
Racial and Ethnic Comparisons in Satisfaction with Services Provided by the Special Supplemental Nutrition Program for Women, Infants, and Children in California

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
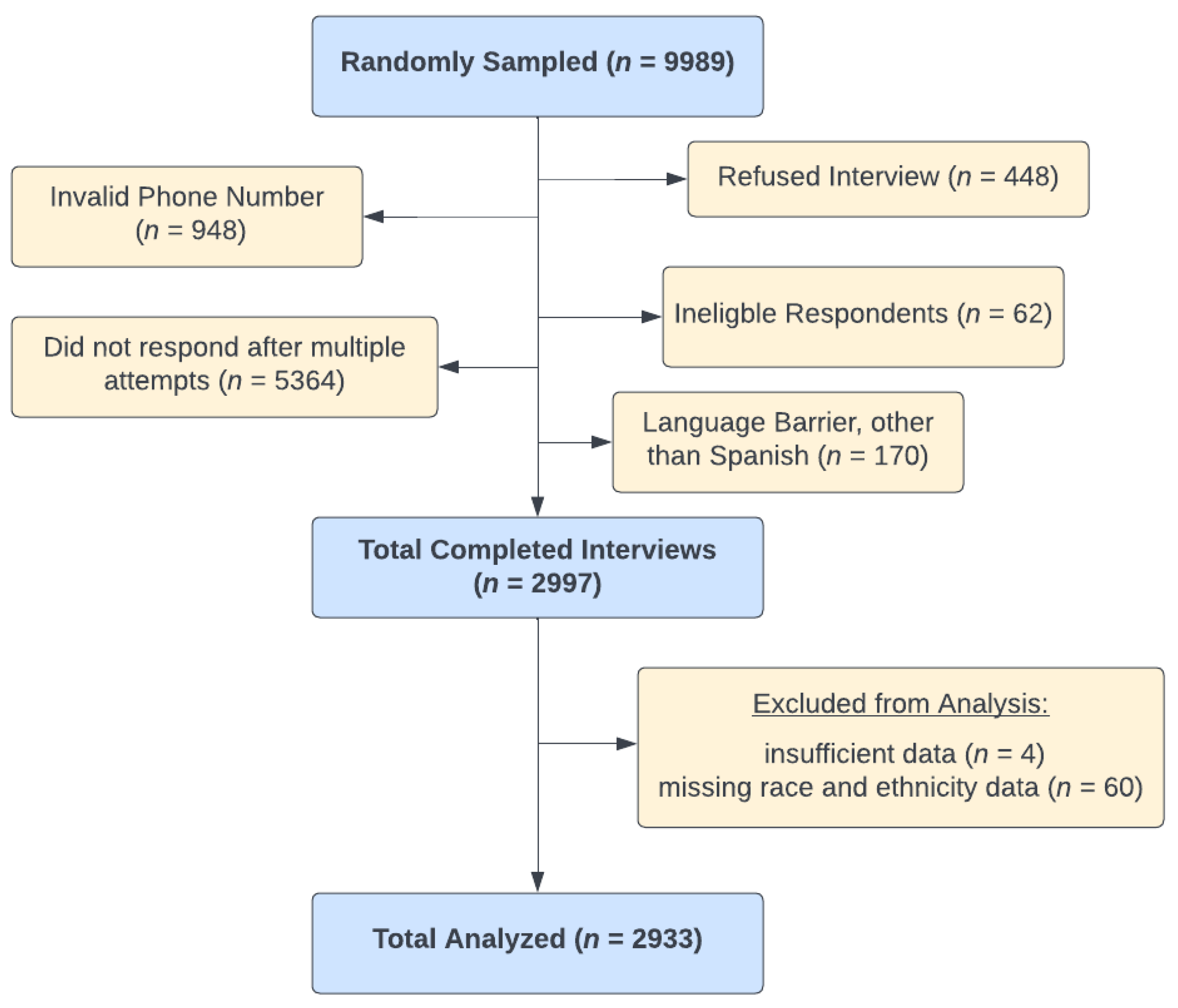
2.1. Survey Respondents
2.2. Survey Development and Administration
2.3. Data Analysis
3. Results
3.1. Respondent Characteristics
3.2. WIC Nutrition Education
3.3. Value of WIC Participation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- U.S. Department of Agriculture. Food and Nutrition Service; Summary, W.D.T.N.L.A., Ed.; U.S. Department of Agriculture: Washington, DC, USA, 2020.
