

Trends in Oxidative Balance Score and Prevalence of Metabolic Dysfunction-Associated Steatotic Liver Disease in the United States: National Health and Nutrition Examination Survey 2001 to 2018

 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Definition of MASLD
2.3. Evaluation of Oxidative Balance Score (OBS)
2.4. Evaluation of the Body’s Inflammatory State
2.5. Evaluation of the Body’s Insulin Resistance (IR) Level
2.6. Covariates
2.7. Statistical Analysis
3. Results
3.1. Prevalence of MASLD in the U.S. Population from 2001 to 2018
3.2. Baseline Characteristics of the Study Population
3.3. Relationship between OBS and US-FLI and MASLD
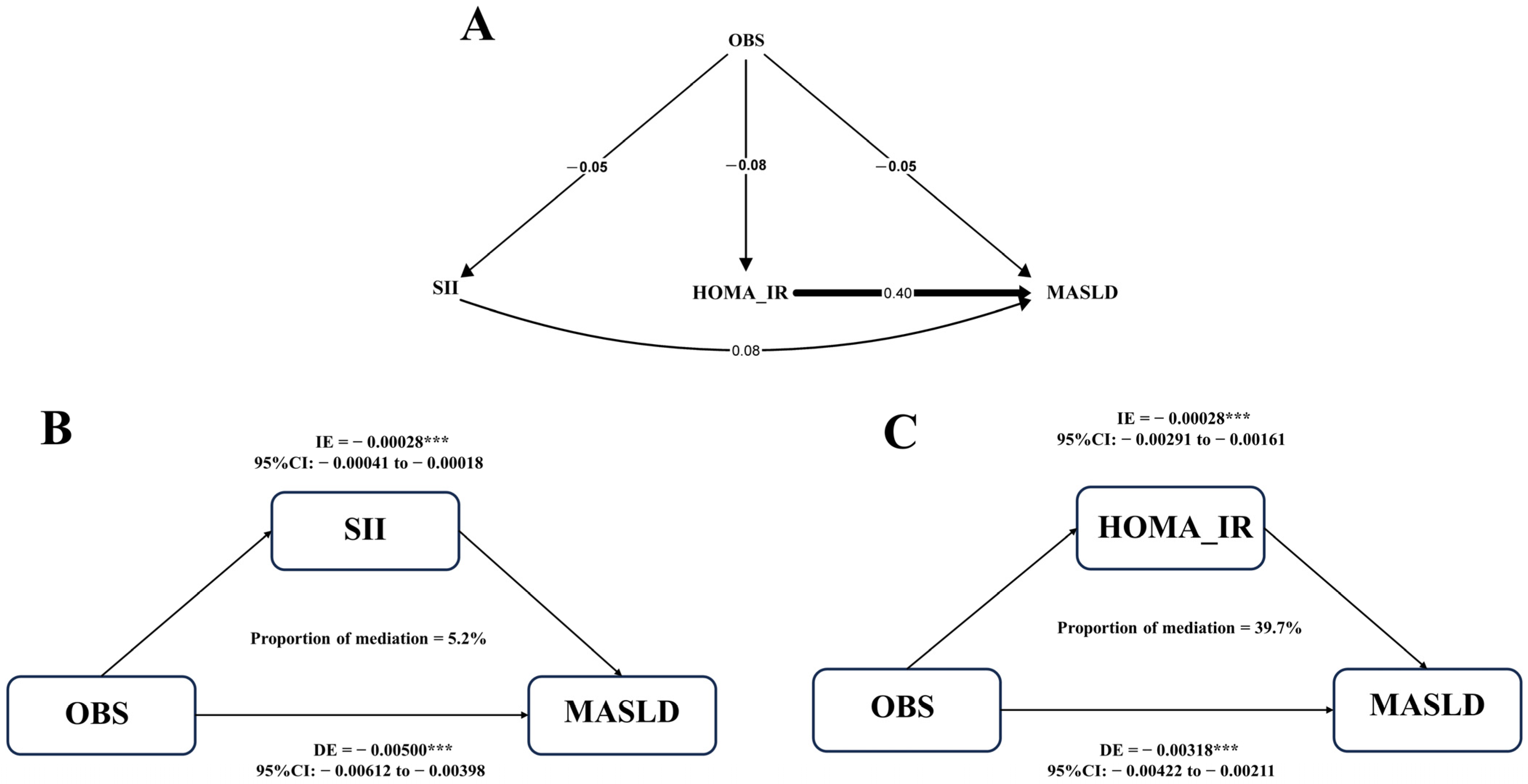
3.4. The Mediation Analysis between OBS and MASLD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Loomba, R.; Friedman, S.L.; Shulman, G.I. Mechanisms and disease consequences of nonalcoholic fatty liver disease. Cell 2021, 184, 2537–2564. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Mark, H.E.; Allen, A.M.; Arab, J.P.; Carrieri, P.; Noureddin, M.; Alazawi, W.; Alkhouri, N.; Alqahtani, S.A.; Arrese, M.; et al. A global research priority agenda to advance public health responses to fatty liver disease. J. Hepatol. 2023, 79, 618–634. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology 2012, 142, 1592–1609. [Google Scholar] [CrossRef] [PubMed]
- Tian, H.; Zhang, K.; Hui, Z.; Ren, F.; Ma, Y.; Han, F.; Sun, X.; Kan, C.; Hou, N. Global burden of non-alcoholic fatty liver disease in 204 countries and territories from 1990 to 2019. Clin. Res. Hepatol. Gastroenterol. 2023, 47, 102068. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.; Ekstedt, M.; Wong, G.L.; Hagstrom, H. Changing epidemiology, global trends and implications for outcomes of NAFLD. J. Hepatol. 2023, 79, 842–852. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.L.; Neuschwander-Tetri, B.A.; Rinella, M.; Sanyal, A.J. Mechanisms of NAFLD development and therapeutic strategies. Nat. Med. 2018, 24, 908–922. [Google Scholar] [CrossRef] [PubMed]
- Kosmalski, M.; Frankowski, R.; Deska, K.; Rozycka-Kosmalska, M.; Pietras, T. Exploring the Impact of Nutrition on Non-Alcoholic Fatty Liver Disease Management: Unveiling the Roles of Various Foods, Food Components, and Compounds. Nutrients 2023, 15, 2838. [Google Scholar] [CrossRef]
- Oya, J.; Nakagami, T.; Sasaki, S.; Jimba, S.; Murakami, K.; Kasahara, T.; Wasada, T.; Sekiguchi, H.; Hasegawa, M.; Endo, Y.; et al. Intake of n-3 polyunsaturated fatty acids and non-alcoholic fatty liver disease: A cross-sectional study in Japanese men and women. Eur. J. Clin. Nutr. 2010, 64, 1179–1185. [Google Scholar] [CrossRef]
