič, M.; Adamič, M.; Čampa, A. Smernice Zdravega Prehranjevanja v Vzgojno-izobraževalnih ustanovah (Od Prvega Leta Starosti Naprej). Minist. Za Zdr. 2005, 1–80. Available online: https://nijz.si/wp-content/uploads/2022/07/smernice_zdravega_prehranjevanja_v_viu.pdf (accessed on 15 September 2022).
- School Nutrition Act (Uradni list RS, št. 3/13, 46/14, 46/16—ZOFVI-K in 76/23). Available online: http://pisrs.si/Pis.web/pregledPredpisa?id=ZAKO6564 (accessed on 15 August 2023).
- NIJZ. Strokovno Spremljanje Prehrane s Svetovanjem v Vzgojno-Izobraževalnih Zavodih v Letu 2018. 2018. Available online: strokovno_spremljanje_prehrane_s_svetovanjem_v_vzgojno-izobrazevalnih_zavodih_v_letu_2015.pdf(nijz.si) (accessed on 15 September 2022).
- NIJZ. Različni Vidiki Prehranjevanja Prebivalcev Slovenije: V Starosti Od 3 Mesecev Do 74 Let. 2019. Available online: https://nijz.si/wp-content/uploads/2022/07/razlicni_vidiki_prehranjevanja_prebivalcev_slovenije.pdf (accessed on 3 January 2023).
- Tugault-Lafleur, C.N.; Black, J.L. Lunch on school days in Canada: Examining contributions to nutrient and food group intake and differences across eating locations. J. Acad. Nutr. Diet. 2020, 120, 1484–1497. [Google Scholar] [CrossRef]
- Luecking, C.T.; Mazzucca, S.; Vaughn, A.E.; Ward, D.S. Contributions of early care and education programs to diet quality in children aged 3 to 4 years in central North Carolina. J. Acad. Nutr. Diet. 2020, 120, 386–394. [Google Scholar] [CrossRef]
- Korkalo, L.; Nissinen, K.; Skaffari, E.; Vepsäläinen, H.; Lehto, R.; Kaukonen, R.; Koivusilta, L.; Sajaniemi, N.; Roos, E.; Erkkola, M. The contribution of preschool meals to the diet of Finnish preschoolers. Nutrients 2019, 11, 1531. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation 2018, 137, 67–492. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, A.; Mann, J.; Cummings, J.; Winter, N.; Mete, E.; Te Morenga, L. Carbohydrate quality and human health: A series of systematic reviews and meta-analyses. Lancet 2019, 393, 434–445. [Google Scholar] [CrossRef]
- Ros, E. Eat nuts, live longer. J. Am. Coll. Cardiol. 2017, 70, 2533–2535. [Google Scholar] [CrossRef]
- Lieffers, J.R.L.; Ekwaru, J.P.; Ohinmaa, A.; Veugelers, P.J. The economic burden of not meeting food recommendations in Canada: The cost of doing nothing. PLoS ONE 2018, 13, 0196333. [Google Scholar] [CrossRef] [PubMed]
- Hasnin, S.; Dev, D.A.; Tovar, A. Participation in the CACFP ensures availability but not intake of nutritious foods at lunch in preschool children in childcare centers. J. Acad. Nutr. Diet. 2020, 120, 1722–1729. [Google Scholar] [CrossRef]
- Sisson, S.B.; Kiger, A.C.; Anundson, K.C.; Rasbold, A.H.; Krampe, M.; Campbell, J.; Degrace, B.; Hoffman, L. Differences in preschool-age children’s dietary intake between meals consumed at childcare and at home. Prev. Med. Rep. 2017, 6, 33–37. [Google Scholar] [CrossRef]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- EFSA. General principles for the collection of national food consumption data in the view of a pan-European dietary survey. EFSA J. 2009, 7, 1435. [Google Scholar] [CrossRef]
- NIJZ. Slikovno Gradivo Za Določanje Vnosa Živil. 2017. Available online: https://www.nijz.si/wp-content/uploads/2022/07/slikovno_gradivo_nijz.pdf (accessed on 20 September 2022).