- Oliveira, V.; Elizabeth, R.; Jennifer, O.; Ghelfi, L.M. The WIC Program Background, Trends, and Issues; US Department of Agriculture, Economic Research Service: Washington, DC, USA, 2002. [Google Scholar]
- Ng, S.W.; Hollingsworth, B.A.; Busey, E.A.; Wandell, J.L.; Miles, D.R.; Poti, J.M. Federal Nutrition Program Revisions Impact Low-income Households’ Food Purchases. Am. J. Prev. Med. 2018, 54, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Kreider, B.; Pepper, J.V.; Roy, M. Identifying the Effects of WIC on Food Insecurity Among Infants and Children. South. Econ. J. 2016, 82, 1106–1122. [Google Scholar] [CrossRef]
- Andreyeva, T.; Tripp, A.S. The healthfulness of food and beverage purchases after the federal food package revisions: The case of two New England states. Prev. Med. 2016, 91, 204–210. [Google Scholar] [CrossRef] [Green Version]
- Tester, J.M.; Leung, C.W.; Crawford, P.B. Revised WIC Food Package and Children’s Diet Quality. Pediatrics 2016, 137, e20153557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jun, S.; Catellier, D.J.; Eldridge, A.L.; Dwyer, J.T.; Eicher-Miller, H.A.; Bailey, R.L. Usual Nutrient Intakes from the Diets of US Children by WIC Participation and Income: Findings from the Feeding Infants and Toddlers Study (FITS) 2016. J. Nutr. 2018, 148, 1567S–1574S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmer, M.C.; Vernarelli, J.A. Changes in nutrient and food group intakes among children and women participating in the Special Supplemental Nutrition Program for Women, Infants, and Children: Findings from the 2005-2008 and 2011-2014 National Health and Nutrition Examination Surveys. Public Health Nutr. 2019, 22, 3309–3314. [Google Scholar] [CrossRef] [PubMed]
- Weinfield, N.S.; Borger, C.; Au, L.E.; Whaley, S.E.; Berman, D.; Ritchie, L.D. Longer Participation in WIC Is Associated with Better Diet Quality in 24-Month-Old Children. J. Acad. Nutr. Diet. 2020, 120, 963–971. [Google Scholar] [CrossRef]
- Daepp, M.I.G.; Gortmaker, S.L.; Wang, Y.C.; Long, M.W.; Kenney, E.L. WIC Food Package Changes: Trends in Childhood Obesity Prevalence. Pediatrics 2019, 143, e20182841. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture. National- and State-Level Estimates of Special Supplemental Nutrition Program for Women, INfants, and Children (WIC) Eligibles and Program Reach in 2016. Available online: https://www.fns.usda.gov/wic/national-and-state-level-estimates-wic-eligibility-and-wic-program-reach-2018-updated (accessed on 12 February 2019).
- Borger, C.; Paolicelli, C.P.; Sun, B. Duration of Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) Participation is Associated With Children’s Diet Quality at Age 3 Years. Am. J. Prev. Med. 2022, 62, e343–e350. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture. WIC Program Nutrition Education Guidance; Service, F.a.N., Ed.; U.S. Department of Agriculture: Washington, DC, USA, 2006.