- Wang, X.; Seo, Y.A.; Park, S.K. Serum selenium and non-alcoholic fatty liver disease (NAFLD) in U.S. adults: National Health and Nutrition Examination Survey (NHANES) 2011–2016. Environ. Res. 2021, 197, 111190. [Google Scholar] [CrossRef]
- van Kleef, L.A.; Hofman, A.; Voortman, T.; de Knegt, R.J. Objectively Measured Physical Activity Is Inversely Associated With Nonalcoholic Fatty Liver Disease: The Rotterdam Study. Am. J. Gastroenterol. 2022, 117, 311–318. [Google Scholar] [CrossRef]
- Goodman, M.; Bostick, R.M.; Dash, C.; Flanders, W.D.; Mandel, J.S. Hypothesis: Oxidative stress score as a combined measure of pro-oxidant and antioxidant exposures. Ann. Epidemiol. 2007, 17, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Son, D.H.; Lee, H.S.; Seol, S.Y.; Lee, Y.J.; Lee, J.H. Association between the Oxidative Balance Score and Incident Chronic Kidney Disease in Adults. Antioxidants 2023, 12, 335. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Liu, X.; Wang, Y.; Zeng, B.; Zhu, B.; Dai, F. Association between depression and oxidative balance score: National Health and Nutrition Examination Survey (NHANES) 2005–2018. J. Affect. Disord. 2023, 337, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Sohouli, M.H.; Rohani, P.; Hosseinzadeh, M.; Hekmatdoost, A. Adherence to oxidative balance scores and lower odds of non-alcoholic fatty liver disease: A case-control study. Sci. Rep. 2023, 13, 6140. [Google Scholar] [CrossRef] [PubMed]
- Cho, A.R.; Kwon, Y.J.; Lee, J.H. Oxidative balance score is inversely associated with the incidence of non-alcoholic fatty liver disease. Clin. Nutr. 2023, 42, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- Ruhl, C.E.; Everhart, J.E. Fatty liver indices in the multiethnic United States National Health and Nutrition Examination Survey. Aliment. Pharmacol. Ther. 2015, 41, 65–76. [Google Scholar] [CrossRef]
- Ma, N.; Yip, R.; Lewis, S.; Dinani, A.; Wyatt, C.; Crane, M.; Jirapatnakul, A.; Li, L.; Aloman, C.; Bansal, M.B.; et al. Environmental exposures are important risk factors for advanced liver fibrosis in African American adults. JHEP Rep. 2023, 5, 100696. [Google Scholar] [CrossRef]
- Song, Y.; Guo, W.; Li, Z.; Guo, D.; Li, Z.; Li, Y. Systemic immune-inflammation index is associated with hepatic steatosis: Evidence from NHANES 2015–2018. Front. Immunol. 2022, 13, 1058779. [Google Scholar] [CrossRef]