- Korošec, M.; Golob, T.; Bertoncelj, J.; Stibilj, V.; Seljak, B.K. The Slovenian food composition database. Food Chem. 2013, 140, 495–499. [Google Scholar] [CrossRef]
- Ross, A.B.; van der Kamp, J.W.; King, R.; Lê, K.A.; Mejborn, H.; Seal, C.J.; Thielecke, F.; Healthgrain Forum. Perspective: A definition for whole-grain food products-recommendations from the healthgrain forum. Adv. Nutr. 2017, 8, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Regulation (EC) 1924/2006 of the European Parliament and of the Council of 20 December 2006 on nutrition and health claims made on foods. Off. J. Eur. Communities 2006, L 404, 9–25. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A32006R1924 (accessed on 15 August 2023).
- Fagerland, M.W.; Sandvik, L. Performance of five two-sample location tests for skewed distributions with unequal variances. Contemp. Clin. Trials 2009, 30, 490–496. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. 2018. Available online: https://www.gbif.org/tool/81287/r-a-language-and-environment-for-statistical-computing (accessed on 1 October 2022).
- Deon, V.; Del Bo’, C.; Guaraldi, F.; Abello, F.; Belviso, S.; Porrini, M.; Riso, P.; Guardamagna, O. Effect of hazelnut on serum lipid profile and fatty acid composition of erythrocyte phospholipids in children and adolescents with primary hyperlipidemia: A randomized controlled trial. Clin. Nutr. 2018, 37, 1193–1201. [Google Scholar] [CrossRef]
- Berlic, M.; Jug, U.; Battelino, T.; Levart, A.; Dimitrovska, I.; Albreht, A.; Korošec, M. Antioxidant-rich foods and nutritional value in daily kindergarten menu: A randomized controlled evaluation executed in Slovenia. Food Chem. 2023, 404, 134566. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, J.R.; Cezaro, C.D.; Fisberg, R.M.; Fisberg, M.; Vitolo, M.R. Estimation of energy and macronutrient intake at home and in the kindergarten programs in preschool children. J. Pediatr. 2010, 86, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Andreyeva, T.; Kenney, E.L.; O’Connell, M.; Sun, X.; Henderson, K.E. Predictors of nutrition quality in early child education settings in Connecticut. J. Nutr. Educ. Behav. 2018, 50, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Romo-Palafox, M.J.; Ranjit, N.; Sweitzer, S.J.; Roberts-Gray, C.; Byrd-Williams, C.E.; Briley, M.E.; Hoelscher, D.M. Adequacy of parent-packed lunches and preschooler’s consumption compared to dietary reference intake recommendations. J. Am. Coll. Nutr. 2017, 36, 169–176. [Google Scholar] [CrossRef]
- Robson, S.M.; Khoury, J.C.; Kalkwarf, H.J.; Copeland, K. Dietary intake of children attending full-time child care: What are they eating away from the childcare center? J. Acad. Nutr. Diet. 2015, 115, 1472–1478. [Google Scholar] [CrossRef]
- Embling, R.; Pink, A.E.; Gatzemeier, J.; Price, M.D.; Lee, M.; Wilkinson, L.L. Effect of food variety on intake of a meal: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2021, 113, 716–741. [Google Scholar] [CrossRef]