- Anderson, C.E.; O’Malley, K.; Martinez, C.E.; Ritchie, L.D.; Whaley, S.E. Longer Family Participation in WIC is Associated With Lower Childhood Sugar-Sweetened Beverage Intake. J. Nutr. Educ. Behav. 2022, 54, 239–248. [Google Scholar] [CrossRef]
- Ritchie, L.D.; Whaley, S.E.; Spector, P.; Gomez, J.; Crawford, P.B. Favorable impact of nutrition education on California WIC families. J. Nutr. Educ. Behav. 2010, 42 (Suppl. 3), S2–S10. [Google Scholar] [CrossRef]
- Vasan, A.; Kenyon, C.C.; Feudtner, C.; Fiks, A.G.; Venkataramani, A.S. Association of WIC Participation and Electronic Benefits Transfer Implementation. JAMA Pediatr. 2021, 175, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Cates, S.; Kristen, C.; Linnea, S.; Karen, D.; Celia, E.; Shawn, K.; Samantha, B.; Jenna, K.B.; Karen, C.-B. WIC Nutrition Education Study: Phase 1 Report; U.S. Department of Agriculture, Food and Nutrition Service: Alexandria, VA, USA, 2016. [Google Scholar]
- U.S. Department of Agriculture, F.a.N.S. Revitalizing Quality Nutrition Services (RQNS). Available online: https://www.fns.usda.gov/wic/revitalizing-quality-nutrition-services-rqns#:~:text=What%20is%20the%20Goal%20of,and%20maintain%20optimal%20nutritional%20status. (accessed on 30 July 2020).
- Ritchie, L.D.; Whaley, S.E.; Crocker, N.J. Satisfaction of California WIC participants with food package changes. J. Nutr. Educ. Behav. 2014, 46 (Suppl. 3), S71–S78. [Google Scholar] [CrossRef]
- Hager, E.R.; Quigg, A.M.; Black, M.M.; Coleman, S.M.; Heeren, T.; Rose-Jacobs, R.; Cook, J.T.; de Cuba, S.A.E.; Casey, P.H.; Chilton, M.; et al. Development and validity of a 2-item screen to identify families at risk for food insecurity. Pediatrics 2010, 126, e26–e32. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.H.; Liu, H. Concerns and Structural Barriers Associated with WIC Participation among WIC-Eligible Women. Public Health Nurs. 2016, 33, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Au, L.E.; Whaley, S.; Gurzo, K.; Meza, M.; Ritchie, L.D. If You Build It They Will Come: Satisfaction of WIC Participants With Online and Traditional In-Person Nutrition Education. J. Nutr. Educ. Behav. 2016, 48, 336–342.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whaley, S.E.; Anderson, C.E. The Importance of Federal Waivers and Technology in Ensuring Access to WIC During COVID-19. Am. J. Public Health 2021, 111, 1009–1012. [Google Scholar] [CrossRef] [PubMed]
- McElrone, M.; Zimmer, M.C.; Anderson Steeves, E.T. A Qualitative Exploration of Predominantly White Non-Hispanic Tennessee WIC Participants’ Food Retail and WIC Clinic Experiences During COVID-19. J. Acad. Nutr. Diet. 2021, 121, 1454–1462. [Google Scholar] [CrossRef]
- Au, L.E.; Whaley, S.E.; Hecht, C.A.; Tsai, M.M.; Anderson, C.E.; Chaney, A.M.; Vital, N.; Martinez, C.E.; Ritchie, L.D. A Qualitative Examination of California WIC Participants’ and Local Agency Directors’ Experiences during the COVID-19 Pandemic. J. Acad. Nutr. Diet. 2022, 122, 2218–2227.e21. [Google Scholar] [CrossRef] [PubMed]
