
Abnormal Maternal Body Mass Index and Customized Fetal Weight Charts: Improving the Identification of Small for Gestational Age Fetuses and Newborns
 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Method
2.1. Outcomes
2.2. Subgroups and Comparisons
- -
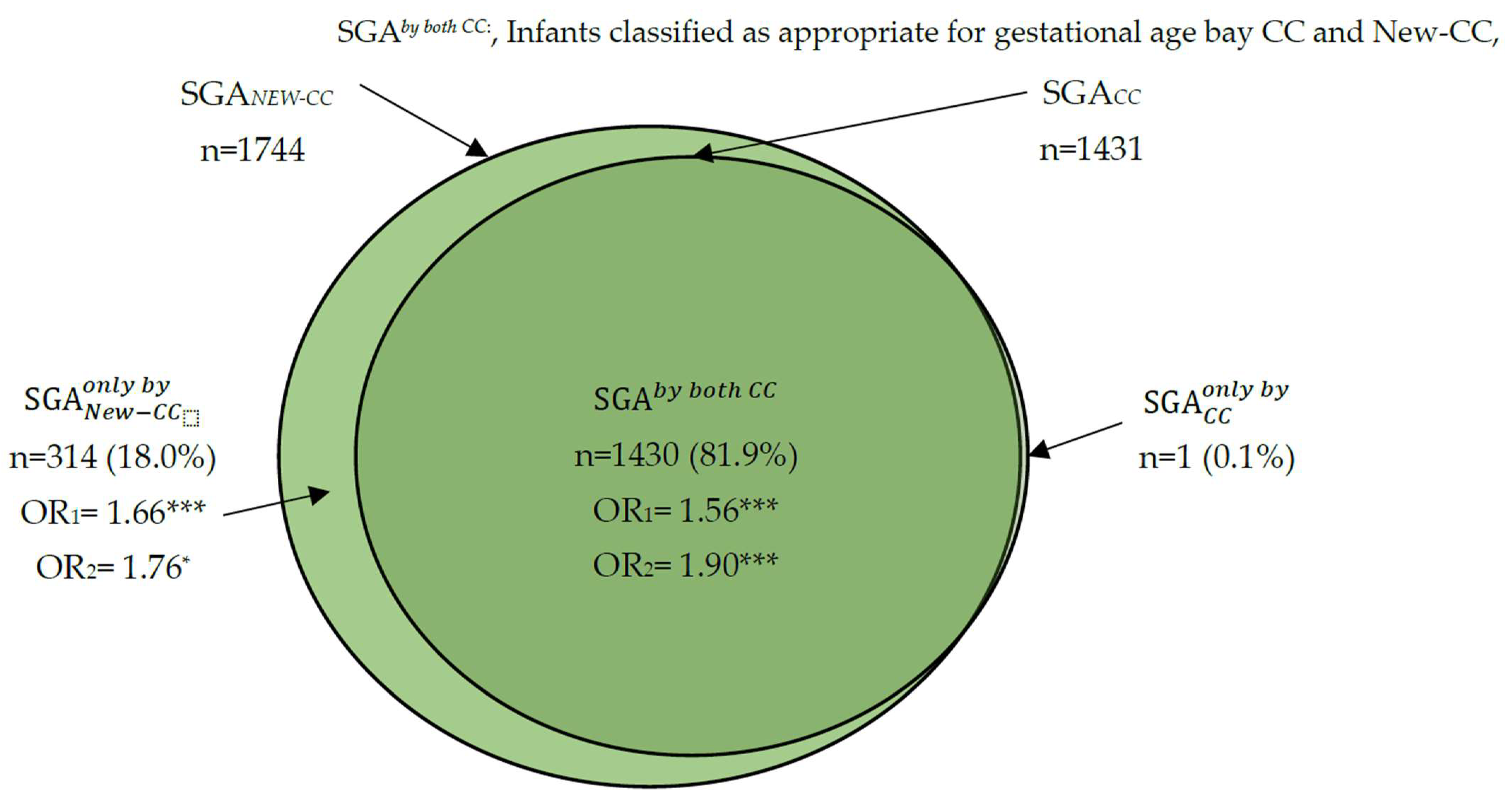
- SGA according to the standard CCs, SGA according to the new CCs, SGA according to both the CCs and new CCs, SGA according only to the standard CCs, and SGA according only to the new CCs.