- Roe, L.S.; Meengs, J.S.; Birch, L.L.; Rolls, B.J. Serving a variety of vegetables and fruit as a snack increased intake in preschool children. Am. J. Clin. Nutr. 2013, 98, 693–699. [Google Scholar] [CrossRef]
- Roe, L.S.; Sanchez, C.E.; Smethers, A.D.; Keller, K.L.; Rolls, B.J. Portion size can be used strategically to increase intake of vegetables and fruits in young children over multiple days: A cluster-randomized crossover trial. Am. J. Clin. Nutr. 2022, 115, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Spill, M.K.; Birch, L.L.; Roe, L.S.; Rolls, B.J. Hiding vegetables to reduce energy density: An effective strategy to increase children’s vegetable intake and reduce energy intake. Am. J. Clin. Nutr. 2011, 94, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Larrosa, S.; Luque, V.; Grote, V.; Closa-Monasterolo, R.; Ferré, N.; Koletzko, B.; Verduci, E.; Gruszfeld, D.; Xhonneux, A.; Escribano, J. Fibre intake is associated with cardiovascular health in European children. Nutrients 2020, 13, 12. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Bi, Y.; Tang, X.; Zhang, P.; Tong, J.; Peng, X.; Tian, J.; Liang, X. Protective effects of appropriate amount of nuts intake on childhood blood pressure level: A cross-sectional study. Front. Med. 2022, 8, 793672. [Google Scholar] [CrossRef] [PubMed]
- Mead, L.C.; Hill, A.M.; Carter, S.; Coates, A.M. The effect of nut consumption on diet quality, cardiometabolic and gastrointestinal health in children: A systematic review of randomized controlled trials. Int. J. Environ. Res. Public Health 2021, 18, 454. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, T.; Sicherer, S. Current perspectives on tree nut allergy: A review. J. Asthma Allergy 2018, 11, 41–51. [Google Scholar] [CrossRef]
- Taylor, C.M.; Emmett, P.M. Picky eating in children: Causes and consequences. Proc. Nutr. Soc. 2019, 78, 161–169. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Food Groups 1 | Meat and Substitutes (g) | Milk and Dairy Products (g) | Fruits (g) | Vegetables (g) | Nuts (g) | Whole Grains (g) | Refined Grains and Potatoes (g) | |
|---|---|---|---|---|---|---|---|---|
| Variable of interest | RDFI 2 4–6 years (75% RDFI) 3 | 110 (82.5) | 400 4 (300) | 200 (150) | 300 (225) | 11 5 (8) | 115 6 (86) | 115 6 (86) |
| Offered in kindergarten Mean (SD) 7 | PG | 78 (36) | 325 (162) | 143 (61) | 188 (66) | 14 (13) | 137 (62) | 74 (71) |
| CG | 69 (28) | 200 (136) | 198 (64) | 103 (58) | 0 | 54 (45) | 169 (108) | |
| p-value | 1 | 0.231 | 0.233 | 0.011 * | <0.001 * | 0.002 * | 0.152 | |
| Weekday in kindergartens Mean (SD) 8 | PG | 59 (23) | 289 (94) | 112 (34) | 136 (48) | 8 (6) | 106 (35) | 66 (23) |
| CG | 50 (24) | 220 (101) | 134 (74) | 60 (51) | 0 | 49 (26) | 119 (48) | |
| p-value | 1 | 0.137 | 1 | <0.001 * | <0.001 * | <0.001 * | 0.002 * | |
| Weekdays outside kindergartens Mean (SD) 9 | PG | 42 (28) | 216 (111) | 88 (65) | 33 (31) | 0.8 (3) | 9 (13) | 62 (39) |
| CG | 51 (29) | 275 (199) | 82 (64) | 35 (36) | 0.3 (1) | 5 (10) | 78 (39) | |