- Morris, E.J.; Otten, J.J.; Quinn, E.L.; Rose, C.M.; Spiker, M.; Leary, J.O. Insights from Washington State’s COVID-19 response: A mixed-methods evaluation of WIC remote services and expanded food options using the RE-AIM framework. J. Acad. Nutr. Diet. 2022, 122, 2228–2242.e7. [Google Scholar] [CrossRef]
- Katz, V.S.; Gonzalez, C.; Clark, K. Digital Inequality and Developmental Trajectories of Low-income, Immigrant, and Minority Children. Pediatrics 2017, 140 (Suppl. 2), S132–S136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritchie, L.L.D.; Linnea, S.; Christina, C.; Georgia, M.; Loan, K.; Lanxin, S.; Shannon, E.W. Multi-State WIC Participant Satisfaction Survey: Learning from Program Adaptations during COVID; WIC Research Policy Practice: Washington, DC, USA, 2021. [Google Scholar]
- Henchy, G. Making WIC Work Better: Strategies to Reach More Women and Children and Strengthen Benefits Use; Food Research & Action Center: Washington, DC, USA, 2019. [Google Scholar]
- Sheridan, M.; Ferrant, C. Participation in the Women, Infants and Children (WIC) Program: A Synthesis of the Literature. Sciences Po University Press: Paris, France, 2022. [Google Scholar]
- Au, L.E.; Ritchie, L.D.; Tsai, M.; Randel-Schreiber, H.R.; Martinez, C.; Gradziel, P.H.; Sabatier, S.M.; Whaley, S.E. Alignment of California WIC Participant Preferences With Proposed WIC Food Package Recommendations. J. Nutr. Educ. Behav. 2021, 53, 60–66. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total (n = 2993) | Race/Ethnicity 2 | ||||||
|---|---|---|---|---|---|---|---|
| Non-Hispanic White (n = 374) | Hispanic English-Speaking (n = 753) | Hispanic Spanish-Speaking (n = 1445) | Non-Hispanic Black (n = 119) | Asian (n = 89) | Other 3 (n = 153) | ||
| Age of child under study (mean years, SD) | 2.5 (1.1) | 2.4 (1.1) | 2.5 (1.0) | 2.6 (1.1) | 2.4 (1.0) | 2.4 (0.9) | 2.4 (1.0) |
| Sex of child under study (n, % female) | 1439 (49.1) | 179 (47.9) | 359 (47.7) | 705 (48.8) | 68 (57.1) | 44 (49.4) | 84 (54.9) |
| Child under study currently in WIC (n, %) | 2753 (93.9) | 343 (91.7) | 694 (92.2) | 1380 (95.5) | 112 (94.1) | 80 (89.9) | 144 (94.1) |
| Number of months household participated in WIC (mean, SD) | 70.7 (52.4) | 61.6 (47.7) | 59.3 (46.6) | 81.9 (54.7) | 74.4 (60.8) | 50.9 (45.4) | 51.8 (39.3) |
| Number of young children (<5 y) in household (mean, SD) | 1.2 (0.5) | 1.3 (0.5) | 1.3 (0.5) | 1.2 (0.4) | 1.3 (0.5) | 1.3 (0.5) | 1.3 (0.5) |
| Highest level of education of respondent (n, %) | |||||||
| 8th grade or less | 468 (16.4) | 19 (5.1) | 3 (0.4) | 437 (30.6) | 0 (0) | 1 (1.2) | 8 (5.2) |
| Some high school | 5494 (17.0) | 32 (8.6) | 79 (10.5) | 356 (24.9) | 8 (6.7) | 6 (7.0) | 13 (8.5) |