- -
- AGA according only to the new CCs, and AGA according to both the standard CCs and the new CCs.
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gardosi, J. Customized fetal growth standards: Rationale and clinical application. Semin. Perinatol. 2004, 28, 33–40. [Google Scholar] [CrossRef]
- Gardosi, J.; Madurasinghe, V.; Williams, M.; Malik, A.; Francis, A. Maternal and fetal risk factors for stillbirth: Population based study. Br. J. Obstet. Gynecol. 2013, 346, f108. [Google Scholar] [CrossRef]
- Han, Z.; Mulla, S.; Beyene, J.; Liao, G.; McDonald, S.D. Maternal underweight and the risk of preterm birth and low birth weight: A systematic review and meta-analyses. Int. J. Epidemiol. 2011, 40, 65–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varvarigou, A.A. Intrauterine growth restriction as a potential risk factor for disease onset in adulthood. J. Pediatr. Endocrinol. Metab. 2010, 23, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Castro Conde, J.R.; González Campo, C.; González González, N.L.; Reyes Millan, B.; González Barrios, D.; Quintero Fuetes, I. Assessment of neonatal EEG background and neurodevelopment in full-term small for their gestational age infants. Pediatr. Res. 2020, 88, 91–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González González, N.L.; González Dávila, E.; García Hernández, J.A.; Cabrera Morales, F.; Padrón, E.; Domenech, E. Construction of model for calculating and recording neonatal weight percentiles. Anales de Pediatria 2014, 80, 81–88. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetrics and Gynecology. Fetal Growth Restriction: ACOG Practice Bulletin Summary. Number Obstet. Gynecol. 2021, 137, 385–387. [Google Scholar] [CrossRef]
- Obiyo, O.O.; Danielle, J.R. Small for Gestational Age; StatPearls Publishing: Tampa, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK563247/ (accessed on 4 October 2022).
- Gardosi, J.; Chang, A.; Kalyan, B.; Sahota, D.; Symonds, E.M. Customized antenatal growth charts. Lancet 1992, 339, 283–287. [Google Scholar] [CrossRef]
- Gardosi, J.; Francis, A. Customised Weight Centile Calculator–GROW-Centile v.5.12/6.2 2009. Gestation Network. Available online: www.gestation.net (accessed on 11 November 2022).
- Clausson, B.; Gardosi, J.; Francis, A.; Cnattingius, S. Perinatal outcome in SGA births defined by customized versus populationbased birthweight standards. Br. J. Obstet. Gynecol. 2001, 108, 830–834. [Google Scholar]
- Jong, C.L.; Gardosi, J.; Dekker, G.A.; Colenbrander, G.J.; Geijn, H.P. Application of a customized birthweight standard in the assessment of perinatal outcome in a high risk population. Br. J. Obstet. Gynecol. 1998, 105, 531–535. [Google Scholar] [CrossRef]
- McCowan, L.M.; Harding, J.E.; Stewart, A.W. Customized birthweight centiles predict SGA pregnancies with perinatal morbidity. Br. J. Obstet. Gynecol. 2005, 112, 1026–1033. [Google Scholar] [CrossRef] [PubMed]
- Figueras, F.; Figueras, J.; Meler, E.; Eixarch, E.; Coll, O.; Gratacos, E.; Gardosi, J.; Carbonell, X. Customized birthweight standards accurately predict perinatal morbidity. Arch. Dis. Chilhood Fetal Neonatal Ed. 2007, 92, F277–F280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueras, F.; Eixarch, E.; Gratacos, E.; Gardosi, J. Predictiveness of antenatal umbilical artery Doppler for adverse pregnancy outcome in small-for-gestational-age babies according to customized birthweight centiles: Population-based study. Br. J. Obstet. Gynecol. 2008, 115, 590–594. [Google Scholar] [CrossRef] [PubMed]
- Gardosi, J.; Francis, A. Adverse pregnancy outcome and association with small for gestational age birthweight by customized and population-based percentiles. Am. J. Obstet. Gynecol. 2009, 201, 28.e1–28.e8. [Google Scholar] [CrossRef]
- González González, N.L.; González Dávila, E.; Cabrera, F.; Vega, B.; Padron, E.; Bartha, J.L.; Armas-Gonzalez, M.; García-Hernández, J.A.; García-Hernández, J.A. Application of customized birth weight curves in the assessment of perinatal outcomes in infants of diabetic mothers. Fetal Diagn. Ther. 2015, 37, 117–122. [Google Scholar] [CrossRef]
