
Dietary Effects on Pain Symptoms in Patients with Fibromyalgia Syndrome: Systematic Review and Future Directions


Abstract
:1. Introduction
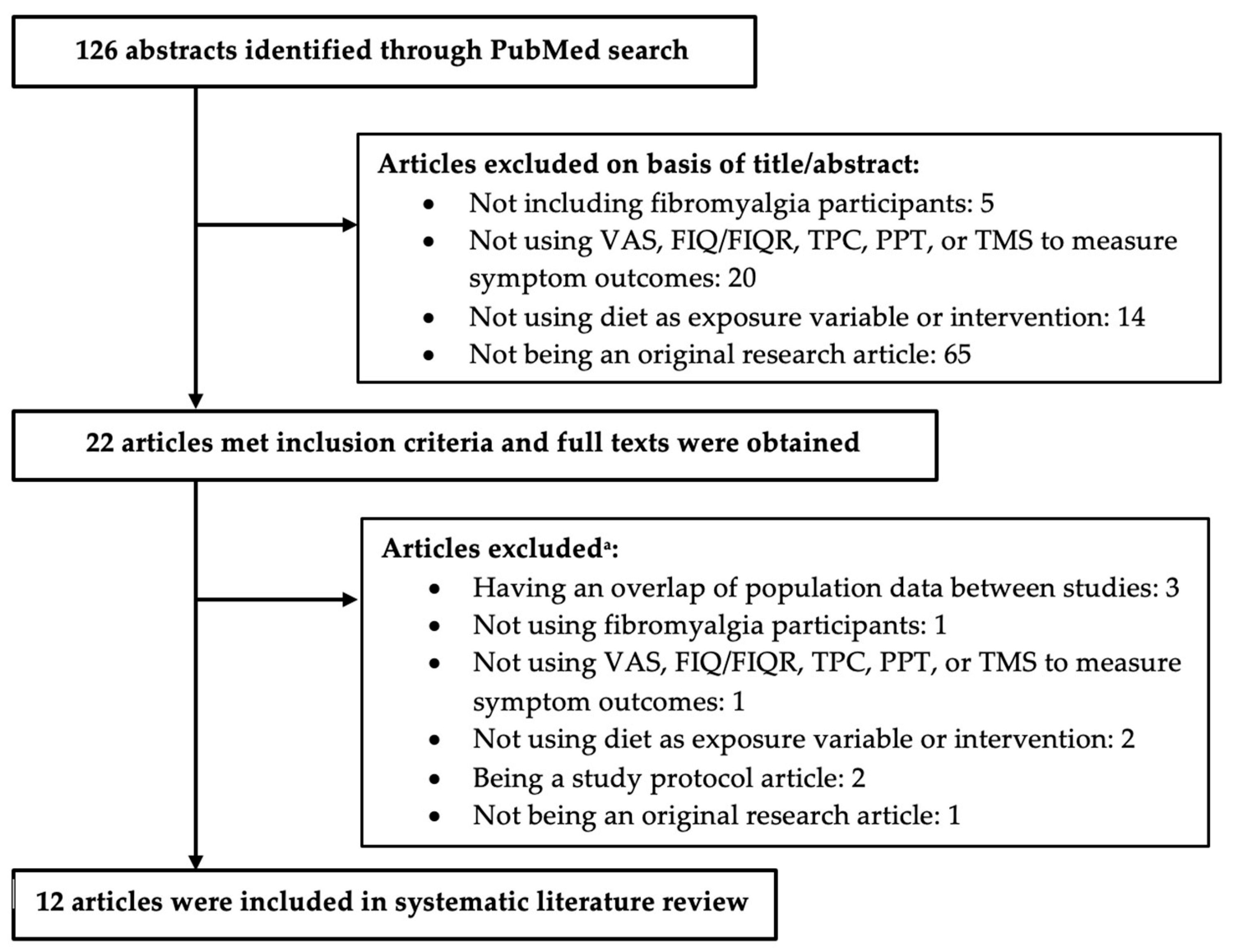
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siracusa, R.; Paola, R.D.; Cuzzocrea, S.; Impellizzeri, D. Fibromyalgia: Pathogenesis, Mechanisms, Diagnosis and Treatment Options Update. Int. J. Mol. Sci. 2021, 22, 3891. [Google Scholar] [CrossRef] [PubMed]
- Sarzi-Puttini, P.; Giorgi, V.; Marotto, D.; Atzeni, F. Fibromyalgia: An update on clinical characteristics, aetiopathogenesis and treatment. Nat. Rev. Rheumatol. 2020, 16, 645–660. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.D.; Albenberg, L.; Lee, D.; Kratz, M.; Gottlieb, K.; Reinisch, W. The Importance and Challenges of Dietary Intervention Trials for Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2017, 23, 181–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clem, J.; Barthel, B. A Look at Plant-Based Diets. Missouri Med. 2021, 118, 233–238. [Google Scholar] [PubMed]
- Haefeli, M.; Elfering, A. Pain assessment. Eur. Spine J. 2006, 15 (Suppl. 1), S17–S24. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef] [PubMed]
- National Heart Lung and Blood Institute. Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 5 July 2022).