- Hu, B.; Yang, X.R.; Xu, Y.; Sun, Y.F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.M.; Qiu, S.J.; Zhou, J.; et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin. Cancer Res. 2014, 20, 6212–6222. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Hadefi, A.; Arvanitakis, M.; Trepo, E.; Zelber-Sagi, S. Dietary strategies in non-alcoholic fatty liver disease patients: From evidence to daily clinical practice, a systematic review. United Eur. Gastroenterol. J. 2023, 11, 663–689. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvado, J.; Diaz-Lopez, A.; Ruiz-Canela, M.; Basora, J.; Fito, M.; Corella, D.; Serra-Majem, L.; Warnberg, J.; Romaguera, D.; Estruch, R.; et al. Effect of a Lifestyle Intervention Program with Energy-Restricted Mediterranean Diet and Exercise on Weight Loss and Cardiovascular Risk Factors: One-Year Results of the PREDIMED-Plus Trial. Diabetes Care 2019, 42, 777–788. [Google Scholar] [CrossRef]
- Zelber-Sagi, S.; Nitzan-Kaluski, D.; Goldsmith, R.; Webb, M.; Zvibel, I.; Goldiner, I.; Blendis, L.; Halpern, Z.; Oren, R. Role of leisure-time physical activity in nonalcoholic fatty liver disease: A population-based study. Hepatology 2008, 48, 1791–1798. [Google Scholar] [CrossRef]
- Barrea, L.; Verde, L.; Savastano, S.; Colao, A.; Muscogiuri, G. Adherence to Mediterranean Diet: Any Association with NAFLD? Antioxidants 2023, 12, 1318. [Google Scholar] [CrossRef]
- Tian, T.; Zhang, J.; Xie, W.; Ni, Y.; Fang, X.; Liu, M.; Peng, X.; Wang, J.; Dai, Y.; Zhou, Y. Dietary Quality and Relationships with Metabolic Dysfunction-Associated Fatty Liver Disease (MAFLD) among United States Adults, Results from NHANES 2017-2018. Nutrients 2022, 14, 4505. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, R.; De Nucci, S.; Castellana, F.; Di Chito, M.; Giannuzzi, V.; Shahini, E.; Zupo, R.; Lampignano, L.; Piazzolla, G.; Triggiani, V.; et al. The Effects of Eight Weeks’ Very Low-Calorie Ketogenic Diet (VLCKD) on Liver Health in Subjects Affected by Overweight and Obesity. Nutrients 2023, 15, 825. [Google Scholar] [CrossRef]
- Salas-Salvado, J.; Bullo, M.; Babio, N.; Martinez-Gonzalez, M.A.; Ibarrola-Jurado, N.; Basora, J.; Estruch, R.; Covas, M.I.; Corella, D.; Aros, F.; et al. Reduction in the incidence of type 2 diabetes with the Mediterranean diet: Results of the PREDIMED-Reus nutrition intervention randomized trial. Diabetes Care 2011, 34, 14–19. [Google Scholar] [CrossRef]
- Yaskolka Meir, A.; Rinott, E.; Tsaban, G.; Zelicha, H.; Kaplan, A.; Rosen, P.; Shelef, I.; Youngster, I.; Shalev, A.; Bluher, M.; et al. Effect of green-Mediterranean diet on intrahepatic fat: The DIRECT PLUS randomised controlled trial. Gut 2021, 70, 2085–2095. [Google Scholar] [CrossRef]