- Kabiri, D.; Romero, R.; Gudicha, D.W.; Hernandez-Andrade, E.; Pacora, P.; Benshalom-Tirosh, N.; Tirosh, D.; Yeo, L.; Erez, O.; Hassan, S.S.; et al. Prediction of adverse perinatal outcome by fetal biometry: Comparison of customized and population-based standards. Ultrasound Obstet. Gynecol. 2020, 55, 177–188. [Google Scholar] [CrossRef]
- Gardosi, J.; Francis, A.; Turner, S.; Wlliams, M. Customized growth charts: Rationale, validation and clinical benefits. Am. J. Obstet. Gynecol. 2018, 218, S609–S618. [Google Scholar] [CrossRef] [Green Version]
- Tenenbaum-Gavish, K.; Hod, M. Impact of maternal obesity on fetal health. Fetal Diagn. Ther. 2013, 34, 1–7. [Google Scholar] [CrossRef]
- Catalano, P.M.; Shankar, K. Obesity and pregnancy: Mechanisms of short term and long term adverse consequences for mother and child. Br. J. Obstet. Gynecol. 2017, 356, j1. [Google Scholar] [CrossRef]
- Lisonkova, S.; Muraca, G.M.; Potts, J.; Liauw, J.; Chan, W.S.; Skoll, A.; Lim, K.I. Association Between Prepregnancy Body Mass Index and Severe Maternal Morbidity. J. Am. Med. Assoc. 2017, 318, 1777. [Google Scholar] [CrossRef]
- Santos, S.; Voerman, E.; Amiano, P.; Barros, H.; Beilin, L.J.; Bergström, A.; Charles, M.A.; Chatzi, L.; Chevrier, G.P.; Corpeleijn, E.; et al. Impact of maternal body mass index and gestational weight gain on pregnancy complications: An individual participant data meta-analysis of European, North American and Australian cohorts. Br. J. Obstet. Gyneoclogy 2019, 126, 984–995. [Google Scholar]
- Zehravi, M.; Maqbool, M.; Ara, I. Correlation between obesity, gestational diabetes mellitus and pregnancy outcomes: An overview. Int. J. Adolesc. Med. Health 2021, 33, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Marshall, N.E.; Abrams, B.; Barbour, L.A.; Catalano, P.; Christian, P.; Friedman, J.E.; Hay, W.W.; Hernandez, T.L.; Hernandez, N.F.; Oken, E.; et al. The importance of nutrition in pregnancy and lactation: Lifelong consequences. Am. J. Obstet. Gynecol. 2022, 226, 607–632. [Google Scholar] [CrossRef] [PubMed]
- González González, N.L.; González Dávila, E.; Cabrera, F.; Padrón, E.; Castro, J.R.; García Hernández, J.A. Customized weight curves for Spanish fetuses and newborns. J. Matern. Fetal Neonatal Med. 2014, 27, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- González, N.L.G.; Dávila, E.G.; Martín, A.G.; Padrón, E.; Hernández, J.Á.G. Maternal Thinness and Obesity and Customized Fetal Weight Charts. Fetal Diagn. Ther. 2021, 48, 551–559. [Google Scholar] [CrossRef]
- WHO. Physical Status: The Use and Interpretation of Anthropometry. Report of a WHO Expert Committee; WHO Technical Report Series 854; World Health Organization: Geneva, Switzerland, 1995. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Lees, C.C.; Stampalija, A.A.; Bschat, F.; da Silva Costa, E.; Ferrazzi, F.; Hecher, K.; Poon, L.C.; Salomon, L.; Unterscheider, J. ISUOG Practice Guidelines: Diagnosis and management of small-for-gestational-age fetus and fetal growth restriction. Ultrasound Obstet. Gynecol. 2020, 56, 298–312. [Google Scholar] [CrossRef]
- Chiossi, G.; Pedroza, C.; Constantine, M.M.; Truong, V.T.T.; Gargano, G.; Saade, G.R. Customized vs population-based growth charts to identify neonates at risk of adverse outcoms: Systematic review and Bayesian meta-analysis of observational studies. Ultrasound Obstet. Gynecol. 2017, 50, 156–166. [Google Scholar] [CrossRef] [Green Version]
- Royal College of Obstetricians and Gynaecologists. The Investigation and Management of the Small for Gestational Age Fetus; Green Top Guideline No 31; Royal College of Obstetricians and Gynecologists (RCOG): London, UK, 2013. [Google Scholar]
- Clifford, S.; Giddings, S.; Southam, M.; Williams, M.; Gardosi, J. The growth assessment protocol: A national program to improve patient safety in maternity care. Midwife Dig. 2013, 23, 516–523. [Google Scholar]
- Office of National Statistics. Statistical Bulletin: Births in England and Wales. 2016. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/livebirths/bulletins/birthsummarytablesenglandandwales/ (accessed on 14 November 2022).