- Kaartinen, K.; Lammi, K.; Hypen, M.; Nenonen, M.; Hanninen, O.; Rauma, A.L. Vegan diet alleviates fibromyalgia symptoms. Scand. J. Rheumatol. 2000, 29, 308–313. [Google Scholar] [CrossRef]
- Marum, A.P.; Moreira, C.; Tomas-Carus, P.; Saraiva, F.; Guerreiro, C.S. A low fermentable oligo-di-mono-saccharides and polyols (FODMAP) diet is a balanced therapy for fibromyalgia with nutritional and symptomatic benefits. Nutr. Hosp. 2017, 34, 667–674. [Google Scholar] [CrossRef] [Green Version]
- Rodrigo, L.; Blanco, I.; Bobes, J.; de Serres, F.J. Effect of one year of a gluten-free diet on the clinical evolution of irritable bowel syndrome plus fibromyalgia in patients with associated lymphocytic enteritis: A case-control study. Arthritis Res. Ther. 2014, 16, 421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schrepf, A.; Harte, S.E.; Miller, N.; Fowler, C.; Nay, C.; Williams, D.A.; Clauw, D.J.; Rothberg, A. Improvement in the Spatial Distribution of Pain, Somatic Symptoms, and Depression After a Weight Loss Intervention. J. Pain 2017, 18, 1542–1550. [Google Scholar] [CrossRef] [PubMed]
- Isasi, C.; Colmenero, I.; Casco, F.; Tejerina, E.; Fernandez, N.; Serrano-Vela, J.I.; Castro, M.J.; Villa, L.F. Fibromyalgia and non-celiac gluten sensitivity: A description with remission of fibromyalgia. Rheumatol. Int. 2014, 34, 1607–1612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen, L.B.; Mikkelsen, K.; Haugen, M.; Pripp, A.H.; Fields, J.Z.; Forre, O.T. Treatment of fibromyalgia at the Maharishi Ayurveda Health Centre in Norway II--a 24-month follow-up pilot study. Clin. Rheumatol. 2012, 31, 821–827. [Google Scholar] [CrossRef]
- Rasmussen, L.B.; Mikkelsen, K.; Haugen, M.; Pripp, A.H.; Forre, O.T. Treatment of fibromyalgia at the Maharishi Ayurveda Health Centre in Norway. A six-month follow-up study. Clin. Exp. Rheumatol. 2009, 27, S46–S50. [Google Scholar]
- Bennett, R.M. A raw vegetarian diet for patients with fibromyalgia. Curr. Rheumatol. Rep. 2002, 4, 284. [Google Scholar] [CrossRef] [PubMed]
- Correa-Rodriguez, M.; Casas-Barragan, A.; Gonzalez-Jimenez, E.; Schmidt-RioValle, J.; Molina, F.; Aguilar-Ferrandiz, M.E. Dietary Inflammatory Index Scores Are Associated with Pressure Pain Hypersensitivity in Women with Fibromyalgia. Pain Med. 2020, 21, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, L.; Blanco, I.; Bobes, J.; de Serres, F.J. Clinical impact of a gluten-free diet on health-related quality of life in seven fibromyalgia syndrome patients with associated celiac disease. BMC Gastroenterol. 2013, 13, 157. [Google Scholar] [CrossRef] [Green Version]