- Finkel, T.; Holbrook, N.J. Oxidants, oxidative stress and the biology of ageing. Nature 2000, 408, 239–247. [Google Scholar] [CrossRef]
- Lin, M.T.; Beal, M.F. Mitochondrial dysfunction and oxidative stress in neurodegenerative diseases. Nature 2006, 443, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Reuter, S.; Gupta, S.C.; Chaturvedi, M.M.; Aggarwal, B.B. Oxidative stress, inflammation, and cancer: How are they linked? Free Radic. Biol. Med. 2010, 49, 1603–1616. [Google Scholar] [CrossRef]
- Houstis, N.; Rosen, E.D.; Lander, E.S. Reactive oxygen species have a causal role in multiple forms of insulin resistance. Nature 2006, 440, 944–948. [Google Scholar] [CrossRef] [PubMed]
- Hurrle, S.; Hsu, W.H. The etiology of oxidative stress in insulin resistance. Biomed. J. 2017, 40, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Berna, G.; Romero-Gomez, M. The role of nutrition in non-alcoholic fatty liver disease: Pathophysiology and management. Liver Int. 2020, 40 (Suppl. 1), 102–108. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, P.; Janmeda, P.; Docea, A.O.; Yeskaliyeva, B.; Abdull Razis, A.F.; Modu, B.; Calina, D.; Sharifi-Rad, J. Oxidative stress, free radicals and antioxidants: Potential crosstalk in the pathophysiology of human diseases. Front. Chem. 2023, 11, 1158198. [Google Scholar] [CrossRef] [PubMed]
- Chaki, B.; Pal, S.; Chattopadhyay, S.; Bandyopadhyay, A. High-intensity exercise-induced oxidative stress in sedentary pre-pubertal & post-pubertal boys: A comparative study. Indian. J. Med. Res. 2019, 150, 167–174. [Google Scholar] [CrossRef]
- Cuthbertson, D.J.; Shojaee-Moradie, F.; Sprung, V.S.; Jones, H.; Pugh, C.J.; Richardson, P.; Kemp, G.J.; Barrett, M.; Jackson, N.C.; Thomas, E.L.; et al. Dissociation between exercise-induced reduction in liver fat and changes in hepatic and peripheral glucose homoeostasis in obese patients with non-alcoholic fatty liver disease. Clin. Sci. 2016, 130, 93–104. [Google Scholar] [CrossRef]
- Lavoie, J.M.; Gauthier, M.S. Regulation of fat metabolism in the liver: Link to non-alcoholic hepatic steatosis and impact of physical exercise. Cell Mol. Life Sci. 2006, 63, 1393–1409. [Google Scholar] [CrossRef]
- Zhang, W.; Peng, S.F.; Chen, L.; Chen, H.M.; Cheng, X.E.; Tang, Y.H. Association between the Oxidative Balance Score and Telomere Length from the National Health and Nutrition Examination Survey 1999–2002. Oxidative Med. Cell. Longev. 2022, 2022, 1345071. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characters | 2001–2002 (n = 1854) | 2003–2004 (n = 1737) | 2005–2006 (n = 1647) | 2007–2008 (n = 1520) | 2009–2010 (n = 1701) | 2011–2012 (n = 1496) | 2013–2014 (n = 1564) | 2015–2016 (n = 1398) | 2017–2018 (n = 1135) | p-Trend |