| High school graduate | 946 (32.5) | 119 (31.8) | 270 (35.9) | 455 (31.8) | 35 (29.4) | 20 (23.3) | 47 (30.7) |
| Some college or trade school | 735 (25.2) | 141 (37.7) | 329 (43.8) | 105 (7.3) | 57 (47.9) | 35 (40.7) | 68 (44.4) |
| College graduate or more | 271 (9.3) | 63 (16.8) | 71 (9.4) | 77 (5.4) | 19 (16.0) | 24 (27.9) | 17 (11.1) |
| Respondent working for pay 4 (n, %) | 1229 (42.1) | 176 (47.2) | 375 (49.8) | 515 (35.8) | 60 (50.9) | 36 (41.4) | 67 (43.8) |
| Household receives SNAP 5 (n, %) | 1103 (37.8) | 147 (39.3) | 280 (37.3) | 513 (35.7) | 71 (60.2) | 24 (27.0) | 68 (44.7) |
| Household receives Medicaid (n, %) | 2515 (86.6) | 309 (82.6) | 640 (85.5) | 1250 (88.0) | 109 (91.6) | 74 (83.2) | 133 (86.9) |
| Household experienced food insecurity in prior 12 months (n, %) | 1459 (49.8) | 200 (53.5) | 378 (50.2) | 682 (47.3) | 60 (50.4) | 47 (52.8) | 92 (60.1) |
| Total (n = 2933) | Race/Ethnicity 2 | |||||||
|---|---|---|---|---|---|---|---|---|
| Non-Hispanic White (n = 374) | Hispanic English-Speaking (n = 753) | Hispanic Spanish-Speaking (n = 1445) | Non-Hispanic Black (n = 119) | Asian (n = 89) | Other 3 (n = 153) | p Value 4 | ||
| (n, %) | ||||||||
| Modes of WIC nutrition education currently received 5 | ||||||||
| One-on-one in person | 2678 (91.3) | 334 (89.3) | 685 (91.0) | 1334 (92.3) | 110 (92.4) | 80 (89.9) | 135 (88.2) | 0.3 |
| Video/DVD | 2192 (74.7) | 254 (67.9) a | 559 (74.2) ab | 1120 (77.5) b | 84 (70.6) ab | 65 (73.0) ab | 110 (71.9) ab | 0.004 |
| Group session in person | 1832 (62.6) | 189 (50.5) ac | 434 (57.6) a | 1021 (70.7) b | 50 (42.0) c | 49 (55.1) ac | 89 (58.2) ac | <0.001 |
| Online | 1682 (57.5) | 254 (67.9) a | 551 (73.2) a | 628 (43.5) b | 79 (66.4) a | 67 (75.3) a | 103 (67.3) a | <0.001 |
| Two-way texting | 875 (29.8) | 84 (22.5) a | 245 (32.5) b | 421 (29.1) ab | 31 (26.1) ab | 38 (42.7) b | 56 (36.6) b | <0.001 |
| Modes of WIC nutrition education preferred in future 5 | ||||||||
| One-on-one in person | 2535 (86.4) | 309 (82.6) a | 635 (84.3) a | 1287 (89.1) b | 96 (80.7) ab | 76 (85.4) ab | 132 (86.3) ab | 0.002 |
| Video/DVD | 2227 (75.9) | 239 (63.9) a | 538 (71.5) a | 1208 (83.6) b | 76 (63.9) a | 67 (75.3) ab | 99 (64.7) a | <0.001 |
| Online | 2021 (68.9) | 277 (74.1) a | 610 (81.0) a | 866 (59.9) b | 83 (69.8) ab | 73 (82.0) a | 112 (73.2) a | <0.001 |
| WIC mobile app | 2017 (68.8) | 273 (73.0) a | 588 (78.1) a | 891 (61.7) b | 90 (75.6) a | 63 (70.8) ab | 112 (73.2) ab | <0.001 |
| Group session in person | 1826 (62.3) | 177 (47.3) ac | 412 (54.7) a | 1062 (73.5) b | 47 (39.5) c | 53 (59.6) abc | 75 (49.0) ac | <0.001 |
| Two-way texting | 1624 (55.4) | 197 (52.7) | 409 (54.3) | 828 (57.3) | 55 (46.2) | 51 (57.3) | 84 (54.9) | 0.17 |
| Very satisfied with WIC nutrition education 6 | 2528 (86.3) | 295 (79.1) a | 646 (85.8) ab | 1300 (90.1) b | 94 (79.0) a | 74 (83.2) ab | 119 (77.8) a | <0.001 |