- World Health Organization. Available online: https://www.who.int/health-topics/malnutrition#tab=tab_1) (accessed on 4 October 2022).
- Lewandowska, M. Maternal Obesity and Risk of Low Birth Weight, Fetal Growth Restriction, and Macrosomia: Multiple Analyses. Nutrients 2021, 13, 1213. [Google Scholar] [CrossRef]
- Chen, Y.H.; Li, L.; Chen, W.; Liu, Z.B.; Ma, L.; Gao, X.X.; He, J.L.; Wang, H.; Zhao, M.; Yang, Y.Y.; et al. Pre-pregnancy underweight and obesity are positively associated with small-for-gestational-age infants in a Chinese population. Sci. Reprod. 2019, 9, 15544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papageorghiou, A.T.; Ohuma, E.O.; Noble, J.A.; Pang, R.; Victora, C.G.; Barros, F.C. International standards for fetal growth based on serial ultrasound measurements: The Fetal Growth Longitudinal Study of the INTERGROWTH-21st Project. International Fetal and Newborn Growth Consortium for the 21st Century (INTERGROWTH 21st). International standards for fetal growth based on serial ultrasound measurements: The Fetal Growth Longitudinal Study of the INTERGROWTH-21st Projet. Lancet 2014, 384, 869–879. [Google Scholar] [PubMed] [Green Version]
- Kiserud, T.; Piaggio, G.; Carroli, G.; Widmer, M.; Carvalho, J.; Jensen, N.L.; Giordano, D.; Cecatti, J.G.; Aleem, H.A.; Talegawkar, S.A.; et al. The World Health Organization fetal growth charts: A multinational longitudinal study of ultrasound biometric measurements and estimated fetal weight. PLoS Med. 2017, 14, e1002220. [Google Scholar]
- Buck, L.G.M.; Grewal, J.; Albert, P.S.; Sciscione, A.; Wing, D.A.; Grobman, W.A.; Newman, R.B.; Wapner, R.; D’Alton, M.E.; Skupski, D.; et al. Racial/ethnic standards for fetal growth: The NICHD Fetal Growth Studies. Fetal growth velocity: The NICHD fetal growth studies. Am. J. Obstet. Gynecol. 2015, 213, 449.e1–449.e41. [Google Scholar]
- Ohuma, E.O.; Njim, T.; Sharps, M.C. Current Issues in the Development of Foetal Growth References and Standards. Curr. Epidemiol. Rep. 2018, 5, 388–398. [Google Scholar] [CrossRef] [PubMed]
- Grantz, K.L.; Heidiger, M.L.; Liu, D.; Buck, L.G.M. Fetal growth standards: The NICHD fetal growth study approach in context with INTERGROWTH-21st and the World Health Organization Multicentre Growth Reference Study. Am. J. Obstet. Gynecol. 2018, 218, S641–S655.e28. [Google Scholar] [CrossRef] [Green Version]
- Anderson, N.H.; Sadler, L.C.; McKinlay, C.J.D.; McCowan, L.M.E. INTERGROWTH-21st vs customized birthweight standards for identification of perinatal mortality and morbidity. Am. J. Obstet. Gynecol. 2016, 214, 509.e1–509.e7. [Google Scholar] [CrossRef] [Green Version]
- Francis, A.; Hugh, O.; Gardosi, J. Customized vs INTERGROWTH-21st standards for the assessment of birthweight and stillbirth risk at term. Am. J. Obstet. Gynecol. 2018, 218, S692–S699. [Google Scholar] [CrossRef] [PubMed]