| p-value | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| Total weekdays Mean (SD) | PG | 101 (37) | 505 (145) | 200 (80) | 169 (59) | 8.3 (7) | 115 (36) | 128 (40) |
| CG | 101 (35) | 495 (210) | 216 (118) | 95 (53) | 0.3 (1) | 54 (23) | 197 (56) | |
| p-value | 1 | 1 | 1 | <0.001 * | <0.001 * | <0.001 * | 0.005 * | |
| Total Weekend Mean (SD) 10 | PG | 113 (61) | 365 (227) | 153 (109) | 66 (58) | 2 (7) | 13 (22) | 164 (86) |
| CG | 101 (54) | 388 (285) | 131 (112) | 52 (57) | 0.2 (0.7) | 13 (20) | 152 (80) | |
| p-value | 1 | 1 | 1 | 1 | 0.288 | 1 | 1 |
| Energy (kcal) | Total Fat (g) | Protein (g) | CH (g) | DF (g) | Na (mg) | ||
|---|---|---|---|---|---|---|---|
| Variable of interest | DRI 1 4–6 years. (75% DRI) 2 | 1550 (1162) | 52–60 (39–45) | 39–58 (29–44) | >194 (>146) | ˃15 (˃11) | <1180 (880) |
| Offered in kindergartens Mean (SD) 3 | PG | 1115 (221) | 43 (12) | 39 (7) | 143 (31) | 20 (5) | 1983 (1148) |
| CG | 883 (178) | 25 (12) | 35 (8) | 128 (30) | 14 (5) | 1605 (718) | |
| p-value | 0.031 * | <0.001 * | 1 | 1 | 0.017 * | 1 | |
| Weekday in kindergartens Mean (SD) 4 | PG | 830 (176) | 30 (8) | 29 (6) | 112 (23) | 15 (3) | 1478 (400) |
| CG | 664 (239) | 20 (8) | 28 (11) | 94 (34) | 10 (4) | 1126 (521) | |
| p-value | 0.097 | <0.001 * | 1 | 0.334 | <0.001 * | 0.196 | |
| Weekdays outside kindergartens Mean (SD) 5 | PG | 660 (206) | 25 (9) | 22 (8) | 87 (30) | 6 (2) | 687 (286) |
| CG | 799 (289) | 32 (15) | 27 (8) | 101 (37) | 6 (3) | 757 (366) | |
| p-value | 0.508 | 0.587 | 0.227 | 0.956 | 1 | 1 | |
| Total weekdays Mean (SD) | PG | 1486 (250) | 55 (12) | 50 (10) | 198 (35) | 21 (4) | 2154 (463) |
| CG | 1462 (317) | 52 (16) | 54 (11) | 195 (46) | 16 (5) | 1910 (517) | |
| p-value | 1 | 1 | 1 | 1 | 0.010 * | 0.627 | |
| Total Weekend Mean (SD) 6 | PG | 1336 (374) | 50 (17) | 48 (14) | 173 (56) | 11 (5) | 1648 (852) |
| CG | 1440 (289) | 57 (15) | 48 (8) | 183 (44) | 12 (3) | 1519 (527) | |
| p-value | 1 | 0.808 | 1 | 1 | 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berlic, M.; Battelino, T.; Korošec, M. Can Kindergarten Meals Improve the Daily Intake of Vegetables, Whole Grains, and Nuts among Preschool Children? A Randomized Controlled Evaluation. Nutrients 2023, 15, 4088. https://doi.org/10.3390/nu15184088
Berlic M, Battelino T, Korošec M. Can Kindergarten Meals Improve the Daily Intake of Vegetables, Whole Grains, and Nuts among Preschool Children? A Randomized Controlled Evaluation. Nutrients. 2023; 15(18):4088. https://doi.org/10.3390/nu15184088
Chicago/Turabian StyleBerlic, Maja, Tadej Battelino, and Mojca Korošec. 2023. "Can Kindergarten Meals Improve the Daily Intake of Vegetables, Whole Grains, and Nuts among Preschool Children? A Randomized Controlled Evaluation" Nutrients 15, no. 18: 4088. https://doi.org/10.3390/nu15184088
APA StyleBerlic, M., Battelino, T., & Korošec, M. (2023). Can Kindergarten Meals Improve the Daily Intake of Vegetables, Whole Grains, and Nuts among Preschool Children? A Randomized Controlled Evaluation. Nutrients, 15(18), 4088. https://doi.org/10.3390/nu15184088