- Lamb, J.J.; Konda, V.R.; Quig, D.W.; Desai, A.; Minich, D.M.; Bouillon, L.; Chang, J.L.; Hsi, A.; Lerman, R.H.; Kornberg, J.; et al. A program consisting of a phytonutrient-rich medical food and an elimination diet ameliorated fibromyalgia symptoms and promoted toxic-element detoxification in a pilot trial. Altern. Ther. Health Med. 2011, 17, 36–44. [Google Scholar] [PubMed]
- Marum, A.P.; Moreira, C.; Saraiva, F.; Tomas-Carus, P.; Sousa-Guerreiro, C. A low fermentable oligo-di-mono saccharides and polyols (FODMAP) diet reduced pain and improved daily life in fibromyalgia patients. Scand. J. Pain 2016, 13, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Vellisca, M.Y.; Latorre, J.I. Monosodium glutamate and aspartame in perceived pain in fibromyalgia. Rheumatol. Int. 2014, 34, 1011–1013. [Google Scholar] [CrossRef] [PubMed]
- Azad, K.A.; Alam, M.N.; Haq, S.A.; Nahar, S.; Chowdhury, M.A.; Ali, S.M.; Ullah, A.K. Vegetarian diet in the treatment of fibromyalgia. Bangladesh Med. Res. Counc. Bull. 2000, 26, 41–47. [Google Scholar]
- Donaldson, M.S.; Speight, N.; Loomis, S. Fibromyalgia syndrome improved using a mostly raw vegetarian diet: An observational study. BMC Complement Altern. Med. 2001, 1, 7. [Google Scholar] [CrossRef] [Green Version]
- Holton, K.F.; Taren, D.L.; Thomson, C.A.; Bennett, R.M.; Jones, K.D. The effect of dietary glutamate on fibromyalgia and irritable bowel symptoms. Clin. Exp. Rheumatol. 2012, 30, 10–17. [Google Scholar] [PubMed]
- Slim, M.; Calandre, E.P.; Garcia-Leiva, J.M.; Rico-Villademoros, F.; Molina-Barea, R.; Rodriguez-Lopez, C.M.; Morillas-Arques, P. The Effects of a Gluten-free Diet Versus a Hypocaloric Diet Among Patients with Fibromyalgia Experiencing Gluten Sensitivity-like Symptoms: A Pilot, Open-Label Randomized Clinical Trial. J. Clin. Gastroenterol. 2017, 51, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Pagliai, G.; Colombini, B.; Dinu, M.; Whittaker, A.; Masoni, A.; Danza, G.; Amedei, A.; Ballerini, G.; Benedettelli, S.; Sofi, F. Effectiveness of a Khorasan Wheat-Based Replacement on Pain Symptoms and Quality of Life in Patients with Fibromyalgia. Pain Med. 2020, 21, 2366–2372. [Google Scholar] [CrossRef] [PubMed]
- Senna, M.K.; Sallam, R.A.; Ashour, H.S.; Elarman, M. Effect of weight reduction on the quality of life in obese patients with fibromyalgia syndrome: A randomized controlled trial. Clin. Rheumatol. 2012, 31, 1591–1597. [Google Scholar] [CrossRef] [PubMed]
- Hanninen, O.; Kaartinen, K.; Rauma, A.L.; Nenonen, M.; Torronen, R.; Hakkinen, A.S.; Adlercreutz, H.; Laakso, J. Antioxidants in vegan diet and rheumatic disorders. Toxicology 2000, 155, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Kocyigit, B.F.; Okyay, R.A. The relationship between body mass index and pain, disease activity, depression and anxiety in women with fibromyalgia. PeerJ 2018, 6, e4917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spencer, E.A.; Appleby, P.N.; Davey, G.K.; Key, T.J. Diet and body mass index in 38000 EPIC-Oxford meat-eaters, fish-eaters, vegetarians and vegans. Int. J. Obes. Relat. Metab. Disord. 2003, 27, 728–734. [Google Scholar] [CrossRef] [Green Version]