- Tarca, A.L.; Romero, R.; Gudicha, D.W.; Erez, O.; Hernandez-Andrade, E.; Yeo, L.; Bhatti, G.; Pacora, P.; Maymon, E.; Hassan, S.H. A new customized fetal growth standard for African American women: The PRB/NICHD Detroit study. Am. J. Obstet. Gynecol. 2018, 218, S679–S691. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Model | Customized Curves | New Customized Curves (18.5–25) | |
|---|---|---|---|
| Constant | 3289.681 | 3304.579 | |
| Maternal height (MH, cm) (from 163) | 9.392 | 6.987 | |
| Maternal weight (MW, kg) (from 65) | |||
| Linear | 4.856 | 7.510 | |
| Squared | −0.098 | - | |
| Cubed | 0.001 | - | |
| Parity (Birth ≥ 1) | 113.889 | 113.530 | |
| Ethnic origin | |||
| East-Asia | 165.560 | 143.461 | |
| South America | 161.550 | 134.161 | |
| Rest of Europe | 67.927 | 68.934 | |
| North Africa | 109.265 | 62.447 | |
| GA (weeks) (from 40) | |||
| Linear | 135.413 | 134.457 | |
| Squared | −14.063 | −13.435 | |
| Cubed | −0.838 | −0.803 | |
| Sex | |||
| Male | 67.188 | 67.552 | |
| Female | −67.188 | −67.552 | |
| Interactions | |||
| GA (linear) with | Sex | 6.890 | 8.501 |
| Parity (Birth ≥ 1) | 9.032 | 11.300 | |
| MH (cubed) | 0.006 | 0.008 | |
| MW (squared) | 0.260 | - | |
| GA (squared) with | MH (linear) | −0.378 | - |
| MH (squared) | −0.008 | −0.011 | |
| GA (cubed) with | MH (linear) | −0.032 | - |
| Mean square error | 144,630.076 | 133,659.796 | |
| R2 | 0.454 | 0.451 | |
| Coefficient of variation (cv) | 0.1156 | 0.1106 | |
| Total (N = 14,740) | New Customized Curves (New CCs) | Conventional Customized Curves (CC) | ||||||
|---|---|---|---|---|---|---|---|---|
| SGA (S) (N = 1744) 11.8% | AGA(A) (N = 10,984) 74.5% | LGA (L) (N = 2012) 13.7% | p-Value (Homogeneous Subset) | SGA (N = 1431) 9.7% | AGA (N = 11,197) 76% | LGA (N = 2112) 14.3% | ||
| Maternal age, years | 31.7 ± 5.9 | 32.1 ± 5.9 | 31.7 ± 5.9 | 31.3 ± 5.9 | <0.001 (L; A; S) | 32.2 ± 6.0 | 31.7 ± 5.9 | 31.4 ± 5.8 |
| Weight, kg | 64.4 ± 13.4 | 66.8 ± 15.8 | 64.2 ± 13.2 | 63.3 ± 12.0 | <0.001 (L; A; S) | 64.9 ± 14.2 | 64.2 ± 13.2 | 65.2 ± 13.8 |
| Height, m | 161.1 ± 6.6 | 161.4 ± 6.6 | 161.2 ± 6.6 | 160.4 ± 6.9 | <0.001 (L; A-S) | 161.5 ± 6.5 | 161.2 ± 6.6 | 160.4 ± 6.9 |
| BMI, kg/m2 | 24.8 ± 4.9 | 25.6 ± 5.7 | 24.7 ± 4.8 | 24.6 ± 4.3 | <0.001 (L-A; S) | 24.9 ± 5.1 | 24.7 ± 4.8 | 25.3 ± 4.9 |
| Nulliparous | 7509 (50.9) | 902 (51.7) | 5595 (50.9) | 1012 (50.3) | 0.685 | 753 (52.6) | 5721 (51.1) | 1035 (49.0) |
| Cigarette smoker | 2118 (14.5) | 459 (26.5) | 1511 (13.9) | 148 (7.4) | <0.001 (L; A; S) | 385 (27.1) | 1578 (14.2) | 155 (7.4) |
| Diabetes mellitus | 154 (1.0) | 12 (0.7) | 87 (0.8) | 55 (2.7) | <0.001 (S-A; L) | 9 (0.6) | 87 (0.8) | 58 (2.7) |