| Very satisfied with WIC customer service 6 | 2555 (87.2) | 321 (85.8) | 637 (84.6) | 1285 (89.1) | 99 (83.9) | 82 (92.1) | 131 (85.6) | 0.07 |
| Changed behavior because of WIC nutrition education | 2537 (86.8) | 294 (79.0) c | 652 (86.7) ab | 1308 (90.8) a | 87 (73.7) c | 73 (83.0) abc | 123 (80.9) bc | <0.001 |
| Total (n = 2933) | Race/Ethnicity 2 | |||||||
|---|---|---|---|---|---|---|---|---|
| Non-Hispanic White (n = 374) | Hispanic English-Speaking (n = 753) | Hispanic Spanish-Speaking (n = 1445) | Non-Hispanic Black (n = 119) | Asian (n = 89) | Other 3 (n = 153) | p Value 4 | ||
| (n, %) | ||||||||
| Reasons for participating in WIC | ||||||||
| Fruits and vegetables | 2541 (92.5) | 306 (89.2) a | 616 (88.8) a | 1335 (97.0) b | 92 (82.1) a | 68 (85.0) a | 124 (86.7) a | <0.001 |
| Information from WIC staff | 2383 (87.0) | 246 (71.9) a | 554 (80.5) b | 1323 (96.0) c | 78 (69.6) ab | 69 (86.3) ab | 113 (80.1) ab | <0.001 |
| Support from WIC staff | 2357 (86.0) | 259 (76.0) a | 538 (77.9) a | 1316 (95.6) b | 68 (60.7) c | 65 (81.3) a | 111 (79.3) a | <0.001 |
| Classes and group sessions | 1790 (65.7) | 161 (47.2) a | 378 (54.5) ac | 1089 (79.6) b | 52 (46.4) ac | 49 (61.3) ac | 61 (43.0) ac | <0.001 |
| Relative importance of WIC nutrition education versus WIC foods | ||||||||
| Equally important | 2624 (89.4) | 289 (77.5) a | 672 (89.4) b | 1354 (93.7) c | 102 (85.7) abc | 77 (87.5) bc | 130 (85.0) ab | <0.001 |
| Food is more important | 232 (7.9) | 76 (20.4) | 45 (6.0) | 72 (5.0) | 14 (11.8) | 6 (6.8) | 19 (12.4) | |
| Education is more important | 74 (2.6) | 8 (2.1) | 35 (4.7) | 19 (1.3) | 3 (2.5) | 5 (5.7) | 4 (2.6) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaney, A.M.; Ritchie, L.D.; Whaley, S.E.; Tsai, M.M.; Randel-Schreiber, H.R.; Yepez, C.E.; Sabatier, S.; Young, A.; Meza, M.; Au, L.E. Racial and Ethnic Comparisons in Satisfaction with Services Provided by the Special Supplemental Nutrition Program for Women, Infants, and Children in California. Nutrients 2023, 15, 447. https://doi.org/10.3390/nu15020447
Chaney AM, Ritchie LD, Whaley SE, Tsai MM, Randel-Schreiber HR, Yepez CE, Sabatier S, Young A, Meza M, Au LE. Racial and Ethnic Comparisons in Satisfaction with Services Provided by the Special Supplemental Nutrition Program for Women, Infants, and Children in California. Nutrients. 2023; 15(2):447. https://doi.org/10.3390/nu15020447
Chicago/Turabian StyleChaney, Alana M., Lorrene D. Ritchie, Shannon E. Whaley, Marisa M. Tsai, Hallie R. Randel-Schreiber, Catherine E. Yepez, Susan Sabatier, Adrian Young, Martha Meza, and Lauren E. Au. 2023. "Racial and Ethnic Comparisons in Satisfaction with Services Provided by the Special Supplemental Nutrition Program for Women, Infants, and Children in California" Nutrients 15, no. 2: 447. https://doi.org/10.3390/nu15020447