|---|---|---|---|---|---|---|---|---|---|---|
| Total | 26.21 (23.14, 29.29) | 23.75 (19.84, 27.66) | 26.88 (23.30, 30.47) | 27.33 (23.94, 30.72) | 25.93 (23.22, 28.64) | 26.24 (22.35, 30.13) | 24.70 (22.23, 27.17) | 29.53 (26.57, 32.49) | 36.04 (32.13, 39.96) | <0.001 |
| Sex | ||||||||||
| Male | 31.86 (26.20, 37.52) | 31.17 (27.85, 34.50) | 33.48 (29.39, 37.57) | 33.76 (29.70, 37.82) | 32.79 (28.97, 36.61) | 28.52 (23.74, 33.30) | 26.19 (22.10, 30.29) | 35.55 (29.95, 41.15) | 40.48 (33.77, 47.20) | 0.211 |
| Female | 20.39 (16.05, 24.72) | 16.18 (10.82, 21.54) | 19.92 (15.37, 24.47) | 20.90 (16.37, 25.43) | 19.17 (15.45, 22.89) | 24.15 (18.33, 29.98) | 23.29 (20.30, 26.27) | 23.78 (20.28, 27.27) | 31.79 (25.62, 37.95) | <0.001 |
| Race | ||||||||||
| Mexican | 34.28 (28.15, 40.41) | 28.31 (19.94, 36.68) | 34.37 (29.45, 39.28) | 43.42 (38.03, 48.81) | 39.38 (33.22, 45.53) | 41.00 (33.12, 48.87) | 34.90 (27.39, 42.41) | 42.30 (33.44, 51.17) | 50.56 (41.80, 59.32) | 0.001 |
| White | 27.26 (23.84, 30.67) | 25.03 (20.31, 29.75) | 28.85 (24.41, 33.30) | 27.89 (24.06, 31.73) | 26.33 (22.95, 29.72) | 26.18 (20.70, 31.66) | 25.66 (22.17, 29.15) | 29.89 (26.05, 33.74) | 38.03 (33.03, 43.03) | 0.006 |
| Black | 16.71 (13.00, 20.42) | 13.48 (9.82, 17.14) | 13.77 (10.44, 17.11) | 13.19 (9.15, 17.23) | 16.49 (10.67, 22.31) | 17.81 (12.61, 23.00) | 16.45 (11.40, 21.51) | 18.43 (14.33, 22.53) | 20.61 (15.98, 25.24) | 0.013 |
| Other | 21.66 (14.27, 29.06) | 21.20 (11.49, 30.90) | 21.44 (11.46, 31.42) | 27.49 (22.86, 32.11) | 21.57 (16.09, 27.05) | 24.43 (19.10, 29.76) | 19.63 (15.72, 23.54) | 30.22 (25.69, 34.76) | 31.01 (23.65, 38.37) | 0.042 |
| BMI | ||||||||||
| <25 | 3.67 (2.02, 5.31) | 2.73 (1.06, 4.39) | 2.11 (0.91, 3.31) | 2.64 (0.95,4.33) | 2.73 (1.38, 4.07) | 1.86 (0.42, 3.31) | 1.89 (0.31, 3.46) | 3.07 (1.15, 4.98) | 5.56 (2.55, 8.56) | 0.590 |
| ≥25 | 42.65 (38.94, 46.37) | 36.15 (31.88, 40.42) | 41.90 (36.37, 47.43) | 42.48 (37.27, 47.68) | 43.27 (39.41, 47.13) | 40.71 (35.23, 46.20) | 38.62 (34.79, 42.44) | 42.06 (38.88, 45.24) | 48.80 (43.52, 54.09) | 0.041 |
| Diabetes mellitus | ||||||||||
| No | 22.08 (19.12, 25.04) | 19.99 (16.11, 23.86) | 22.09 (18.34, 25.85) | 22.17 (18.21, 26.13) | 21.57 (18.84, 24.30) | 21. 29 (17.21, 25.37) | 19.65 (17.07, 22.23) | 22.80 (19.11, 26.48) | 28.23 (23.78, 32.67) | 0.081 |