| Assisted reproduction techniques | 1150 (7.8) | 140 (8.0) | 863 (7.9) | 147 (7.3) | 0.333 | 119 (8.3) | 879 (7.9) | 152 (7.2) |
| Gestational age (days) | 274 ± 14.2 | 267 ± 20.4 | 275 ± 12.6 | 273 ± 14.6 | <0.001 (S; L; A) | 267 ± 20.5 | 275 ± 12.6 | 273 ± 15.5 |
| Cesarean section | 3527 (23.9) | 587 (33.7) | 2358 (21.5) | 582 (28.9) | <0.001 (A; L; S) | 488 (34.1) | 2406 (21.5) | 633 (30.0) |
| Prematurity | 1271 (8.6) | 319 (18.3) | 753 (6.9) | 199 (9.9) | <0.001 (A; L; S) | 267 (18.7) | 788 (7.0) | 216 (10.2) |
| <28 | 55 (0.4) | 28 (1.6) | 18 (0.2) | 9 (0.4) | 21 (1.5) | 18 (0.2) | 16 (0.8) | |
| (28–34) | 286 (1.9) | 105 (6.0) | 148 (1.3) | 33 (1.6) | 89 (6.2) | 160 (1.4) | 37 (1.8) | |
| (34–37) weeks | 930 (6.3) | 186 (10.7) | 587 (5.3) | 157 (7.8) | 157 (11.0) | 610 (5.4) | 163 (7.7) | |
| Umbilical artery pH | 7.25 ± 0.094 | 7.23 ± 0.101 | 7.25 ± 0.093 | 7.25 ± 0.088 | 0.010 (S; A-L) | 7.23 ± 0.104 | 7.25 ± 0.092 | 7.24 ± 0.094 |
| Apgar < 7at 1st min. | 541 (3.7) | 151 (10.7) | 313 (3.5) | 77 (4.7) | <0.001 (A-L; S) | 129 (9.0) | 325 (2.9) | 87 (4.1) |
| Apgar < 7 at 5th min. | 100 (0.7) | 36 (2.5) | 56 (0.6) | 8 (0.5) | <0.001 (L-A; S) | 30 (2.1) | 57 (0.5) | 13 (0.6) |
| NICU admission | 363 (2.5) | 140 (8.0) | 180 (1.6) | 43 (2.1) | <0.001 (L-A; S) | 117 (8.2) | 192 (1.7) | 54 (2.6) |
| Perinatal mortality | 65 (0.4) | 28 (1.6) | 32 (0.3) | 5 (0.2) | <0.001 (L-A; S) | 26 (1.8) | 31 (0.3) | 8 (0.4) |
| Composite outcome 1 | 3878 (26.3) | 665 (38.1) | 2582 (23.5) | 631 (31.4) | <0.001 (A; L; S) | 549 (38.4) | 2642 (23.6) | 687 (32.5) |
| Composite outcome 2 | 832 (5.6) | 245 (14.0) | 473 (4.3) | 114 (5.7) | <0.001 (A-L; S) | 208 (14.5) | 495 (4.4) | 129 (6.1) |
| Perinatal Outcome | (n = 10,984) | (n = 1744) | (n = 1) | (n = 314; 18%) | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| P1 vs. | P2 vs. SGANewCC | P3 vs. | P4 vs. | |||||
| Cesarean section | 2358 (21.5) | 587 (33.7) | 1 (100) | 100 (31.8) | 0.215 | 0.337 | <0.001 | 0.559 |
| Prematurity | 753 (6.9) | 319 (18.3) | 1 (100) | 53 (16.9) | 0.069 | 0.183 | <0.001 | 0.578 |
| < 28 | 18 (0.2) | 28 (1.6) | 1 (100) | 8 (2.5) | ||||
| (28–34) | 148 (1.3) | 105 (6.0) | - | 16 (5.1) | ||||
| (34–37) weeks | 587 (5.3) | 186 (10.7) | - | 29 (9.2) | ||||
| Umbilical artery pH | 7.25 ± 0.093 | 7.23 ± 0.101 | - | 7.23 ± 0.089 | - | - | 0.150 | 0.902 |
| Apgar < 7at 1st min. | 313 (3.5) | 151 (10.7) | - | 22 (9.0) | 0.972 | 0.913 | <0.001 | 0.497 |
| Apgar < 7 at 5th min. | 56 (0.6) | 36 (2.5) | - | 6 (2.4) | 0.995 | 0.979 | 0.007 | 0.924 |
| NICU admission | 180 (1.6) | 140 (8.0) | 1 (100) | 24 (7.6) | 0.016 | 0.081 | <0.001 | 0.910 |
| Perinatal mortality | 32 (0.3) | 28 (1.6) | - | 2 (0.6) | 0.997 | 0.984 | 0.244 | 0.302 |