- Barone, M.; Della Valle, N.; Rosania, R.; Facciorusso, A.; Trotta, A.; Cantatore, F.P.; Falco, S.; Pignatiello, S.; Viggiani, M.T.; Amoruso, A.; et al. A comparison of the nutritional status between adult celiac patients on a long-term, strictly gluten-free diet and healthy subjects. Eur. J. Clin. Nutr. 2016, 70, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Field, R.; Field, T.; Pourkazemi, F.; Rooney, K. Low-carbohydrate and ketogenic diets: A scoping review of neurological and inflammatory outcomes in human studies and their relevance to chronic pain. Nutr. Res. Rev. 2022. [Google Scholar] [CrossRef]


{kind=link}
| First Author, Publication Year | Study Design | Year(s) | Country | Number of Participants | Sex a | Age b | Race or Ethnicity | Diagnosis c |
|---|---|---|---|---|---|---|---|---|
| Azad 2000 [21] | Intervention Control Trial | No data | Bangladesh | 78 | Female 78% Male 22% | 30.9 (12–60) | No data | FMS |
| Correa-Rodríguez 2020 [16] | Observational, Cross-sectional | 2018 | Spain | 95 | Female 100% | 55.76 | No data | FMS |
| Donaldson 2001 [22] | Intervention Pre and Post Trial | No data | United States | 20 | Female 93% Male 7% | (45–54) | No data | FMS |
| Hänninen 2000 [27] | Intervention Pre and Post Control Trial | No data | Finland | 33 | No data | 51 | No data | FMS |
| Holton 2012 [23] | Intervention Pre and Post Trial | No data | United States | 37 | Female 92% Male 8% | 51.6 | No data | FMS and IBS |
| Lamb 2011 [18] | Intervention Cross-over Trial | 2008 | United States | 8 | Female 100% | 55.6 (48–74) | White | FMS |
| Marum 2016 [19] | Intervention Pre and Post Trial | 2015 | Portugal | 38 | Female 100% | 51 | No data | FMS and GID |
| Pagliai 2020 [25] | Intervention Cross-over Trial | No data | Italy | 20 | Female 95% Male 5% | 48.95 | No data | FMS |
| Rodrigo 2013 [17] | Intervention Pre and Post Trial | 2007–2012 | Spain | 7 | Female 100% | 49 (34–68) | White | FMS, IBS and CD |
| Senna 2012 [26] | Intervention Control Trial | 2011 | Egypt | 83 | Female 90% Male 10% | 45.6 | No data | FMS |
| Slim 2017 [24] | Intervention Parallel-group Trial | 2012–2014 | Spain | 55 | Female 97% Male 3% | HCD: 53 (32–65) GFD: 52 (36–66) | No data | FMS and GS |
| Vellisca 2014 [20] | Intervention Control Trial | No data | Spain | 72 | Female 100% | 40.98 (24–65) | No data | FMS |