| Yes | 73.74 (64.68, 82.80) | 61.79 (54.69, 68.90) | 66.71 (60.20, 73.22) | 66.56 (57.92, 75.20) | 61.33 (53.87, 68.78) | 67. 85 (59.83,75.88) | 64.20 (58.10, 70.30) | 65.79 (58.18, 73.40) | 78.76 (72.30, 85.21) | 0.151 |
| Hypertension | ||||||||||
| No | 17.27 (13.98, 20.56) | 15.36 (13.14, 17.57) | 17.66 (14.34, 20.99) | 18.86 (15.62, 22.11) | 17.22 (15.08, 19.36) | 17.07 (13.09, 21.05) | 17.31 (14.61, 20.01) | 20.28 (16.15, 24.42) | 24.88 (18.86, 30.89) | 0.010 |
| Yes | 49.13 (39.56, 58.70) | 40.99 (33.84, 48.15) | 47.68 (42.21, 53.15) | 46.29 (40.26, 52.32) | 48.33 (42.58, 54.08) | 48.65 (40.94, 56.36) | 40.16 (36.48, 43.85) | 46.55 (42.15, 50.95) | 55.31 (48.10, 62.53) | 0.261 |
| Hyperlipidemia | ||||||||||
| No | 6.74 (4.07, 9.42) | 10.27 (6.92, 13.62) | 11.11 (6.95, 15.27) | 7.83 (5.04, 10.62) | 11.43 (8.19, 14.67) | 6.58 (4.46, 8.70) | 8.72 (5.95, 11.49) | 12.26 (7.57, 16.94) | 14.88 (8.91, 20.84) | 0.056 |
| Yes | 34.98 (31.62, 38.35) | 29.96 (25.53, 34.38) | 34.76 (30.48, 39.04) | 36.22 (32.21, 40.24) | 33.92 (30.99, 36.85) | 35.97 (30.84, 41.10) | 33.75 (31.18, 36.32) | 38.31 (33.87, 42.75) | 46.48 (42.25, 50.71) | <0.001 |
| Variable | Total (n = 14,052) | Non-MASLD (n = 10,391) | MASLD (n = 3661) | p Value |
|---|---|---|---|---|
| Age, Mean ± SD | 43.59 ± 0.29 | 41.00 ± 0.32 | 50.48 ± 0.34 | <0.001 |
| US-FLI, Mean ± SD | 22.14 ± 0.27 | 11.18 ± 0.11 | 51.25 ± 0.37 | <0.001 |
| BMI, Mean ± SD | 27.84 ± 0.09 | 25.54 ± 0.07 | 33.93 ± 0.14 | <0.001 |
| Energy kcal, Mean ± SD | 2182.88 ± 11.88 | 2150.55 ± 12.79 | 2268.73 ± 23.37 | <0.001 |
| ALT, Mean ± SD | 23.85 ± 0.26 | 20.78 ± 0.13 | 32.01 ± 0.88 | <0.001 |
| AST, Mean ± SD | 24.22 ± 0.13 | 23.29 ± 0.15 | 26.68 ± 0.29 | <0.001 |
| OBS, Mean ± SD | 21.37 ± 0.13 | 21.76 ± 0.14 | 20.32 ± 0.19 | <0.001 |
| SII, Mean ± SD | 519.78 ± 3.76 | 503.37 ± 4.37 | 563.34 ± 6.52 | <0.001 |
| HOMA_IR, Mean ± SD | 3.32 ± 0.05 | 1.97 ± 0.02 | 6.91 ± 0.16 | <0.001 |
| BMI (%) | <0.001 | |||
| <25 | 5706 (40.61) | 5536 (49.76) | 170 (3.87) | |
| ≥25 | 8346 (59.39) | 4855 (50.24) | 3491 (96.13) | |
| Sex (%) | <0.001 | |||
| Female | 6881 (48.97) | 5324 (53.99) | 1557 (40.84) | |
| Male | 7171 (51.03) | 5067 (46.01) | 2104 (59.16) | |
| Race (%) | <0.001 | |||
| Black | 3117 (22.18) | 2656 (11.74) | 461 (6.08) | |
| Mexican | 2490 (17.72) | 1564 (5.95) | 926 (10.04) | |
| Other | 2361 (16.8) | 1788 (11.72) | 573 (10.22) | |
| White | 6084 (43.3) | 4383 (70.59) | 1701 (73.66) | |
| Educational level (%) | <0.001 | |||
| Below high school | 2536 (18.05) | 1986 (10.45) | 550 (7.02) | |
| High school | 5305 (37.75) | 3892 (32.56) | 1413 (35.47) | |