| - Composite outcome 1 | 2582 (23.5) | 665 (38.1) | 1 (100) | 117 (37.3) | 0.235 | 0.382 | <0.001 | 0.810 |
| - Composite outcome 2 | 473 (4.3) | 245 (14.0) | 1 (100) | 38 (12.1) | 0.043 | 0.141 | <0.001 | 0.423 |
| Perinatal Outcome | Small for Gestational Age | (N = 10,812) | ||
|---|---|---|---|---|
(N = 1430) | (N = 1) | (N = 314) | ||
| Cesarean section † | 34.1% 1.55 (1.36, 1.75) *** | 100% - | 31.8% 1.53 (1.19, 1.96) ** | 21.2% |
| pHUA (mean ± s.d.; IC95%) | 7.23 ± 0.10 (−0.022, −0.004) ** | - | 7.23 ± 0.09; (−0.034, 0.034) | 7.25 ± 0.09 |
| pHUA < 7 | 0.8% 2.41 (1.18, 4.91) * | - | 0.3% 1.00 (0.13, 7.43) | 0.3% |
| Apgar < 7 at 1st min. † | 9.0% 2.26 (1.79, 2.86) *** | - | 7.0% 1.81 (1.12, 2.93)* | 2.8% |
| Apgar < 7 at 5th min. † | 2.1% 2.43 (1.46, 4.04) ** | - | 1.9% 2.04 (0.79, 5.24) | 0.5% |
| Prematurity (total) † | 18.6% 3.20 (2.74, 3.73) *** | 100% - | 16.9% 2.84 (2.09, 3.85) *** | 6.7% |
| <28 | 1.4% 17.03 (7.74, 37.46) *** | 100% - | 2.6% 31.38 (12.03, 81.89) *** | 0.1% |
| (28–34) | 6.2% 5.06 (3.85, 6.64) *** | - | 5.1% 4.09 (2.41, 6.95) *** | 1.3% |
| (34–37) weeks | 11.0% 2.21 (1.83, 2.66) *** | - | 9.2% 1.82 (1.23, 2.69) ** | 5.3% |
| NICU admission † | 8.1% 5.77 (4.52, 7.37) *** | 100% - | 7.6% 5.41 (3.47, 8.43) *** | 1.5% |
| Perinatal mortality † | 1.8% 2.95 (1.61, 5.40) *** | - | 0.6% 2.38 (0.57, 10.03) | 0.3% |
| Composite outcome (at least one perinatal outcome) | ||||
| - Composite outcome 1 | 38.3% 1.56 (1.38, 1.77) *** | 100% - | 37.3% 1.66 (1.30, 2.11) *** | 23.2% |
| - Composite outcome 2 | 14.5% 1.90 (1.54, 2.35) *** | 100% - | 12.1% 1.76 (1.06, 2.60) * | 4.2% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González González, N.L.; González Dávila, E.; González Martín, A.; Armas, M.; Tascón, L.; Farras, A.; Higueras, T.; Mendoza, M.; Carreras, E.; Goya, M. Abnormal Maternal Body Mass Index and Customized Fetal Weight Charts: Improving the Identification of Small for Gestational Age Fetuses and Newborns. Nutrients 2023, 15, 587. https://doi.org/10.3390/nu15030587
González González NL, González Dávila E, González Martín A, Armas M, Tascón L, Farras A, Higueras T, Mendoza M, Carreras E, Goya M. Abnormal Maternal Body Mass Index and Customized Fetal Weight Charts: Improving the Identification of Small for Gestational Age Fetuses and Newborns. Nutrients. 2023; 15(3):587. https://doi.org/10.3390/nu15030587
Chicago/Turabian StyleGonzález González, Nieves Luisa, Enrique González Dávila, Agustina González Martín, Marina Armas, Laura Tascón, Alba Farras, Teresa Higueras, Manel Mendoza, Elena Carreras, and María Goya. 2023. "Abnormal Maternal Body Mass Index and Customized Fetal Weight Charts: Improving the Identification of Small for Gestational Age Fetuses and Newborns" Nutrients 15, no. 3: 587. https://doi.org/10.3390/nu15030587