| First Author of Article | Dietary Variable or Intervention | Length of Intervention | FIQ/FIQR c | VAS d | |||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | End | ||||||||
| Azad | Vegetarian | 6 weeks | 5.7 ± 1.8 | 5.0 ± 1.8 * | |||||
| Control | 6 weeks | 6.2 ± 1.9 | 2.3 ± 1.3 * | ||||||
| Cross-sectional | Cross-sectional | ||||||||
| Correa-Rodríguez a | Anti-Inflammatory diet: DII score Quartile 1 | N/A | 70.5 ± 13.3 | 7.20 ± 1.64 | |||||
| Quartile 2 | 79.9 ± 10.5 | 7.91 ± 1.57 | |||||||
| Quartile 3 | 69.2 ± 20.1 | 7.48 ± 2.10 | |||||||
| Quartile 4 | 71.9 ± 15.4 | 7.40 ± 1.14 | |||||||
| Baseline | 2 months | End | Baseline | 2 months | End | ||||
| Donaldson | Raw Vegetarian | 7 months | 51.4 ± 14.2 | 33.6 ± 15.6 | 27.6 ± 19.0 * | ||||
| Baseline | Middle | End | |||||||
| Hänninen b | Living Food | 3 months | 6.0 | 3.0 | 3.2 * | ||||
| Control | 3 months | 5.8 | 4.8 | 6.5 | |||||
| Baseline | End | Baseline | End | ||||||
| Holton | Dietary Additive Excitotoxin Elimination | 4 weeks | 58.6 | 36.4 * | 13.1 | 7.7 * | |||
| Baseline | End | ||||||||
| Lamb | Control | 4 weeks | 46.3 ± 3.4 | 43.6 ± 5.1 | |||||
| Modified Elimination | 4 weeks | 36.6 ± 8.2 | |||||||
| Baseline | End | Baseline | End | ||||||
| Marum | Low FODMAP | 4 weeks | 61.6 | 47.9 * | 6.6 | 4.9 * | |||
| Baseline | End | Baseline | End | ||||||
| Rodrigo | Gluten-Free | 1 year | 74.3 ± 2.9 | 36.6 ± 4.0 * | 8.0 ± 0.5 | 3.9 ± 1.0 * | |||
| Baseline | End | ||||||||
| Senna | Energy-restricted | 6 months | 54.6 ± 13.1 | 47 ± 5.1 * | |||||
| Control | 6 months | 53.2 ± 11.55 | 51.6 ± 9.4 | ||||||
| Baseline | End | ||||||||
| Slim | Gluten-Free | 24 weeks | 69.5 ± 16.3 | 60.3 ± 19.6 | |||||
| Hypocaloric (Control) | 24 weeks | 70.4 ± 16.1 | 61.7 ± 22.2 | ||||||
| Baseline | End | ||||||||
| Pagliai | Khorasan Wheat Replacement | 8 weeks | 54.3 | 42.06 * | |||||
| Control | 8 weeks | 54.06 | 53.87 | ||||||
| Baseline | 1 month | 2 months | End | ||||||
| Vellisca | Control | 3 months | 5.63 ± 0.86 | 5.41 ± 0.73 | 5.05 ± 0.82 | 5.31 ± 0.88 | |||
| Dietary Additive Excitotoxin Elimination | 3 months | 5.58 ± 0.91 | 5.05 ± 0.82 | 4.88 ± 0.97 | 5.15 ± 0.95 | ||||
| First Author of Article | Dietary Variable or Intervention | Length of Intervention | TPC | TMS | ||
|---|---|---|---|---|---|---|
| Baseline | End | Baseline | End | |||
| Azad | Vegetarian | 6 weeks | 15.7 ± 2.4 | 14.7 ± 3.6 * | - | - |
| Control | 6 weeks | 16.1 ± 2.3 | 6.4 ± 3.0 * | - | - | |
| Holton | Dietary Additive Excitotoxin Elimination | 4 weeks | 16.5 | 14.0 * | 35.2 | 25.7 * |
| Rodrigo | Gluten-Free | 1 year | 16.3 ± 2.4 | 8.0 ± 1.6 * | - | - |
| Senna | Energy-restricted | 6 months | 4.9 ± 0.8 | - | ||
| Control | 6 months | 5.7 ± 1 | ||||