| More than high schools | 6211 (44.2) | 4513 (56.99) | 1698 (57.51) | |
| Hypertension (%) | <0.001 | |||
| No | 9794 (69.7) | 8037 (77.03) | 1757 (45.88) | |
| Yes | 4258 (30.3) | 2354 (22.97) | 1904 (54.12) | |
| Diabetes mellitus (%) | <0.001 | |||
| No | 12,218 (86.95) | 9723 (94.88) | 2495 (71.61) | |
| Yes | 1834 (13.05) | 668 (5.12) | 1166 (28.39) | |
| Hyperlipidemia (%) | <0.001 | |||
| No | 5310 (37.79) | 4792 (41.12) | 518 (12.13) | |
| Yes | 8742 (62.21) | 5599 (58.88) | 3143 (87.87) |
| Outcome | Variable | Model 1 | p | Model 2 | p | Model 3 | p |
|---|---|---|---|---|---|---|---|
| β (95% CI) | β (95% CI) | β (95% CI) | |||||
| Relationship between OBS and US-FLI | OBS | −0.43 (−0.49, −0.36) | <0.001 | −0.65 (−0.73, −0.57) | <0.001 | −0.17 (−0.22, −0.12) | <0.001 |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |||||
| OBS | 0.96 (0.95, 0.97) | <0.001 | 0.94 (0.93, 0.95) | <0.001 | 0.98 (0.96, 0.99) | <0.001 | |
| Relationship between OBS and MASLD | Q1 | ref | ref | ref | ref | ref | ref |
| Q2 | 0.85 (0.74, 0.98) | 0.027 | 0.72 (0.62, 0.85) | <0.001 | 0.88 (0.74, 1.06) | 0.188 | |
| Q3 | 0.60 (0.52, 0.70) | <0.001 | 0.46 (0.38, 0.55) | <0.001 | 0.72 (0.57, 0.92) | 0.009 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, Z.; Wu, Y.; Meng, Y.; Liu, C.; Deng, B.; Zhen, J.; Dong, W. Trends in Oxidative Balance Score and Prevalence of Metabolic Dysfunction-Associated Steatotic Liver Disease in the United States: National Health and Nutrition Examination Survey 2001 to 2018. Nutrients 2023, 15, 4931. https://doi.org/10.3390/nu15234931
Tan Z, Wu Y, Meng Y, Liu C, Deng B, Zhen J, Dong W. Trends in Oxidative Balance Score and Prevalence of Metabolic Dysfunction-Associated Steatotic Liver Disease in the United States: National Health and Nutrition Examination Survey 2001 to 2018. Nutrients. 2023; 15(23):4931. https://doi.org/10.3390/nu15234931
Chicago/Turabian StyleTan, Zongbiao, Yanrui Wu, Yang Meng, Chuan Liu, Beiying Deng, Junhai Zhen, and Weiguo Dong. 2023. "Trends in Oxidative Balance Score and Prevalence of Metabolic Dysfunction-Associated Steatotic Liver Disease in the United States: National Health and Nutrition Examination Survey 2001 to 2018" Nutrients 15, no. 23: 4931. https://doi.org/10.3390/nu15234931
APA StyleTan, Z., Wu, Y., Meng, Y., Liu, C., Deng, B., Zhen, J., & Dong, W. (2023). Trends in Oxidative Balance Score and Prevalence of Metabolic Dysfunction-Associated Steatotic Liver Disease in the United States: National Health and Nutrition Examination Survey 2001 to 2018. Nutrients, 15(23), 4931. https://doi.org/10.3390/nu15234931