| First Author of Article | Dietary Variable or Intervention | Length of Intervention | PPT | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Occiput | Trapezius | Zygapophyseal Joint | Supraspinatus | Second Rib | Epicondyle | Gluteus | Greater Trochanter | Knee | ||||||||||||
| Cross-Sectional | ||||||||||||||||||||
| Correa-Rodríguez a | Anti-Inflammatory: DII score Quartile 1 Quartile 2 Quartile 3 Quartile 4 | N/A | 1.18 ± 0.79 | 1.37 ± 0.84 | 1.50 ± 1.12 | 1.61 ± 1.14 | 1.09 ± 0.49 | 1.24 ± 0.74 | 2.43 ± 1.63 | 2.39 ± 0.95 | 2.17 ± 1.00 | |||||||||
| 0.94 ± 0.75 | 0.97 ± 0.65 | 0.97 ± 0.72 | 1.31 ± 0.89 | 0.87 ± 0.52 | 0.95 ± 0.59 | 2.12 ± 1.70 | 2.36 ± 1.47 | 1.91 ± 1.43 | ||||||||||||
| 0.72 ± 0.44 | 0.83 ± 0.41 | 0.90 ± 0.53 | 1.08 ± 0.52 | 0.80 ± 0.37 | 0.85 ± 0.43 | 1.65 ± 1.32 | 1.78 ± 0.87 | 1.05 ± 1.05 | ||||||||||||
| 0.57 ± 0.37 * | 0.73 ± 0.45 * | 0.80 ± 0.53 * | 0.99 ± 0.51 | 0.67 ± 0.25 * | 0.78 ± 0.35 | 1.44 ± 0.78 | 1.65 ± 0.72 * | 1.20 ± 0.65 * | ||||||||||||
| BL | End | BL | End | BL | End | BL | End | BL | End | BL | End | BL | End | BL | End | BL | End | |||
| Lamb | Control | 4 weeks | 0.89 | 1.35 | 1.62 | 2.11 | 1.11 | 1.64 | 1.85 | 2.19 | 1.11 | 1.03 | 0.94 | 1.13 | 2.38 | 2.73 | 1.78 | 2.26 | 1.41 | 1.29 |
| Modified Elimination | 4 weeks | 1.48 | 2.33 | 2.05 | 2.50 | 0.93 | 1.54 | 2.81 | 2.41 | 1.87 | ||||||||||
| End | End | End | End | End | End | End | End | End | ||||||||||||
| Senna | Energy-restricted | 6 months | 4.5 ± 2.9 | 6 ± 2.3 * | 4.7 ± 1.9 | 4.6 ± 2.1 * | 5.8 ± 1.5 | 4.9 ± 1.8 | 4.3 ± 1.8 * | 4.9 ± 2.1 * | 4.2 ± 1.8 ** | |||||||||
| Control | 5.1 ± 2.7 | 7.3 ± 2.4 | 4.5 ± 1.7 | 5.9 ± 2.7 | 6 ± 1.7 | 4.3 ± 2.2 | 5.7 ± 2.2 | 6.2 ± 2.4 | 6.1 ± 2 | |||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maddox, E.K.; Massoni, S.C.; Hoffart, C.M.; Takata, Y. Dietary Effects on Pain Symptoms in Patients with Fibromyalgia Syndrome: Systematic Review and Future Directions. Nutrients 2023, 15, 716. https://doi.org/10.3390/nu15030716
Maddox EK, Massoni SC, Hoffart CM, Takata Y. Dietary Effects on Pain Symptoms in Patients with Fibromyalgia Syndrome: Systematic Review and Future Directions. Nutrients. 2023; 15(3):716. https://doi.org/10.3390/nu15030716
Chicago/Turabian StyleMaddox, Emma K., Shawn C. Massoni, Cara M. Hoffart, and Yumie Takata. 2023. "Dietary Effects on Pain Symptoms in Patients with Fibromyalgia Syndrome: Systematic Review and Future Directions" Nutrients 15, no. 3: 716. https://doi.org/10.3390/nu15030716
APA StyleMaddox, E. K., Massoni, S. C., Hoffart, C. M., & Takata, Y. (2023). Dietary Effects on Pain Symptoms in Patients with Fibromyalgia Syndrome: Systematic Review and Future Directions. Nutrients, 15(3), 716. https://doi.org/10.3390/nu15030716